
Abstract
General practitioners (GPs) play a pivotal role in managing migraine and ensuring that patients have a positive first experience when seeking treatment. A large proportion of migraineurs do not consult a GP, preferring to rely on over-the-counter remedies to reduce pain and disability. For those who do consult, receiving a satisfactory outcome at their first consultation is important for ensuring subsequent effective management of their migraine. If patient expectations are not met at their first visit (prescribed treatment is ineffective or GP does not empathize with their suffering), patients may not return for further consultation. There remains a need to improve migraine diagnosis and treatment, and GPs require continuing medical education and neurologist support to ensure that they are providing the best migraine treatments and outcomes. More widespread use of diagnostic tools, standardized management guidelines and individualized treatment regimens will help GPs successfully manage both migraine symptoms and patient expectations.
Introduction
Migraine is a widespread, chronic and intermittently disabling disorder characterized by recurrent headaches with or without aura. It is estimated that approximately 11% of the adult population worldwide are affected by migraine (1), and it occurs with the highest prevalence between the ages of 25 and 55 years (2). Triggers for migraine include foods, hormonal changes, and stressors (3, 4), and migraine has an enormous impact on the physical, mental and social aspects of the health-related quality of life of sufferers (5–7).
Patients seeking assistance with migraine most often present to their general practitioners (GPs); therefore, GPs have a pivotal role to play in the diagnosis and treatment process (8). However, many patients with migraine (approximately 40–63%) (9–11) do not consult their GP, preferring to rely instead on over-the-counter (OTC) remedies to reduce their pain and disability (10). For those migraineurs who do consult their GP, a satisfactory outcome at their first consultation is of paramount importance to ensure subsequent effective management of their migraine (12). If patient expectations are not met, i.e. if their prescribed treatment is ineffective or the GP does not appear to empathize with their suffering, patients may not return for further consultation (10, 12).
Here we discuss how GPs can ensure that patients have a positive first experience when seeking treatment for migraine, and examine the tools available to assist in the accurate diagnosis and effective management of migraine pain.
Migraine management
Migraine and GPs—missed opportunities?
Although migraine is widespread in the general population, studies have indicated that only a minority of migraineurs are being actively managed by their GPs (12, 13). In a French study, all patients who presented during surgery hours to 49 GPs on a single day were asked to complete a questionnaire prior to their consultation (14). Responses were obtained from 696 patients, of whom 176 (25%) were identified from their questionnaires as being migraineurs. Of these, only 71 (40%) were recognized as migraineurs by their GPs and only 50 (28%) were being actively managed. The high proportion of migraine sufferers that remains unrecognized and untreated may be related to statistics showing that < 50% of migraineurs consult a physician about headache (15). Studies in France have shown that 40% of migraine sufferers have never consulted a GP, whereas of those that have, a further 40% have lapsed, leaving just 20% currently in consultation (12, 13). A similar situation is indicated by data obtained from other European countries and the USA (16).
In a recent study, it was found that 40.8% of migraine sufferers did not consult their GP because they treated their headache themselves with OTC medications, and 33% of migraineurs were satisfied with the OTC remedies that they used (17). However, some (18%) of the patients also believed that consultation with their GP about migraine would be of no benefit to them (Fig. 1). Such data are consistent with findings from previous studies, in which patients reported a low level of confidence in the ability of their GP to manage migraine (10). While 12% of patients believed that their GP's knowledge of migraine was poor or very poor, approximately one-third (33%) also believed that the information provided by their GP on different migraine treatment options was inadequate (18).
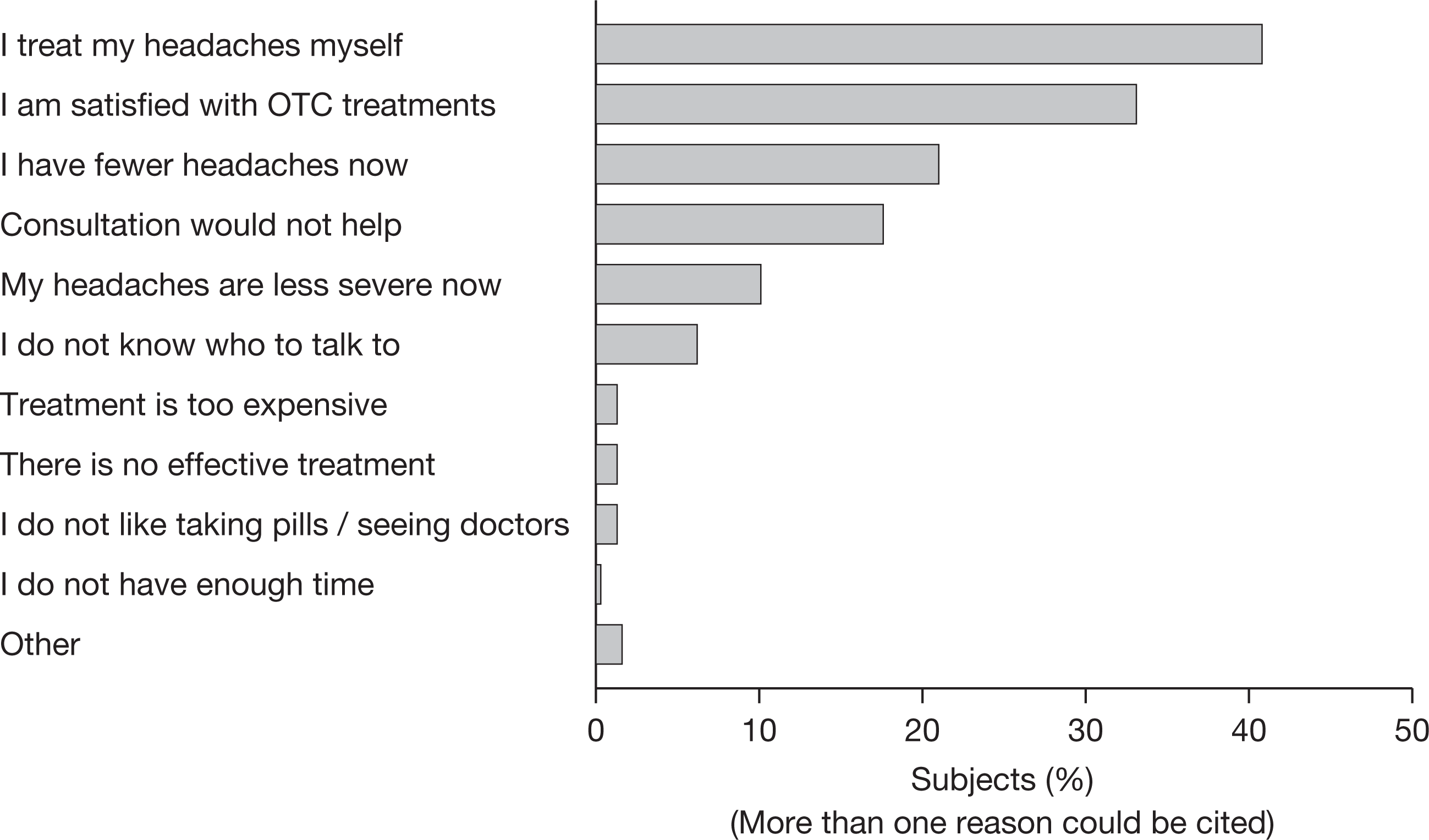
Reasons for not consulting for migraine headache (17). OTC, over-the-counter.
Given that many migraine sufferers admit to self-medication with OTC remedies, it is no surprise to learn that most migraineurs (60%) in the general French population use paracetamol to treat their acute migraine (13). This is despite the fact that paracetamol is not recommended for migraine, since it does not provide significant relief of migraine pain at 2 h in almost one-third (30%) of patients, and often several doses of paracetamol are required to reduce pain (12, 19). Other non-specific medications such as aspirin and non-steroidal anti-inflammatory drugs (NSAIDs) are known to be used by 29% and 28% of migraineurs, respectively (13). Opiates, which are also not recommended for migraine treatment but are generally marketed in France in fixed combinations, are used by 23% of migraine patients (13). However, of those patients using opiates, 38% did not have significant pain relief at 2 h, 44% required several doses, and 28% did not regain rapid functional ability (12). In contrast, migraine-specific medications such as triptans are used by only 8% of the general French population (13). Such widespread use of OTC remedies may also account for the fact that 56% of French migraineurs suffering from chronic daily headache fall into the category of multiple medication overuse (20), and many patients suffer from adverse events, drug interactions and analgesic-rebound headaches, which could have been avoided with appropriate medical management (21). Clearly then, the first step towards better, more effective treatment of migraine and reduction of migraine-associated disability is to encourage migraineurs who need medical care to seek it.
The importance of a positive first experience
Most patients seeking assistance for migraine initially present to their GPs, and only 4% consult headache specialists or pain experts (22). Migraineurs managed in primary care do not differ significantly from those referred to neurologists in terms of headache disability, impact on functioning, comorbid anxiety or depression, and satisfaction with care (23). However, those patients referred to a neurologist do consult more frequently than those managed by a GP (23).
The quality of the first consultation is a major determining factor in whether patients will continue to consult. Diagnosis must be accurate and effectively communicated to the patient (24), while effective and well-tolerated treatment must be prescribed. A recent French study has demonstrated that of those patients who remain in consultation, significantly more (44%) are prescribed a recommended acute treatment at the first consultation, compared with just 33% of patients who subsequently lapse (P < 0.01) (12). Patients must also feel that their GP understands the severity and impact of their condition. If patient expectations are not met, they are unlikely to return for further consultations. Physicians must therefore manage patient expectations by providing both information and empathy, and by gaining the trust of the patient through effective communication (10).
Currently, for many patients and GPs, the first consultation is time-consuming, limiting the opportunity to establish a meaningful therapeutic relationship, and potentially reducing the probability of an accurate diagnosis and treatment selection (25). During the average 7–10-min consultation, GPs have to complete a complex series of tasks, including: taking a history and examining the patient; making a clinical diagnosis and considering a broad treatment strategy; explaining the selected treatment, likely outcome and possible side-effects to the patient; and recording the details of the consultation (26). In this scenario, the patient is often a passive recipient, increasing the likelihood of later dissatisfaction if the recommended treatment is less efficacious than expected. One way to make the first consultation less time-consuming is to give the patient a questionnaire to complete, allowing the GP to review the questionnaire later when a longer consultation is available. In this scenario, the first consultation allows the GP to provide the patient with information about headache, migraine and the treatment options available. The second consultation then allows more detailed examination and discussion as to the most beneficial management strategy for the patient (26). This direct patient involvement results in a more balanced therapeutic relationship (27) and may improve treatment outcomes and give patients more realistic expectations (10).
In order to achieve patient satisfaction during the consultation process, GPs require tools to improve migraine diagnosis and to assess the impact of migraine pain on the patient. It is also important for them to have an understanding of the most appropriate treatments available, the ability to communicate the benefits of these to patients, and viable strategies to reduce the risk of disease progression.
Accurate diagnosis of migraine
In order to improve satisfaction with migraine treatment, GPs must first increase the rate of diagnosis amongst migraineurs—this lays the foundation for subsequent treatment strategies and provides an opportunity to educate and reassure patients (24). The International Headache Society (IHS) has produced the International Classification of Headache Disorders, 2nd edition (ICHD-II), which is now widely used throughout the world to standardize diagnosis of migraine (28). The diagnostic criteria of ICHD-II include the minimum number of attacks over a lifetime, typical headache duration, typical headache characteristics and non-pain-associated symptoms. ICHD-II also allows differentiation between chronic migraine (which fulfils all of the criteria) and probable migraine (fulfils all but one criteria).
In the clinic, diagnosis may be facilitated by the use of brief, simple and easy-to-use screening tools, such as the ID-migraine screener, which has been comprehensively validated in migraine sufferers (29). Of nine diagnostic questions in this self-administered screener, a three-item subset of nausea, disability and sensitivity to light provides the most accurate diagnosis of migraine, compared with a diagnosis based on the IHS classifications (Fig. 2). If patients respond positively to two out of the three symptoms in this subset of the ID-migraine screener, they have an 81% probability of having migraine, whereas patients who report all three symptoms have a 93% probability of meeting the IHS diagnostic criteria for migraine. This ID-migraine subset, known as ‘PIN’—photophobia, inability to function and nausea—is, therefore, a reliable tool that may improve migraine recognition in primary care (30).

The ID-migraine screener: adjusted odds ratio of a diagnosis of migraine given that a headache feature is present (30). Reprinted by permission. Lipton RB, Bigal ME. Ten lessons on the epidemiology of migraine. Headache 2007; 47 (Suppl. 1):S2–9.
Migraine impairment and disability
In addition to diagnosing migraine, GPs must also appreciate that migraine causes significant impairment in sufferers. Assessing migraine-related impairment is crucial, for these reasons: it improves doctor/patient communication; it allows patients to recognize for themselves the impact that migraine has on their lives and thus increases their motivation to seek medical care; and it provides a basis for predicting treatment need (30). Migraine-related impairment should be considered from both emotional and functional perspectives.
Emotional impact
It is important for GPs to recognize that migraine has an emotional impact on the sufferer and is often associated with comorbid conditions such as anxiety and depression. In the FRAMIG study of the general French population, significantly more subjects with migraine scored highly (> 7 on the Hospital Anxiety and Depression Scale) for anxiety and depression compared with non-migraine subjects (P < 0.01 for both) (9). Indeed, 51% of patients with migraine were found to exhibit symptoms of anxiety and/or depression, with 28% having only anxiety, 4% only depression and 19% suffering from comorbid depression and anxiety (31). Similar results were obtained in the recent SMILE study, in which 67% of migraineurs in the French primary care population were found to have symptoms of anxiety or depression, or both (32). Anxiety has been shown to be associated with more severe migraine attacks (higher frequency, higher intensity and greater functional impact). Patients with comorbid anxiety have a lower migraine-specific quality of life (MSQ4) score compared with non-anxious patients (45.1 vs. 60.8; P < 0.01) and a higher rate of treatment ineffectiveness (78.0% vs. 64%; P < 0.01) (33).
Functional impact
Assessment of migraine-related functional impact must also be improved. In a sample of 3168 GPs in Spain, 85% reported the importance of assessment of functional impairment in order to improve migraine management, but only 16% admitted using functional impairment assessment scales (34). Optimal migraine management requires brief self-administered questionnaires to quantify migraine-related disability or impact, such as the Headache Impact Test (HIT-6) (35) or the Migraine Disability Assessment Scale (MIDAS) (36).
The HIT-6 is a six-item questionnaire that yields an impact score, allowing patients to be assigned to one of four grades: little/no impact (grade 1); moderate impact (grade 2); substantial impact (grade 3); and severe impact (grade 4). In a French study of primary care patients, those subjects whose migraine was recognized by their GP had a higher mean HIT score than those in whom migraine had not been recognized (P < 0.001) (14). Although a larger proportion of patients with severe impact were recognized to have migraine, 70% of patients with substantial functional impact and 43% of patients with very severe impact were not recognized by their GPs as migraine sufferers (Table 1). However, the mean HIT score and grade distribution were not associated with the rate of migraine management in those patients whose migraine was recognized (Table 1).
Assessment of migraine-related functional impairment (14)
MIDAS allows assessment of migraine-related disability retrospectively over 3 months, scoring in intuitively meaningful units of lost days and using five questions to consider three life domains: paid work and education; household work; family, social and leisure activities (36, 37). It stratifies migraineurs into four grades of severity: grade I (scoring 0–5, minimal or infrequent disability); grade II (6–10, mild or infrequent disability); grade III (11–20, moderate); and grade IV (≥ 21, severe). It also helps the physician to select treatment based on individual patient need. Many migraine patients with low MIDAS grades (I–II) find relief of symptoms with simple analgesics or combination therapies. Some, however, experience infrequent but severely disabling migraine attacks requiring specific, acute migraine therapy (e.g. with a triptan) for effective relief. Patients with moderately or severely disabling migraine (MIDAS grades III–IV) require specific, acute migraine therapy for effective relief and restoration of function.
Tailoring treatment to patients
Not all migraines are the same, and it is therefore important that GPs tailor their treatment to individual patients using a stratified-care regimen, rather than prescribing the same non-specific analgesics to all (8). This would reduce both the risk of overuse of non-specific pain-relieving agents and the risk of side-effects associated with NSAIDs (38), as well as improving patient outcomes. In a step-care regimen, treatment is escalated after first-line medications fail, but this strategy may lengthen the time that patients must wait before obtaining effective treatment, and can delay the onset of pain relief and return to normal function (Fig. 3) (39). In a stratified-care regimen, physicians can use the MIDAS or HIT-6 tools to classify patients based on their level of disability and are therefore better able to predict treatment needs (40). A low MIDAS or HIT score indicates that the patient is less likely to require escalating treatment and more likely to benefit from low-end therapy. A high score, however, suggests that patients will respond better to more specific treatments, such as triptans (30).

Step-care and stratified-care treatment regimens (8). Treatment should be individualized using a stratified-care regimen, to provide the right treatment for the right patient. SA, simple analgesic; NSAID, non-steroidal anti-inflammatory drug; MIDAS, Migraine Disability Assessment Scale.
Preventing migraine progression
It has been known for several years that patients who initially present with episodic migraine sometimes progress and experience attacks with increasing frequency, resulting in headaches that occur on a daily or near-daily basis. This condition of chronic daily headache can result from several factors, although it is most often associated with medication overuse (30). Modifiable risk factors include attack frequency, patient obesity, medication overuse, stressful life events, and snoring/sleep apnoea (41). These factors may be addressed by both GP and patient, via the prescription of preventative medication, weight loss, use of specific acute migraine treatments to reduce repeat dosing of less-effective remedies, and counselling or behavioural therapy to reduce stress and stop snoring. However, some factors are not so easily modified, including migraine as a risk factor, being female, low socioeconomic status and the effects of head injury or stroke (41). GP awareness that progression may be more likely in some individuals and clinical vigilance to prevent such progression are, therefore, also important factors when consulting with migraine patients.
Conclusions
Based upon the prevalence and epidemiology of migraine, it is clear that GPs are key to successful management of those migraine patients who do not require specialized neurological treatment. The first consultation is critical: if patients are not satisfied with the outcome, many will not return and will instead resort to self-medication.
Unlike many neurologists, physicians in the primary care environment have generally received little specialized training in migraine diagnosis and treatment. GPs, therefore, require tools both to improve diagnosis and to assess the impact of the migraine pain on the patient. In addition, more treatment should be individualized using a stratified-care regimen, and physicians at all levels must be vigilant in order to prevent migraine progression to chronic daily headache. However, such improvement requires the widespread use of standardized management guidelines, as well as continuing education and neurologist support for GPs.
Footnotes
Competing interests
M. L-M. has acted as a paid consultant to Almirall, GlaxoSmithKline, Grunenthäl, Johnson & Johnson, Lilly, Medtronic, Menarini, MSD and Pfizer.
Acknowledgements
The author would like to thank Sally Mitchell PhD, from Complete Medical Communications, who provided medical writing support funded by Almirall.