
Abstract
Depression is a disabling disorder that is now acknowledged as the leading cause of years of life lost to disability in many developed countries [1]. Among older adults, the presence of depressive symptoms can complicate the clinical course of medical conditions [2] and increase mortality [3]. With approximately 80% of adults aged 60 years and over visiting their general practitioner (GP) at least once per year [4], [5], the GP is in the best possible position to detect and treat cases of depression in later life [6]. Unfortunately, while 5–10% of older adults who visit a general practitioner will be affected by major depression [7], depression is consistently reported to be inadequately diagnosed and treated in primary care settings [8].
As part of an educational project designed to enhance GPs' detection and management of older adults at risk of suicide, we report on the characteristics of depressed older patients detected by their GP versus those depressed patients who are missed.
Methods
Study population
The study population consisted of 218 patients scoring above the cut-off (≥ 16) of the Center for Epidemiological Studies – Depression Scale [9], from a sample of 916 consecutive patients aged 60 years or over attending one of 54 randomly selected GPs in the State of Western Australia (WA) during a specified four-week period between October 2002 and June 2003. A maximum of 15 patients from each clinic was invited to participate. The Human Research Ethics Committee of the University of Western Australia approved the study.
General practitioner participants had a mean age of 52.3 years (range: 38–82) and tended to be male (65.5%), work full time (70.9%) in group practices (81.8%) and completed their medical training in Australia or New Zealand (69.1%). Approximately a quarter (23.6%) of the GPs had not attended a mental health-training event over the past 2 years, while the remaining doctors had participated in one (9.1%) to five or more (12.7%) mental health educational activities during the previous 24 months.
Survey methods
Patients awaiting general practice consultations were given the study's self-report questionnaire by the practice nurse or receptionist and instructed to complete it prior to the medical appointment. After each consultation, general practitioners recorded the patient's presenting complaint(s), medication information, and mental health details (i.e. their opinion of the presence of psychological distress and an esti-mation of depression and suicide risk) on a patient summary sheet. General practitioners were not aware of patients' participation status or the results of their preconsultation questionnaires. At the end of the four-week study period, patient questionnaires and the consultation summary sheets were mailed to the research team.
Instruments
The following variables were assessed from the patient-completed questionnaire.
Demographic factors: age, gender, relationship status, country of origin and language spoken at home were systematically recorded.
Lifestyle and physical health: patients were dichotomised based on their current tobacco smoking status, current use of sleeping tablets, and those who perceived their current health to be either poor or good.
Depression: the presence of depressive symptomatology was assessed with the 20-item Center for Epidemiologic Studies – Depression Scale (CES-D) [9]. The scale has been widely used in epidemiological surveys, with demonstrated reliability and validity. We utilized the recommended cut-off score of 16 or greater on the CES-D [9] to classify patients as experiencing significant depressive symptomatology, and a score of 22 or greater to identify subjects likely to be suffering from a major depressive episode [10].
Patient summary sheet: based on the consultation information provided by the doctor, patients' presenting complaints were classified by the authors as either medical (including well-person care) or psychological (with or without accompanying medical complaints). Patients taking three or more medications were classified as receiving polypharmacy, while doctors systematically estimated the presence of depression for each patient.
Statistical analysis
The data were analysed using the statistical package SPSS-11. The influence of several patient variables on GPs' classification of depression status amongst their older patients was examined using Student's t-test, chi-square using Yates' Correction, and logistic regression.
Results
In total, 218/916 (23.8%) patients were classified as experiencing clinically significant depressive symptomatology based on their CES-D score (≥ 16). Of these 218 CES-D depressed patients, 39.9% (87/218) were also registered as depressed by their GP following their medical consultation. Older adults with CES-D case range scores who were classified as depressed by their GP were more likely to smoke, use sleeping tablets, receive three or more medications, present with psychological complaints, and have high CES-D scores compared to those CES-D case range patients not registered as depressed by their GP (Table 1).
Associations between various patient factors and GP classification of depression in 218 general practice patients 60 years or older with clinically significant self-reported depression (CES-D ≥ 16)
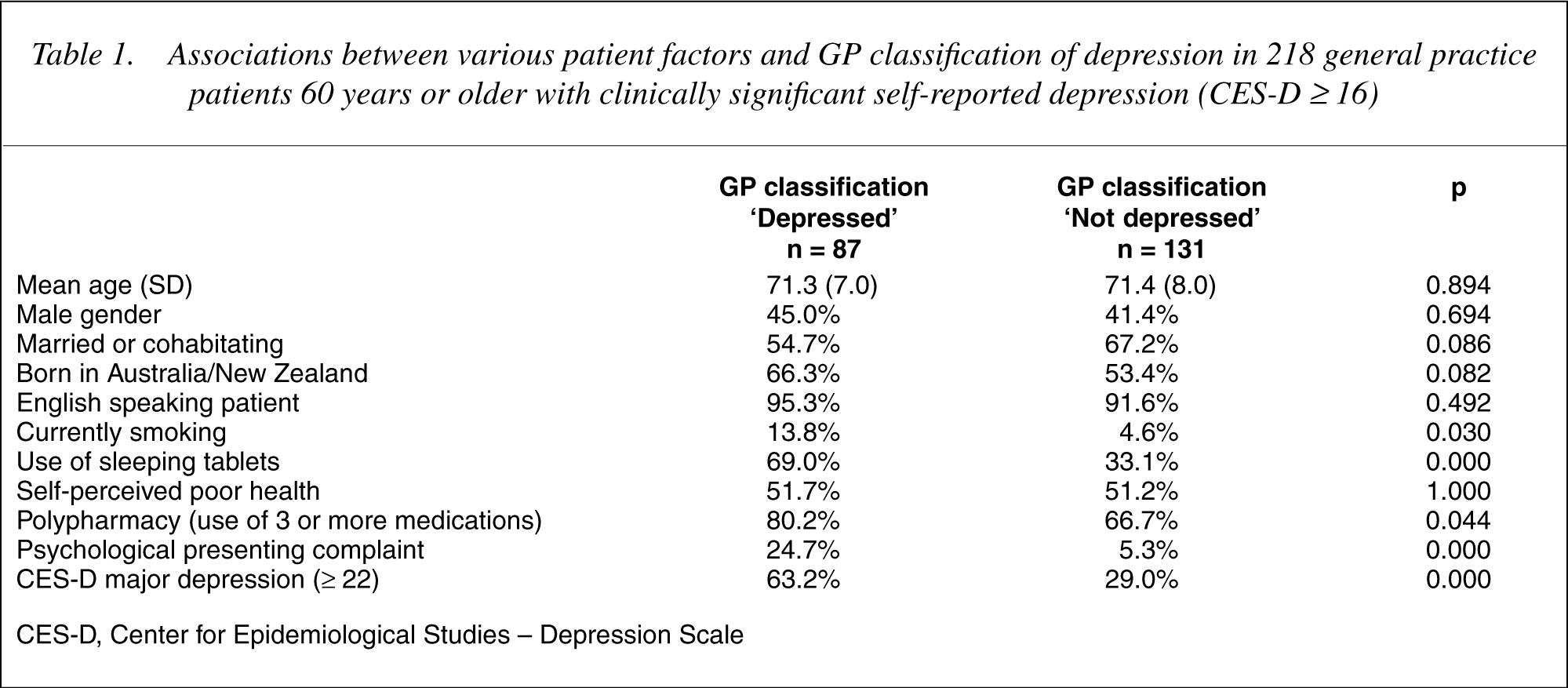
CES-D, Center for Epidemiological Studies – Depression Scale
An explanatory logistic regression model was fitted to the variables that most distinguished GPs' classification of depression status amongst participants in the univariate analyses. This multivariate analysis revealed that older patients experiencing significant levels of self-reported depression (CES-D ≥ 16) were more likely to be classified as ‘not depressed’ by their GP when they were born outside of Australia or New Zealand, did not smoke or use sleeping tablets, acknowledged milder levels of depression (CES-D = 16–21), and presented to their GP with primarily somatic complaints (Table 2).
Results of logistic regression analysis of association between patient factors and GP classification of ‘not depressed’ in 210 general practice patients 60 years or older with clinically significant self-reported depression (CES-D ≥ 16)
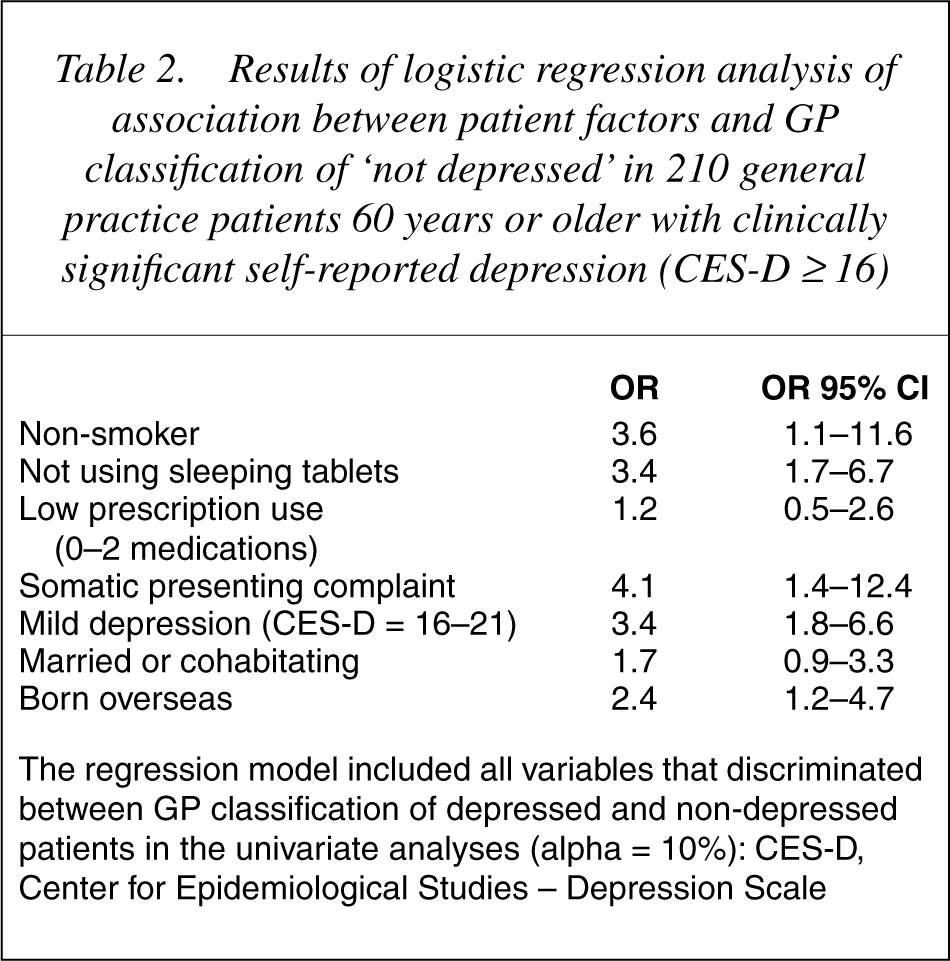
The regression model included all variables that discriminated between GP classification of depressed and non-depressed patients in the univariate analyses (alpha = 10%): CES-D, Center for Epidemiological Studies – Depression Scale
Discussion
We found approximately 24% of our sample of older primary care attendees presented with significant depressive symptomatology, falling within the range of clinically significant depression previously found among this age group in primary care settings (17–37%) [11]. While less than half of our depressed patients' mental health status was registered by their GP, those with overt or severe symptoms (i.e. sleep disturbance, psychological presenting complaints, or major depression) were more likely to be classified as depressed. That patients with salient mental health symptoms are more likely to be recognized by their GP should be of no surprise. Short consultation times with a focus on somatic complaints, lack of confidence in diagnosing geriatric depression, incorrectly attributing depressive symptoms to the ‘normal’ ageing process, an under-diagnosis of mental health symptoms in foreign patients and limited knowledge of depressive symptomatology may all contribute to the failure to recognize depression in older primary care patients [12–16].
While strong evidence supports the efficacy of pharmacological and psychological treatments of depressive disorders in later life [17], if these disorders are not detected, they cannot be treated. Patients can assist the GP in the diagnostic process, as the recognition rate of depression is greatly enhanced when patients talk about feeling depressed, sad or irritable [18], do so early in the consultation [19], and avoid trying to normalize their symptom presentation [20]. Unfortunately, elderly patients tend to present with a higher prevalence of comorbid medical illness compared to younger cohorts, leaving mental health concerns as only one of a number of health problems requiring the doctor's attention [21].
It could be argued that a limitation of our study is that our measure, results, and conclusions may not apply to a formal clinical diagnosis of depression. However, it is important to emphasize that our aim was to assist clinicians in detecting and managing those older patients who were experiencing significant depressive symptomatology – a factor that impacts strongly on morbidity and mortality in this age group. While our results suggest that GPs are more able to detect depression among older patients with prominent depressive symptoms, there remains a high proportion of patients in this age group who silently experience significant depressive symptomatology and miss the opportunity for effective treatment (60%). Our results suggest that current smoking, use of sleeping tablets, polypharmacy and psychological complaints should increase the level of suspicion that depression may be present. However, to enhance the detection of silently disturbed patients, brief screening strategies may be the most cost-effective means to identify older adults at risk for depression in primary care [22]. For example, Arroll et al. [23] showed that the use of two simple questions (feeling down/depressed/hopeless or lack of interest/pleasure in doing things) is highly effective in detecting cases of depression in general practice settings (97% sensitivity and 67% specificity), which suggests that screening for depression could be incorporated into the routine assessment of older adults in general practice.
Footnotes
Acknowledgements
This project was supported by a grant from the Commonwealth Department of Health and Ageing, as part of the National Suicide Prevention Strategy. We thank WA GPs and older adults under their care who agreed to take part in this study.