
Abstract
Objectives:
To describe from the perspective of people living with psychotic illness their use of general practitioner services over a 12-month period and the experiences, attitudes and challenges general practitioners face providing health care to this population.
Methods:
A two-phase design was used. Phase 1, screening for psychosis, occurred in public specialised mental health services and non-government organisations within seven catchment sites across Australia. In Phase 2, 1825 people who were screened positive for psychosis were randomly selected for interview which included questions about frequency and reason for general practitioner contact in the 12 months prior to interview. General practitioners (1473) of consenting participants were also surveyed.
Results:
Almost all (90.3%) survey participants had consulted a general practitioner in the 12-month period, on average 8.9 times, and 28.8% of attenders had consulted 12 times or more. The majority (83.5%) attended one general practitioner practice. Most (77.6%) general practitioners wanted to be involved in the mental health care of their patient. Although 69.1% said the management of their patient was not problematic for their practice, one in five general practitioners reported issues related to patient non-compliance with treatment and non-attendance at scheduled appointments; time constraints; and lack of feedback from treating mental health services.
Conclusion:
People with psychotic disorders consult general practitioners, some very frequently. Most Australian general practitioners believe they have a responsibility to review the physical and mental health of their patients. Improved communication between general practitioners and mental health services, and easier access to mental health support, may help general practitioners manage the complex mental, physical and social problems of their patients.
Background
People with psychotic disorders often have complex health problems, with rates of preventable illnesses such as cardiovascular disease, obesity and diabetes higher than general population rates (Hert et al., 2011). A number of lifestyle risk factors, common in people living with psychosis, including smoking (Hahn et al., 2013), cannabis use (Waterreus et al., 2016), a diet low in fruit and vegetables (Dipasquale et al., 2013) and physical inactivity (Nyboe and Lund, 2013), may be contributory factors. Inequality in access to and use and quality of health care may also be contributing to their poor health outcomes (Lawrence and Kisely, 2010; Mai et al., 2011). In an attempt to improve the health of people with severe mental illness, health services around the world are adopting integrated models of care. This is not a new concept. In 1969, Scherl and English described a neighbourhood health centre providing mental health care ‘that is integrated into a system of comprehensive general health care’ and, in 1979, a conference was held in the United States to ‘examine the benefits as well as the potential disadvantages and difficulties in linking mental health services and primary care in a coordinated approach to health care’ (Pardes, 1979). Almost 30 years later, the World Health Organization (WHO, 2008) released Integrating mental health into primary care: A global perspective, a report highlighting the advantages of providing mental health services in primary care and advice on how to implement it. Recently, the Australian Government announced funding for people with severe and complex mental illness to receive integrated health care packages delivered through primary health services and, late in 2016, released the Fifth National Mental Health Plan Consultation Draft which has integration of services as its first priority, with primary health networks essential to supporting service integration (Australian Government, 2016). Furthermore, the Royal Australian and New Zealand College of Psychiatrists (RANZCP) highlighted the importance of communication, collaboration and partnerships between mental health professionals and general practitioners (GPs) in both their clinical practice guidelines for the management of schizophrenia and related disorders (Galletly et al., 2016) and the consensus statement for the treatment, management and monitoring of the physical health of people with an enduring psychotic illness (Lambert et al., 2017).
In Australia, most people see a GP at least once in a 12-month period; commonly making two or more visits a year (Australian Bureau of Statistics, 2011b). However, for a person with a psychotic illness, difficulties managing appointment systems (Lester et al., 2005), feelings of anxiety and stigma when sitting in a crowded GP waiting room (Magin et al., 2013) and symptoms of mental illness including paranoia, depression and negative symptoms may impede GP attendance. In addition, mental illness recognition and treatment may be limited by a number of other factors including people presenting with physical not mental health issues (Reilly et al., 2012), cognitive impairment and co-morbid substance use (Lambert and Newcomer, 2009; Phelan et al., 2001). Despite these obstacles, research shows that people with mental health problems consult GPs more frequently than people without (Knox and Britt, 2004; Reilly et al., 2012) and three quarters of GPs are treating at least three people with a psychotic illness (Lewin and Carr, 1998; Simon et al., 2005). But according to Jones et al. (2015), ‘the evidence that primary care physicians are equipped, resourced and motivated to provide routine medical care to this vulnerable group is lacking’.
Using data collected from a large representative sample of people living in Australia with a psychotic illness, and their GPs, this study aims to describe (1) from the participants’ perspective, their use of GP services over a 12-month period and (2) the experiences, attitudes and challenges GPs face in providing this health care.
Methods
The second Australian national survey of psychosis, Survey of High Impact Psychosis (SHIP), was conducted in 2010, within seven catchment sites across Australia, covering a population of some 1.5 million people aged 18–64 years, approximately 10% of the Australian population in this age group. Its main aims were to estimate the treated prevalence of psychosis for people aged 18−64 years and to describe the characteristics and use of health and other services by people with psychotic illness. A two-phase design was used. In Phase 1, screening for psychosis took place in public specialised mental health services and non-government organisations supporting people with mental illness. This screening identified all people resident in the survey catchment sites and in contact with the above services in the census month (March 2010). A psychosis screener was used to identify individuals likely to meet criteria for formal diagnosis (Jablensky et al., 2000). In addition, administrative records were scanned to identify people resident in the catchment, with a recorded diagnosis of psychosis, and in contact with public specialised mental health services in the 11 months prior to census but not in the census month. In Phase 2, 1825 people who were screened positive for psychosis were randomly selected, stratified by catchment site and age group, for interview and physical health assessment. All participants gave written informed consent for interview, and each were asked to provide separate consent for their GP to be contacted. The Institutional Human Research Ethics Committees at all sites approved the study. Full details of the survey methodology have been published elsewhere (Morgan et al., 2012).
Participant assessments
Each participant had a 3- to 4-hour interview, including a physical assessment, administered by a mental health professional who had undergone extensive training.
Socio-demographic characteristics
Information collected included age, sex, marital status, where and who they were living with and residential postcode. The latter was used to categorise socio-economic status and geographical remoteness using Australian Bureau of Statistics Socio-Economic Indexes for Areas (Index of Relative Socio-Economic Disadvantage) (Australian Bureau of Statistics, 2008) and Australian Standard Geographic Classification – Remoteness Area (Australian Bureau of Statistics, 2006).
Physical health, lifestyle and cognition
Interviewers measured blood pressure, height, weight and waist circumference. Fasting blood samples were taken at accredited pathology laboratories for assays of high-density lipoprotein (HDL), triglycerides and plasma glucose. Metabolic syndrome was defined using the International Diabetes Federation criteria – meeting the threshold for at least three of the five components of metabolic syndrome (elevated waist circumference, blood pressure, triglycerides and glucose, and reduced HDL cholesterol) (Alberti et al., 2009). The WHO body mass index (BMI) reference range was used to classify participants as obese (⩾30), overweight (25–29) or underweight/normal (<25) (WHO, 2000). A list of health conditions was read aloud and participants were asked to indicate which, if any, they had been told by a doctor they had and all prescribed medication taken for at least the previous 4 weeks was recorded. The Alcohol Use Disorders Identification Test (AUDIT; Saunders et al., 1993) was administered and the derived AUDIT-C score (Bush et al., 1998) calculated. A score of 3 or more for women and 4 or more for men indicated hazardous drinking in the previous 12 months. Use of cannabis in the past year and tobacco in the last 4 weeks was recorded. Self-perceived physical health was measured using the question ‘How would you rate your overall physical health?’ with answers on a 5-point scale from excellent to poor and a binary variable created using the categories ‘excellent/very good/good’ and ‘fair/poor’.
The Digit Symbol Coding Test, a brief and reliable test of current general cognitive function from the Repeatable Battery for the Assessment of Neuropsychological Status (Randolph et al., 1998), was administered. The raw score was benchmarked against age-stratified Australian population means (Australian Schizophrenia Research Bank, 2011) and cognitive ability was classified as ‘impaired’ if the score was more than 1 standard deviation below the age-stratified population mean.
Psychopathology and loneliness
The Diagnostic Interview for Psychosis (DIP; Castle et al., 2006), a semi-structured clinical interview, contains items on present, past year and lifetime symptoms including depression, mania, hallucinations and delusions and was used to classify psychotic illness according to the International Classification of Diseases, 10th Revision (ICD-10) criteria. Negative symptoms including poverty of speech, diminished sense of purpose and emotional range present in the 12-month period were rated, but without including aetiological attribution (Kirkpatrick et al., 1989). Loneliness was assessed using a question adapted from the Assessment of Quality of Life instrument (Hawthorne et al., 1999): ‘In the last 12 months have you felt lonely?’ Participants were given the choice of four responses which reflected increasing feelings of loneliness.
GP contact
Participants were asked about GP contact in the 12 months prior to interview including the total number of visits, the number of visits for physical and mental health reasons, the most recent contact, the number of different GPs seen, the ease of getting an appointment and the out-of-pocket cost of visits. Based on responses, participants were classified as non-attenders if they reported no GP consultations in the 12-month period and attenders if they had any GP consultations. Those participants who had visited 12 times or more were considered frequent attenders.
GP questionnaires
Nominated GPs were mailed two questionnaires with reply paid envelopes (Figure 1). Questionnaire 1 comprised a series of tick box questions asking about past 12-month contact with the named participant. It included questions about the usual length of and reason for consultations, whether they had noted any adverse effects of antipsychotic treatment, whether they had treated or referred the participant for any metabolic, cardiovascular or kidney problems, and any difficulties and challenges they had in managing the patient. It also asked about their interactions with mental health services regarding this person. GPs who did not return the questionnaire were mailed a second time. After completion of participant interviews, Questionnaire 2 was mailed to the nominated GPs. This questionnaire inquired about their overall treatment and management of psychosis in general practice, collaboration with mental health services, attitudes to roles and responsibilities, mental health skills and training, and what GPs thought would help them to better manage patients with a psychotic disorder in their practice.
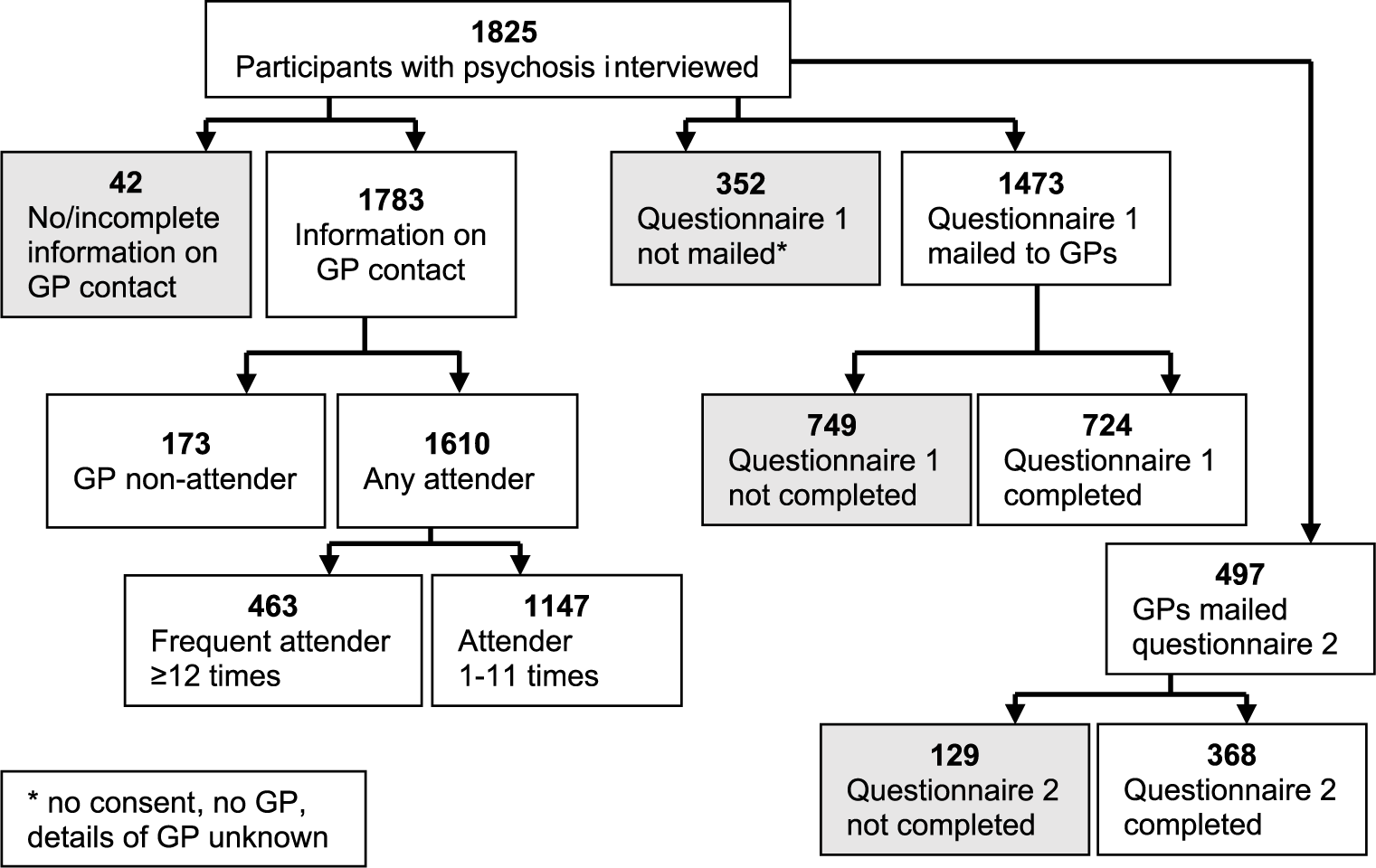
Flow chart illustrating sample selection from the SHIP study for the present sub-study.
Statistical analysis
Socio-demographic characteristics and physical and mental health profiles were summarised for participants in the GP non-attender, any attender and frequent attender groups using descriptive statistics. For discrete variables, chi-square tests of association were run to highlight any significant differences in characteristics between non-attender and any attender and frequent and less frequent groups. Analysis of variance was used to assess differences in means for continuous variables. GPs’ responses were summarised using descriptive statistics. Analysis was performed using SPSS (version 21).
Results
A total of 1783 (97.7%) of the interviewed participants provided information about their contact with GPs in the previous 12 months. Most (90.3%) participants had consulted a GP in the 12-month period; this was higher than the figure of 79.0% for the general population aged 15–64 years (Australian Bureau of Statistics, 2011a). Further comparisons with the Australian general population are provided in Figure 2 (Australian Bureau of Statistics, 2011b). A significantly greater proportion of females than males had seen a GP (94.3% vs 87.6%; p < 0.001) in the past 12 months, and the proportion who did increased with age. Over half (55.6%) of all participants had seen a GP at least once in the 4 weeks prior to interview (Figure 3). Only 5.8% of people indicated they had made a visit to a hospital emergency department because they could not get an appointment to see a GP.
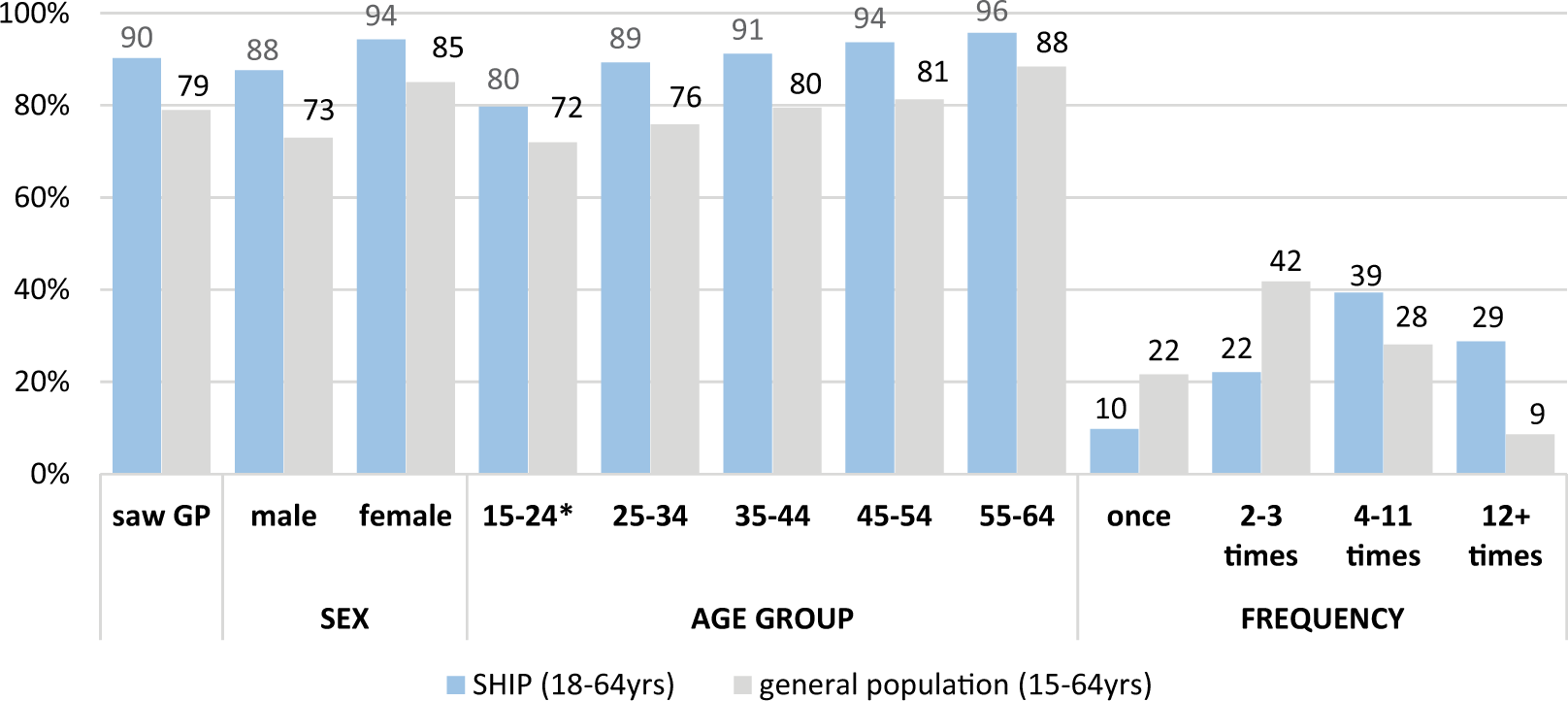
Comparison of GP consultations in the last 12 months between SHIP participants (aged 18–64 years) and the Australian general population (aged 15–64 years)*.
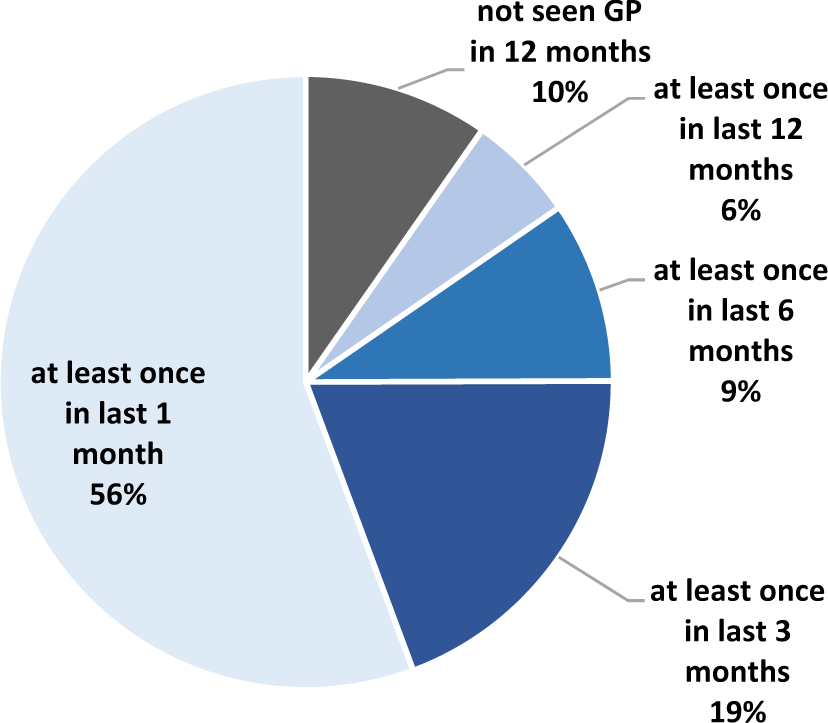
Recency of GP contact in the last 12 months.
Characteristics of GP attenders
The mean number of visits to a GP was 8.9 annually (median: 5, range: 1–60) compared to 5.3 for the general population (Britt et al., 2010). The majority (64.5%) of GP attenders said they saw the same GP at each visit, while a further 19.0% saw multiple GPs who worked in the same practice. Most (93.2%) saw a bulk billing GP. Three quarters (74.1%) said they had no difficulty getting a routine appointment within a few days and 58.4% indicated they could get an urgent appointment on the same day.
Participants cited visiting a GP more frequently for physical rather than mental health reasons (86.5% and 55.0%, respectively). Musculoskeletal problems such as back, knee or foot complaints or injuries were the most common reason given for a physical health consultation, while the most common reason for a mental health consultation was medication-related, for example, to collect a prescription or to review or discuss side-effects (Figure 4).
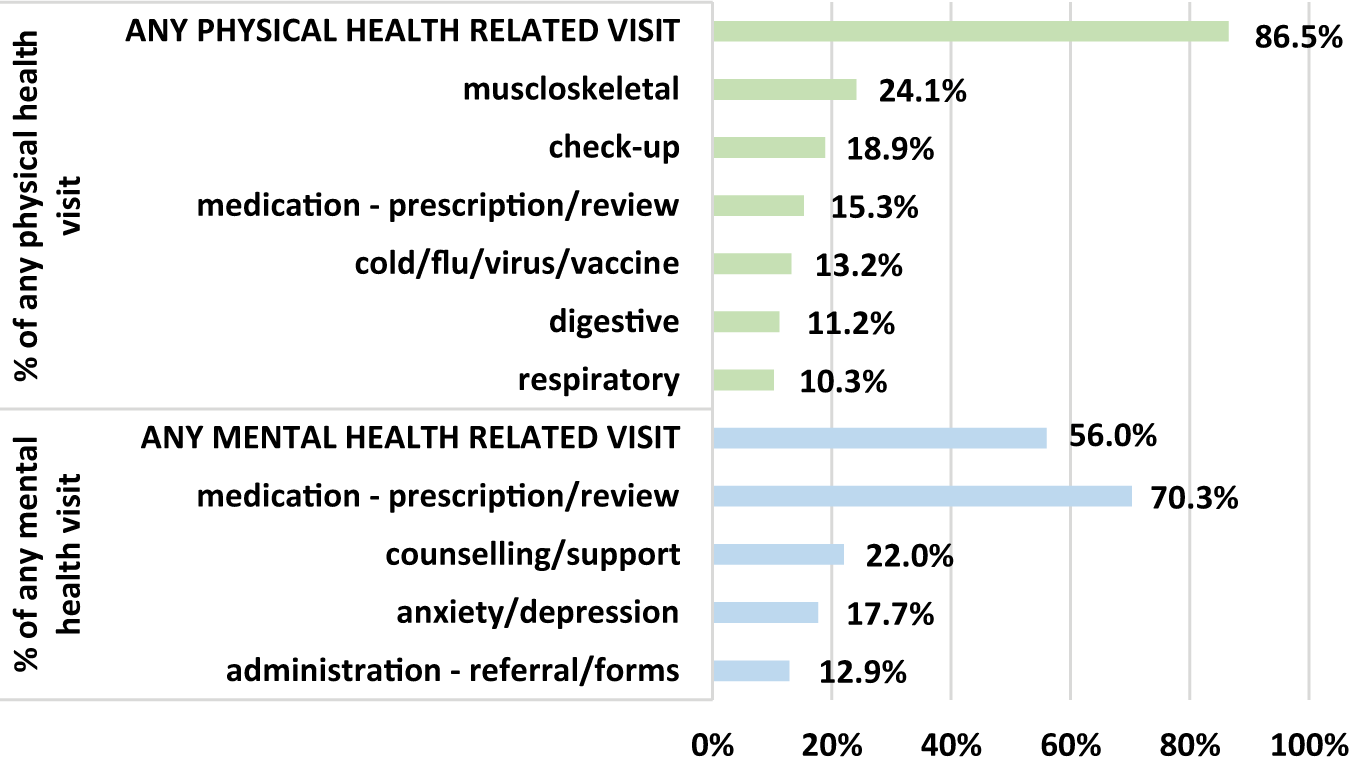
Most frequent physical- and mental-health-related reasons given by participants for consulting with a GP in the past 12 months.
Frequent attenders
Frequent attenders (those who had consulted a GP 12 times or more in the 12-month period) represented 28.8% of all GP attenders in contrast to only 9% of the general population (Figure 2). Compared to participants who had made fewer visits, frequent attenders were more likely to be older, living alone, feeling socially isolated and lonely, with impaired cognitive function and experiencing greater socio-economic disadvantage. They were also more likely to suffer from chronic physical health problems, to perceive their physical health as poor and to have experienced hallucinations, depression and suicidal ideation in the previous 12 months (Table 1).
Characteristics of survey participants by 12-month GP contact.
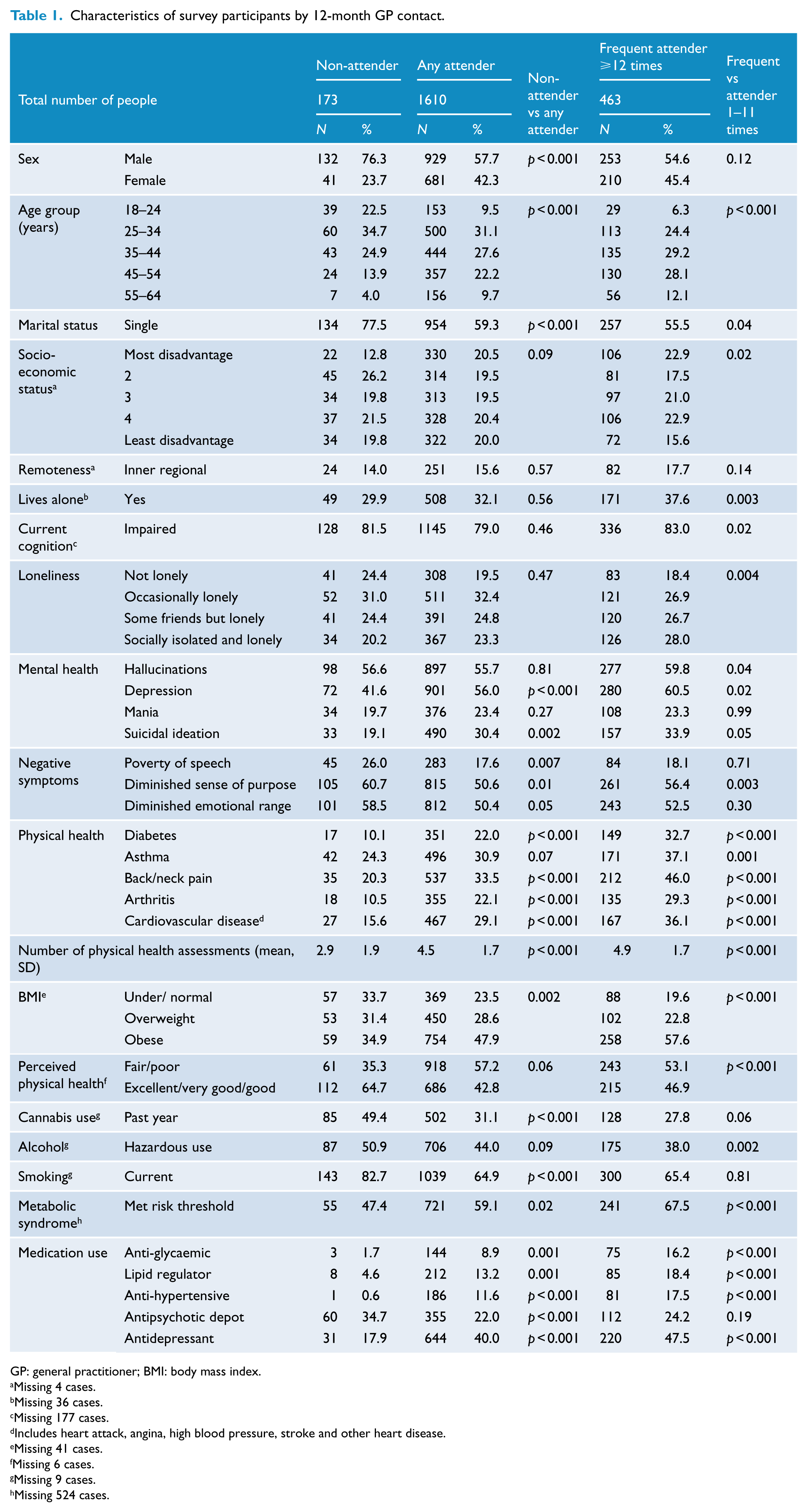
GP: general practitioner; BMI: body mass index.
Missing 4 cases.
Missing 36 cases.
Missing 177 cases.
Includes heart attack, angina, high blood pressure, stroke and other heart disease.
Missing 41 cases.
Missing 6 cases.
Missing 9 cases.
Missing 524 cases.
Characteristics of non-attenders
One in 10 people (9.7%) reported having no contact with a GP in the previous 12 months. These non-attenders were more likely to be young, single, male, to smoke tobacco and use cannabis. They were less likely to report suffering from chronic physical health conditions, although 47.4% met the risk threshold for metabolic syndrome. Non-attenders were more likely than GP attenders to have had negative symptoms, including poverty of speech, diminished sense of purpose and diminished emotional range in the 12-month period (see Table 1). The most common reasons given for not seeing a GP were as follows: ‘I am never sick’ (67.6%), ‘I never think about it’ (32.9%) and ‘I have too many other problems’ (11.0%). Only 3.5% indicated that cost was a barrier to consulting a GP.
GP experiences managing SHIP participants
A total of 1473 (80.7%) participants could name their current GP and gave consent for them to be contacted. Almost half (49.2%) of the questionnaires mailed out to GPs were completed. Of the remaining 352 participants, most had no GP (273), did not give consent (70) or could not provide GP details for contact (9). The mean number of GP visits per participant in the 12-month period was 11.7 (median: 9, range: 1–70). GPs reported that for 65.4% of participants, the usual length of a consultation was between 10 and 19 minutes, with only a small proportion (4.5%) usually having an appointment of 30 minutes or more; 10.4% usually had short consultations (10 minutes or less). Participants seeing a GP 12 times or more were significantly more likely to have shorter consultations (lasting less than 10 minutes) than participants consulting less frequently (χ2 = 15.17, p = 0.002) (Figure 5). More than half (55.6%) the GPs indicated they ‘usually’ had enough time in a consultation to deal with the participants’ mental health problems, with 32.4% reporting this was the case only ‘sometimes’, while 9.3% said they ‘never/rarely’ had enough time.
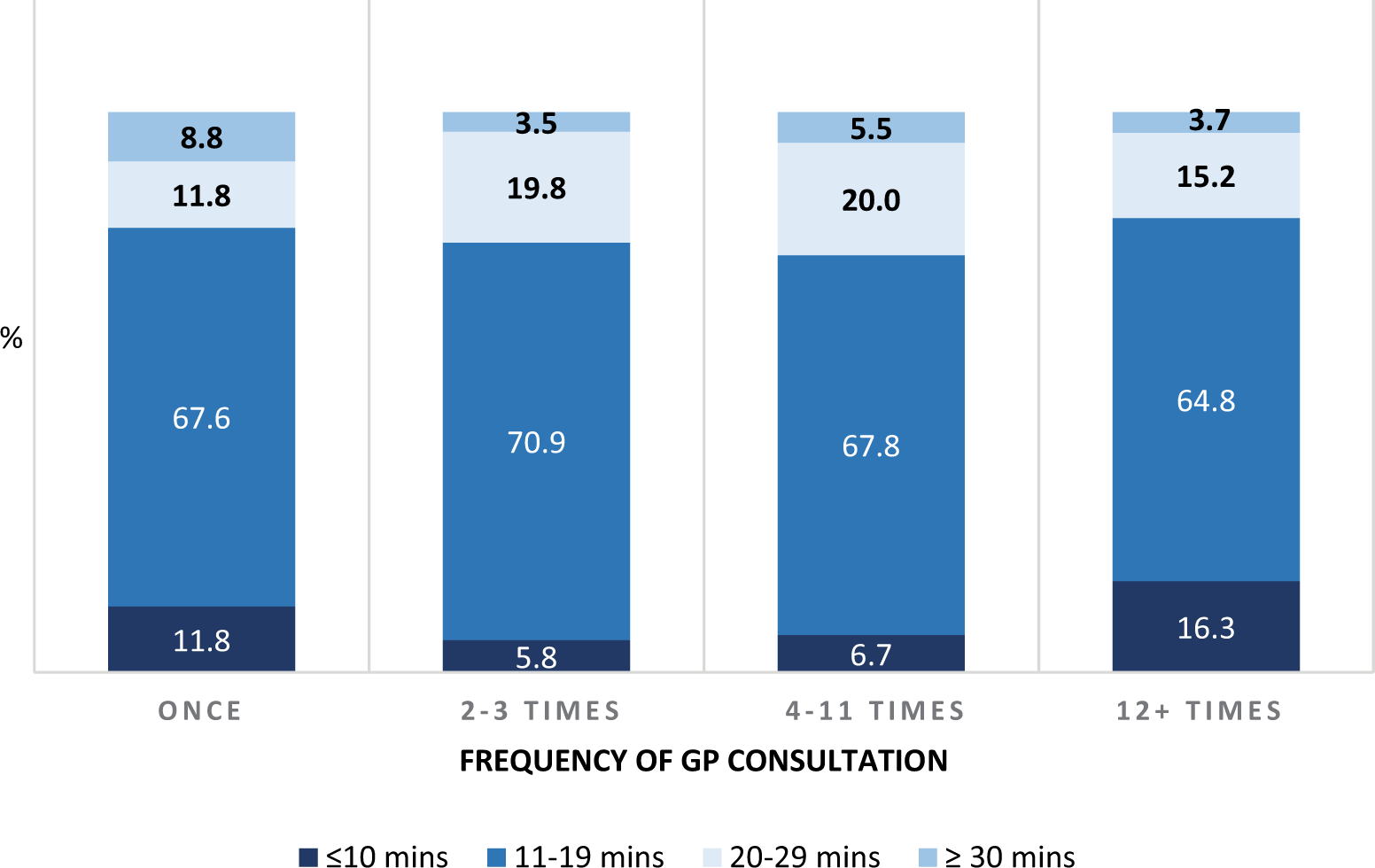
Frequency of past 12-month GP contact and usual length of consultation.
In the previous year, 42.6% of GPs had encountered side-effects of long-term antipsychotic treatment in their patient, most commonly weight gain. One-third (32.2%) had treated a participant for metabolic, cardiovascular or kidney problems and 11.4% had referred a participant for specialist treatment. Most (77.6%) GPs said that they wanted to be involved in the mental health care of their patient with a psychotic illness. As many as 10.2% indicated that they were currently treating the participant exclusively, not in collaboration with a mental health team. While 69.1% of GPs felt the management of the survey participant was not problematic for their practice, others highlighted a number of factors that contributed to difficulties in management. The most commonly reported factors included the following: non-compliance with treatment (noted by 22.1% of GPs), non-attendance at scheduled appointments (20.7%), time constraints (22.1%) and lack of feedback from treating mental health service providers (20.0%). Related to lack of feedback, almost two out of five GPs (37.4%) had not received any formal correspondence from a mental health team in the previous 12 months regarding the participant. However, of those GPs who had, 85.0% felt the correspondence was adequate.
Managing psychosis in general practice
A total of 368 (74%) GPs completed the second questionnaire which covered general management of psychosis in their practice. GPs who responded were more likely to be seeing a greater number of survey participants than those who did not respond, with one-third (36.1%) indicating that they had treated 10 or more patients with psychosis in the past 12 months. While only 4.1% of GPs reported that they had a post-graduate qualification in mental health, the majority (66.6%) had attended at least one mental-health-related workshop or seminar in the previous 12 months (Table 2). A small proportion (10.9%) of GPs felt that they did not have the skills and knowledge to treat patients with a psychotic illness in their practice but almost all (96.7%) believed they had a responsibility (shared or exclusively) to review the physical and mental health of patients with psychosis. However, 75.8% said they had no clear system for reaching agreement with secondary care services on the responsibility for reviewing patients.
Skills, resources and motivation of GPs to provide routine medical care to people with a psychotic illness (N = 368).
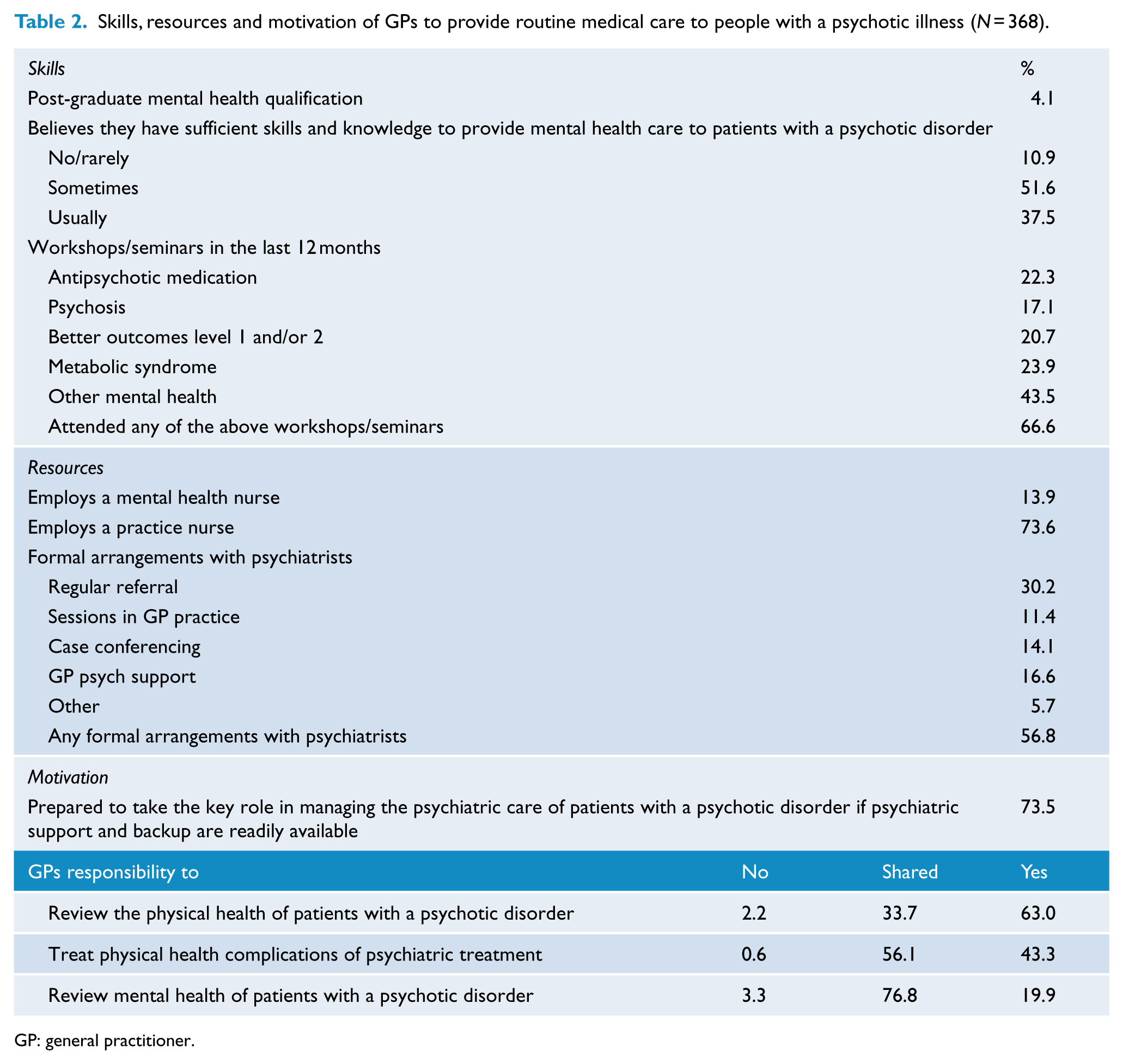
GP: general practitioner.
In the previous 12 months, 82.6% of GPs had had at least one patient with a psychotic disorder referred back to them and 84.5% had developed a mental health care plan for a patient. Few (13.9%) GPs employed a mental health nurse, but almost half (49.3%) had some formal arrangement with a psychiatrist. For example, 11.4% had a psychiatrist conduct sessions in the GP practice and 14.1% undertook case conferencing with a psychiatrist. The majority (85.3%) had referred patients to a psychologist and 43.2% to a non-government organisation for help, support and information.
Three quarters (73.1%) of GPs indicated they were prepared to take the key role in managing the psychiatric care of their patients with a psychotic disorder, if psychiatric support and backup were readily available. However, a similar proportion (73.4%) reported experiencing difficulties interfacing with the mental health services to obtain an assessment or treatment for a patient with a psychotic disorder; one in four (23.9%) said this occurred often. The final question (free text) asked GPs what they thought would help them to better manage patients with a psychotic disorder in their practice. Of the 259 GPs who responded to this question, the majority (80.7%) of comments referred to mental health services; most frequently, these related to the need for easier access to mental health services (Table 3). One-third (33.6%) highlighted areas in their own practice including having more time to allow for longer consultations, the need to employ a mental health nurse or mental health trained practice nurse and updating skills regarding psychosis management and medication.
What GPs feel would help them to better manage their patients with a psychotic disorder including direct quotes (N = 259).
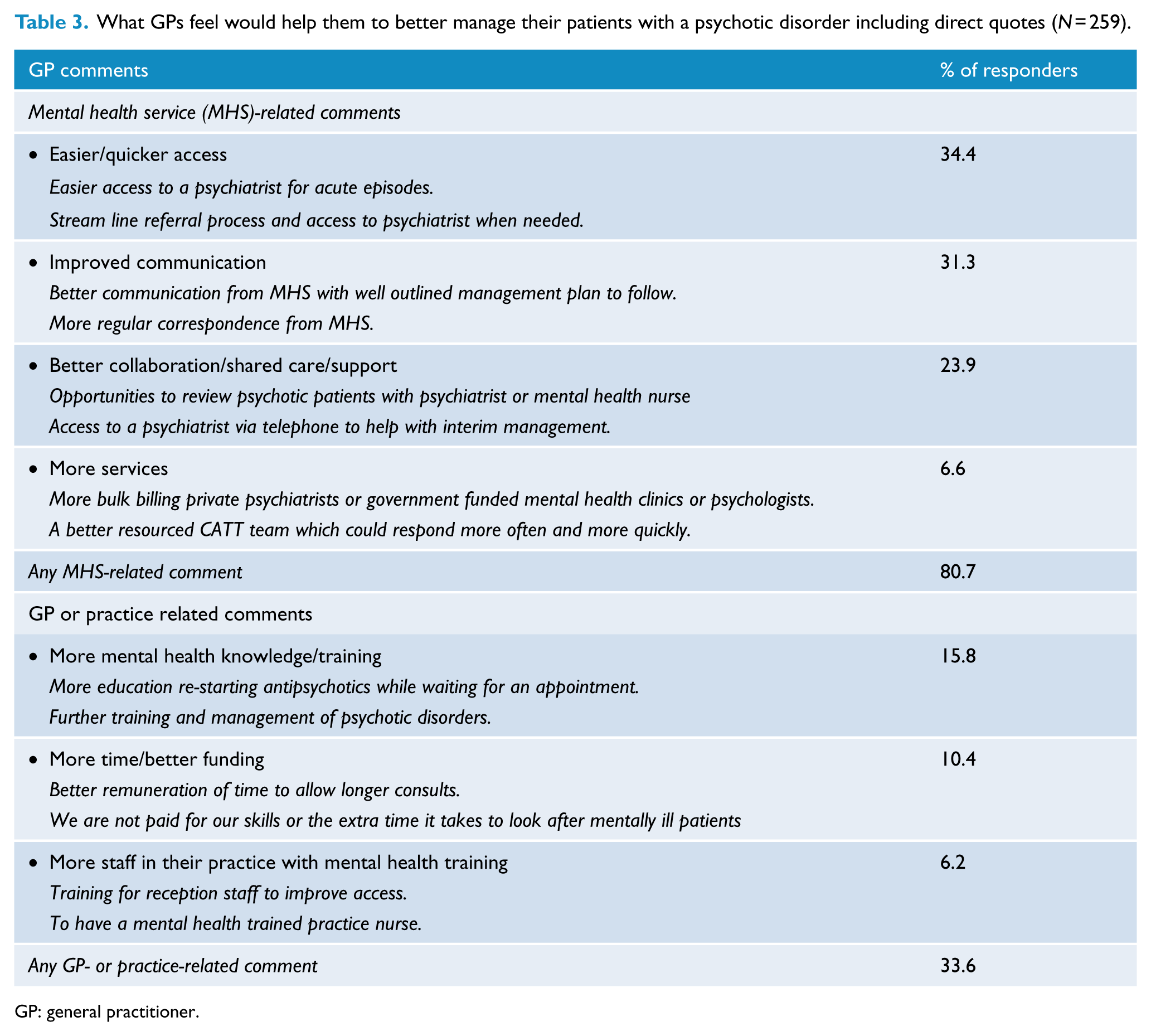
GP: general practitioner.
Discussion
‘GPs need to have an interest in patients’ mental health. Psychiatrists need to have interest in patients’ physical health’. Comment from SHIP participant.
This large Australian survey found that since the first national survey of psychosis in 1997/1998, the use of GP services by people living with a psychotic illness has increased from 76.7% to 90.3% (Raudino et al., 2014) as part of a shift from inpatient to community-based care. Each year, people with a psychotic illness consult GPs 8.9 times on average, with almost one-third (28.8%) making 12 or more visits over this period. Most people (83.5%) chose continuity of care and attended only one GP practice, although this is slightly lower than for the general Australian population (93%) (Menzies Centre for Health Policy and Nous Group, 2012). While it was more common to consult with a GP regarding a physical-health-related issue, more than half the participants indicated they had seen a GP regarding a mental health issue. People with a psychotic illness living in regional Australia were no less likely to see a GP than those in a major city. Moreover, no differences were seen across socio-economic groups.
In keeping with findings from general population studies (Ellaway et al., 1999; Knox and Britt, 2004; Van Steenkiste et al., 2010; Young et al., 2005), we found that SHIP participants with chronic physical health problems including diabetes, obesity, back complaints, depression, loneliness and poor perceived physical health made more visits to a GP than those in better health. Our results also showed that frequent attenders reported receiving a significantly greater number of physical assessments including having blood pressure, waist and weight measured, eye sight, hearing and teeth checked and blood tests, than those attending less frequently. This frequent attendance may reflect better management and monitoring of the complex social, physical and mental health problems which many of these participants experience, but it places considerable demands on a GP’s time and resources. Across Australia, between 2009 and 2012, there was a 20% increase in the number of nurses working in general practice, (Australian Medicare Local Alliance, 2012) with 73.6% of the GPs in the SHIP study employing at least one nurse. With professional development, these practice nurses could extend their scope of patient care to include the routine clinical management of chronic diseases in people with mental health problems (Young et al., 2016).
Of concern is the small proportion of people who had not seen a GP in the previous 12 months. Although they were more likely to be younger and less likely to report suffering from chronic physical health conditions than those participants who had seen a GP, almost half met the risk threshold for metabolic syndrome (47.4%), used cannabis (49.4%), drank alcohol at hazardous levels (50.9%) and 82.7% smoked. Although two-thirds (67.6%) of non-attenders indicated the reason for not seeing a GP was that they were never sick, they were more likely to experience negative symptoms than attenders which may act as a barrier to them accessing GP care. In addition, co-locating GP services in or adjacent to mental health services may remove actual or perceived barriers to GP attendance.
We found most Australian GPs surveyed believe they have a responsibility to review the physical and mental health of their patients with severe mental illness, and 2010 data from the BEACH survey (Britt et al., 2010) showed that 11.7% of all GP encounters were mental-health-related. While very few had a post-graduate qualification in mental health, two-thirds had attended at least one mental-health-related workshop or seminar in the previous 12 months, more than half employed a mental health nurse or had some formal arrangement with mental health services including having a psychiatrist conduct sessions in the practice and the majority felt they had the skills and knowledge to treat patients with a psychotic illness. Three quarters indicated they are prepared to take the key role in managing the psychiatric care of their patients if they are supported by the mental health services. Effective communication between all health service providers is critical, but previous research indicates that mental health specialists feel the referral information they receive from primary care is insufficient (Hartveit et al., 2017), while GPs feel it takes too long to receive feedback from the specialist (Vermeir et al., 2015); this is similar to the findings reported here. With the aim of improving patient outcomes, the Royal Australian College of General Practitioners (RACGP) has published guidelines on best practice principles for effective communication between medical and mental health professionals (The General Practice Mental Health Standards Collaboration, 2016). The RANZCP clinical practice guidelines for the management of schizophrenia and related disorders also highlight the importance of regular communication with the GP including providing clear written information and the treatment plan (Galletly et al., 2016).
Several limitations to this cross-sectional study should be noted. It is likely that there has been some under-reporting of GP service use by participants. Information gathered relied on their recalling use of GP services over a 12-month period. A long time period and increased frequency of use have been found to be susceptible to under-reporting (Bhandari and Wagner, 2006; Marshall et al., 2001). It is also likely that there has been a response bias in the GP questionnaires returned, with GP responders more likely to see a greater number of SHIP participants than non-responders. As a result, GP responders may reflect those with more skills, experience and interest in managing psychotic illness in their practices. However, as we did not gather any data on GP non-responders, we are unable to comment further.
Each year, people with a psychotic illness are consulting GPs, some very frequently and many with complex mental, physical and social issues which may require longer consultations. This study has shown that in 2010, many GPs had the resources and were motivated to provide care to people living with psychotic illness. The successful implementation of new, integrated health care packages and Government initiatives including Better Access, Health Care Home, the Mental Health Nurse Incentive Program and the adoption of recommendations in the RACGP (The General Practice Mental Health Standards Collaboration, 2016) and RANZCP guidelines and consensus statement (Galletly et al., 2016; Lambert et al., 2017) will require a better partnership between mental health services and primary care, including enhanced communication, agreement on pathways to care and whose responsibility it is to do what and when, and easier access to support from mental health services for GPs.
The current situation is best summed up by this comment from a GP: ‘This is a very rewarding area to work in when things are going well, but as a GP I can feel stranded if things start to deteriorate’.
This study was undertaken prior to many of these health service changes, which were put into practice to improve quality of care and access to that care for people with mental health problems. Five years after their participation in SHIP, the West Australian participants and their GPs have been surveyed again. Data from the SHIP survey will form the benchmark against which data from the second survey will be compared and the impact of these changes evaluated.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group at the time of the Survey were as follows: V Morgan (Project Director); A Jablensky (Chief Scientific Advisor); A Waterreus (Project Coordinator); A Mackinnon (Statistician); R Bush, D Castle, M Cohen, C Galletly, C Harvey, P McGorry, J McGrath, and H Stain (Site Directors); V Carr (Australian Schizophrenia Research Bank); A Neil (Health Economics); B Hocking (SANE Australia); and S Saw (Australian Government Department of Health and Ageing). This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders and their GPs who gave their time and whose responses form the basis of this publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.