
Abstract
Psychopathy has traditionally been characterised as a disorder primarily of personality (particularly affective deficits) and, to a lesser extent, behaviour. Although often used interchangeably, the diagnostic constructs of psychopathy, antisocial personality disorder, and dissocial personality disorder are distinct. In this article, the relevant historical and contemporary literature concerning psychopathy is briefly reviewed. The diagnostic criteria for psychopathy, antisocial personality disorder, and dissocial personality disorder are compared. Consideration is given to the assessment, prevalence, and implications of psychopathy for violence risk and treatment efficacy. The DSM-IV-TR criteria for antisocial personality disorder, in particular, are largely behaviourally based. The ICD criteria for dissocial personality disorder, while paying more attention to affective deficits, also do not represent the broad personality and behavioural components of psychopathy. Since 1980, a great deal of research on these disorders has been conducted, using the Hare Psychopathy Checklist, Revised (PCL-R). The PCL-R assesses both personality (interpersonal and affective) and behavioural (lifestyle and antisocial) deficits. As such, the research and clinical implications of psychopathy, as operationalised by the PCL-R, cannot be readily extrapolated to the diagnoses of antisocial personality disorder and dissocial personality disorder. As currently construed, the diagnosis of antisocial personality disorder grossly over-identifies people, particularly those with offence histories, as meeting the criteria for the diagnosis. For example, research shows that between 50% and 80% of prisoners meet the criteria for a diagnosis of antisocial personality disorder, yet only approximately 15% of prisoners would be expected to be psychopathic, as assessed by the PCL-R. As such, the characteristics and research findings drawn from the psychopathy research may not be relevant for those with antisocial or dissocial personality disorder.
Australian and New Zealand Journal of Psychiatry 2006; 40:519–528
Each generation of mental health professionals has to discover for itself the importance of personality disorder [1].
Sadly, and improperly, the place of personality and personality disorder in contemporary mental health has been either ignored wholly or employed as yet another reason to exclude patients from the services offered by increasingly over-taxed public mental-health systems. Although these comments pertain to personality disorders generally, the focus here will be on ‘psychopathy’, or as it has been termed in contemporary nosological systems, Antisocial Personality Disorder (Antisocial PD; Diagnostic and Statistical Manual of Mental Disorders [DSM]-IV-TR) or Dissocial Personality Disorder (Dissocial PD; the tenth edition of International Classification of Diseases [ICD-10]).
Little is known about the aetiology of psychopathy and Antisocial PD. Although attention has been paid to the possible biological, social, psychological and environmental factors that lead to psychopathy, no definitive results have been identified. A recent review of structural and functional neuroimaging studies and psychopathy has been conducted [2]. The results show that to date the structural brain differences that have been identified have been few and none has been replicated. By contrast, imaging studies investigating brain function have shown, with some degree of reliability, evidence for dysfunction in the frontal and temporal lobes, and perhaps some other brain structures. The authors caution that the research is difficult to compare and most studies have not been replicated.
Livesley [3] has written that most of the variance that explains psychopathic traits comes from environmental and social influences, but that genotype might explain a relatively small but significant proportion of the variance. Considerable contemporary work has been conducted identifying precursors and developmental traits that may lead to psychopathy [4]. Doubtless, ‘psychopathy is likely the product of complex interactions between biological predispositions and social forces’ [5].
Defining psychopathy and antisocial PD
Millon
Scholars and practitioners alike have debated the merits of conditions such as those characterized by so-called antisocial features for as long as attempts have been made to classify mental disorder. For example, the term ‘manie sans délire’ (i.e. mania without confusion of the mind), which Pinel [9] coined in the 1700s to describe patients whose ‘affective faculties were disordered’ (pp. 155–156), was criticized as early as 1866 for only having use in court [10].
Over the years a number of different labels have been used for the condition that has come to be known as psychopathy (e.g. manie sans délire, moral insanity, moral imbecility, degenerate constitution, congenital delinquency, constitutional inferiority, psychopathic taint, psychopathic personality, psychopathy, and most recently Antisocial PD and Dissocial PD). All of the terms that have been used are pejorative and there is little doubt that each would conjure up very negative images for people. The term with the longest clinical tradition is ‘psychopathy’. As such, it has been the subject of considerable research and scholarly writing. As we shall see below, the contemporary personality disorder ‘Antisocial PD’, while sharing characteristics with psychopathy is much broader and is based more on behavioural traits than on some of the traditional personality characteristics associated with psychopathy.
In 1941, the American psychiatrist Hervey Cleckley described the condition of psychopathy in his now classic book the
Superficial charm and good intelligence.
Absences of delusions and other signs of irrational thinking.
Absence of ‘nervousness’ or psychoneurotic manifestations.
Unreliability.
Untruthfulness and insincerity.
Lack of remorse or shame.
Inadequately motivated antisocial behaviour.
Poor judgement and failure to learn from experience.
Pathological egocentricity and incapacity for love.
General poverty in major affective reactions.
Specific loss of insight.
Unresponsiveness in general interpersonal relations.
Fantastic and uninviting behaviour, with drink and sometimes without.
Suicide rarely carried out.
Sex life impersonal, trivial and poorly integrated.
Failure to follow any life plan.
In the precursor to the DSM, the American Psychiatric Association published a collection of psychiatric illnesses in 1932. At that time, the term ‘Psychopathic Personalities’ was used. In the first edition of the DSM, published in 1952, ‘Sociopathic Personality Disorders’ (Subcategory: Antisocial Reaction) appeared. By 1968, with the second edition of the DSM [11], the disorder was labelled ‘Personality Disorder, Antisocial Type’. At that time, those with the disorder were described as follows:
basically unsocialized and whose behaviour patterns bring them repeatedly into conflict with society. They are incapable of significant loyalty to individuals, groups or social values. They are grossly selfish, callous, irresponsible, impulsive, J.R.P. OGLOFF 521 © 2006 The Author Journal compilation © 2006 The Royal Australian and New Zealand College of Psychiatrists and unable to feel guilt or to learn from experience or punishment. Frustration tolerance is low. They tend to blame others or offer a plausible rationalization for their behaviour [11].
At the time of the DSM-II, considerable criticism was brought against psychiatry for having diagnoses that were unreliable (i.e. about which psychiatrists could not agree). As a result, rather than employing clinical descriptions for diagnoses, specific criteria were developed. This format remained with the most recent editions of the DSM [12], published in 1994 and 2000 (DSM-IVTR; APA, 2000).
In the DSM-IV-TR (APA, 2000), the criteria for Antisocial PD are as follows:
Evidence of conduct disorder before age 15 years pervasive pattern of disregard for, and violation of, the rights of others since the age of 15 years, as indicated by three or more of the following: Failure to conform to social norms with respect to lawful behaviours, as indicated by repeatedly performing acts that are grounds for arrest; Deceitfulness, as indicated by repeated lying, use of aliases, or conning others for personal profit or pleasure; Impulsivity or failure to plan ahead; Irritability and aggressiveness, as indicated by repeated physical fights or assaults; Reckless disregard for safety of self or others; Consistent irresponsibility, as indicated by repeated failure to sustain consistent work behaviour or honour financial obligations; and Lack of remorse, as indicated by being indifferent to or rationalizing having hurt, mistreated, or stolen from another.
The need for evidence of conduct disorder before age 15 years reflects the research that shows that personality disorders are of long duration and have an onset that can be traced back at least to adolescence. The problem with the current DSM-IV-TR criteria, as compared with the criteria that appeared in the DSM-II or the Cleckley criteria, is that they are based largely on behavioural symptoms and do not reflect the rich clinical descriptions of psychopathy and its progeny. Regrettably, the disorder has become a diagnostic category for behavioural diffi- culties pertaining to criminality. Moreover, as will be discussed below under implications, far more people (particularly prisoners) meet the criteria for a diagnosis of Antisocial PD, than is warranted.
In recognition of the overlap between symptoms of some personality disorders, and the difficulty in differentially diagnosing one personality disorder from the others, the DSM-IV divided personality disorders into three categories or ‘clusters’ organized by disorders that share characteristics. Antisocial PD falls into ‘Cluster B’ – the dramatic-eccentric-emotional cluster – that includes Antisocial PD, Borderline Personality Disorder, Histrionic Personality Disorder and Narcissistic Personality Disorder.
The 10th edition of the International Classification of Diseases (World Health Organization, 1990) [13] uses both personality traits and behaviours for the diagnosis of Dissocial PD, conceptually similar to psychopathy. The criteria for this disorder are:
callous unconcern for the feelings of others and lack of the capacity for empathy;
gross and persistent attitude of irresponsibility and disregard for social norms, rules and obligations;
incapacity to maintain enduring relationships;
very low tolerance to frustration and a low threshold for discharge of aggression, including violence;
incapacity to experience guilt and to profit from experience, particularly punishment;
marked proneness to blame others or to offer plausible rationalizations for the behaviour bringing the subject into conflict with society; and
persistent irritability.
As compared with Antisocial PD, Dissocial PD places more emphasis on traditional psychopathy features. In particular, Dissocial PD emphasizes deficits of affect or expressed emotion, which have been seen as among the central personality features of psychopathy.
The assessment of antisocial PD and psychopathy
Partly because of the changing criteria of Antisocial PD that have been used in the various editions of the DSM, relatively little empirical work has been conducted using the current criteria. This is unfortunate indeed as considerable research has been conducted using a standardized measure of psychopathy known as the Hare Psychopathy Checklist, Revised [5], that was first developed in 1980. In addition, as noted above, as currently defined in the DSM-IV-TR, a diagnosis of Antisocial PD is largely a reflection of behavioural difficulties related to criminality. As a result of the changing criteria for Antisocial PD, and the fact that so much research has used the PCL-R and other definitions of psychopathy, all too often a diagnosis of Antisocial PD is made and clinicians believe that the implications of the disorder are similar to the vast literature on psychopathy. This is simply not true. For example, research shows that the prevalence of Antisocial PD ranges from 50% to 80% in prisons [5].
In sharp contrast, research shows that only 15% of prisoners (drawn largely from North American samples) would receive scores on the PCL-R high enough to suggest that they possess enough characteristics to be identified as psychopaths [5]. Lower rates of psychopaths have been identified in other countries, including Scotland [14]. Thus, among prisoners, the criteria for Antisocial PD produce three to five times as many people with the diagnoses as compared with the narrower construct of psychopathy, as assessed by the PCL-R. Clearly, then, the research findings obtained from studies of psychopathy
The Hare Psychopathy Checklist, Revised [5] was developed to measure the extent to which an individual meets the criteria for psychopathy (see Fig. 1). As Fig. 1 shows, psychopathy, as measured by the PCL-R is comprised of interpersonal, affective, lifestyle and antisocial features. The PCL-R includes two additional items that do not load on the two main factors, promiscuous sexual behaviour and many short-term marital relationships. The PCL-R provides a score of the extent to which an individual possesses the characteristics consistent with psychopathy. As such, the PCL-R is a dimensional measure of the traits of psychopathy. While it is true that people may possess some of the characteristics to some extent, very few people possess enough of the traits to be considered ‘psychopathic’ (i.e. approximately 15% of North American male prisoners, 7.5% of North American female prisoners, 10% of male forensic psychiatric patients, fewer than 3% of psychiatric patients and an estimated 1% or less of the general community [5,19]).
Scale structure of the PCL-R: 2nd edn (Hare [5]).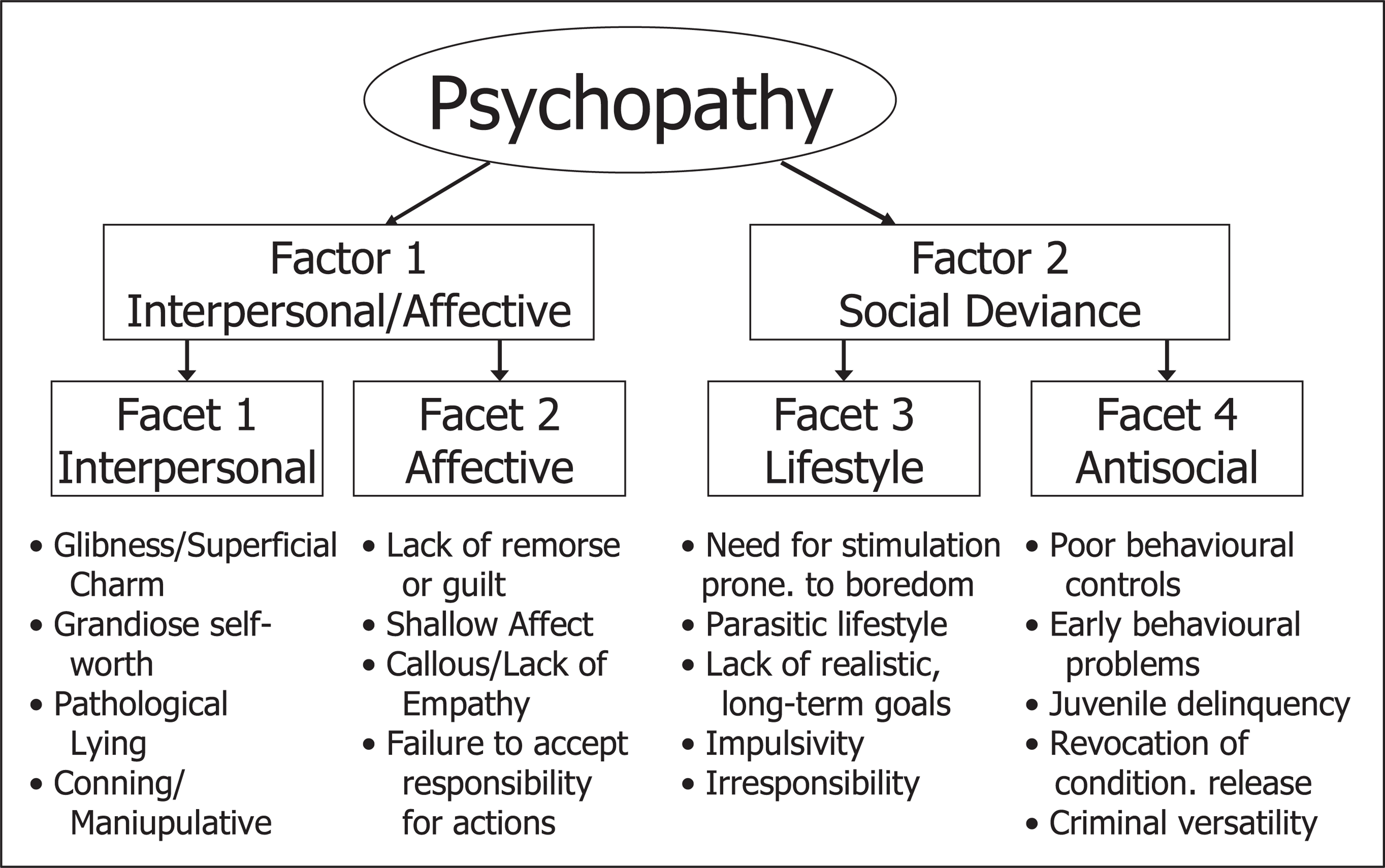
Although not without its detractors [20,21], legal and ethical issues [22–24], reviews of the PCL-R have been positive and literally more than 100 peer reviewed studies support the reliability and validity of the PCL-R. In a review of the PCL-R for the
In addition to the PCL-R, a screening version has been developed that includes 24 items [28] and a version for youth (12–18 years) [29].
Comparing the PCL-R with antisocial PD and dissocial PD
The conceptualization of psychopathy, as operationalized by the PCL-R, is based on the clinical tradition of the disorder, as described by Cleckley [8] and based on Hare's earlier work [30–32]. As described above, the PCL-R is comprised of two factors and four facets that, together, represent the range of symptoms of the disorder: interpersonal, affective, lifestyle and antisocial. In this section, a comparison of the PCL-R items and the criteria for Antisocial PD and Dissocial PD is presented.
A comparison of the criteria for Antisocial PD with the items on the PCL-R, reveals that only three of the eight items from Factor 1 (two items from Facet 1 – pathological lying and conning/manipulative – and one item from Facet 2 – lack of remorse or guilt) are found in the criteria for Antisocial PD. By contrast, six out of 10 of the items from Factor 2 (three items from Facet 3 – need for stimulation and proneness to boredom, impulsivity and irresponsibility – and three from Facet 4 – poor behavioural controls, early behavioural problems and criminal versatility) overlap with Antisocial PD criteria. Thus, as a crude measure, 3/8 (37.5%) of the interpersonal or affective symptoms from the PCL-R and 6/10 (60%) of the social deviance symptoms can be found in the criteria for Antisocial PD. This suggests, first, that the Antisocial PD criteria are much broader (i.e. less precise) than the PCLR criteria and, second, that Antisocial PD contains many more behaviourally based (social deviance) symptoms than personality-based (interpersonal or affective) symptoms. These comparisons help explain how the Antisocial PD criteria over-identify prisoners as having the disorder, compared with the more comprehensive criteria found in the PCL-R.
Of particular concern is the virtual absence of affective criteria from Antisocial PD, with only lack of remorse or guilt being present. Indeed, affective deficits, including shallow affect, lack of remorse or guilt, callousness, have long been seen as central features of psychopathy [8,27,33].
When the criteria for Dissocial PD were compared with items on the PCL-R, the results show that no items from Facet 1 (interpersonal) are found in the Dissocial PD criteria. By contrast, the criteria for Dissocial PD overlap with three out of four of PCL-R Facet 2 (affective) items (i.e. lack of remorse or guilt, callous/lack of empathy and failure to accept responsibility for their own actions). Taken together, like the Antisocial PD criteria, 3/8 (37.5%) items on the PCL-R overlap with the Dissocial PD criteria.
While none of the interpersonal items from the PCL-R is found in the Dissocial PD criteria, unlike the criteria for Antisocial PD, the Dissocial PD criteria emphasize affective deficits. This can be seen as a positive feature because of the importance of affective symptoms in the clinical tradition of psychopathy. While the criteria for Antisocial PD over-emphasize behavioural/antisocial traits as compared with interpersonal/ affective features, the same is not true for the Dissocial PD criteria. Indeed, the Dissocial PD criteria only overlap with two of the 10 items (20%) from Factor 2 – one from each of Facet 3 (i.e. irresponsibility) and Facet 4 (i.e. poor behavioural controls). Similar to the PCL-R item ‘many short-term marital relationships’ that does not load on any particular facet, the Dissocial PD criteria include the item ‘incapacity to maintain enduring relationships’.
All of the criteria for Antisocial PD overlap with items from the PCL-R – with the emphasis being on the behavioural facets (i.e. lifestyle and antisocial). All but one of the criteria for Dissocial PD (i.e. persistent irritability) are found in the PCL-R. Like the Antisocial PD criteria, though, the Dissocial PD criteria are far less comprehensive than the PCL-R. Unlike the criteria for Antisocial PD, however, the Dissocial PD emphasizes affective symptoms and de-emphasizes behavioural symptoms.
The differences between the constructs are significant. Above it was noted that some 50% to 80% of prisoners meet the criteria for Antisocial PD [5] whereas only 15% of prisoners would have PCL-R scores in the ‘high’ range [5]. These differences raise important concerns about the extent to which findings from the PCL-R – and the psychopathy construct more traditionally – are applied to a diagnosis of Antisocial PD. In a recent study, the PCLR was compared with DSM-IV disorders, including Antisocial PD among male forensic psychiatric patients from the Netherlands [34]. The results showed that, consistent with the above comparison, ‘the link between PCL-R psychopathy and antisocial PD is asymmetric. Most patients (81%) diagnosed as psychopaths by the PCL-R criteria met criteria for a diagnosis of antisocial PD, whereas a minority (38%) of those with antisocial PD received a diagnosis of PCL-R psychopathy’ (p. 245). Moreover, the correlation between Antisocial PD and PCL-R scores was much higher for Factor 2 (social deviance) (r = 0.65) than for Factor 1 (interpersonal/affective) (r = 0.39). These results are consistent with previous data from forensic psychiatric patients in Canada [35] and Sweden [36].
Taken together, while the constructs of Psychopathy, Antisocial PD and Dissocial Personality are often referred to interchangeably, the reality is that there are significant differences with the symptoms/items underlying these disorders. As such, the implications of psychopathy, discussed below, do not pertain equally to either Antisocial PD or Dissocial PD.
Implications of psychopathy
The implications of psychopathy, as measured by the PCL-R, will be briefly reviewed here. It must be emphasized that the results reflect information obtained about those who obtain high scores on the PCL-R (typically greater than 30/40) and cannot be extended to a diagnosis of Antisocial PD or Dyssocial Personality.
Prevalence
Although almost impossible to evaluate, it has been estimated that approximately 3% − 5% of people in the general population would meet the criteria for a diagnosis of Antisocial PD. By contrast, less than 1% are thought to possess enough characteristics of psychopathy to obtain a high score (30/40) on the PCL-R. Naturally, the relative prevalence varies significantly by population. Approximately 15% of male prisoners, 10% of forensic patients, 7% of female prisoners, and 1% of involuntarily committed psychiatric patients have scores that fall in the high range on the PCL-R [5,18].
Comparable data available for Antisocial PD or Dissocial Personality, provide much higher rates of those disorders [34–36]. In one relatively small-scale study of 289 mostly male patients in a methadone-maintenance program in the US, Tourian
Risk for offending and violence
Although not developed as a risk assessment tool, the PCL-R and the Psychopathy Checklist: Screening Version (PCL : SV) have been found to be among the best predictors of risk for offending and risk for violence. For example, following a meta-analysis of all available studies at the time, Hemphill
It must be emphasized that while the PCL-R and PCL : SV have been found to be moderate to strong predictors of future offending and violence, contemporary approaches to risk assessment require that these measures not be employed in isolation [39].
In an early studied conducted to investigate the relationship of the PCL to offending, Hart
In New Zealand, Wilson has conducted a number of studies with the Psychopathy Checklist: Screening Version [27]. Wilson and Bakker [42] found that the PCL : SV correlated strongly with reconvictions (r = 0.50) and re-imprisonment (r = 0.49). With a PCL : SV score of 16/24, the true positive rate (76%) and true negative rate (68%) were high. The false positive rate (32%) and false negative rate (24%) were appropriately low. Wilson further attempted to investigate the 32 offenders who had been classified as false positives (i.e. those with high scores who apparently did not re-offend). He found that two of the men had died, one was in the witness protection program, and two were remanded for committing a crime. Taking these cases into account, the false positive rate fell to 25%; however, almost all of the remaining people (91%) were said to have been convicted of a crime but did not return to prison. If the researchers had considered reconvictions as ‘failures’, there would have been virtually no false positives.
In addition to offenders, research has also found that the Hare Psychopathy Checklist is a strong predictor of violence and offending in populations of male and female [43] psychiatric patients. It is important to emphasize that this is the case even though the rate of psychopathy in psychiatric populations is very low (i.e. approximately 1–2%). Douglas
In the US, a large scale study of almost 1000 involuntarily hospitalized psychiatric patients, Monahan
Research exploring the construct of psychopathy and its relationship with violence and crime among women from the general population, female offenders, female forensic psychiatric patients and female substance abusers suggests the PCL measures have a relationship with violence among women similar to what has been reported in the literature with samples of men [39].
When considered together – while certainly not a perfect predictor and never designed as a measure of violence risk assessment – the Hare Psychopathy Checklist measures are relatively strongly related to risk for future violence.
Treatment implications
To date, there is little evidence that conventional approaches to psychological treatment are successful for use with psychopaths. Salekin argued that the research that has been conducted to assess the efficacy of treatment with psychopaths has been largely deficient and he suggests that there is some reason for guarded optimism that it may be possible to treat psychopaths [46].
Wong conducted a review of the existing studies that have attempted to assess the efficacy of treating psychopaths [47]. Unfortunately, only two studies were found to be methodologically sound enough to warrant consideration and both of those employed inappropriate treatment approaches. Wong and Hare have developed a best-practice model for the institutional treatment of psychopaths [48]. Wong has found that approaches such as those outlined in the book show promise to be effective if implemented systematically [48]. Generally speaking, those treatment guidelines suggest a focus on behaviour change and control rather than targeting traditional emotional and cognitive factors, such as empathy training, social skills, etc.
To illustrate one study of the effect of treatment on psychopathy, it may be worth considering the work of Ogloff
Those prisoners in the high psychopathy group performed significantly worse than either those with medium or low psychopathy scores on
In addition to being ineffective for the psychopaths themselves, having psychopaths in conventional treatment groups may serve to detrimentally affect the group functioning and dynamics. As a result, it is important that offenders being considered for conventional psychological treatment programs be screened for psychopathy. Those with high scores (e.g. PCL-R scores greater than 30) require appropriate, modified, intervention approaches, rather than simply mixing them in with other offender treatment groups.
Finally, caution must be used when relying on treating clinicians' reports of treatment progress for psychopathic offenders. Seto and Barbaree investigated treatment change ratings and psychopathy scores for 216 offenders who were treated in a sexual offender treatment program in Canada [50]. Treatment change ratings were made by clinical staff and used to divide offenders into ‘Good’ and ‘Poor’ treatment change groups. Similarly, participants were divided into those with ‘High’ (>15/40) and ‘Low’ (<15/40) PCL-R scores. The offenders were followed up in the community for an average of 32 months following release from prison. Participants in the Low PCL-R group had low rates of general (10% recidivism) and serious offending (5% recidivism), and their reoffence rates were unrelated to treatment change ratings. Unfortunately, the re-offence rates of participants who were in the High PCL-R group were strongly related to their treatment change scores – but in the opposite direction to what would be expected following treatment. That is, offenders in the High PCL-R group, who received ‘Good’ treatment change ratings, had the highest rates of re-offending for both general (28%) and serious (21%) offences. Even those in the High PCL-R group who received poor treatment change ratings had lower reoffence rates. Thus, the treatment change ratings derived from clinicians' perceptions of treatment change were unrelated to re-offending for those in the Low PCL-R group and were inversely related to likelihood of reoffending for those in the High PCL-R group. In fact, the re-offence rate for the High PCL-R group whom clinicians thought had shown improvement during treatment had a re-offence rate for sexual and other violent offences that was more than four times higher than all other offenders.
Unfortunately, the findings of Seto and Barbaree [50] have recently been found by other researchers. Unlike Seto and Barbaree, though, who used very low scores to subdivide the ‘high’ and ‘low’ PCL-R groups (i.e. 15/ 40), Looman
These findings show that the offenders with high scores on the PCL-R who were believed to have made good progress in treatment actually were most likely to re-offend over the follow-up period. The results show the importance of conducting independent ratings of risk for re-offending for offenders who have undergone treatment as clinicians' ratings of treatment change do not seem reliable measures of risk of re-offending – particularly for those offenders with high PCL-R scores. As the above results were found for sexual offenders, some caution should be exercised about extrapolating the findings to other offender groups.
The information presented in this section shows that the treatment of psychopathic offenders is particularly difficult, with little empirical support that positive change, measured by re-offence rates, can be easily achieved. Nonetheless, some recent work shows promise. Consideration must be given, as well, to the ‘contamination’ that can occur in a treatment program when psychopathic offenders form part of the group. Finally, recent findings show that the highest recidivism rates have been found for those sexual offenders with higher PCL-R scores who are believed by treatment staff to have made positive changes in treatment. As such, caution must be taken when relying on treatment teams' reports to determine the likelihood of future offending.
Limitations of psychopathy
There are a number of limitations that apply to the concept of psychopathy, and to the Hare Psychopathy Checklist measures. First, the assessment of psychopathy using the Hare Psychopathy Checklist requires expertise in psychiatry or psychology, which includes training and experience in psychopathology, psychometric assessment, and the research in the field of psychopathy. Without proper training and supervised experience, particularly in the areas of psychometric testing, psychopathology and offending, there can be little confidence that the psychopathy scores obtained are reliable or valid. Second, the Hare Psychopathy Checklist cannot be administered based on an interview alone. Rather, the clinician must also have access to good file and collateral information. Third, the administration of the tool is timeconsuming (although the relevant information should be obtained by any proper assessment, particularly if assessing the risk of offending and violence). Fourth, while a significant predictor of risk for offending and violence, many offenders (the majority in fact) have low or moderate scores on psychopathy and of those with high scores, typically up to 20% do not re-offend or are not re-incarcerated during follow-up studies. As a result, there are both false positive and false negative errors that much be considered. Fifth, scores obtained from the Hare Psychopathy Checklist are generally stable or static and do not change much over time. As a result, the instrument
As a result of the above limitations, while it is a useful measure for a number of purposes, care must be taken in the administration and interpretation of the Hare Psychopathy Checklist. In particular, the instrument must be administered by trained professionals and the instrument must be used appropriately.
Summary and conclusions
As the information reviewed in this article shows, there is likely an over-diagnosis of Antisocial PD in our prisons and mental-health systems because of the largely behaviourally based nature of the diagnostic criteria of Antisocial PD. Moreover, Antisocial PD and Dissocial PD does not measure the same symptoms as the PCL-R and, for that matter, are significantly different from one another. Importantly, the findings that have been found to pertain to ‘psychopathy’ – particularly as operationalized by the Hare Psychopathy Checklist – may not be extended to those diagnosed with Antisocial PD or Dissocial PD. In fact, relatively little is known about the nature and outcome of those who meet the DSM-IV-TR criteria for a diagnosis of Antisocial PD and Dissocial PD. Certainly the all-too-common practice expressed by many of those in mainstream and forensic mental-health services that somehow those with Antisocial PD are to be considered high risk for aggression and excluded from treatment is simply unwarranted.
With its emphasis on interpersonal characteristics, affective features, lifestyle variables and antisocial features, the Hare Psychopathy Checklist is an operationalization of the construct of psychopathy that reflects a long-standing clinical tradition. The prevalence of psychopathy is much lower than that found for a diagnosis of Antisocial PD. Indeed, approximately 15% of male prisoners, 10% of forensic patients, 7% of female prisoners [5], and 1% of psychiatric patients [19] likely have high scores on the PCL-R. The PCL-R and PCL : SV have been found to be significantly related to ongoing offending and violence by male and female prisoners, forensic patients and psychiatric patients.
Given the characteristics of psychopathy, caution must be exercised in attempting conventional psychological treatment for those with high scores on the PCL-R or PCL : SV. Rather than simply having them participate in group programs that are typical of prison programming, those with high psychopathy scores would benefit more from an approach using the guidelines developed by Wong and Hare [48].