
Abstract
Introduction:
Treatment guidelines for schizophrenia represent a standard way to manage patients, especially in countries with limited staff resources. However, they have not been compared on their efficacy with treatment as usual, despite adult studies suggesting they can be more effective.
Methods:
Inpatient and outpatient adolescents with schizophrenia were randomly allocated to be either treated according to a guideline-based treatment (n = 43) or treatment as usual (n = 44). The effects on symptoms, psychosocial functioning and cognition were compared in a 6-month follow-up.
Results:
There were no differences between groups in the pharmacological treatment, reduction in symptom severity or cognition. The guideline-based treatment group showed a better functioning at months 3 and 6.
Conclusion:
The guideline-based treatment had a greater effect than the treatment as usual in the psychosocial functioning of adolescent patients (www.clinicaltrials.gov; II3/02/0811).
Introduction
Psychiatric associations, medical associations and health ministries of a large number of countries have developed clinical guidelines for the management of schizophrenia in adults (Gaebel et al., 2005, 2011; Galletly et al., 2016). These guidelines, despite being carefully elaborated, have barely been examined with respect to their feasibility and efficacy in comparison with the usual treatment. One example is the Texas Medication Algorithm Project, which compared the outcome (symptoms and cognition) over a 12-month period in patients treated according to a pharmacologic and education package algorithm with a group of patients treated as usual. The results showed that the first group displayed an earlier response and had a larger improvement in cognitive functions (Miller et al., 2004).
In the case of early onset schizophrenia, treatment guidelines should take into account age-specific aspects, such as school attendance, peer relationships and family involvement, in order to avoid long-term consequences such as educational failure, unemployment, social withdrawal and further mental health problems such as substance abuse (Yung, 2016). Based on this, both the American Academy of Child and Adolescent Psychiatry and the National Institute for Health and Clinical Excellence elaborated guidelines for the treatment of young people with schizophrenia. In the latest versions, they incorporated psychoeducation, healthcare promotion and the inclusion of patients in socially useful activities such as school attendance or work. They also recommended the use of second-generation antipsychotics as the first pharmacological choice and the use of clozapine after two 6- to 8-week trials on other antipsychotics (McClellan and Stock, 2013; National Institute for Health and Care Excellence, 2013). However, these guidelines have not been evaluated with respect to their feasibility or compared with the usual treatment. Currently, the only published study comparing the effectiveness of a multimodal treatment versus the treatment as usual (TAU) in adolescents was the Trialog Project, which was designed as a 2-year program of residential outpatient care for patients with early onset schizophrenia. Although the results showed that the program had a larger effect on positive and negative symptoms, social functioning and some cognitive impairments, they could not be generalized due to limitations such as a small sample size, an open design and the use of different instruments for the assessment of patients (Hemmerle et al., 2010).
Recently, Greenhalgh et al. (2014) discussed the importance of adapting clinical guidelines to the local setting. This article emphasized that the success of interventions depends on local feasibility and fit with context, claiming that those who produce and summarize research evidence must attend more closely to the needs of those who might use it.
In Mexico, as in other countries, distance, access and funding constitute the main challenges to provide specialized health care to patients with serious mental illnesses. In view of this, the Child Psychiatric Hospital of Mexico City published a guideline for the diagnosis and treatment of children and adolescents with schizophrenia, aiming to adjust the evidence-based treatment to the conditions of the local clinical setting. The Clinical Guideline of the Child Psychiatric Hospital (CGCPH) (Ulloa et al., 2010) included information from the best evidence available and proposed an algorithm-based pharmacological treatment and the inclusion of psychoeducation, social skills training (SST) and healthy habits programs. The CGCPH was adjusted to the recommendations of the AGREE Instrument (AGREE Next Steps Consortium, 2009).
Considering the paucity of studies evaluating the efficacy of a clinical guideline in adolescents with schizophrenia, the objective of this study was to compare the efficacy of CGCPH versus TAU in terms of symptom severity, psychosocial functioning and cognition, during a 6-month follow-up.
Methods
Study design
This was a 6-month, randomized, follow-up study of adolescents diagnosed with schizophrenia who were treated according to either the CGCPH or the TAU.
Participants
Male and female youths, aged 12–17 years, with a DSM-IV (Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition) diagnosis of schizophrenia or schizophreniform disorder recruited between October 2011 and April 2015 from consecutive admissions at the inpatient and outpatient services of the Child Psychiatric Hospital of Mexico City, a public tertiary level mental health facility receiving children and adolescents from all over the country.
They were included if they had a total score ⩾70 on the Positive and Negative Syndrome Scale (PANSS) and a score of at least 4 (moderate) on three of the following core items (conceptual disorganization, hallucinatory behavior, suspiciousness and unusual thought content). In addition, patients had not received a regular antipsychotic treatment for the last 4 weeks. Exclusion criteria were the presentation of unstable medical conditions, a diagnostic change, substance-related disorders (except cannabis abuse) or pregnancy.
Measures
Mini-International Neuropsychiatric Interview: Child and Adolescent Version
A structured diagnostic interview was conducted to assess short-term psychopathology of children and adolescents. The Spanish version showed significant concurrent validity and good inter-rater and test–retest reliability (Sheehan et al., 2010).
The PANSS
The scale assesses the severity of symptoms in a semistructured interview. It was evaluated according to the five factor–dimensional model of schizophrenic symptoms (positive, negative, excitement, anxiety/depression and cognitive) (Fresán et al., 2005).
The Personal and Social Performance Scale
The Personal and Social Performance Scale (PSP) is a short scale which is rated based on four domains following specific operational definitions: (A) socially useful activities, (B) personal and social relationships, (C) self-care and (D) disturbing and aggressive behaviors, and a global functioning score rated on a 100-point scale based on the combination of the scores of the four domains (Morosini et al., 2000). A previous study reported its validity and reliability in adolescent patients (Ulloa et al., 2015).
The MATRICS Consensus Cognitive Battery
This instrument evaluates seven cognitive domains: speed of processing, attention-vigilance, working memory, verbal learning, visual learning, reasoning/problem solving and social cognition (Nuechterlein et al., 2008).
The MATRICS Consensus Cognitive Battery (MCCB) has been examined in samples of healthy adolescents (Nitzburg et al., 2014) and used to compare the cognitive functioning of patients with and without schizophrenia (Holmén et al., 2010).
Study procedures and assessments
The research staff included mental health professionals (psychiatrists, child psychiatrists and psychologists) with at least 2 years of experience. They were trained on CGCPH procedures and rating scales. Inter-rater reliability for each scale was established using case vignettes and videotapes. An 80% of agreement and intraclass correlation coefficients ⩾0.70 were achieved.
Determination of sample size
A power calculation for a paired t test estimated that a sample size of 34 participants per group would have an 80% power to detect an effect size of 0.5 in PANSS scores between baseline and final visits. Additionally, with an estimated 20% dropout rate (Findling et al., 2010; Mueller et al., 2015), the sample size was set at least 40 subjects per group.
Allocation of participants
Numbers representing the order of recruitment (from 1 to 120) were drawn using sampling without replacement and arranged into two columns: those in the first column were assigned to CGCPH and those in the second to TAU.
TAU
In this treatment, psychiatrists prescribed their antipsychotic drug of choice, being risperidone the most frequent. Clinician decisions to modify the medication were based on the persistence of symptoms in a variable time frame. Some patients also received individual psychotherapy according to clinician’s criteria.
CGCPH treatment
The pharmacological treatment algorithm is shown in Figure 1. The psychosocial treatment started at week 3 and included the following elements:
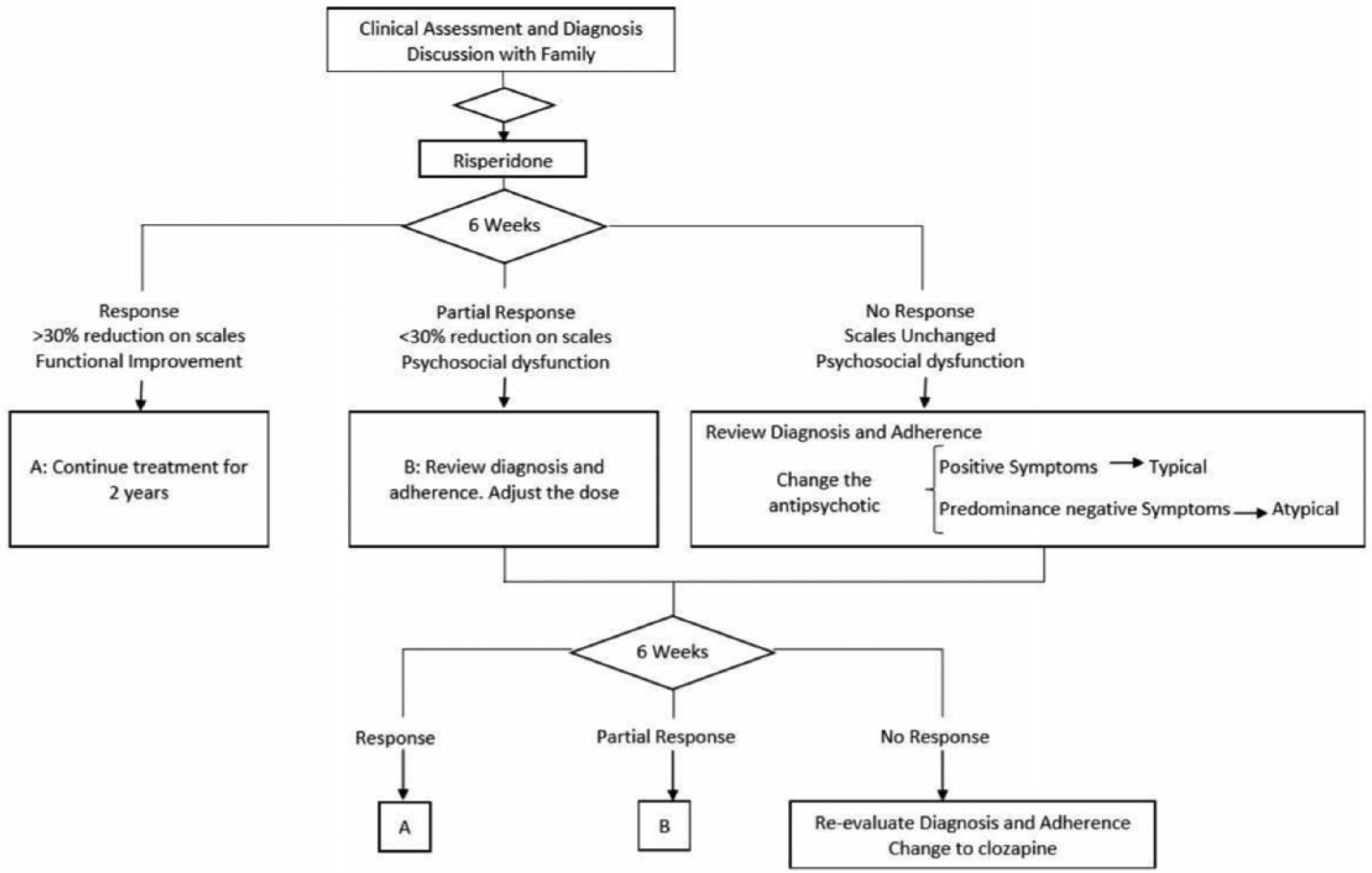
Pharmacological treatment algorithm in CGCPH.
Psychoeducation
A program was developed where caregivers received three 90-minute sessions, in which the following topics were addressed: clinical characteristics and etiology, multimodal treatment, relapse prevention and management of stigma. To confirm that the caregivers understood the discussed topics, a brief test was administered before and after each session.
SST
This program consisted of a series of nine weekly sessions conducted over 45 minutes, covering verbal and nonverbal communication, paralinguistic components and conversational skills.
Healthy habits program
This program was conducted over nine weekly sessions and included nutrition counseling, the importance of physical activity and avoiding substance abuse, followed by 30 minutes of aerobic exercise.
Schedule of assessments
Participants underwent a complete evaluation at the baseline visit. PANSS was administered on the following visits (weeks 3, 6 and 9, months 3, 4, 5 and 6). The PSP and MCCB were administered at baseline and months 3 and 6. An independent evaluator who was blind to the patient’s group scored the PANSS and PSP at months 3 and 6.
Human subjects protections
The study was conducted in accordance with international guidelines for good practice and the Declaration of Helsinki. It was approved by the Institutional Review Board of the Child Psychiatric Hospital (approval number CEI/105). Written subject assent and parental informed consent were obtained for all of the participants.
Statistical analyses
Continuous variables were analyzed using a Student’s t test and a repeated measures analysis of variance (RM-ANOVA) from baseline to month 6. Categorical outcomes were compared across treatment groups using χ2 tests. Values are expressed as mean ± standard deviation. Significance for all tests was set at p ⩽ 0.05. All analyses were conducted using IBM PASW 21.
Results
Baseline characteristics and treatment
From a total of 87 patients, 74.7% completed the 6-month follow-up. Figure 2 shows the rates of discontinuation of patients in each group.
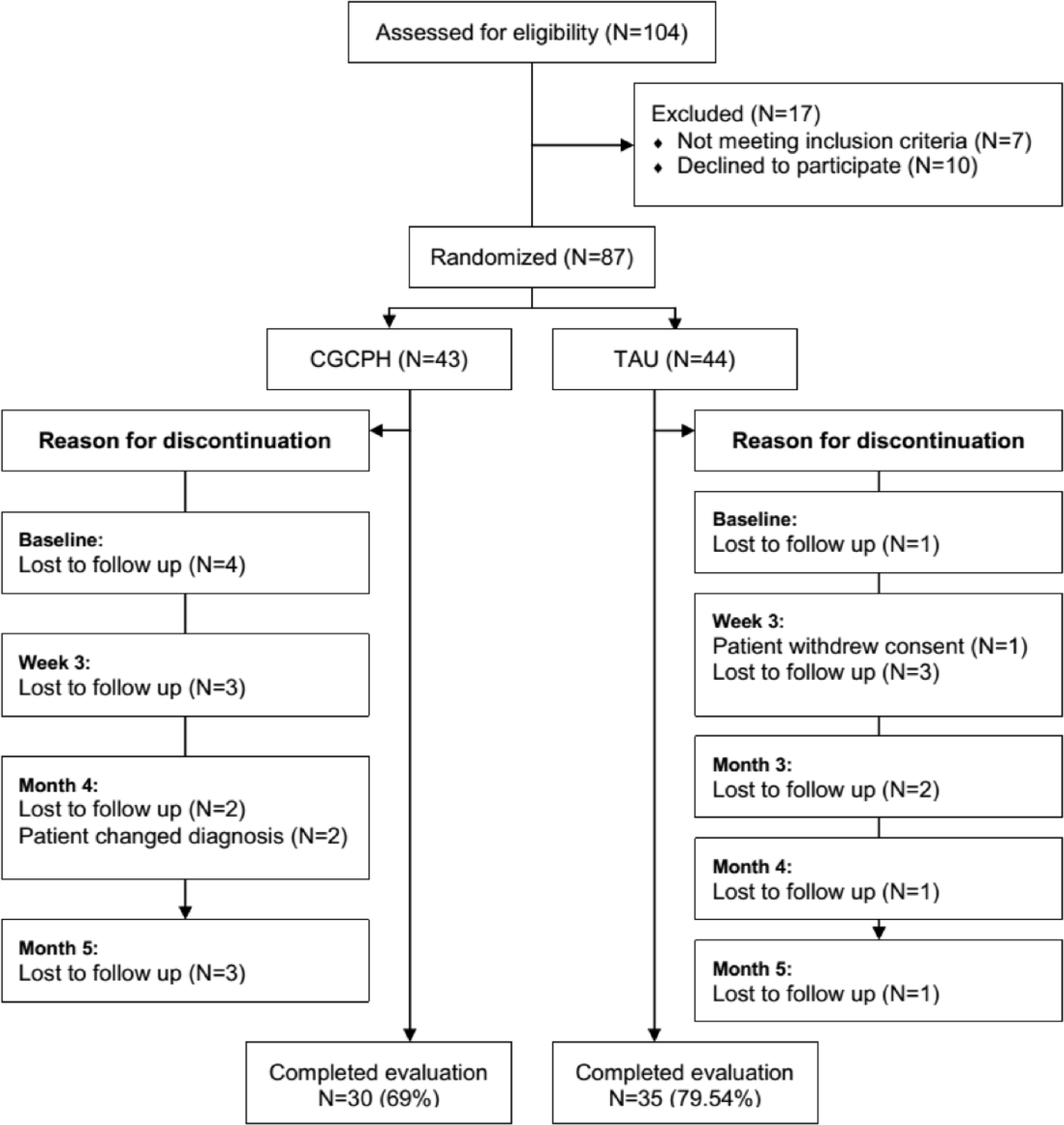
Participants flow diagram.
Baseline evaluation of the sample showed that among those with comorbid disorders, the most frequent diagnoses were Major Depressive Episode (17%), Generalized Anxiety Disorder (22.2%), Obsessive Compulsive Disorder (14.3%) and Attention Deficit Hyperactivity Disorder (11.4%). No differences were observed in the demographic and clinical characteristics of patients on each treatment group (Table 1).
Demographic and clinical characteristics of the sample.
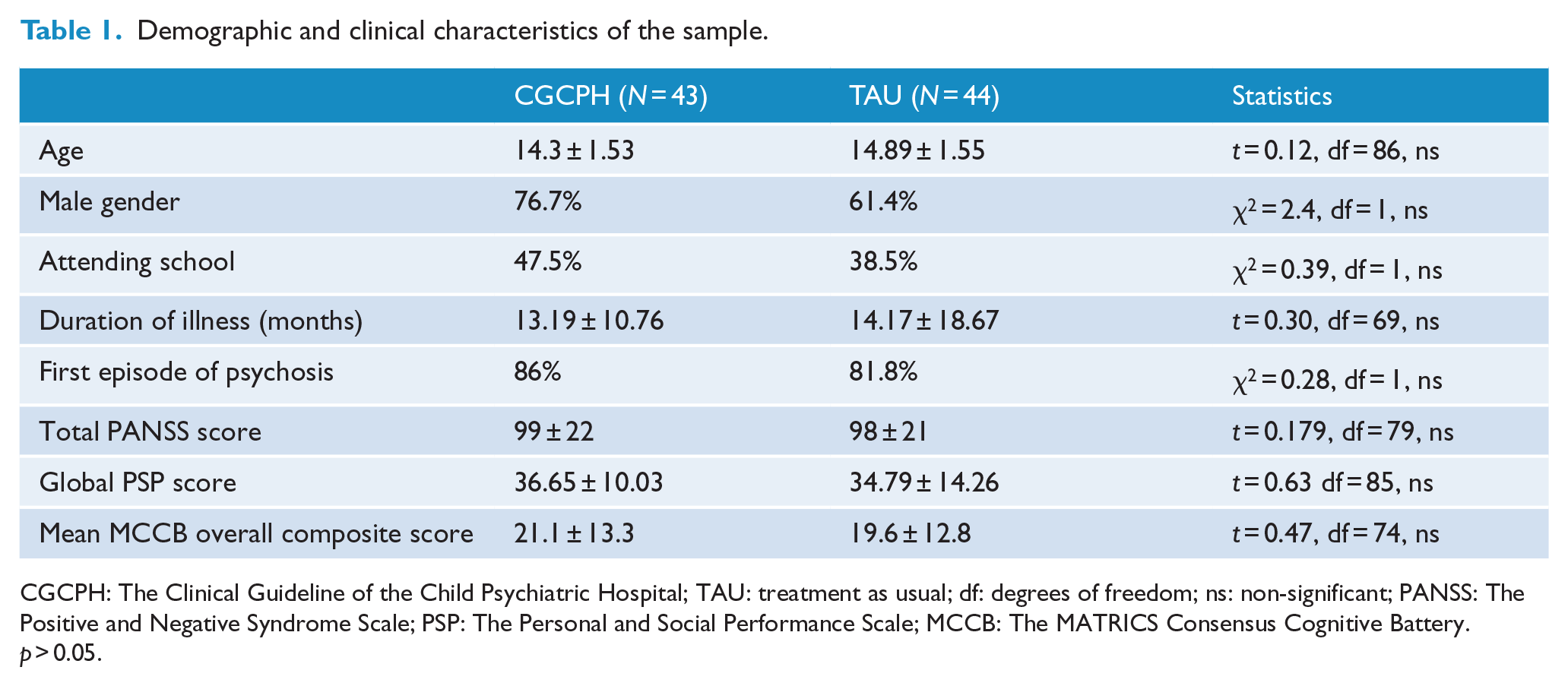
CGCPH: The Clinical Guideline of the Child Psychiatric Hospital; TAU: treatment as usual; df: degrees of freedom; ns: non-significant; PANSS: The Positive and Negative Syndrome Scale; PSP: The Personal and Social Performance Scale; MCCB: The MATRICS Consensus Cognitive Battery.
p > 0.05.
The pharmacological treatment of the CGCPH group was based mainly on risperidone (86%) and olanzapine (11.6%), with a mean dose of 219.37 ± 72.1 mg in chlorpromazine equivalents. In the TAU group, 77.3% of patients received risperidone, 11.4% quetiapine and 6.8% olanzapine with a mean dose of 220.4 ± 72.9 mg in chlorpromazine equivalents. There were no differences in the mean dose of antipsychotics during the follow-up. While a 100% of the CGCPH group received the three components of psychosocial treatment, only 31.8% of patients in the TAU group received individual brief psychotherapy.
Outcome measurements
PANSS factors scores decreased throughout the follow-up. At month 3, the CGCPH group showed significantly lower scores in negative (12.05 ± 4.78 vs 17.31 ± 6.28, t = 3.93, df = 63, p < 0.001), excitement (7.22 ± 2.53 vs 10.62 ± 6.14, t = 3, df = 68, p = 0.003) and cognitive (10.42 ± 4.03 vs 14.41 ± 6.40, t = 3.1, df = 67, p = 0.003) factors. No significant differences between groups were observed at the final visit (Table 2).
Mean (SD) of PANSS factors scores during follow-up.
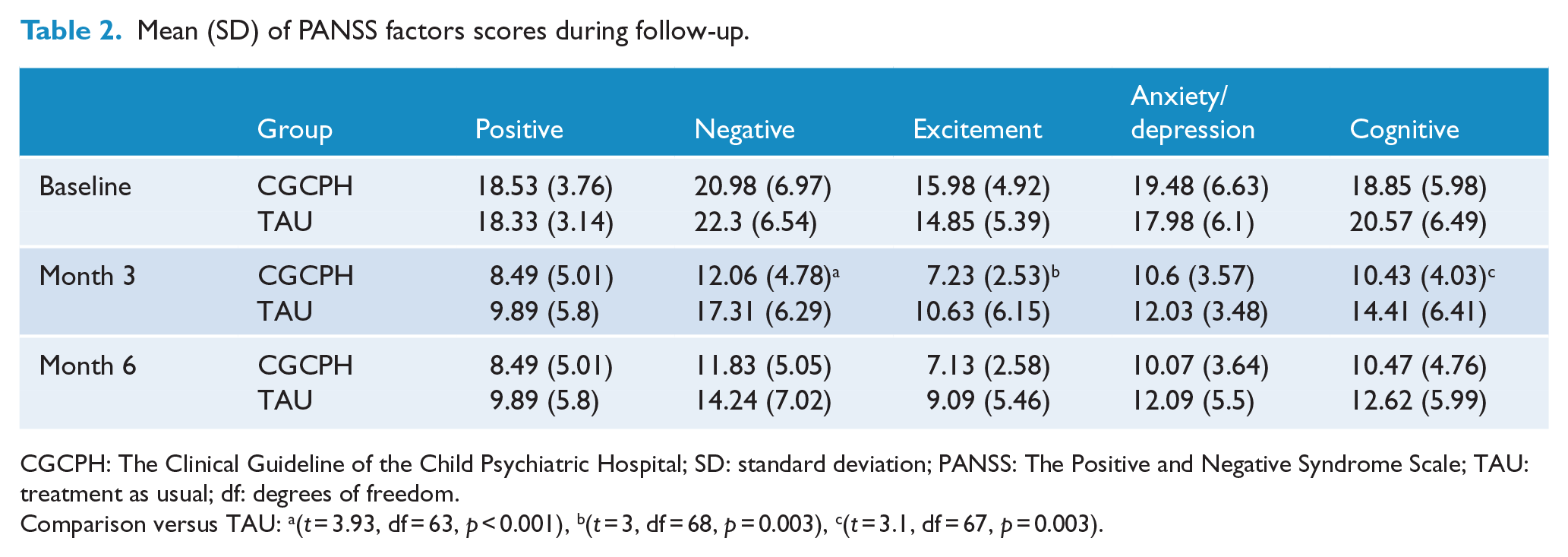
CGCPH: The Clinical Guideline of the Child Psychiatric Hospital; SD: standard deviation; PANSS: The Positive and Negative Syndrome Scale; TAU: treatment as usual; df: degrees of freedom.
Comparison versus TAU: a(t = 3.93, df = 63, p < 0.001), b(t = 3, df = 68, p = 0.003), c(t = 3.1, df = 67, p = 0.003).
Although the percentage of subjects reaching PSP subscales scores of 1 (absent) and 2 (mild difficulties) increased in both groups, most patients of the CGCPH group showed higher levels of functioning from month 3 on socially useful activities (PSP-A), self-care (PSP-C) and disturbing and aggressive behaviors (PSP-D) and maintained them at month 6, by which they had also improved on personal and social relationships (PSP-B) (Table 3). The MCCB scores showed similar levels of cognition improvement in both groups (Table 4).
Percentage of patients exhibiting good functioning during the follow-up according to PSP.
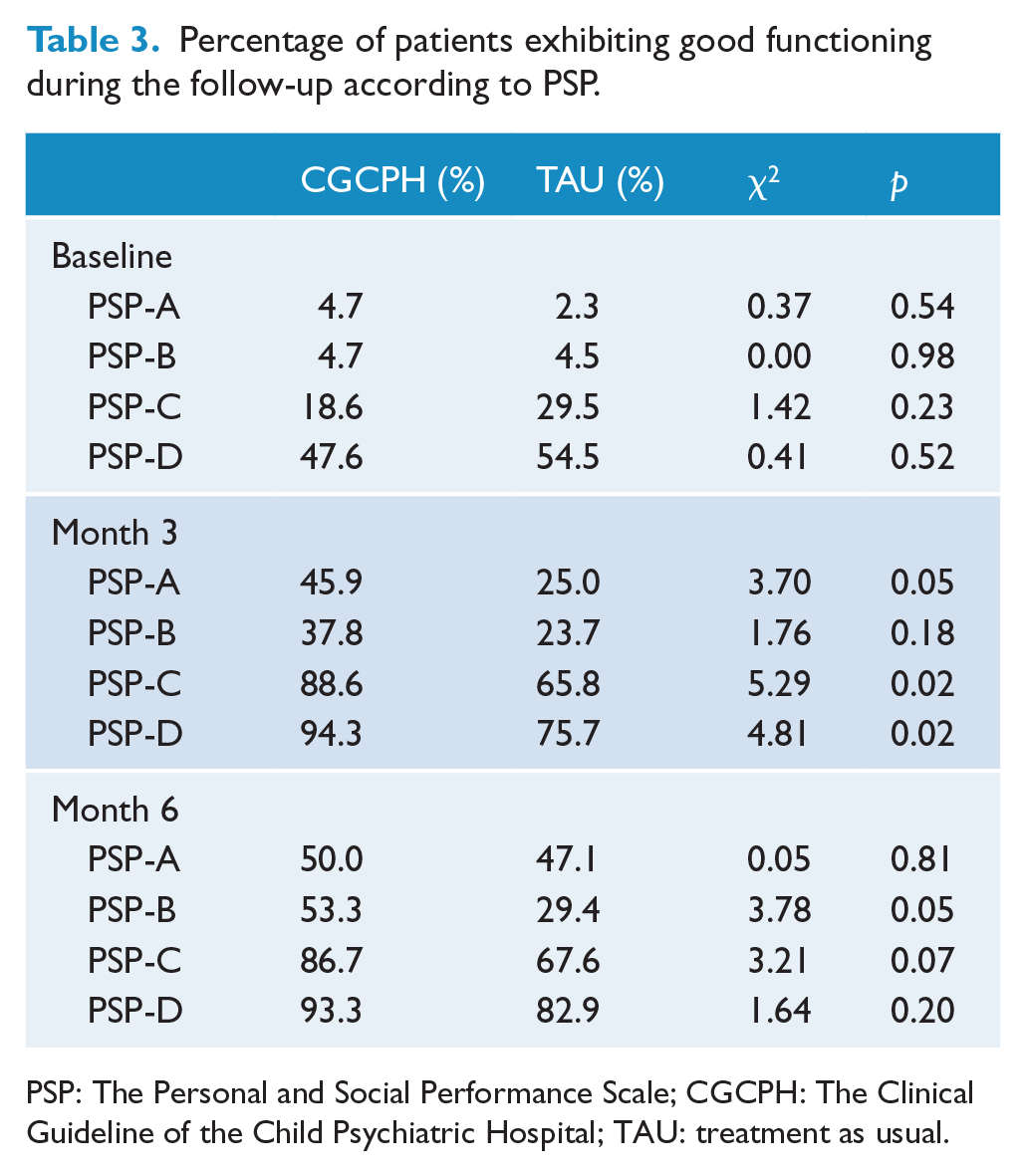
PSP: The Personal and Social Performance Scale; CGCPH: The Clinical Guideline of the Child Psychiatric Hospital; TAU: treatment as usual.
Mean scores of MCCB domains during follow-up.
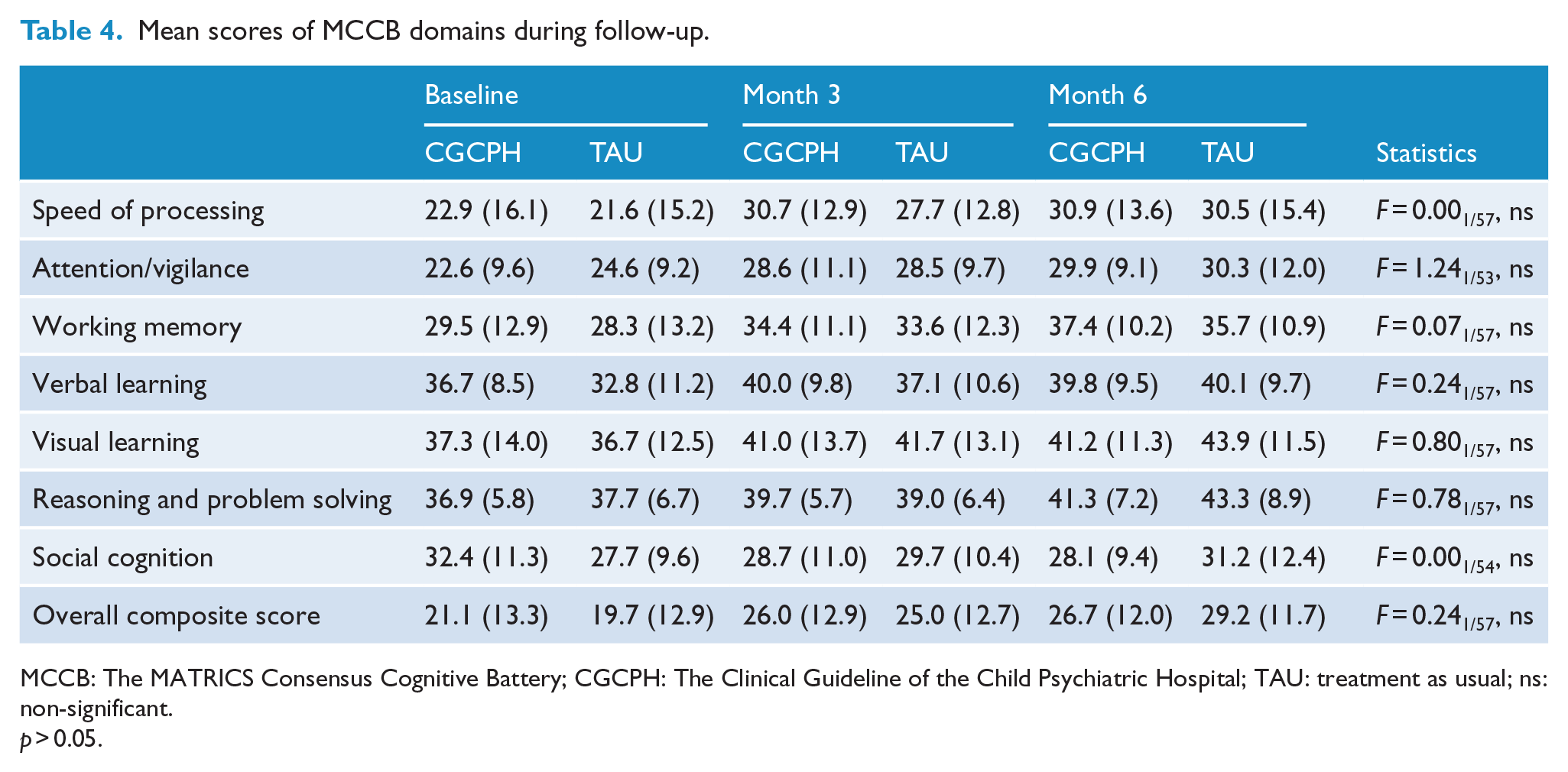
MCCB: The MATRICS Consensus Cognitive Battery; CGCPH: The Clinical Guideline of the Child Psychiatric Hospital; TAU: treatment as usual; ns: non-significant.
p > 0.05.
Discussion
This study compared the effectiveness of a guideline-based treatment versus TAU in adolescents with schizophrenia. The results showed that patients treated according to the CGCPH had an earlier response and a greater improvement on psychosocial functioning. These findings could be contrasted with studies comparing a multimodal treatment with standard treatment. The study by Falloon (2004) showed that the implementation of optimal treatment including minimal effective antipsychotic doses, psychoeducation and social/occupational skills training led to a greater improvement on patients evaluated with global measures of mental functioning and disability. Other studies displaying similar results include the research of Nordentoft et al. (2015) in adults with a first episode of psychosis and the trials in adults with chronic illness using the Texas Algorithm (Miller et al., 2004). Both these reports showed similar results regarding the earlier improvement on negative symptoms in patients treated according to the algorithm. However, the study by Miller reported an improvement on cognitive functioning, a finding that was not present in this study. This difference could be due to the use of different methods of assessment and follow-up time frames. Taken together, all these reports point to the fact that the use of a guideline-based treatment is associated with a higher level of improvement in patients with schizophrenia.
The earlier response observed in the CGCPH group could be associated with the consistent application of psychosocial interventions, which largely contrasts with the inconsistencies of TAU. The positive effect of psychosocial interventions on a patient’s outcome has long been documented (Galletly et al., 2016). In particular, psychoeducation could contribute to reduce the patient’s aggressive behaviors through its effect on their families, who received help to improve their coping skills to assist their patient’s needs and manage their crisis. Previous studies have reported the effect of psychoeducation on psychotics symptoms (Koolaee and Etemadi, 2010), social relationships (Magliano et al., 2006), adherence to treatment and relapse reduction (Ngoc et al., 2016; Petretto et al., 2013; Xia et al., 2011), while SST allows patients to acquire new social roles, improving assertiveness and communication (Chien et al., 2003; Cirici and Obiols Llandrich, 2008; Kurtz and Richardson, 2012). These improvements were achieved despite the fact that the CGCPH does not include some previously tested interventions, such as cognitive behavioral therapy, in order to reduce costs and make the most out of the available trained staff in the hospital.
Similar PANSS scores observed in both groups at the end of follow-up could reflect a declining effect pattern, which is seen when a new modality of treatment is compared with TAU (Kashner et al., 2003). An algorithm-driven treatment, such as CGCPH, could help practitioners find the service combination that optimizes outcomes sooner, yet it can be hypothesized that physicians using the TAU would also eventually find the optimum mix, allowing these patients to catch up with those treated according to guidelines. Thus, the use of CGCPH can lead to an earlier functional recovery as seen in the current results.
Regarding cognitive measures, both groups exhibited similar levels of improvement in most of the assessed domains, which could be attributed to the antipsychotic treatment (Karson et al., 2016). However, the scores of domains such as speed of processing, attention/vigilance and working memory remained below the normative mean (Kern et al., 2011). In light of this finding, future studies should evaluate the inclusion of a cognitive remediation program in the CGCPH, which has been shown to have a positive effect on these domains (McGurk et al., 2007; Puig et al., 2014; Wykes et al., 2011). This is particularly relevant given the relationship between cognition, functioning and quality of life (Brissos et al., 2011; Green et al., 2004).
Strengths and limitations
To the best of our knowledge, this is the first study evaluating the efficacy of a guideline-based treatment in a group of adolescent patients in a Latin American country. This region of the world, representative of middle- and low-income countries, has not been included in previous comparisons of guideline use surveys or implementation (Falloon et al., 2004; Gaebel et al., 2005). This highlights the opportunity to test guidelines, such as CGCPH, which are simple, harmless and inexpensive, characteristics accounting for feasibility (Van Der Krieke et al., 2015) in mental health facilities with limited staff and resources. In fact, the CGCPH proved to be cost-effective in terms of functional recovery (Ayala et al., 2017). All the above-mentioned characteristics highlight that elements such as adequate assessment, better interventions and communication between practitioners, patients and their family improve treatment effectiveness and reduce relapses (Catts and O’Toole, 2016).
A limitation is the relatively short duration of the study. Although a 6-month follow-up allowed to observe the time course of treatment response for each group, it may not be long enough to determine long-term changes. Future studies should examine the effect of CGCPH treatment for longer periods in other clinical samples.
Conclusion
A higher and earlier functional recovery has observed in adolescents with schizophrenia after guideline-based treatment.
Footnotes
Acknowledgements
The authors thank the staff of the Child Psychiatric Hospital, Mexico City. R.-E.U and R.A. designed the study and wrote the protocol. S.A. G.V., E.S., I.J., E.A., A.-T.D.C., M.D.V. and G.S. recruited patients and carried out measurements. R.-E.U., S.A., I.J. and G.V. wrote the first draft. R.-E.U. and M.R. performed statistical analyses. All authors contributed to editing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The Child Psychiatric Hospital covered the costs of lab tests and protocol visits.