
Abstract
Objective:
We examined two hypotheses regarding the potential association of pornography use with body image–related and eating disorder–related psychopathology among sexual minority males (i.e. non-heterosexual males). Our primary hypothesis was that pornography use would be associated with males’ body dissatisfaction, eating disorder symptoms, thoughts about using anabolic steroids and quality of life impairment; our secondary hypothesis was that the type of pornography, namely, professional versus amateur pornography, which contains idealised and non-idealised (i.e. regular) bodies, respectively, would moderate these associations.
Methods:
A sample of 2733 sexual minority males living in Australia and New Zealand completed an online survey that contained measures of pornography use, body dissatisfaction, eating disorder symptoms, thoughts about using anabolic steroids and quality of life.
Results:
Almost all (98.2%) participants reported pornography use with a median use of 5.33 hours per month. Multivariate analyses revealed that increased pornography use was associated with greater dissatisfaction with muscularity, body fat and height; greater eating disorder symptoms; more frequent thoughts about using anabolic steroids; and lower quality of life. Effect sizes for these associations were uniformly small. Neither relationship status nor genital dissatisfaction was associated with pornography use. The association between pornography use and thoughts about using anabolic steroids was stronger for viewers of professional pornography than viewers of amateur pornography.
Conclusion:
The findings suggest that the use of pornography is weakly associated with body dissatisfaction and related variables and that the type of pornography (amateur vs professional) viewed may be a moderating factor in some cases. Within the limits of a cross-sectional study design, these findings may have implications for clinicians who treat individuals with eating disorders, body dysmorphic disorder, anabolic-androgenic steroid dependence and related concerns.
Several theories of body image and eating disorders posit that cumulative exposure to media containing idealised (i.e. unrealistic) bodies promotes the development of poor body esteem, via mechanisms such as body objectification and physical appearance self-comparisons (Michaels et al., 2012; Thompson et al., 1999; Tiggemann and Williams, 2012; Tylka, 2011; Tylka and Andorka, 2012). Experimental and cross-sectional studies have shown that exposure to idealised bodies in various forms of media, including static images, videos, television advertisements, magazines and action figures, can increase body dissatisfaction, with small-to-moderate effect sizes (Blond, 2008; Hausenblas et al., 2013). More recently, there has been increasing interest in the potential effects on body image of non-traditional forms of media, and in particular, forms of social media, including thinspiration and fitspiration imagery, that emphasise physical appearance, dieting and exercise (Boepple and Thompson, 2015; Murray et al., 2016b; Tiggemann and Zaccardo, 2015). Social media may exact a particularly potent effect due to the considerable amount of time individuals spend interacting with this form of media compared with traditional media (Sampasa-Kanyinga et al., 2016).
Pornography is a hitherto understudied form of non-traditional media, the use of which has become ubiquitous among males in the general population. Findings from recent studies suggest that 82–99% of males currently use one or more forms of pornography at least occasionally, with estimates for sexual minority males towards the higher end of this range (Carroll et al., 2008; Hald and Malamuth, 2007; Kvalem et al., 2015; Sun et al., 2014; Tylka, 2015). As with most forms of mass media, the bodies contained in pornography are often idealised, featuring actors whose body dimensions and proportions are far removed from those of the general population in terms of muscularity, body fat, height and the size and shape of genitalia and other body features (Elder et al., 2012, 2015; Löfgren-Mårtenson and Månsson, 2010; McKee et al., 2008). For example, a content analysis of pornographic videos sold in Australia found that pornographic actors were frequently highly muscular with notably idealised and unrealistic genitalia (McKee et al., 2008). Thus, the use of pornography has the potential to promote body dissatisfaction relating to various body image domains, and males may be particularly susceptible to such effects by virtue of their high levels of use (Corneau and Van der Meulen, 2014; Tylka, 2015).
Studies of the associations between pornography use and body dissatisfaction and related variables among males suggest small positive correlations (Peter and Valkenburg, 2014; Ridgeway and Tylka, 2005). To date, however, studies have typically been limited to heterosexual males and/or have not examined genital dissatisfaction, despite the obvious relevance of this in the context of pornography use. Furthermore, associations with certain variables likely to be of interest, namely, quality of life and thoughts about using anabolic steroids, are also yet to be explored. Quality of life assessment is increasingly used as an outcome measure in studies seeking to determine the public health burden of different health states and risk factors for these, and to inform public health policy and decision-making, including in relation to body dissatisfaction and eating disorders (Gouveia et al., 2014; Griffiths et al., 2016, 2017b; Mitchison et al., 2013). Anabolic steroids are among the most concerning of the behaviours associated with muscularity-oriented body image psychopathology and are increasingly being studied – and treated – by academics and health professionals with an interest in body image disturbance and eating disorders (Griffiths et al., 2017a; Kanayama et al., 2010; Murray et al., 2016a; Tod et al., 2016; Hildebrandt et al. 2010; Murray et al. 2016c).
Examination of the associations between pornography use and body image–related and eating disorder–related psychopathology among sexual minority males may be of particular interest because, unlike for heterosexual males, the primary viewing subject is typically a male. Since the operative mechanism in extant theories of media and body dissatisfaction is that the viewer compares his (or her) self to the bodies contained in the media, examination of the correlates of pornography among sexual minority males arguably provides a more compelling test of the hypothesis that pornography is associated with body dissatisfaction. Furthermore, sexual minority males are at increased risk for the development of body image psychopathology, including that related to body dissatisfaction, eating disorders and the use of anabolic steroids (Blashill et al., 2017; Blashill and Safren, 2014; Martins et al., 2007; Yelland and Tiggemann, 2003).
Also of interest is the possibility that any observed association between pornography use and body dissatisfaction may be moderated by the type of pornography viewed, namely, amateur or professional pornography (Peter and Valkenburg, 2014). Given that professional pornography, which features ‘porn stars’, is more likely to involve the viewing of unrealistic bodies than amateur pornography, which by definition involves amateur performers, with less idealised bodies, it is reasonable to hypothesise that stronger associations with body dissatisfaction might be observed for the former when compared with the latter. Indeed, the depiction of more ‘realistic’ bodies in popular media, including, for example, ‘plus size models’, is increasingly advocated, the premise being that exposure to more realistic bodies may be less likely to promote body dissatisfaction and eating-disordered behaviour than exposure to idealised body types, such as those of supermodels (Owen and Spencer, 2013; Papies and Nicolaije, 2012).
In sum, we sought to examine whether, and to what extent, the use of pornography would be associated with body dissatisfaction, eating disorder symptoms, thoughts about using anabolic steroids and quality of life impairment, among a large sample of sexual minority males. We specifically examined visual pornography because self-comparisons based on physical appearance are thought to be the operative mechanism by which media consumption impacts body image, and thus, the subsequent development of body image and eating disorders. Two predictions were made: a primary prediction that increased use of pornography would be associated with greater body dissatisfaction and eating disorder symptoms, more frequent thoughts about using anabolic steroids and greater quality of life impairment; and a secondary prediction that these associations would be moderated by the type of pornography viewed, namely, professional versus amateur.
Method
Procedure
Participants were recruited via an advertisement for ‘Gay Bodies – a study of body image and body change behaviours among gay men only’, which was placed on a popular geo-social networking app for sexual minority males in Australia and New Zealand. Responding to the advertisement re-directed potential participants to an information and consent page for an online survey. Consenting participants continued on to the survey, which took a median time of 11 minutes to complete. Ethical approval was received by the Behavioural and Social Sciences Human Ethics Sub-Committee at the University of Melbourne (ethics ID: 1748752).
Measures
Demographics
Participants were asked to provide information on their gender and age. Cultural background was assessed based on the Australian Standard Classification of Cultural and Ethnic Groups (Australian Bureau of Statistics, 2016). Sexual orientation was measured using a 5-point Kinsey-like scale from ‘exclusively gay’ to ‘exclusively heterosexual’, with ‘bisexual’ as the midpoint. Finally, participants were asked to indicate their relationship status as ‘single’, ‘in a casual relationship (e.g. ‘friends-with-benefits’)’, ‘in a serious relationship’, ‘in a civil union, civil or domestic partnership’, or ‘married’. For participants who felt that their status did not fit within these definitions, a free-text data-field was available for an alternate response.
Pornography use
In line with methodological practices recommended in a review of pornography research by Short et al. (2012), we supplied participants with the following definition of visual pornography: ‘Visual pornography [hereafter called ‘porn’] refers to sexually explicit videos and images in which sexual activities are clearly visible’. In addition, participants were instructed not to respond to the survey questions in relation to audio-only or text-only pornography.
Subsequently, participants were asked how often they watched pornography. Responses were given on a 12-point scale, namely: ‘never’, ‘less than once a month’, ‘once a month’, ‘twice a month’, ‘several times a month’, ‘once a week’, ‘twice a week’, ‘several times a week’, ‘once a day’, ‘twice a day’, ‘several times a day’ and ‘five or more times a day’. In addition, participants were asked: ‘When you watch porn, how long do you typically watch it for?’ Responses to this question were given using a sliding scale, anchored at 0 minutes and 180 minutes, which could be moved in 1-minute increments. A variable indicating participants’ cumulative use of pornography during the past 28 days was derived by re-coding participants’ answers to the question about frequency of pornography use to represent the number of times they watched pornography during this period. Supplementary Table A contains more information about the re-coding process. The variable representing how many times participants watched pornography during a 28-day period was then multiplied with the variable representing average duration of use, resulting in a variable representing consumption of pornography during this period.
Finally, participants were asked questions about the use of amateur versus professional pornography. For this purpose, the following definitions were provided: ‘Amateur porn includes, for example, homemade videos in which the actors/actresses are unpaid’. ‘Professional porn includes, for example, videos with high production values in which the actors/actresses are paid’. To check the validity of these definitions, participants were asked whether the distinction between amateur and professional pornography made sense to them (‘Yes – it makes sense’; ‘Unsure – it kind of make sense’; ‘No – it makes no sense at all’). Participants were then asked to estimate how much of the pornography they watched was amateur versus professional. Responses to this question were given on a 7-point scale anchored with the options ‘I exclusively watch amateur porn’ (1) and ‘I exclusively watch professional porn’ (7) and with a midpoint option of ‘I watch an equal amount of amateur and professional porn’ (4).
Body dissatisfaction
Dissatisfaction with muscularity, body fat and height were measured using the Male Body Attitudes Scale – Revised (MBAS-R; Ryan et al., 2011). The MBAS-R includes three subscales measuring dissatisfaction with muscularity (7 items), body fat (5 items) and height (3 items). Respondents indicate the frequency with which they endorse each statement on a 5-point scale ranging from ‘never’ (1) to ‘always’ (5).
A measure of genital dissatisfaction was created for this study by adapting the item wording of the above-mentioned height dissatisfaction subscale. We chose to adapt the height dissatisfaction subscale because genitals and height, as opposed to muscularity and body fat, cannot (generally) be altered through dieting or exercise. The item wordings for the genital dissatisfaction subscale were ‘I wish I had a larger penis’, ‘I am satisfied with the size of my penis’ (reverse scored) and ‘I feel ashamed of the size of my penis’. Response options for these items were the same as those for the MBAS-R. In previous studies, Cronbach’s α of 0.88, 0.91 and 0.88, for the muscularity, body fat and height subscales, respectively, were reported (Ryan et al., 2011). In this study, Cronbach’s α were 0.88, 0.92 and 0.76, for the muscularity, body fat and height subscales, respectively. For the genital subscale, Cronbach’s α was 0.87.
Eating disorder symptoms
The 12-item, single-factor Eating Disorders Examination Questionnaire Short (EDE-QS; Gideon et al., 2016) was used to measure the frequency and severity of core eating disorder symptoms, such as dietary restriction, binge eating and overvaluation of weight/shape during the past week. Respondents indicate the frequency of symptoms on a 4-point response scale, ranging from 0 (‘0 days’) to 3 (‘6–7 days’). The EDE-QS was based on the EDE-Q (Fairburn and Beglin, 1994), the most widely used self-report measure of eating disorder psychopathology, and was designed to provide a more succinct scale and improved reliability over the EDE-Q. The authors have demonstrated the construct validity, predictive validity and test–retest reliability (intraclass correlation coefficient [ICC] = 0.93, p < 0.001, time range: 2–14 days) of the EDE-QS (Gideon et al., 2016). Cronbach’s α in this study was 0.88.
Thoughts about using anabolic steroids
In order to assess thoughts about using anabolic steroids, participants were asked: ‘How frequently do you think about using anabolic steroids?’ (with no time frame specified). Recommendations made in previous research were used to design this question (Kanayama et al., 2007). First, we used the term ‘anabolic steroids’ rather than the broader and more nebulous term ‘steroids’; second, we provided participants with the names of three types of anabolic steroids commonly used in Australia and New Zealand, namely, testosterone enanthate, dianabol and clenbuterol. Provision of this information was intended to reduce the potential impact of false-positives by helping participants distinguish illicit anabolic (i.e. muscle-building) steroids from legal non-anabolic (i.e. non-muscle-building) steroids; the latter including, for example, corticosteroids used to treat skin conditions. Response options ranged from 1 (‘never’) through 6 (‘always’).
Quality of life
Quality of life was measured using the Brunnsviken Brief Quality of Life Scale (BBQ; Lindner et al., 2016). The BBQ includes 12 items that assess perceived satisfaction with six domains: leisure, creativity, learning, friends and friendship, view on one’s life and view on one’s self. Respondents indicate their level of agreement with each statement on a 5-point scale ranging from 0 (‘strongly disagree’) to 4 (‘strongly agree’). Participants also rank the importance of each domain in determining their overall quality of life. Weighted scores are calculated for each domain by multiplying raw scale scores by the level of importance ascribed to the relevant domain. A total quality of life score, ranging from 0 to 96, is then calculated by summing the six scale scores. The authors have demonstrated a robust single-factor structure and adequate internal consistency (α = 0.76) and test–retest reliability (ICC = 0.82, p < 0.001, time range: 7 days ± 1 days) for the total score (Lindner et al., 2016). Cronbach’s α in this study was 0.81.
Participants
A total of N = 3756 potential participants accessed the survey. Of these, n = 539 did not provide either consent (n = 397) or data (n = 142). Of the remaining N = 3217 participants, n = 452 were excluded due to unacceptably high levels of missing data (i.e. >30%), n = 5 were excluded due to a pattern of implausible data, n = 2 were excluded due to specifying their gender as ‘female’ and n = 25 were excluded due to being younger than 18 years. Single data points that were implausible (e.g. age = ‘6’) were rare (<0.1%) and recoded as missing. The post-exclusion sample thus comprised N = 2733 participants.
The vast majority (99.1%) of participants identified their gender as male (0.4% of participants identified as ‘gender-fluid’, ‘gender-queer’, ‘gender-neutral’ or ‘non-binary’; 0.3% as ‘transgender’; and 0.2% as ‘other’). All participants reported minority sexual orientations (68.4% ‘exclusively gay/homosexual’, 21.4% ‘mostly gay/homosexual’, 8.4% ‘bisexual’, 1.1% ‘mostly straight/heterosexual’, 0.4% ‘other’ and 0.3% ‘pansexual’). A broad age range was observed, from 18 to 78 years (M = 33.93, SD = 11.94). Most participants resided in Australia (78.7%) and reported an ‘Australian’ (50.6%) cultural background. Other cultural backgrounds included New Zealand (15.4%), North-West European (8.0%), South-East Asian (6.4%), Southern and Eastern European (3.5%), Southern and Central Asian (2.8%) and North-East Asian (2.6%). A further 10.7% of participants indicated less prevalent cultural backgrounds (e.g. ‘Indigenous Australian’). The most prevalent relationship status was ‘single’ (66.0%), followed by ‘in a serious relationship’ (13.9%), ‘in a casual relationship’ (9.5%), ‘in a civil union, civil or domestic partnership’ (8.0%), ‘married’ (1.1%) and ‘separated’ (0.3%). Non-traditional relationship statuses (e.g. ‘open’, 0.9%, and ‘polyamorous’, 0.2%) were less frequently endorsed. Some participants clarified that they were married to women despite their sexual orientation or that they were married to their male partners in countries where same-sex marriage is legal.
Statistical analyses
First, participants’ frequency of use of pornography was plotted. Second, because published percentile data for pornography use are sparse, including for sexual minority males, we calculated percentile data for pornography use inclusive of the 5th through 99th percentiles. Third, we conducted a Spearman rank-order correlation analysis to examine the bivariate relationships of pornography, including frequency of use, duration of use and cumulative use, with demographic, anthropometric, psychosocial and clinical variables. Fourth, we conducted a non-parametric Kruskal–Wallis test to examine differences in cumulative pornography use as a function of participants’ relationship status. Fifth, we conducted a series of seven regression models using the PROCESS (Hayes, 2012) module for SPSS in which we examined whether the relationships of cumulative pornography use with muscularity dissatisfaction, body fat dissatisfaction, height dissatisfaction, genital dissatisfaction, eating disorder symptoms, thoughts about using anabolic steroids and quality of life were moderated by participants’ relative use of amateur versus professional pornography. Moderation was deemed present if the interaction term (cumulative pornography use by type of pornography used) was significant. To mitigate the likelihood of generating a Type I error across our seven tests for interaction, we submitted the p-values for each interaction term to a Holm–Bonferroni sequential correction (Holm, 1979).
Results
Pornography was used by 98.2% of males. Figure 1 shows the proportion of participants who selected each response option for the question about frequency of pornography use. The modal response was several times a week (35.0%), followed by once a day (17.3%) and twice a week (9.7%). Participants’ responses to the question about typical duration of pornography use were positively skewed with a mean duration of 30.32 minutes (SD = 24.39 minutes) and a median of 22 minutes. Responses spanned the full response scale, inclusive of 2 minutes (1 participant, <0.1% of responses) through 180 minutes (15 participants, 0.6% of responses). Participants’ scores representing their cumulative pornography use (the product of frequency of use and typical duration of use) during a 28-day period (approximately 1 month) were positively skewed with a mean cumulative use of 11.90 hours (SD = 23.52) and a median cumulative use of 5.33 hours. Cumulative use of pornography during a 28-day period spanned from 0 minutes through 25,200 minutes or 420 hours (17.5 days). Percentile data for cumulative use of pornography are provided in Supplementary Table B.
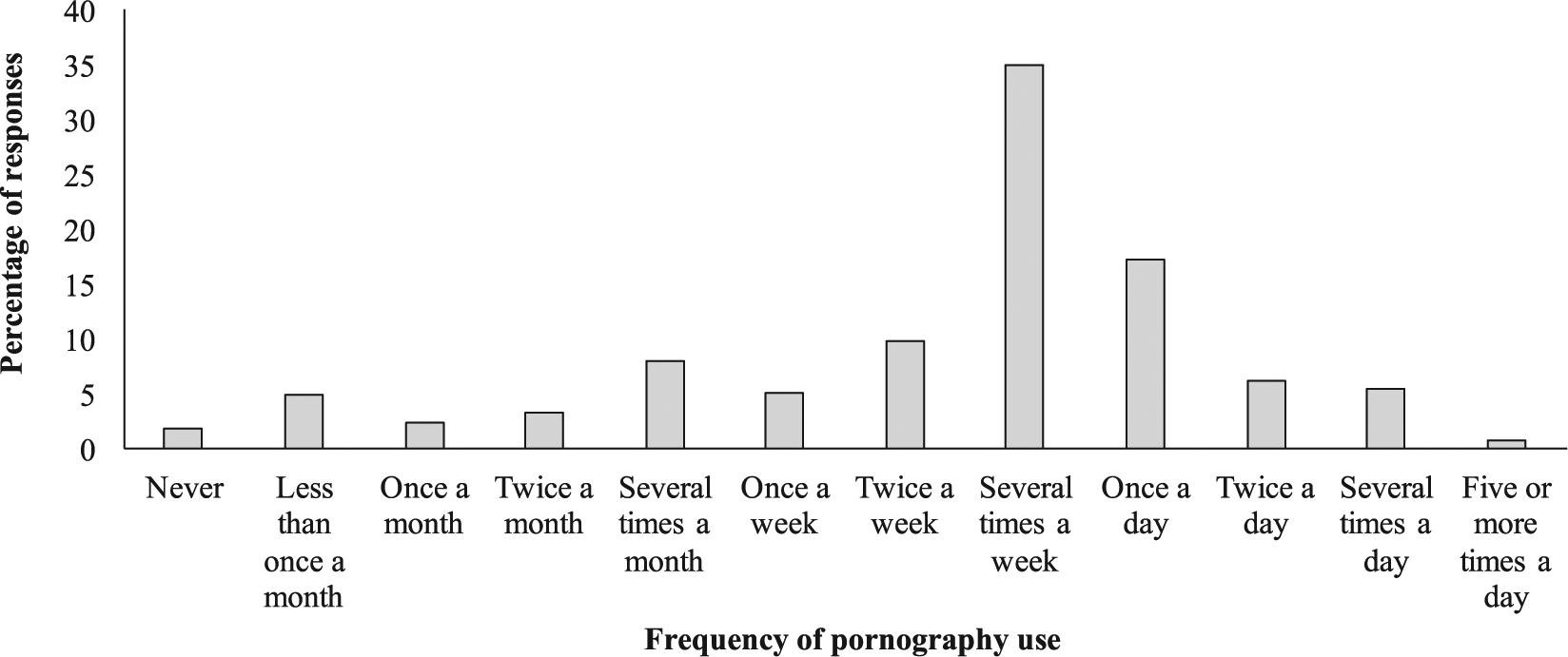
Proportion of participants who selected each response option for the question, ‘How often do you watch porn?’
In response to the question about whether the supplied definitions of amateur and professional pornography made sense, 90.9% indicated the definitions made sense, 6.3% were unsure and 2.8% indicated the definitions made no sense. Figure 2 shows the proportion of participants who selected each response for the question about frequency of use of amateur versus professional pornography. Most participants reported watching an equal amount of amateur and professional pornography (22.2%), watching mostly amateur pornography (21.6%) or watching mostly professional pornography (22.4%).
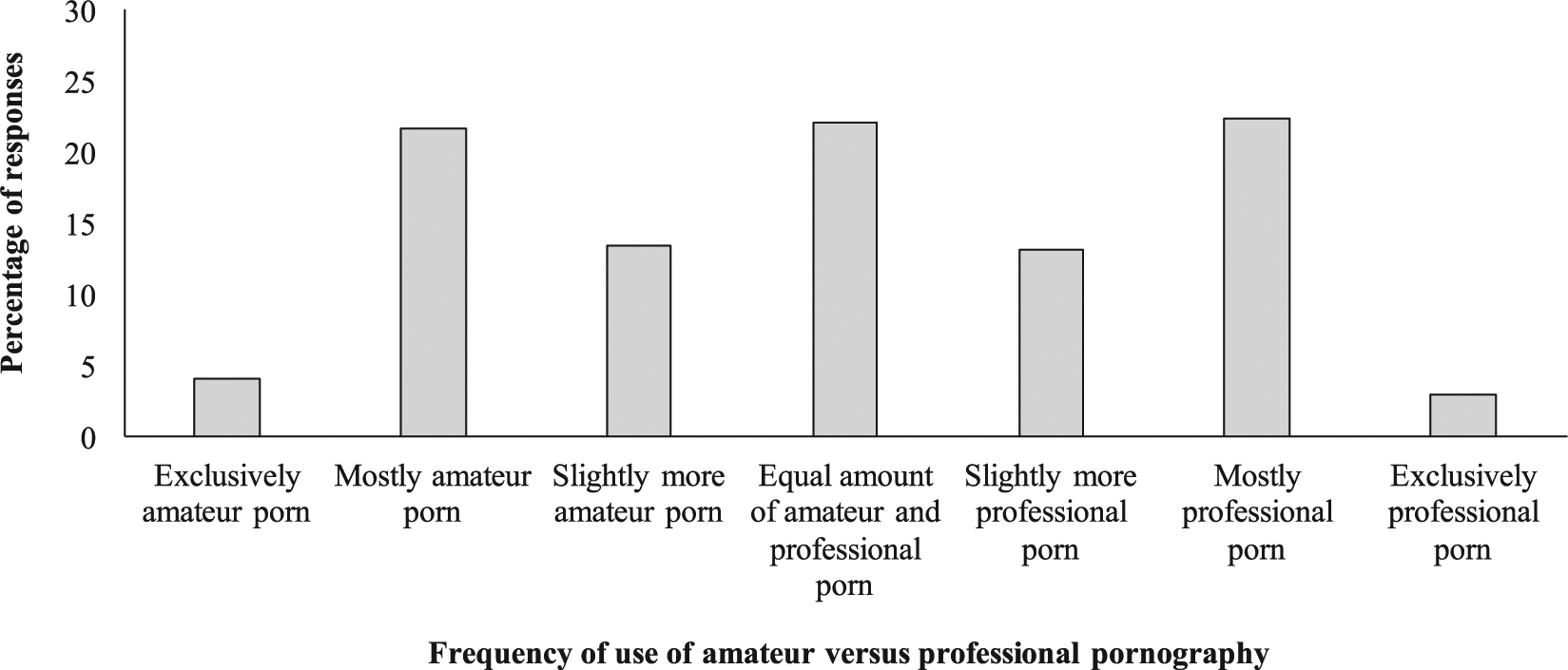
Proportion of participants who selected each response option for the question, ‘How much of the porn you watch is amateur versus professional?’ Data are shown only for those participants who indicated that the supplied definitions of amateur and professional pornography made sense to them (90.9% of participants in total).
The correlational analysis (see Table 1) indicated that increased use of pornography was associated with greater body dissatisfaction, greater eating disorder symptoms, more frequent thoughts about using anabolic steroids and lower quality of life. Effect sizes (correlation coefficients) for these association ranged from 0.05 (height dissatisfaction) to 0.12 (eating disorder symptoms). The non-parametric Kruskal–Wallis analysis revealed that participants’ cumulative use of pornography did not differ as a function of their relationship status (p = 0.095).
Spearman rank-order correlation coefficients representing the bivariate relationships of the four variables representing aspects of pornography use with demographic, anthropometric, psychosocial and clinical variables.
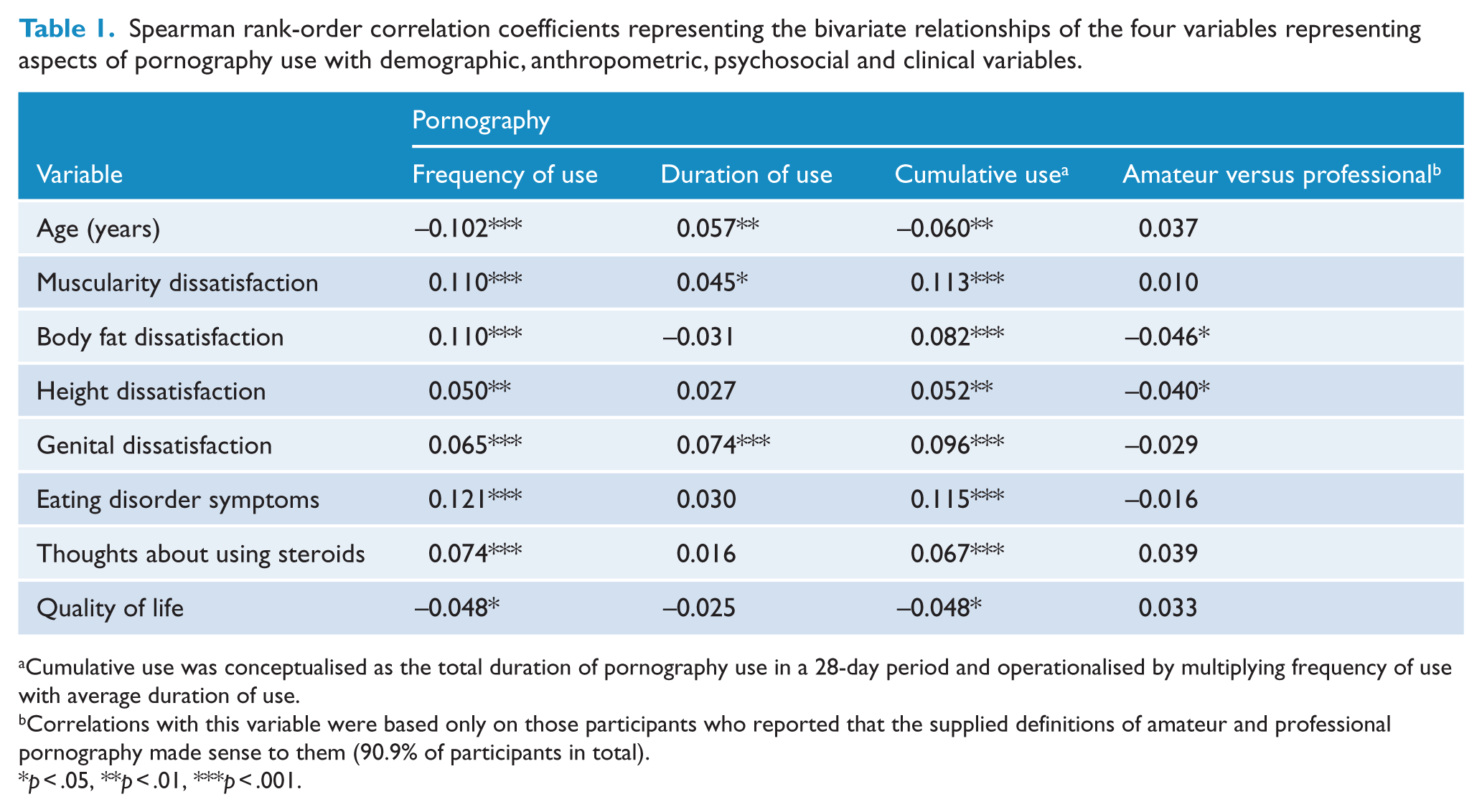
Cumulative use was conceptualised as the total duration of pornography use in a 28-day period and operationalised by multiplying frequency of use with average duration of use.
Correlations with this variable were based only on those participants who reported that the supplied definitions of amateur and professional pornography made sense to them (90.9% of participants in total).
p < .05, **p < .01, ***p < .001.
The regression models (see Table 2) indicated that pornography use was broadly and positively associated with body dissatisfaction–related and eating disorder–related psychopathology, with the notable exception of genital dissatisfaction. The effect sizes for the significant relationships were uniformly small. Furthermore, these relationships were not moderated by the type of pornography viewed, with one exception, namely, participants’ frequency of thoughts about using anabolic steroids. As shown in Figure 3, the relationship of more pornography use with more frequent thoughts about using anabolic steroids was stronger (i.e. steeper) for participants who watched professional pornography relative to participants who watched amateur pornography.
Summary statistics from the regression models conducted to examine the relationships of cumulative pornography use with body image- and eating disorder-related psychopathology is moderated by the relative type of pornography used, namely, amateur versus professional pornography. a
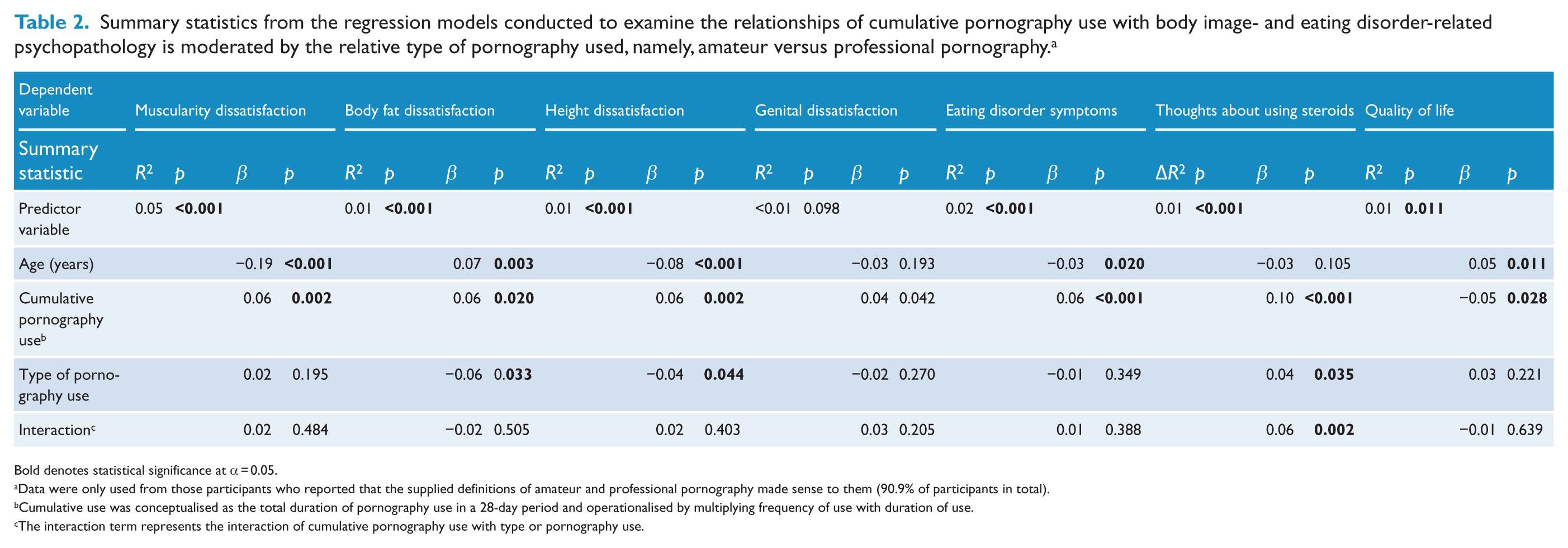
Bold denotes statistical significance at α = 0.05.
Data were only used from those participants who reported that the supplied definitions of amateur and professional pornography made sense to them (90.9% of participants in total).
Cumulative use was conceptualised as the total duration of pornography use in a 28-day period and operationalised by multiplying frequency of use with duration of use.
The interaction term represents the interaction of cumulative pornography use with type or pornography use.
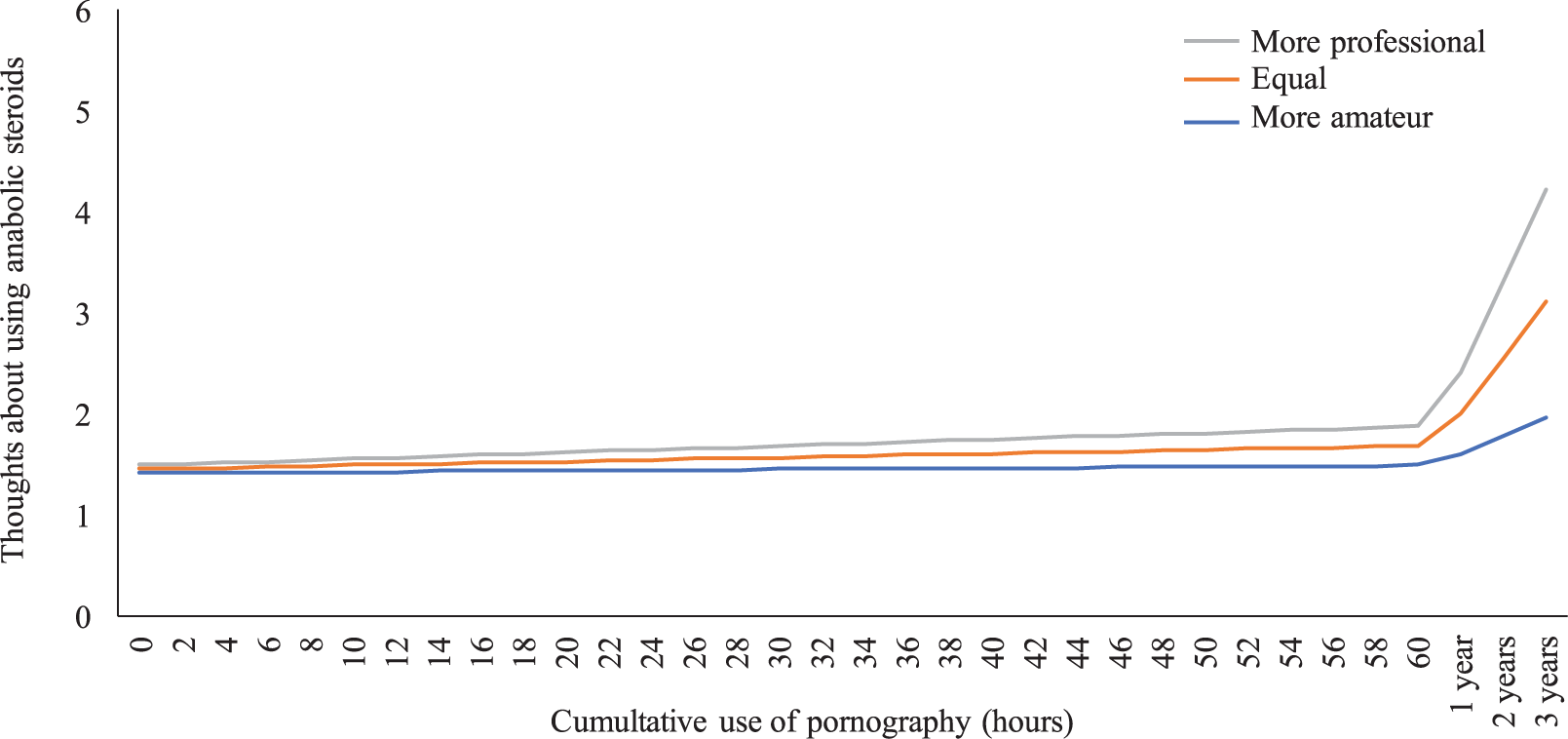
Predicted frequency of thoughts about using anabolic steroids for participants who watch more professional pornography (grey line), an equal amount of professional and amateur pornography (orange line), and more amateur pornography (blue line), as a function of participants’ cumulative use of pornography (in hours). The grey and blue lines represent participants who were +1SD and −1SD, respectively, on the question about relative use of amateur versus professional pornography. Frequency of thoughts about using anabolic steroids were anchored at 1 (‘never’) and 6 (‘always’) with midpoints at 3 (‘sometimes’) and 4 (‘often’). The rightmost values on the X-axis, namely, 1 year, 2 years and 3 years, depict the predicted frequency of thoughts about using anabolic steroids as a function of the cumulative amount of pornography that the average participant would watch in 1 year, 2 years and 3 years, as extrapolated from our data. Data are shown only for those participants who indicated that the supplied definitions of amateur and professional pornography made sense to them (90.9% of participants in total).
Discussion
We sought to examine whether, and to what extent, the use of pornography would be associated with body dissatisfaction, eating disorder symptoms, thoughts about using anabolic steroids and quality of life impairment, among sexual minority males. Two predictions were made. Our primary prediction was that increased use of pornography would be associated with greater body dissatisfaction and eating disorder symptoms, more frequent thoughts about using anabolic steroids and greater quality of life impairment; our secondary prediction was that the type of pornography, namely, professional versus amateur pornography, would moderate these associations.
Our results were broadly supportive of our first hypothesis insofar as more frequent use of pornography was associated, albeit weakly, with greater dissatisfaction with muscularity, body fat and height; greater eating disorder symptoms; more frequent thoughts about using anabolic steroids; and lower quality of life. These findings are in accord with those from previous studies and reviews of traditional media (Blond, 2008; Hausenblas et al., 2013) and provide additional evidence for theories that posit media consumption as a precipitating factor in the development of body dissatisfaction and eating disorders (Michaels et al., 2012; Thompson et al., 1999; Tiggemann and Williams, 2012; Tylka, 2011; Tylka and Andorka, 2012). Furthermore, our study extends the purview of these findings to sexual minority males, hitherto understudied in the fields of body image and eating disorders, and extends the outcomes of media consumption to include height dissatisfaction, which has received scant attention in the literature to date. Finally, we note that the size of the relationships observed in our study was small, which accords with the predominantly small effect sizes observed in previous experimental and cross-sectional studies (Blond, 2008; Hausenblas et al., 2013).
A particularly intriguing finding from our multivariate analyses was that pornography use was not associated with genital dissatisfaction. Given the salience and obvious relevance of genitalia to the form and function of pornography, and given evidence that depictions of genitalia in pornography are often unrealistic (McKee et al., 2008), we expected to find a robust association between pornography use and genital dissatisfaction. Our null finding is consistent, however, with a previous well-controlled study that longitudinally examined the impact of pornography consumption on genital dissatisfaction among 883 mostly heterosexual males and which also found no association between pornography consumption and genital dissatisfaction (Peter and Valkenburg, 2014). Taken together, the results from our study and the study by Peter and Valkenburg (2014) of heterosexual males would seem to suggest that, for males, pornography use does not confer greater risk of developing body image concerns relating to genitalia. Furthermore, while the lack of an association of pornography use with genital dissatisfaction observed in the study by Peter and Valkenburg (2014) could perhaps be explained by their predominantly heterosexual male sample choosing to focus on visual pornographic elements other than male actors’ genitalia, this is a less compelling argument in our study, given our focus on pornography use among sexual minority males. Notably, the findings contradict theories which posit that appearance comparisons produce greater body dissatisfaction when an individual perceives themselves to have little control over that body dimension (Major et al., 1991); certainly, this would more so be the case for one’s genitals than for other body dimensions, including, for example, body fat and muscularity. Additional research is warranted.
Our results were mostly non-supportive of our second hypothesis insofar as participants’ relative use of amateur versus professional pornography did not significantly moderate the relationships of pornography use with six of the seven dependent variables we examined. The exception was the relationship of increased pornography with more frequent thoughts about using anabolic steroids. Specifically, the relationship was stronger for those who watched more professional pornography than those who watched more amateur pornography. Importantly, the finding remained significant following a statistical correction for multiple comparisons, suggesting it was unlikely to be a Type I error. This finding is compelling for two reasons: first, it suggests that the mechanism through which exposure to body ideals contributes to body image and eating disorder psychopathology may also extend to anabolic steroids, and second, the sharp increase in anabolic steroid use in Australia in recent years (Iversen and Maher, 2015) suggests that research examining this mechanism is likely to become more important in the future.
The findings have clinical implications for psychiatrists and mental health professionals who treat clients with body dysmorphic disorder, eating disorders and anabolic-androgenic steroid dependence. Pornography is a substantial component of sexual minority males’ media diet, and, just like traditional forms of media that are more readily recognised as potentially harmful (e.g. movies, television, videogames), there is potential for long-term use of pornography to generate body image concerns and related harmful behaviours. Psychiatrists who treat clients with the above-mentioned disorders ought to examine clients’ pornography use to determine if this is a salient feature of their media diet and/or psychopathology. If deemed salient, clinicians may consider developing their clients’ media literacy, referring to clients’ ability to recognise and critically analyse the idealised bodies featured in various forms of media (Wade et al., 2017). It should be noted, however, that currently available media literacy strategies tend to omit pornography as a potential source of exposure to idealised bodies. Psychiatrists may need to adapt strategies and materials based on traditional media for use in the context of pornography. Finally, psychiatrists may wish to avail themselves of the percentile data presented in Supplementary Table B; these data may help to contextualise clients’ pornography use relative to others. We stress, however, that these data must not be deemed normative or otherwise and that the provision of normative data derived from population samples ought to be a priority for future research. Finally, we note that the findings do not support a statement discouraging pornography use in general; rather, the findings support the clinical utility of examining pornography use among clients who might reasonably be considered vulnerable (i.e. clients with disorders for which body image is a key component).
Limitations of the study are noted. First, the study was cross-sectional, precluding attributions of causality. Second, the findings are specific to visual pornography; other forms of pornography, including, for example, text-only and audio-only pornography, were not examined. Third, the definitions of amateur and professional pornography we supplied to participants, although evidently well understood in our sample, may not generalise to other populations. Fourth, although there is some research suggesting that professional pornography is replete with actors with idealised and unrealistic bodies, there has been no corresponding content analysis of amateur pornography; thus, our contention that amateur pornography contains more realistic bodies is necessarily speculative. Fifth, the sexual minority males in our sample may have been more likely to be experiencing body image and related issues due to the study advertisement explicitly stating that the study was about body image and body change behaviours. Furthermore, our sample likely over-represented younger, single and sexually active sexual minority males. Thus, the degree to which the findings would generalise to the broader population of sexual minority males is uncertain. Sixth, the measure of genital dissatisfaction we created for the study did not include items about genital shape or genital functioning, which may be additional salient aspects of males’ genital dissatisfaction. Seventh, the sample was self-selected. Eighth, our study examined mental health-related quality of life; future research may examine whether pornography use is associated with physical health-related quality of life.
In conclusion, we conducted a study of the prevalence and associations of pornography use among a large sample of sexual minority males living in Australia and New Zealand. We found that increased pornography use was associated with greater dissatisfaction with muscularity, body fat and height; greater eating disorder symptoms; more frequent thoughts about using anabolic steroids; and lower quality of life. Effect sizes for these associations were uniformly small, warranting a commensurate level of concern. Clinicians who treat clients with eating disorders, body dysmorphic disorder, anabolic-androgenic steroid dependence and related disorders ought to consider exploring whether pornography consumption is a salient feature of their client’s psychopathology, and, if present, consider incorporating pornography into a broader strategy of building and improving clients’ media literacy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Scott Griffiths receives funding from the Australian National Health and Medical Research Council (grant number: 1121538)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.