
Abstract
Objectives:
To assess whether there are shared or divergent (a) cognitive and (b) emotion processing characteristics among violent individuals with antisocial personality disorder and/or schizophrenia, diagnoses which are commonly encountered at the interface of mental disorder and violence. Cognition and emotion processing are incorporated into models of violence, and thus an understanding of these characteristics within and between disorder groups may help inform future models and therapeutic targets.
Methods:
Relevant databases (OVID, Embase, PsycINFO) were searched to identify suitable literature. Meta-analyses comparing cognitive function in violent schizophrenia and antisocial personality disorder to healthy controls were conducted. Neuropsychological studies not comparing these groups to healthy controls, and emotion processing studies, were evaluated qualitatively.
Results:
Meta-analyses indicated lower IQ, memory and executive function in both violent schizophrenia and antisocial personality disorder groups compared to healthy controls. The degree of deficit was consistently larger in violent schizophrenia. Both antisocial personality disorder and violent schizophrenia groups had difficulties in aspects of facial affect recognition, although theory of mind results were less conclusive. Psychopathic traits related positively to experiential emotion deficits across the two disorders. Very few studies explored comorbid violent schizophrenia and antisocial personality disorder despite this being common in clinical practice.
Conclusion:
There are qualitatively similar, but quantitatively different, neuropsychological and emotion processing deficits in violent individuals with schizophrenia and antisocial personality disorder which could be developed into transdiagnostic treatment targets for violent behaviour. Future research should aim to characterise specific subgroups of violent offenders, including those with comorbid diagnoses.
Introduction
Although the large majority of those with mental disorder will never be violent, there is a small but independent association between certain mental disorders and violent behaviour. One such group of disorders are psychotic illnesses, including schizophrenia (Walsh et al., 2002). Indeed, a large proportion of offenders utilising forensic mental health services have a diagnosis of schizophrenia or other psychosis (approximately 71% of men in high-secure hospital; Coid et al., 2000). Another class of mental disorders associated with violence are personality disorders (PDs); 16% of homicides by patients in England between 2002 and 2012 were committed by individuals with the diagnosis of a PD (National Confidential Enquiry for Suicide and Homicide, 2014). Antisocial personality disorder (ASPD) specifically is highly prevalent in both prison (47%; Fazel and Danesh, 2002) and forensic mental health populations (55% in high-secure hospital; Coid, 2003).
In order to try to understand these violent behaviours, psychosocial and environmental influences are often considered, such as substance misuse and unemployment (Mullen, 2006). Notwithstanding these important factors, there are also models of violence emerging from the experimental psychology literature which draw on both cognitive and emotion processing traits, including inhibitory control theories (Hoptman, 2015), deficits in social cognitive abilities including facial affect recognition (FAR; Malone et al., 2012) and hostile attribution bias (Harris et al., 2014). In line with this, cognitive and social cognitive functioning in those utilising forensic mental health services has been linked to outcome. Specifically, there is evidence to suggest that poorer neurocognitive (Brugman et al., 2016; Foster et al., 1993) and social cognitive (Brugman et al., 2016; Murphy, 2007; O’Reilly et al., 2015) abilities are related to higher risk of violence. Furthermore, understanding the nature and degree of such problems can assist in understanding the levels of functional impairments which may be experienced by these diagnostic groups; poor neurocognitive and social cognitive functioning among individuals with schizophrenia is already known to be associated with lower levels of community and social functioning (Fett et al., 2011), and this likely applies among ASPD groups too. Thus, these characteristics have potential to (a) inform the development and understanding of models of violent behaviour, (b) inform risk assessment and treatment planning and (c) understand levels of functioning.
As mental health research increasingly aims to move towards transdiagnostic approaches (Insel et al., 2010), the question arises as to which characteristics are shared or divergent between groups exhibiting violent behaviour. This will allow the development and refinement of therapeutic targets which are relevant to many individuals with problematic violent behaviour, both within and across diagnostic groups. Such transdiagnostic targets are desirable for high-cost services, such as forensic mental health services, which in the United Kingdom cost almost £1 billion per year and represents 15% of the total adult mental health budget (Wilson et al., 2011). There are evidence-based psychological therapies for the treatment of cognitive (Wykes et al., 2011) and social cognitive (Kurtz and Richardson, 2012) deficits in individuals with schizophrenia, and these may also be relevant targets in individuals with ASPD. Research indicates that transdiagnostic approaches with these diagnostic groups are feasible. For example, a recent case series of offenders with ASPD found that clozapine effectively reduced the severity of PD symptoms in the large majority of cases (Brown et al., 2014), although this drug is traditionally used to reduce symptoms and aggression in psychosis. This may thus indicate a potentially shared underlying neural basis of violence between ASPD and psychosis. However, further therapeutic options are required, and a thorough understanding of the relevant characteristics of violent groups is an important first step towards this.
Thus, the present systematic review and meta-analysis presents a comprehensive overview of both cognitive and emotion processing traits among violent/antisocial/criminal individuals with diagnoses which are frequently encountered in the interface of mental disorder and violent schizophrenia (VSZ) and ASPD. Meta-analyses comparing neuropsychological function in VSZ and ASPD to healthy controls are presented. Neuropsychological papers not comparing to healthy controls, and emotion processing papers, are synthesised narratively.
Methods
This systematic review and meta-analysis was carried out in accordance with ‘Preferred Reporting Items for Systematic Review and Meta-analysis’ (PRISMA) guidelines.
Information sources and search
Embase (1980–June 2016), Ovid MEDLINE(R) (1946–June 2016) and PsycINFO (2002–June 2016) were searched on 6 June 2016 to identify eligible literature, cross-referencing the following search terms:
cognit* OR neuropsych* OR executive function OR affect* OR emotion;
offender OR criminal OR violen* OR aggress* OR forensic;
schizophrenia OR psychosis OR antisocial personality disorder.
Results were limited to articles in English, featuring human participants and with abstracts available.
Eligibility criteria
Studies were assessed against the following inclusion criteria:
Participants must be adults and have a diagnosis of schizophrenia spectrum disorder, antisocial/dissocial PD or both, using a recognised diagnostic system, and must have a history of violent/aggressive/criminal behaviour. The data must be further reported by diagnostic group status and/or violence status.
Allow comparison between groups. This could be direct comparison between VSZ and ASPD, or a control group including (a) a non-violent sample of clinical cases (e.g. non-violent people with schizophrenia [NVSZ]), (b) non-clinical violent controls (e.g. prisoners), (c) non-clinical, non-violent controls (e.g. hospital staff) and (d) published norms.
Report on (a) at least one standardised neuropsychological measure and/or (b) at least one experimental task of emotion processing including FAR, theory of mind (ToM) or the experience of emotional states.
Studies which focus exclusively on psychopathy (without assessing ASPD) were excluded. Additional assessment of psychopathy when condition #1 is met was acceptable.
Studies must be primary research articles that have been peer-reviewed, i.e. not books, theses.
The decision was made to not exclude studies in which participants were not explicitly characterised as violent, but were characterised as antisocial/criminal, for example, they were incarcerated in prison and/or secure hospitals. This strategy has been applied in other meta-analyses looking at similar groups (Schug and Raine, 2009) and was deemed appropriate in order to incorporate maximal information on a relatively under-studied population. This is in line with spectrum approaches to antisocial behaviour (Krueger et al., 2005), and the exact operationalisation of violence/antisociality in each study is given in Supplementary Table 1.
Study selection
Titles and abstracts were screened to assess for suitability; if insufficient information was provided, the full text was retrieved. After initial screening, the full texts were retrieved to assess its suitability for inclusion. This process was conducted independently by two authors (O.S. and B.G.) and verified between the two authors.
Data collection process
For the meta-analyses, data on cognitive test scores for clinical and control groups were extracted into a spreadsheet by two authors independently (O.S. and B.G.) and reviewed for consistency. Any inconsistencies were discussed until a consensus was reached. For narrative results, data extraction was conducted by the first author, and a random selection of 20 studies was independently extracted by a second author (B.G.) to verify the extraction.
Data items
The following data items were extracted from each paper: sample size, gender, age, diagnosis of participants, method of assessment of violence/antisociality, whether comorbidity was assessed, details of the experimental measures used and the main findings. For papers included in the meta-analyses, mean and standard deviation scores of cognitive tests for clinical and healthy control groups were extracted. Attempts to collect data across multiple cognitive domains were made, including intelligence, memory, executive function and attention. However, due to a lack of available data for the attention domain, only the former three domains were included. Where data were not available, authors were contacted.
Summary measures
For papers reporting on more than one measure purportedly assessing the same domain (e.g. executive function assessed by both the Wisconsin Cart Sorting Test [WCST] and the Tower of London [ToL]), a summary score for that cognitive domain was calculated by taking a mean of the effect sizes of individual scores. Similarly, if a task produced multiple outcome parameters (i.e. categories completed and number of errors on the WCST), then all outcome parameters were extracted and a mean of the effect size was taken for that test. This approach was deemed appropriate as it conferred the lowest risk of researcher bias in choosing one specific parameter/test. When research groups had published data on the same measure(s) with the same sample in different papers, the paper with the largest sample size was chosen. Similarly, for papers where the clinical groups were further divided (i.e. high/low psychopathy groups), the group with the largest number of participants was chosen. For investigations by the same group incorporating the same participants but reporting on different measures (i.e. ToL and WCST in different publications, but in the same sample), these scores were incorporated into a single summary score for the domain. Thus, each sample (as opposed to each paper) had a summary score for each domain.
Synthesis of results
For the meta-analysis, all effect sizes were calculated as Hedge’s g. Effect sizes were calculated so that negative values represent a poorer performance in the clinical group compared to healthy, non-violent controls. A more conservative random effects model was utilised due to the assumption that effect sizes would vary depending on sampling method and population-specific characteristics. Planned analyses included comparing VSZ and ASPD on the cognitive domains of IQ, memory and executive function. Subgroup analyses within diagnostic groups comparing those tasks of executive function assessing impulsivity/inhibitory control with those that did not (see Table 1) were performed due to the hypothesised link with violent behaviour (Hoptman, 2015; Volavka and Citrome, 2008). Publication bias was assessed formally by conducting Egger’s and Begg’s tests. A measure of consistency (I2) was also taken for each set of analyses to assess for heterogeneity. Statistical procedures were carried out using Stata 11 (StataCorp, 2009) metan package for meta-analyses and metabias for publication bias.
Measures included in meta-analyses, grouped by domain.
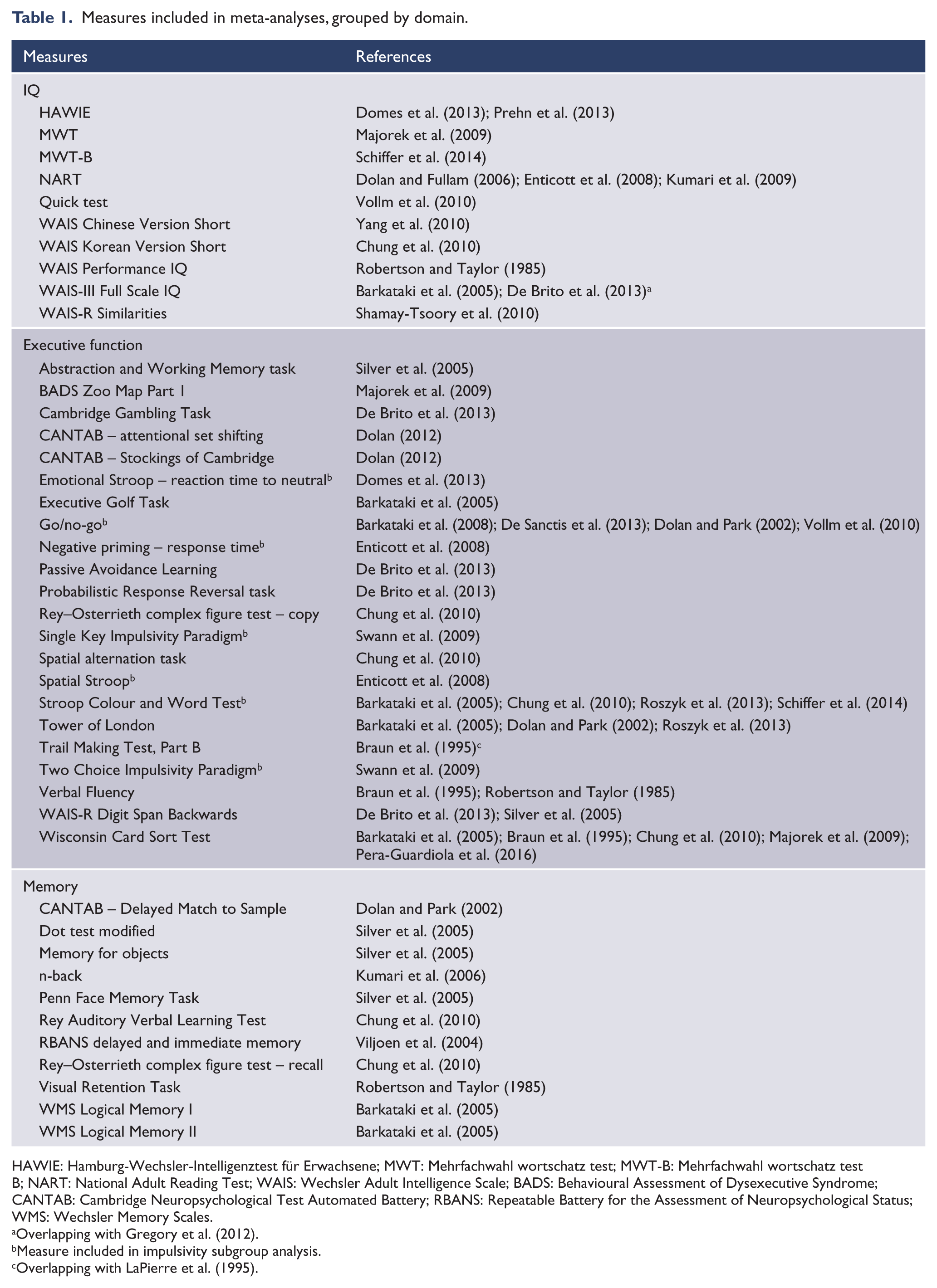
HAWIE: Hamburg-Wechsler-Intelligenztest für Erwachsene; MWT: Mehrfachwahl wortschatz test; MWT-B: Mehrfachwahl wortschatz test B; NART: National Adult Reading Test; WAIS: Wechsler Adult Intelligence Scale; BADS: Behavioural Assessment of Dysexecutive Syndrome; CANTAB: Cambridge Neuropsychological Test Automated Battery; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; WMS: Wechsler Memory Scales.
Overlapping with Gregory et al. (2012).
Measure included in impulsivity subgroup analysis.
Overlapping with LaPierre et al. (1995).
For studies reporting on emotion processing characteristics, or neuropsychological characteristics, comparing to a group other than healthy controls, narrative synthesis was performed.
Results
Study selection
The initial search identified 51 papers (see Figure 1). Reference lists were hand-searched to identify any further literature, including those of two previous meta-analyses on related topics (Ogilvie et al., 2011; Schug and Raine, 2009), resulting in 11 additional papers being added. Thus, 62 papers were included in total (see Table A1 in Supplementary Material).
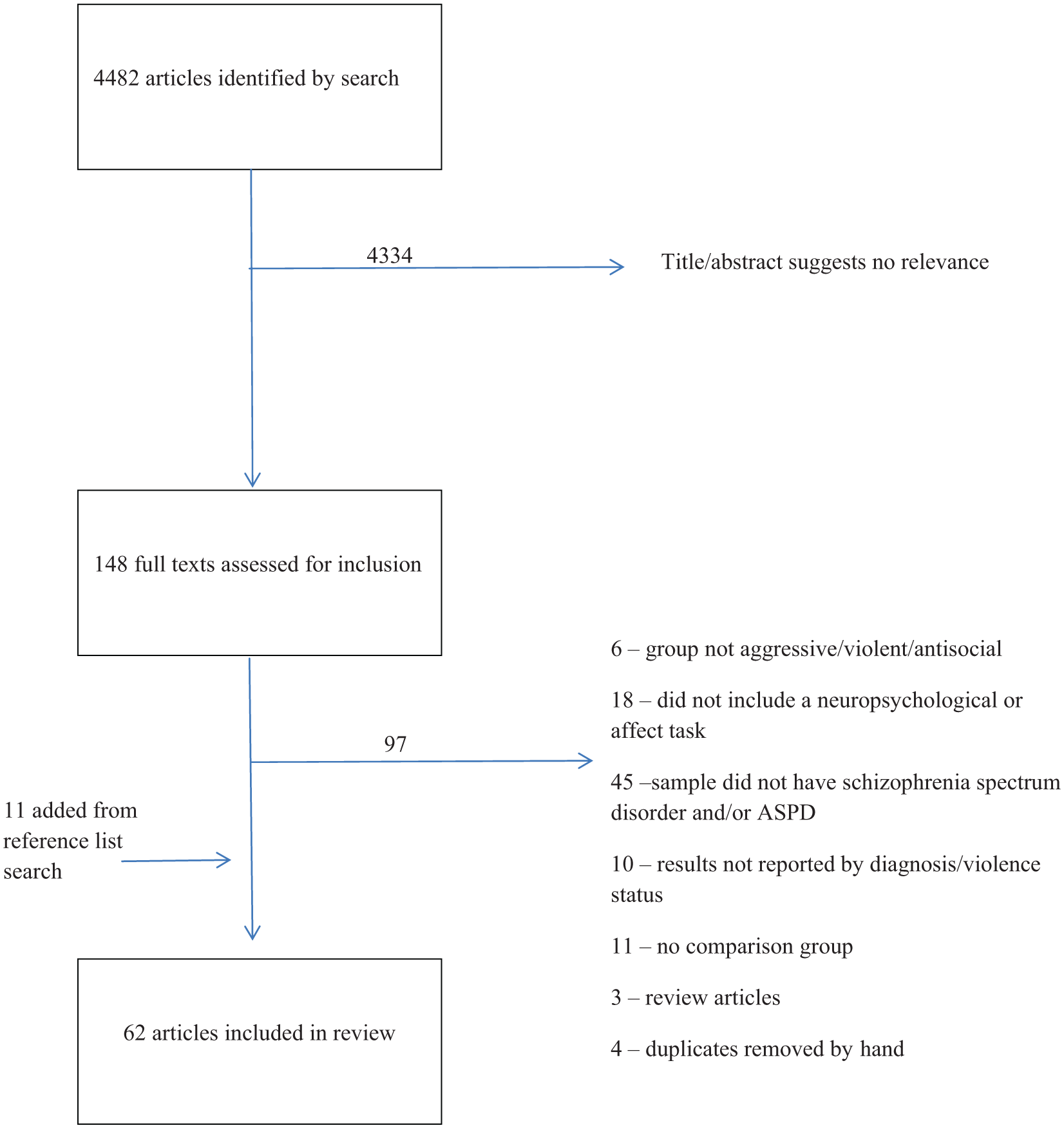
Flowchart of Literature Selection
Study characteristics
A total of 29 studies provided data on cognitive functioning in VSZ and/or ASPD, comparing them to healthy controls. In all, 16 studies compared cognitive functioning in VSZ relative to NVSZ, and eight studies directly compared cognition in VSZ and PD groups. Four studies provided data on comorbid schizophrenia and ASPD. For emotion processing traits, 13 studies examined emotion in VSZ and 13 in ASPD, with two studies providing information on a comorbid group.
Only studies providing cognitive functioning data in VSZ/ASPD groups compared to healthy, non-violent controls (in an effort to standardise the comparison group) were included in the meta-analyses. Thus, 29 studies (including four with overlapping samples) were included in the meta-analyses (see Table 1 for included studies and tests).
Cognitive profiles of violent individuals
Meta-analysis: VSZ and ASPD versus healthy, non-violent controls
Studies assessing IQ showed significantly lower scores in VSZ, compared with healthy, non-violent controls, with a medium-to-large effect size (Hedge’s g = −0.78, df = 5, p < 0.001, CI = [−1.05, −0.52]) and in ASPD with a small effect size (Hedge’s g = −0.30, df = 7, p = 0.003, CI = [−0.50, −0.10]). As confidence intervals do not overlap, it can be inferred that these groups likely also differ significantly from one another, with the VSZ group showing lower IQ than the ASPD group (Figure 2). There was low heterogeneity for both VSZ (I2 = 36.0%, Q = 7.81, p = 0.167) and ASPD groups (I2 = 0.0%, Q = 4.84, p = 0.679).
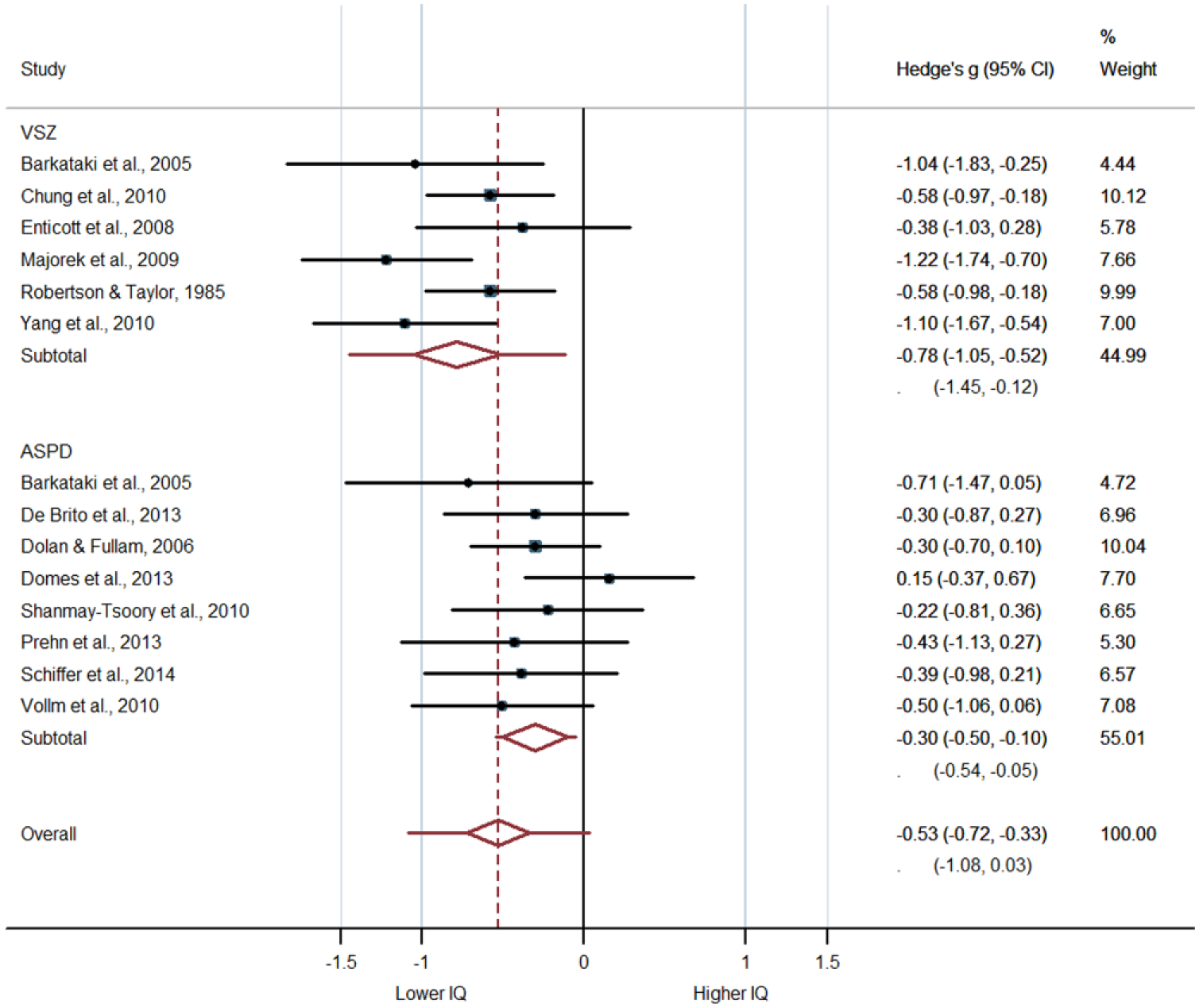
Forest plot presenting effect sizes for studies assessing IQ in violent schizophrenia and antisocial personality disorder.
For memory, there was a significantly poorer performance in VSZ compared with controls, with a large effect size (Hedge’s g = −1.16, df = 4, p < 0.001, CI = [−1.47, −0.86]). The ASPD group also significantly differed from controls with a medium effect size (Hedge’s g = −0.47, df = 2, p = 0.01, CI = [−0.83, −0.10]), and as the confidence intervals do not overlap it is likely that the violent groups also differ from each other (Figure 3). There was moderate but non-significant heterogeneity for the VSZ group (I2 = 45.5%, Q = 7.34, p = 0.119) and low heterogeneity for the ASPD group (I2 = 0.0%, Q = 1.38, p = 0.50).
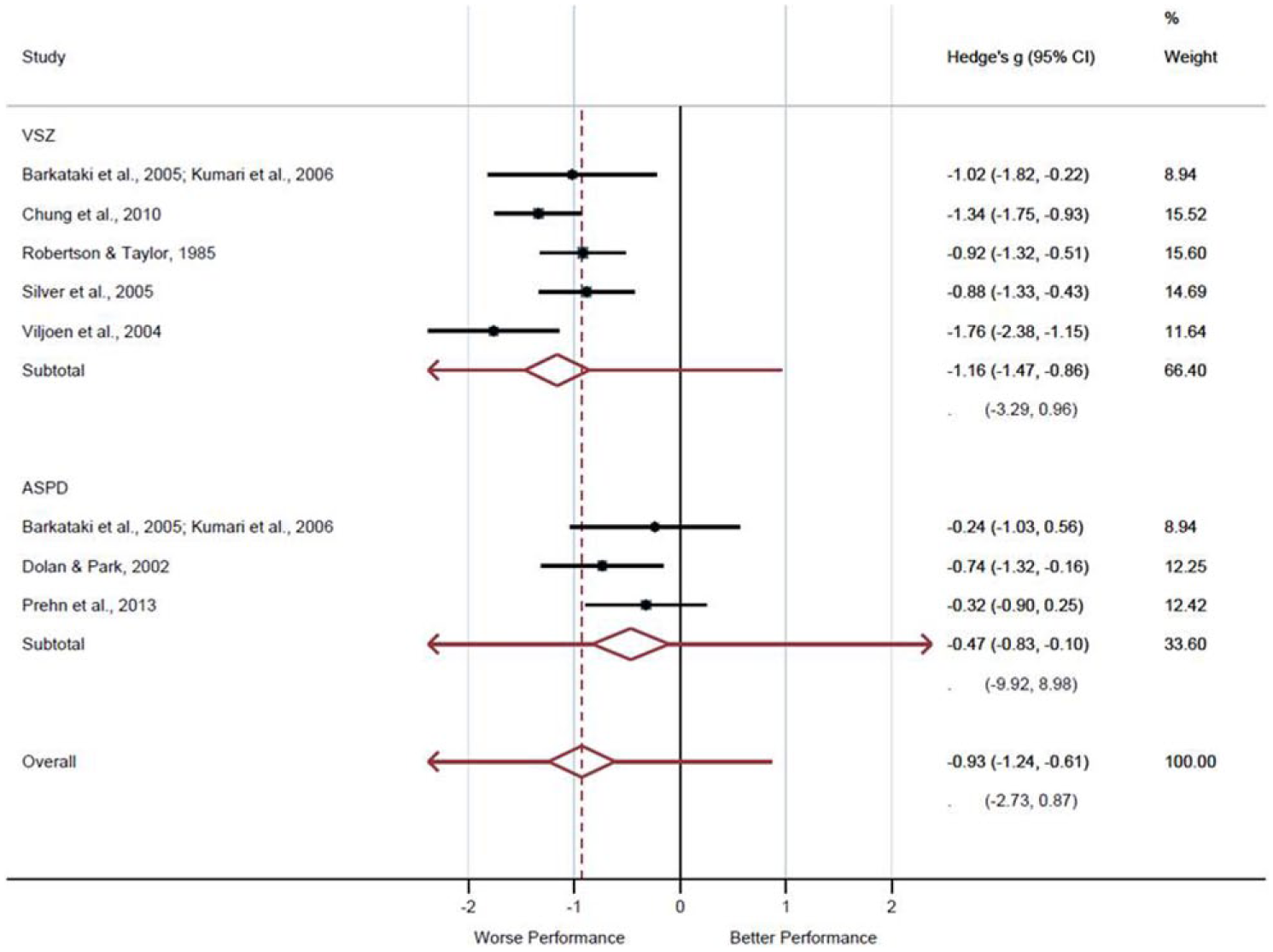
Forest plot presenting effect sizes for studies assessing memory in violent schizophrenia and antisocial personality disorder.
For executive function, there was significantly poorer performance in the VSZ group with a large effect size (Hedge’s g = −0.82, df = 7, p < 0.001, CI = [−1.10, −0.54]) and in the ASPD group with a small-to-medium effect size (Hedge’s g = −0.38, df = 8, p = 0.006, CI = [−0.55, −0.20]). The overlapping confidence intervals suggest that these two groups may not significantly differ from each other, although the degree of overlap is marginal (Figure 4). Significant heterogeneity in the VSZ group must be taken into account (I2 = 58.1%, Q = 16.7, p < 0.019) with a much more consistent result in the ASPD group (I2 = 0.0%, Q = 7.05, p = 0.531).
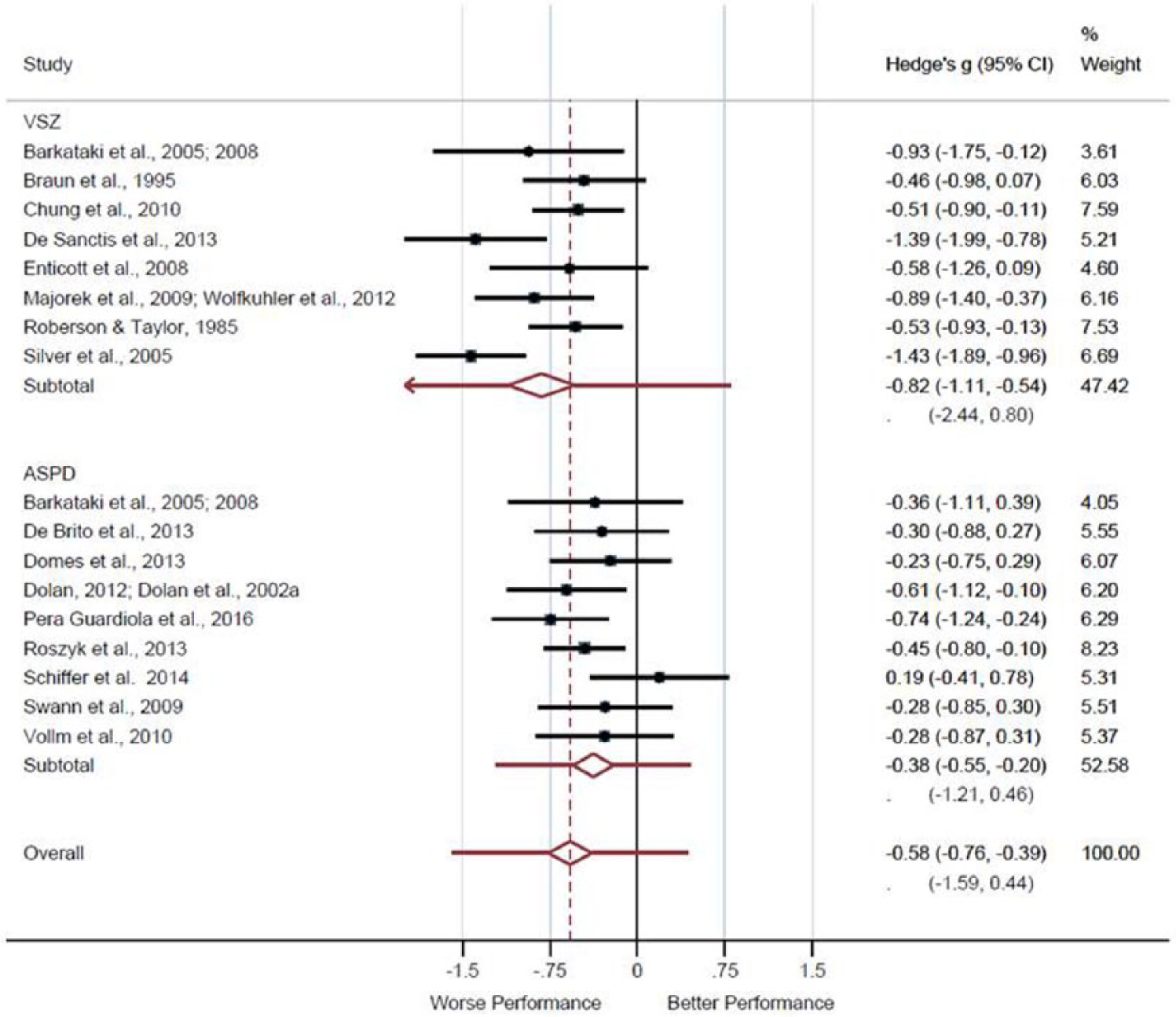
Forest plot presenting effect sizes for studies assessing executive function in violent schizophrenia and antisocial personality disorder.
Subgroup analyses within diagnostic groups to compare executive function tasks which assess impulsivity/cognitive control versus those which do not were conducted to determine whether both or one of these types of tasks was driving the violent groups versus healthy control difference. Within the VSZ group, effect sizes were medium-to-large for both impulsive and non-impulsive tasks, with overlapping confidence intervals, suggesting that this group performs similarly poorly on both types of task compared to controls (impulsive: Hedge’s g = −0.64, df = 3, p = 0.033, CI = [−1.22, −0.05]; non-impulsive: Hedge’s g = −0.81, df = 6, p < 0.001, CI = [−1.08, −0.55]). A similar pattern was observed in the ASPD group, although with smaller effect sizes for both impulsive and non-impulsive tasks (impulsive: Hedge’s g = −0.35, df = 5, p = 0.001, CI = [−0.56, −0.12]; non-impulsive: Hedge’s g= −0.45, df = 5, p < 0.001, CI = [−0.65, −0.26]). There was no significant heterogeneity in the ASPD group (impulsive: I2 = 0.0%, Q = 4.71, p = 0.452; non-impulsive: I2 = 0.0%, Q = 3.92, p = 0.560); however, significant heterogeneity remained in the VSZ group for the impulsive/cognitive control tasks (impulsive: I2 = 74.0%, Q = 11.53, p = 0.009) although there was no longer statistically significant heterogeneity in tasks assessing other aspects of executive function, but was present at a trend level (non-impulsive: I2 = 46.8%, Q = 11.3, p = 0.080).
There was no evidence of publication bias as confirmed using Egger’s and Begg’s tests. This was the case for all domains including IQ (Egger’s p = 0.64, Begg’s p = 0.48), executive function (Egger’s p = 0.99, Begg’s p = 0.71) and memory (Egger’s p = 0.50, Begg’s p = 0.90).
VSZ versus PD
Eight studies directly compared the cognitive profiles of VSZ and PD (Table 2). Although not every study compared with an ASPD group specifically, these studies reported on a VSZ group, thus they were suitable for inclusion based on the stated criteria. However, among the PD groups reported here, a large proportion of ASPD participants would be expected given that most of the studies were conducted in high-secure forensic hospitals (Hill et al., 1997; Murphy, 2003, 2011) where ASPD is the most common PD (Blackburn et al., 2003), or in a psychopathy sample (Kiehl et al., 2000) which has been conceptualised as a severe variant of ASPD (Coid and Ullrich, 2010).
Cognitive functioning in violent individuals with schizophrenia (VSZ) compared to non-violent individuals with schizophrenia (NVSZ).
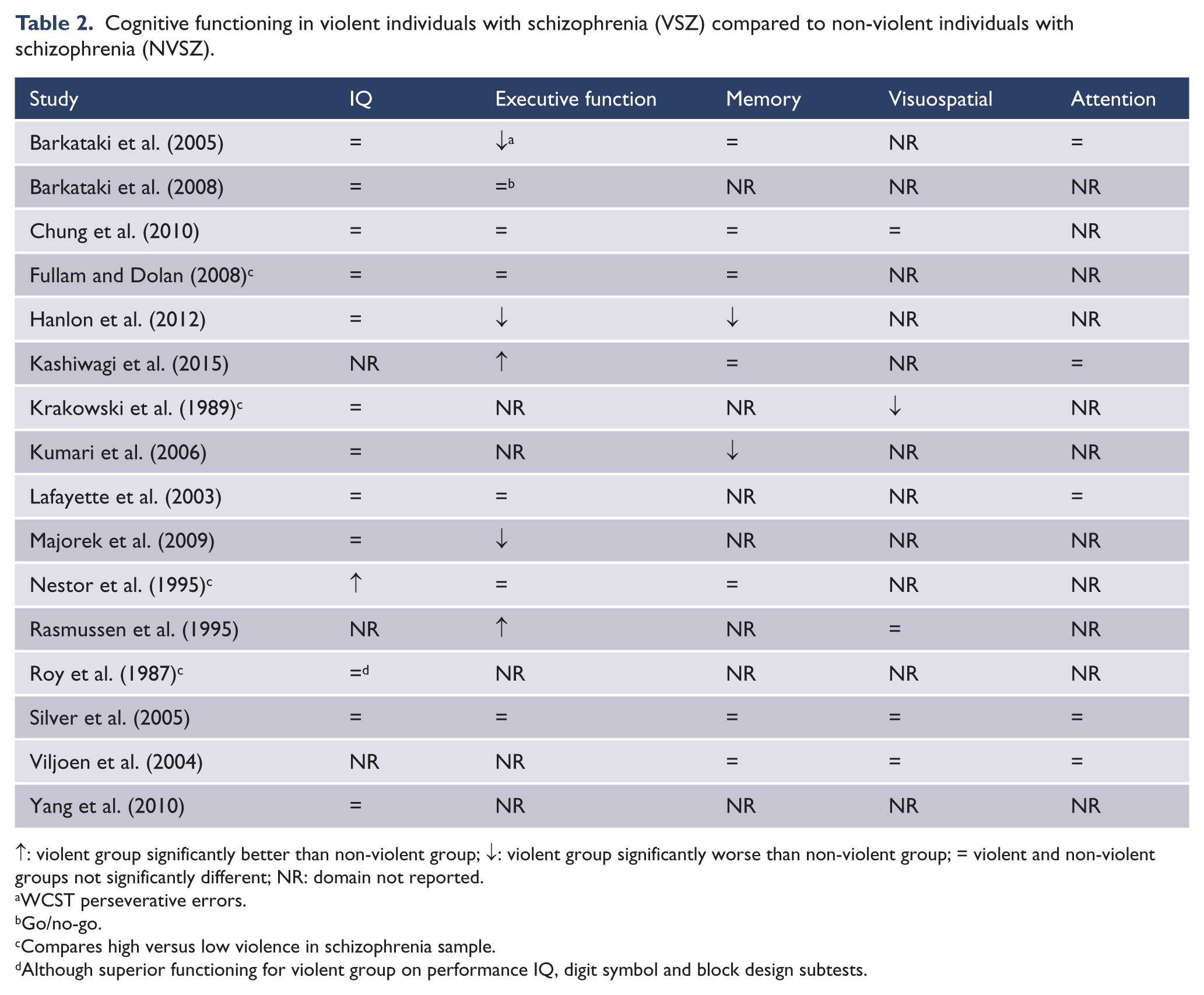
↑: violent group significantly better than non-violent group; ↓: violent group significantly worse than non-violent group; = violent and non-violent groups not significantly different; NR: domain not reported.
WCST perseverative errors.
Go/no-go.
Compares high versus low violence in schizophrenia sample.
Although superior functioning for violent group on performance IQ, digit symbol and block design subtests.
Consistent with the meta-analytic investigation, no studies found better performance in the VSZ group for any domain, and all found equivalent or impaired performance compared to a PD group. The IQ findings were equivocal, with some studies finding equal and some lower IQ in the VSZ group compared to PD, yet this is somewhat complicated by overlapping samples. However, it is notable that one study that found no difference overall (Nijman et al., 2003) did find a relative strength in verbal IQ for the schizophrenia spectrum group, whereas the non-schizophrenia group (largely cluster B PD) had higher performance IQ. Results were also equivocal in the executive function domain, mirroring the high heterogeneity observed in the meta-analysis for this type of task. Similarly, the relative weakness of the VSZ group on memory tasks is also reflected, with all studies finding poorer performance in VSZ relative to PD.
Schizophrenia: with (VSZ) versus without violence (NVSZ)
In all, 16 studies examined the cognitive profiles of VSZ, relative to NVSZ, individuals. As summarised in Table 3, there is clear evidence to suggest that VSZ are at least as impaired as NVSZ individuals across a range of neuropsychological domains. Mirroring the high heterogeneity of effect sizes in the executive function domain observed in the meta-analysis, studies comparing executive function between VSZ and NVSZ groups are mixed in their findings, making a consensus position difficult to reach.
Cognitive functioning in violent individuals with schizophrenia (VSZ) compared to violent individuals with personality disorder (PD).
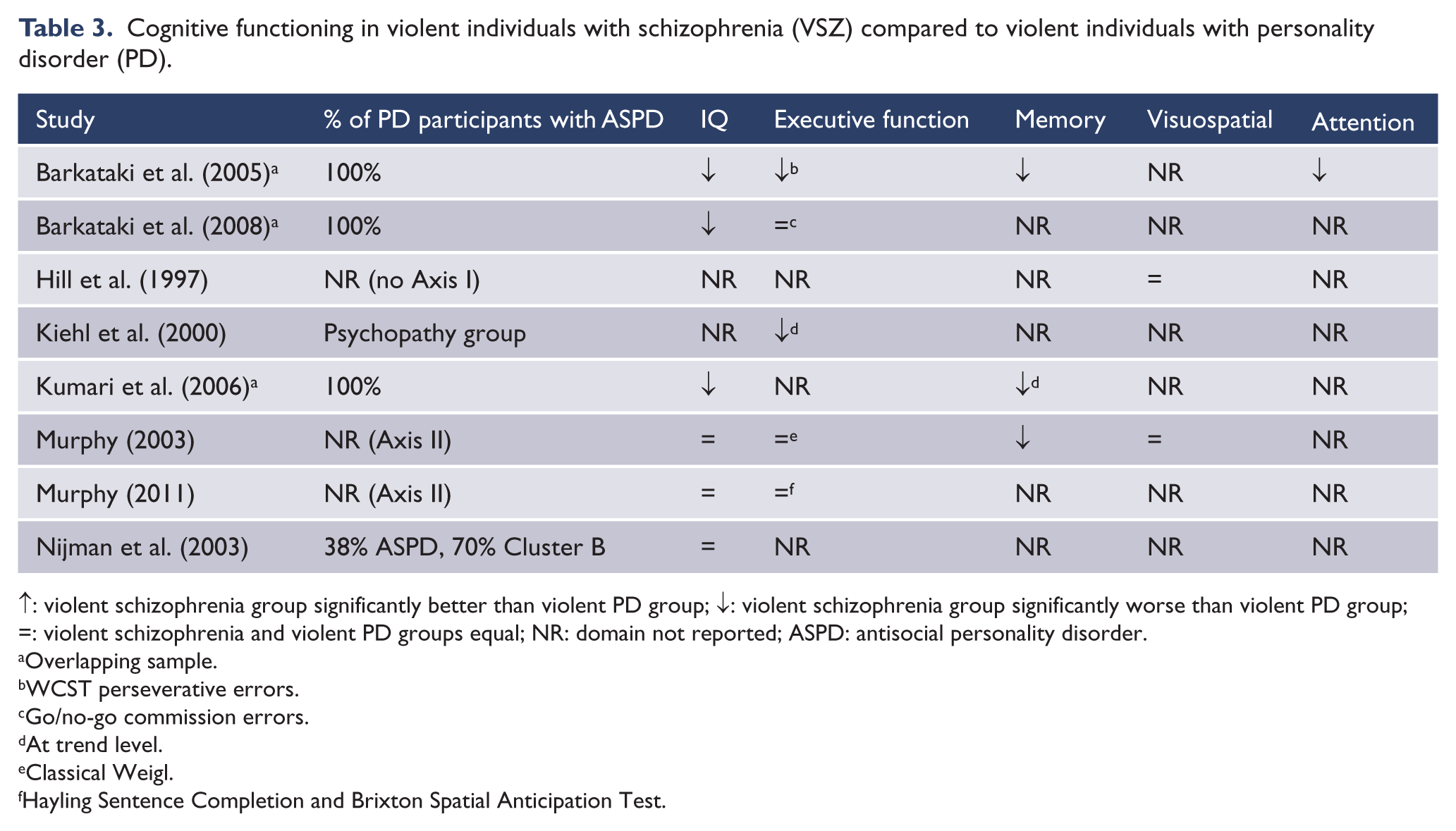
↑: violent schizophrenia group significantly better than violent PD group; ↓: violent schizophrenia group significantly worse than violent PD group; =: violent schizophrenia and violent PD groups equal; NR: domain not reported; ASPD: antisocial personality disorder.
Overlapping sample.
WCST perseverative errors.
Go/no-go commission errors.
At trend level.
Classical Weigl.
Hayling Sentence Completion and Brixton Spatial Anticipation Test.
One study not included in Table 3, due to the results not being reported by cognitive domain, is an early study in aggressive and non-aggressive men with schizophrenia (Adams et al., 1990) who were classified as cognitively ‘impaired’ or not ‘impaired’. Impaired status was associated with ‘severe’ community violence, whereas only one ‘moderately’ violent individual was impaired. Thus, this study supports greater cognitive deficit in more violent groups and also highlights that the severity of violence may be a factor to consider when comparing groups.
ASPD versus healthy offenders
Three studies provide data on cognitive abilities in offenders with ASPD compared with offenders without (Domes et al., 2013; Riser and Kosson, 2013; Yang et al., 2010). Two studies indicate that these groups do not differ on IQ (Domes et al., 2013; Yang et al., 2010). Riser et al. (2013) found cognitive deficits in tasks placing demands on left-hemisphere attention, motor or perceptual demands in individuals with ASPD plus psychopathy, but not in individuals with ASPD alone or non-ASPD offenders.
Comorbid VSZ and ASPD
Only three studies (Hill et al., 1997; Moran and Hodgins, 2004; Tang et al., 2016) provide specific data on comorbid VSZ and ASPD groups. Hill et al. (1997) report the visual reproduction task on the Wechsler Memory Scales in a sample of men detained in high-secure hospital. When those with mental illness were stratified into those with and without ASPD, it was shown that those with comorbid ASPD were significantly more likely to make elaborative errors in the recall of images (i.e. elaborate on the designs; add extra information). In contrast, those without ASPD were more likely to make reduction errors (i.e. simplifying or removing information from designs). Moran and Hodgins (2004) report that violent men with both schizophrenia and ASPD tend to have poorer verbal IQ compared to those with schizophrenia alone (a finding which approached statistical significance), although there were no discernible differences in performance or full-scale IQ.
Tang et al. (2016) found that relative to a non-antisocial schizophrenia group, a group of individuals with schizophrenia and comorbid ASPD performed more poorly on the WCST. This contrasts another study (Lapierre et al., 1995) which provides less specific data, although trends can be inferred. In a sample of schizophrenia outpatients, 42% of whom also had ASPD, the trend for the group was that the number of previous violent incidents was positively correlated with WCST and verbal fluency performance, both sensitive to executive function. This could tentatively suggest that VSZ individuals with ASPD are cognitively less impaired than those with schizophrenia alone. However, this contrasts more specific data (i.e. Moran and Hodgins, 2004; Tang et al., 2016).
Emotion recognition, ToM and experience of emotion in violent individuals
VSZ versus NVSZ and healthy controls
FAR
Five studies examined FAR in VSZ (Antonius et al., 2013; Demirbuga et al., 2013; Frommann et al., 2013; Silver et al., 2005; Wolfkuhler et al., 2012); see Table 4 for summary. The studies that compared VSZ with healthy controls (Silver et al., 2005; Wolfkuhler et al., 2012) support an emotion recognition deficit, as is seen generally in the schizophrenia literature (Trémeau, 2006).
Facial affect recognition in violent individuals with schizophrenia (VSZ) compared to violent individuals with personality disorder (PD) and/or healthy controls.
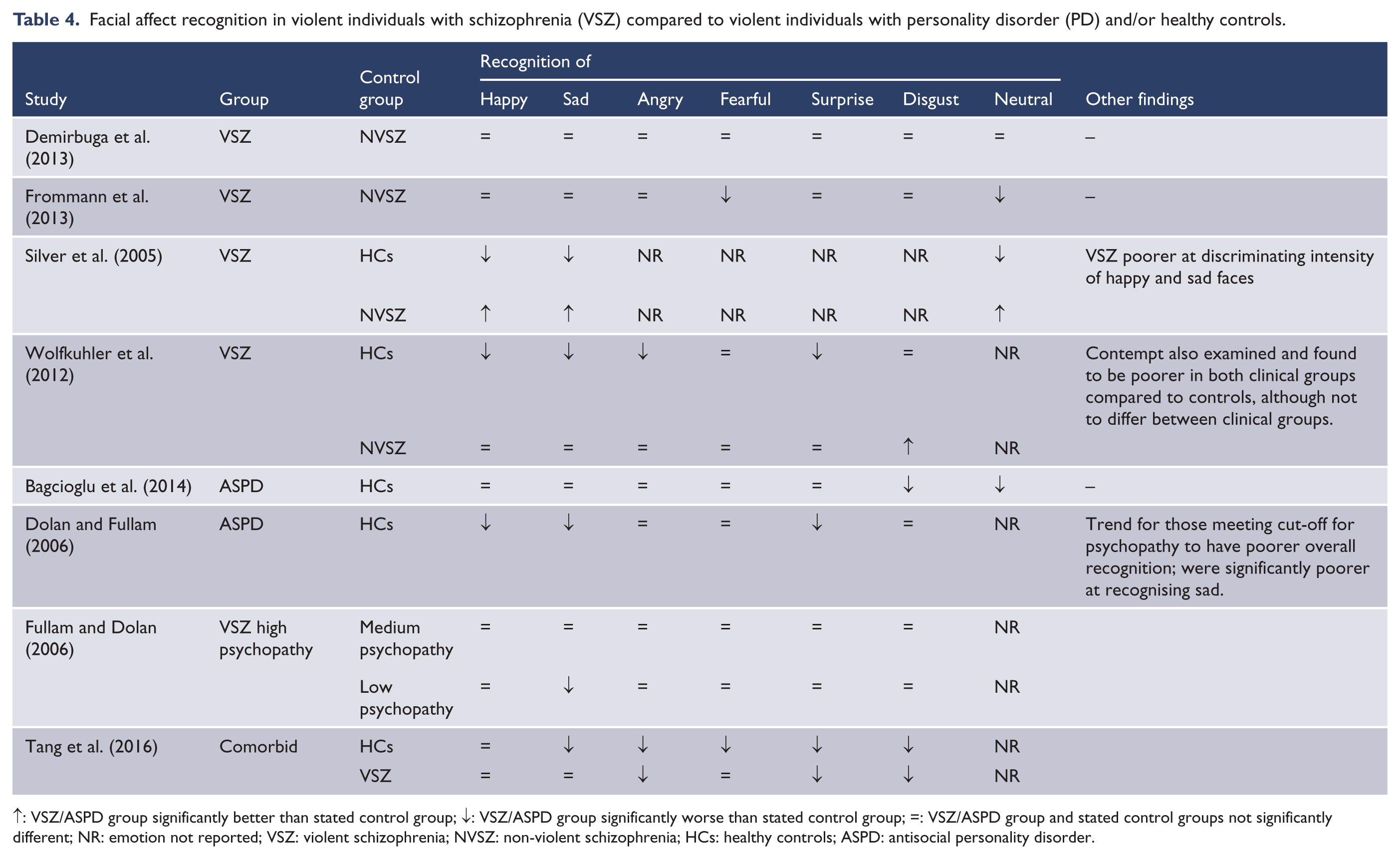
↑: VSZ/ASPD group significantly better than stated control group; ↓: VSZ/ASPD group significantly worse than stated control group; =: VSZ/ASPD group and stated control groups not significantly different; NR: emotion not reported; VSZ: violent schizophrenia; NVSZ: non-violent schizophrenia; HCs: healthy controls; ASPD: antisocial personality disorder.
Comparing VSZ and NVSZ, the differential seems to arise on tasks comparing more complex aspects of FAR: Silver et al. (2005) found that their VSZ group was poorer at discriminating between the intensity of emotion shown by two faces. When participants viewed neutral faces which were altered to show slight emotional expressions and asked to rate the perceived dominance, those with low self-reported aggression rated neutral faces showing micro-expressions of fear as less dominant; however, this effect was not observed in the high aggression group (Antonius et al., 2013). These findings suggest that subtle facial cues are not being identified by VSZ groups, which may impede their ability to appropriately respond.
ToM
Five studies (Abu-Akel, 2004; Arborelius et al., 2013; Majorek et al., 2009; Murphy, 1998, 2006) examined ToM in VSZ, with three studies comparing to different clinical groups. Arborelius et al. (2013) found that VSZ and a violent autism spectrum disorder (ASD) group were less able to attribute appropriate emotions to an individual they viewed in a video-clip and less able to use contextual information to inform these judgements compared to healthy controls. These results are mirrored in two studies carried out in a forensic hospital (Murphy, 1998, 2006) which demonstrate that VSZ individuals have poorer second-order ToM (Murphy, 1998), are less able to interpret emotional information from the eyes and have poorer performance on ToM tasks (Murphy, 2006) compared to a PD group; however, they did not differ from a violent ASD group.
Conversely, Abu-Akel (2004) showed that VSZ individuals were better at second-order ToM tasks and the cognitive component of faux-pas tasks, compared with NVSZ individuals, although they were poorer at recognising faux-pas and empathic inference tasks. In addition, it was shown that ability to infer a cognitive state in others and ability to recognise faux-pas significantly predicted the likelihood of a history of violence. However, others have noted that this study was confounded by a lack of control for cognitive variables and psychopathology, and so conducted an investigation incorporating these factors (Majorek et al., 2009). Comparing forensic and non-forensic individuals with schizophrenia, they found that ToM ability did not differ significantly, although in the forensic group the impairment was driven by the cognitive and excitement (i.e. tension, hostility, poor impulse control) factors of the Positive and Negative Syndrome Scale (Kay et al., 1987), whereas in the non-forensic group it was driven by the cognitive and negative component (flattened affect, etc.). This suggests that similar behavioural outcomes may be driven by diverse underlying deficits.
Experiential emotion
Two studies explored the experience of emotion in VSZ. One study asked participants to complete a go/no-go-type task, in which they were asked to respond to emotionally valenced images as quickly as possible unless it was a repeat of the previous picture (De Sanctis et al., 2013). Using event-related potentials, the authors demonstrated early sensory processing deficits in individuals with schizophrenia (both violent and non-violent) in response to negatively valenced images compared to healthy controls, and this effect was particularly marked in VSZ. The authors suggest that their findings may indicate problems with correctly judging the emotional context of a situation due to poor early processing, possibly resulting in inappropriate responses that could include violence. They also suggest that the lack of modulation when comparing neutral and negative images may potentially reflect a tendency to attribute negative emotion to neutral situations.
Another study examined the experience of threat (Kumari et al., 2009). Participants were told that they were sometimes at risk of receiving an electric shock, while were safe at other points. In reality, no shocks were administered. After completing the task, participants were asked to rate (visual analogue scale; safe to fearful) how they had felt during both conditions; although non-significantly different, the results showed that VSZ patients had the highest levels of fear during both conditions compared to NVSZ and controls. In addition, VSZ believed it to be more likely that the shock was going to be administered in the shock condition than healthy controls at a trend level. The results support an enhanced experience of anticipatory fear in VSZ, which may mediate violence via inappropriate attribution of threat to non-threatening situations.
ASPD versus healthy controls
FAR
Five studies examined FAR in violent individuals with ASPD (Bagcioglu et al., 2014; Dolan and Fullam, 2004, 2006; Schonenberg et al., 2013; Schonenberg and Jusyte, 2014; see Table 4).
Dolan and Fullam (2004) examined the impact of psychopathy; when dividing ASPD individuals into high and low psychopathy, those with low, but not high, psychopathy were poorer at recognising basic and complex emotions shown on a full face compared to healthy controls. When looking specifically at reading emotion from the eyes, low psychopathy scorers were more impaired at recognising basic emotion than healthy controls. In another study examining this effect (Dolan and Fullam, 2006), individuals with dissocial PD were worse than controls at recognising sad, happy and surprised faces, in some cases even at 100% intensity. High psychopathy scorers performed worse than low at recognising sad at a trend level, and total psychopathy score negatively correlated with the correct identification of sad. These studies tend to contradict one another’s findings; in the former, the low psychopathy group is relatively impaired, whereas in the latter impairment is greater in those with high scores.
More contradictive evidence has emerged from studies examining morphed or merged faces. Schonenberg and Jusyte (2014) asked ASPD prisoners to identify the emotion when the stimulus was created from morphing two expressions together, for example, a happy and fearful face. These were combined at different intensities (e.g. 70% fearful and 30% happy). ASPD participants were significantly more likely to identify anger than controls, even at maximal ambiguity (i.e. 50% angry combined with 50% fearful/happy), suggesting a hostile attribution bias. In contrast, an earlier study by the same group (Schonenberg et al., 2013) asked participants to view faces which were animated to change from a neutral expression at 2% intensity increments and to respond as soon as they could recognise the emergent emotion. The ASPD group took significantly longer to recognise angry faces than the controls, which is inconsistent with hostile attribution bias.
ToM
Two studies have investigated ToM in violent ASPD samples. Dolan and Fullam (2004) showed no significant differences between high and low psychopathy ASPD or versus controls, on first order and second order of faux-pas ToM tasks. However, both ASPD groups performed poorly, relative to controls, on the attribution of a mental state and empathic understanding in the faux-pas scenario. Shamay-Tsoory et al. (2010) demonstrated that ASPD individuals were impaired at the second-order, affective ToM (i.e. using information about one person’s mental state to infer a mental state in another).
Experiential emotion
Seven studies examined the experience/salience of emotion in violent ASPD, of which four used lexical tasks. Domes et al. (2013) administered an emotional Stroop task comprising violent, negative and neutral words. Prisoners with ASPD had a significant attentional bias towards violent and negative words compared to neutral words in a congruent condition, relative to healthy controls. However, they did not significantly differ from non-ASPD prisoners. In another lexical task, prisoners with ASPD (with/without psychopathy) and non-ASPD prisoners were asked to categorise strings of letters as words or non-words (Kosson et al., 2006). Offenders with ASPD and psychopathy were significantly slower at classifying affective words than neutral words (i.e. less affective facilitation) when compared to offenders with ASPD alone, or offenders with no ASPD (who did not differ from one another). In addition, the degree of affective facilitation in the ASPD plus psychopathy group was significantly negatively correlated with the number of charges for non-violent offences, adding weight to the ecological validity of the findings.
Another study utilised an anger induction interview followed by two implicit association tests: one assessing ‘self’-‘anger’ associations and one assessing ‘aggressor’ (i.e. an individual the person had had an argument with)–‘swearword’ associations (Lobbestael et al., 2009). Following anger induction, ASPD individuals reported similar levels of anger to healthy controls and other PD participants, but demonstrated decreased heart-rate and increased self-anger associations compared to other groups. These observations were independent of psychopathy score. The authors posit that this demonstrates an anger response style characterised by physiological under-arousal yet cognitive over-arousal, perhaps reflecting an ability to engage in controlled, predatory-type violence.
Verona et al. (2012) examined the interaction between cognition and emotion in ASPD alone, ASPD plus psychopathy and offenders with neither disorder. Participants were asked to complete a linguistic go/no-go task using neutral and negative words as stimuli. Although the reaction times and number of errors did not differ between groups, an effect was found from the event-related potential data. The ASPD-alone group showed enhanced P3 modulation to negative words regardless of whether the word was in the go or no-go condition. This suggests that individuals with ASPD alone fail to ignore emotional material when engaging in inhibitory control, which may give insight into their violent behaviours during episodes of high emotionality. However, the lack of a behavioural effect somewhat weakens this finding. The results regarding psychopathy are consistent with another study examining cognition–emotion interaction (Muller et al., 2008), in which a negative emotion induction paradigm did not affect performance on a cognitive task in those with ASPD who met criteria for psychopathy, but adversely affected performance in healthy controls.
One study examined emotion processing using an affective startle paradigm in ASPD (Loomans et al., 2015), comparing ASPD plus psychopathy with ASPD alone, forensic hospital employees and community controls. It was shown that the typical enhanced startle response to aversive images was present in the community controls and ASPD-alone group, but not in the ASPD plus psychopathy or forensic hospital employee group. This suggests a key role for psychopathy in mediating emotion processing within this population. It may be that forensic hospital employees have built up a level of resilience to aversive experiences or have fearless personality traits which predispose them to a job in which it is necessary to take on risk. The aforementioned study, examining the experience of anticipatory fear, specifically threat of electric shock (Kumari et al., 2009), showed that violent ASPD patients taking part reported the lowest levels of fear under the threat of shock compared to healthy controls, non-violent men with schizophrenia and VSZ. They also reported the lowest anticipation of shock. Thus, while Kumari et al. (2009) support an experiential fear deficit in ASPD, Loomans et al. (2015) indicate that this may be fully mediated by psychopathic traits.
Comorbid VSZ and ASPD
FAR
Only one study specifically addressed FAR in a comorbid schizophrenia and ASPD group (Tang et al., 2016). The comorbid group showed poorer performance, relative to healthy controls, at recognising sad, angry, fearful, surprised and disgusted faces and was poorer at recognising anger, surprise and disgust compared to individuals with schizophrenia alone. One further study provided data examining the effect of antisocial personality traits on affect recognition in VSZ (Fullam and Dolan, 2006). The results showed that VSZ with high psychopathy scores were impaired in comparison to the low or medium scorers at recognising sad faces, an effect which was mediated mainly by factor 2 (antisocial) traits. Taken together, these studies suggest that antisocial personality traits further impair FAR in VSZ.
ToM and experiential emotion
No studies are identified.
An overview of all results is presented in Figure 5.
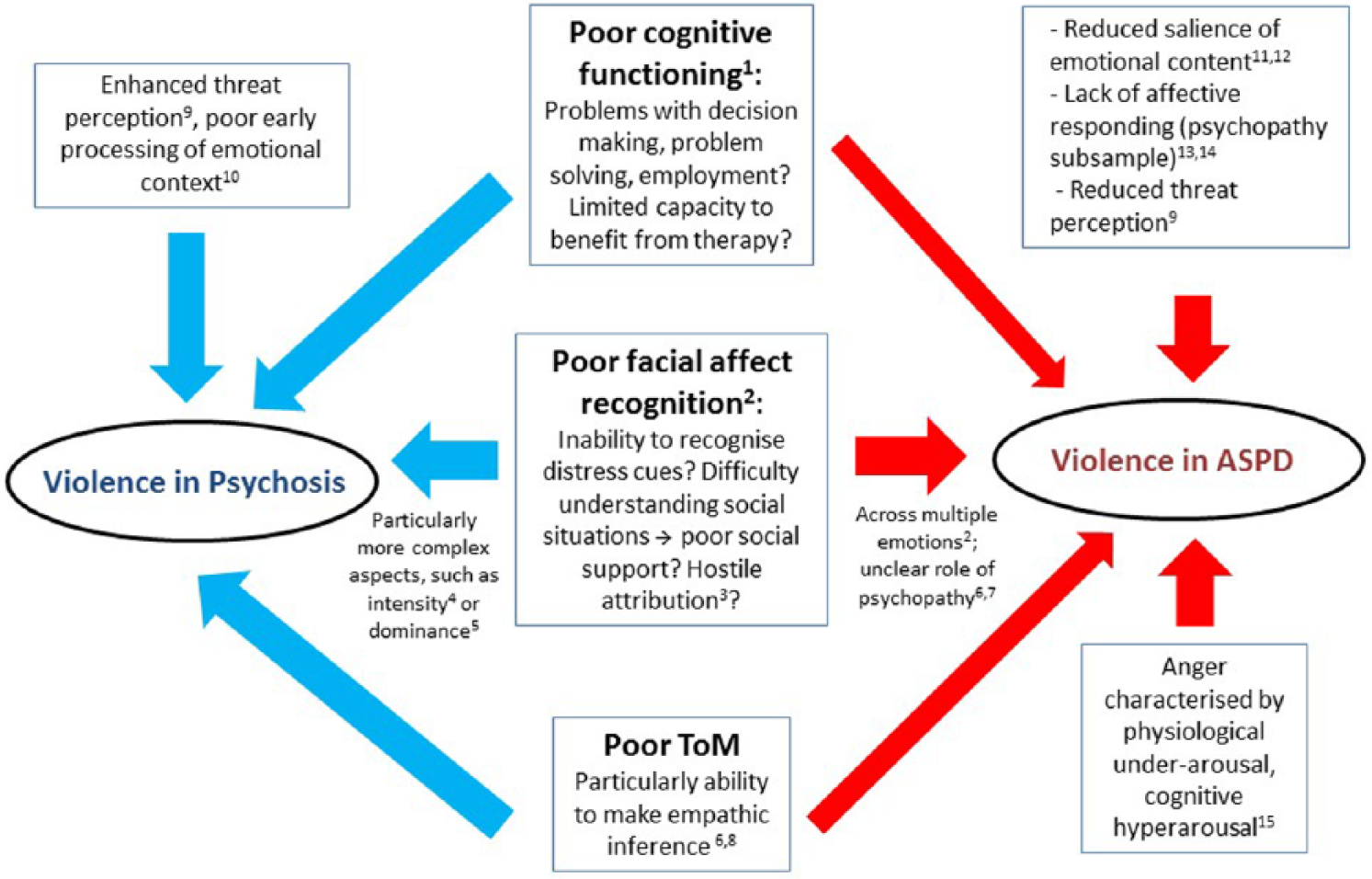
Overview of review findings with potential links to violent behaviour.
Discussion
Neuropsychological profiles
The results of the meta-analyses indicate that both groups perform poorly across all investigated cognitive domains compared to healthy controls, although the effect sizes were consistently larger in VSZ indicating more severe problems in this group. This is largely consistent with the results of the few studies which directly compare VSZ and PD, which show equivalent/worse performance in the VSZ group relative to PD.
Poor performance across domains may have a variety of explanations. A number of the IQ tests included in the meta-analysis were reading-based paradigms (see Table 1) which are sensitive to the educational level (Crawford et al., 1988). Educational attainment is likely to be lower in both clinical groups relative to healthy groups; individuals with comorbid ASPD and schizophrenia are less likely to have completed high school than individuals with schizophrenia alone (Moran and Hodgins, 2004). Thus, these results may be reflective of common developmental experiences as opposed to diagnosis-specific; indeed, both studies comparing offenders with and without ASPD found no difference in IQ (Domes et al., 2013; Yang et al., 2010). The results are complicated by the inclusion of tests purporting to assess both ‘current’ and ‘premorbid’ IQ, although not possible in this analysis due to too little variety in tests.
Both groups showed poorer performance on memory tasks compared to controls. Memory deficits were observed to be specifically present among ‘antisocial’ individuals with schizophrenia, relative to ‘non-antisocial’ schizophrenia, in a previous meta-analysis, and were suggested to reflect a temporo-limbic contribution to violent behaviour, as opposed to frontal circuits (Schug and Raine, 2009). This is consistent with the results of the current analysis where both groups have exhibited violent behaviour, and thus problems with memory may represent a transdiagnostic symptom associated with violence. The hippocampus (a key structure in memory function) has been implicated in violent and antisocial behaviour (Dolan, 2010; Soderstrom et al., 2002) and is also involved in mediating prepulse inhibition, a measure of sensorimotor gating and automatic inhibition, deficits of which have been linked to violence severity (Kumari et al., 2005). Thus, problems with memory may be reflective of underlying temporo-limbic anomalies which also overlap with violence, and this may be more relevant to violence among VSZ.
Significant deficits in executive function were observed across groups, and the effect size confidence intervals marginally overlapped suggesting that they may not differ from each other. This assertion is somewhat supported by a majority of the studies directly comparing PD and VSZ, which found equivalent performance in executive function (see Table 2). However, it is reasonable to conclude that the extant literature cannot provide a consensus as to whether VSZ and ASPD differ on their executive functioning, although it is clear that both diagnoses confer a risk of poorer performance compared to healthy groups. There also appears to be no difference between these groups in contribution of impulsivity, suggesting that both task types are difficult for these diagnostic groups, and impulsivity could be relevant to violence in both (Hoptman, 2015; Schiffer et al., 2014; Volavka and Citrome, 2008).
Significant heterogeneity was observed among executive function effect sizes in the VSZ group. This could be hypothesised to be due to the unspecific definition of ‘executive function’, which is acknowledged in the literature to be an ‘umbrella term’ (Chan et al., 2008); however, this argument is weakened given the lack of significant heterogeneity in the ASPD group. Furthermore, there was a greater diversity of executive function tests included in the meta-analysis from the ASPD group compared to VSZ (15 vs 13, respectively), which arguably would have produced more, as opposed to less, heterogeneity. Another explanation is that VSZ is often heterogeneous in presentation with diverse aetiology (Volavka and Citrome, 2008), and it is likely that these differing subgroups have distinct characteristics such as PD comorbidity. This explanation is strengthened when looking at the number of studies which did not control for PD among their psychosis groups (11 studies did so in this review; four of which were from the same sample), whereas almost every study examining ASPD excluded Axis I diagnoses, making this a much more accurately characterised group.
The current evidence base is lacking data focussing on comorbid presentations of schizophrenia and ASPD. This is common in clinical practice (approximately 45% of those with primary mental illness meet criteria for ASPD in high security; Blackburn et al., 2003) and is a risk factor for violence (odds ratio [OR] = 2.1; Witt et al., 2013). This review highlights cognitive problems among both diagnostic groups, so it is currently unclear how having both diagnoses would affect cognition; is there a ‘double dose’ of problems? The limited data available suggest that this group does differ compared to either disorder alone (Hill et al., 1997; Moran and Hodgins, 2004; Tang et al., 2016), and functional magnetic resonance imaging (MRI) evidence also supports the notion of a distinct group; violent men with diagnoses of schizophrenia, ASPD and substance use disorder showed less activity in frontal regions while completing a go/no-go task compared to those with VSZ alone and healthy controls (Joyal et al., 2007). Thus, there may be specific characteristics relevant to this comorbid group.
The observed deficits across all domains in both groups suggest that cognitive function could represent a potential transdiagnostic therapeutic target which may have an effect on violence. Cognitive remediation has a good evidence base for improving cognitive skills in schizophrenia (Wykes et al., 2011), and a recent trial of cognitive remediation in forensic mental health services for individuals with VSZ showed positive effects on both neurocognition and reduction of violence (Ahmed et al., 2015), and trials of this kind in individuals with ASPD are warranted. Effective treatments for ASPD are still lacking (Rampling et al., 2016), although a cognitive skills programme (R&R2) which incorporates a neurocognitive module has shown beneficial results in a small sample of high-risk PD offenders (Young et al., 2013), further highlighting cognition as a promising target for intervention.
Emotion processing profiles
FAR
Problems in FAR appear common to both groups, at least in comparison to healthy controls. Among the VSZ group, there appears to be clear evidence of a deficit across the majority of emotions examined compared to healthy controls (Silver et al., 2005; Wolfkuhler et al., 2012). The picture comparing VSZ to NVSZ is less clear (see Table 4). However, the VSZ group appears more impaired, relative to NVSZ, on tasks assessing more complex aspects of affect recognition, for example, in discriminating the intensity of displayed emotion (Silver et al., 2005) or attributing dominance to faces (Antonius et al., 2013). These skills are likely key to translating emotion into appropriate behavioural actions, and thus may represent an area for potential therapeutic gains.
Among studies focussing on ASPD, areas of weakness compared to healthy controls have also been noted, although a consensus on the specificity of these has yet to be reached; one study suggested deficits in disgust and neutral (Bagcioglu et al., 2014), whereas another highlighted happiness, sadness and surprise as problematic (Dolan and Fullam, 2006). A meta-analysis of studies examining facial affect perception in psychopathy identified the recognition of a number of emotions to be impaired, including happiness, sadness, fear and surprise (Dawel et al., 2012), and thus it may be that antisocial traits confer a pervasive deficit across many emotions. The studies reviewed here provide contradictory evidence regarding psychopathy in ASPD, with a relative deficit reported in both high (Dolan and Fullam, 2006) and low scorers (Dolan and Fullam, 2004).
It may be that increasing levels of psychopathic traits impede emotion processing up to a point, but that at high levels of psychopathy there is no deficit. This hypothesis is supported by a study which found that metacognitive ability (including attributing mental state to others) was negatively associated with psychopathy score in forensic patients with schizophrenia, until a ‘break point’ score of 24 on the psychopathy checklist, when the relationship reversed and metacognitive score was correlated positively with psychopathy (Abu-Akel et al., 2015). The only domain for which this was not the case was ‘mastery’, which relates to using information about self or others to plan and implement action. Thus, although the ability to understand and/or recognise emotion may be present, using this information to inform behaviour may be the crucial missing link and could represent an area for intervention among high psychopathy scorers.
Both studies examining the role of antisocial personality traits among individuals with schizophrenia (one assessed via psychopathy checklist score, one assessed via a formal ASPD diagnosis) found such traits to contribute to poorer facial affect recognition, relative to non-antisocial/less antisocial schizophrenia groups (Fullam and Dolan, 2006; Tang et al., 2016). As with the neuropsychological findings, this suggests that the comorbid presentation of schizophrenia and ASPD has distinct characteristics, although comparison of this group with a purely ASPD group is still required before firm conclusions can be drawn. Poorer performance is consistent with a ‘double-dose’ explanation of the deficit, although this should be more thoroughly explored in future research.
It has been suggested that FAR problems among individuals with schizophrenia are related to a more general underlying cognitive deficit (Ventura et al., 2013), and given the reported cognitive deficits observed in both groups in the current meta-analyses, this may be an important confounding factor. However, these two constructs may impact differentially on outcome. For example, one study of forensic inpatients with schizophrenia found that social cognitive measures were better than neurocognitive at predicting future violence (O’Reilly et al., 2015). Thus, it is encouraging that initial studies examining the efficacy of social cognition training in forensic populations have shown positive results with respect to improving facial affect recognition (Combs et al., 2007; Taylor et al., 2015).
ToM
VSZ individuals show ToM deficits compared to those with PD or healthy controls, but do not differ from ASD samples (Arborelius et al., 2013; Murphy, 1998; Murphy, 2006). Compared to NVSZ, VSZ groups may show some areas of superiority (second-order ToM, faux-pas cognitive inference) and other areas of deficit (Abu-Akel, 2004), although this has not been robustly demonstrated and it may be that heterogeneous symptomatology profiles drive these differences (Majorek et al., 2009). ToM deficits also appear evident in ASPD groups, although not all investigated areas were impaired (Dolan and Fullam, 2004). One area which appeared to be limited across both groups was the ability to demonstrate empathic inference in faux-pas scenarios (Abu-Akel, 2004; Dolan and Fullam, 2004), although having no difficulty in recognising it. This suggests that although there may not be a gross deficit in cognitively understanding a situation, it is the appropriate behavioural/emotional response that is lacking across both groups. However, this is based on a very small number of studies and further research is required in this area.
Experiential emotion
Within this domain, there has been more focussed research in ASPD compared to VSZ. The finding of high anticipatory fear in VSZ is consistent with threat control-override theories of violence in psychosis (Link et al., 1998), and particularly the enhanced experience of threat has shown to be more related to violence than control-override symptoms, and also linked to the severity of violent acts (Stompe et al., 2004). Most of the experiential emotion deficits observed in ASPD appear to be mediated by psychopathy (e.g. Kosson et al., 2006; Loomans et al., 2015; Muller et al., 2008). This highlights the importance of quantifying such traits when formulating risk, as lack of affective experience is likely relevant to violence but may not be present among those with ASPD alone. This group may have different characteristics (i.e. cognitive hyperarousal) which require specific consideration, and clarification of ASPD specific traits should be addressed in future research.
Overview – links to violence
Poor cognition could enhance the risk of violent behaviour via poorer decision-making or problem-solving abilities, for example, difficulty generating prosocial alternatives for emergent problems, or confer a higher risk for related problems such as unemployment (Dickerson et al., 2007) which may foster or perpetuate offending/reoffending (Appleby et al., 2015). In addition, poor cognitive skills may mean that individuals are less able to participate in, or benefit from, psychological therapy (Granholm et al., 2008) which may be offered in order to reduce violent behaviours/manage symptoms. FAR difficulties could result in poor understanding of social situations or the intentions of others. It may also impair the detection of distress cues in others, thereby removing inhibition that such cues typically evoke against violence (Blair et al., 1997). Such explanations are consistent with the experiential emotion literature within the ASPD group which suggests that especially among those with high levels of psychopathic traits, there is a lack of affective experience, diminished salience of emotional content and reduced threat perception. In contrast, in psychosis, violence may emerge from more of a defensive position (Levi et al., 2010) consistent with enhanced threat perception and poor affective judgement/early emotional processing. These cognitive and emotion processing deficits may combine and contribute additively towards the emergence of violence, or indeed may represent one latent construct as evidence has suggested social and neurocognition may be interrelated (Ventura et al., 2013). These may be mediated via common developmental experiences. For example, childhood adversity (and especially abuse) has been linked with poor ToM in adults (Germine et al., 2015), in addition to poor cognitive functioning in those with relative to those without early life stressors (Gould et al., 2012).
Limitations and recommendation for future research
First, the meta-analyses report summary scores created by averaging a number of outcome variables for the same measure to create a score for that measure (i.e. WCST; ToL) and then averaging across tests to create a domain score for each included study (i.e. executive function score, memory score). Although this inevitably means some level of detail is lost, it was deemed the most appropriate approach to minimise researcher bias. In addition, it is unlikely that the different tests reported across studies are measuring the same exact underlying construct, and thus although some similarity can be assumed, it is difficult to pinpoint precise cognitive characteristics. Future studies should aim to be guided by clear conceptual frameworks and use standardised neurocognitive test batteries (e.g. the MATRICS consensus cognitive battery) wherever feasible to ensure comparability of results across samples. In terms of particular cognitive domains, future studies should pay attention to measures of ‘current’ as well as ‘premorbid’ IQ, memory, executive function and social cognition. Furthermore, as noted earlier in section ‘Methods’, we were unable to incorporate data on attention due to a lack of available studies, and attention has an important relationship with memory (encoding processes, etc.). Attention may be a particularly relevant concept for these clinical groups given the deleterious effect psychological trauma can have on attentional processes (Kimble et al., 2010) and should be incorporated into future studies of this kind.
Second, the definition of violence across samples varied between the reviewed studies. Although efforts were made to ensure the sample was characterised by violent behaviours, studies operationalise this differently and sometimes assumptions had to be made, i.e., that being a prisoner implied a history of violent behaviour. It is acknowledged that this introduces variability into the results, and the reader is directed to Supplementary Table 1 to view how violence/antisociality in each study was operationalised. The field would benefit from a more uniformed conceptualisation of violence/aggression to address these issues (Harris et al., 2013).
Third, the diagnostic label of ASPD is contentious and some have argued that it relies too heavily on behavioural constructs (Ogloff, 2006). This raises the possibility, therefore, that aetiological factors resulting in antisocial behaviour are overlooked in favour of the behavioural phenotype, for example, substance misuse, early childhood trauma/adversity, poor early attachments, which may also be contributing to specific cognitive and emotion processing deficits. Factors such as these are important to consider in future investigations of neuropsychological functioning in these groups, as evidence to date has been limited.
Finally, this review could not address the stability of cognitive and emotion processing characteristics over time or examine them in relation to outcome within and across diagnostic categories due to lack of robust data on this topic. Future studies should aim to fill this gap.
Conclusion
VSZ and ASPD are both characterised by deficits in IQ, memory and executive function, with larger deficits observed in VSZ. Both disorders are characterised by impaired FAR, and psychopathy appears an important consideration in experiential emotion. The characteristics of those with both VSZ and ASPD remain largely unknown and should be investigated further, as initial studies suggest a distinct subgroup.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ottilie Sedgwick received funding support from the National Institute for Health Research (NIHR) Mental Health Biomedical Research Centre at South London and Maudsley National Health Service (NHS) Foundation Trust and King’s College London. Veena Kumari was part funded by the Biomedical Research Centre for Mental Health at the Institute of Psychiatry, Psychology and Neuroscience King’s College London, and the South London and Maudsley NHS Foundation Trust, UK. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.