
Abstract
Mental illness is now the leading cause of long-term sickness absence among Australian workers, with significant costs to the individual, their employers and society more broadly. However, to date, there has been little evidence-informed guidance as to what workplaces should be doing to enhance their employees’ mental health and wellbeing. In this article, we present a framework outlining the key strategies employers can implement to create more mentally healthy workplaces. The five key strategies outlined are as follows: (1) designing work to minimise harm, (2) building organisational resilience through good management, (3) enhancing personal resilience, (4) promoting early help-seeking and (5) supporting recovery and return to work. A narrative review is utilised to outline the theoretical evidence for this framework and to describe the available research evidence for a number of key example interventions for each of the five strategies. While each workplace needs to develop tailored solutions, the five strategy framework proposed in this review will hopefully provide a simple framework for employers and those advising them to use when judging the adequacy of existing services and considering opportunities for further enhancements.
Introduction
Mental illness is now the leading cause of sickness absence and long-term disability worldwide, including Australia. As outlined in Figure 1, in 2011, mental illness overtook musculoskeletal problems as the leading cause of disability support pension (DSP) in Australia, accounting for almost a third of all DSP cases. A similar pattern is also found in the National Data Set for Compensation-based Statistics, which reports annually on trends in work-related injuries. Mental disorder was the only major condition to show an increase in the number of serious compensation claims over the last decade, with an increase of 10% between 2000 and 2013, while over the same period, the number of claims for all other categories such as musculoskeletal disorders fell (Safework, 2013).
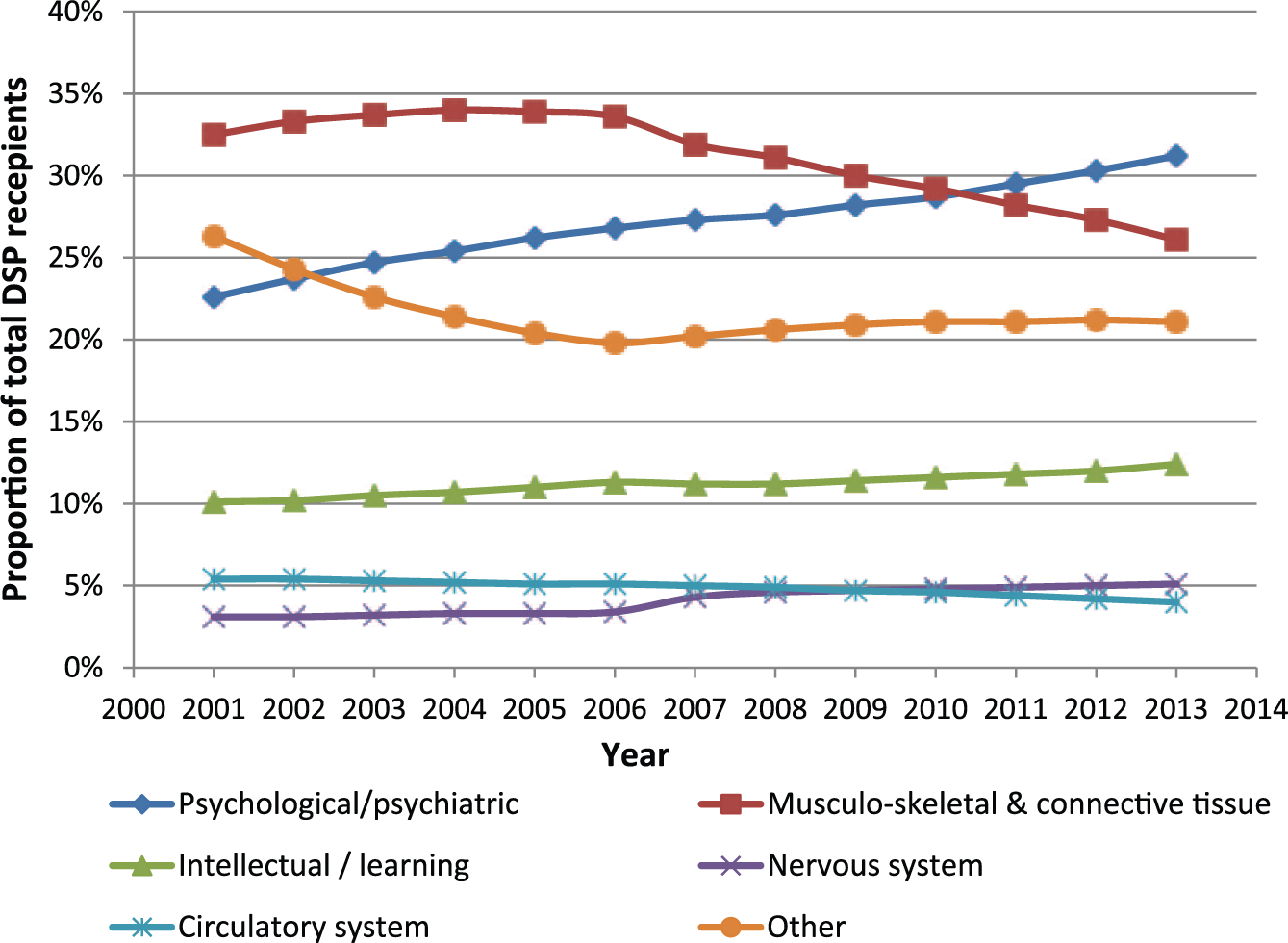
Proportion of DSP recipients by type of medical condition from 2000–2013*.
However, the impact of employee mental ill health goes well beyond sickness absence, compensable injuries and incapacity benefits, with common mental disorders, such as depression and anxiety, having a major impact on work performance and career trajectories (Harvey et al., 2011a; Henderson et al., 2011). Within Australia, it is estimated that depression alone costs the economy more than AUD12 billion each year, mainly due to lost productivity and worker turnover (LaMontagne et al., 2010).
Given such figures, it is not surprising that health professionals, clinicians, policy makers and workplaces now agree that the link between work and mental health problems is a major public health concern that needs to be addressed systematically. As a result, there is increasing interest in examining how work and workplaces can facilitate mental health and well-being and in the types of workplace interventions that may be beneficial in creating a more mentally healthy workplace (Mykletun and Harvey, 2012).
Although there is considerable evidence demonstrating the psychological impact of work on mental health (Harvey et al., 2017), there is surprisingly little consensus about what types of workplace interventions, if any, may be able to mitigate against these factors and improve the mental health of employees (Joyce et al., 2016). In practice, workplace initiated mental health strategies are often reactive and implemented without formal empirical evaluation (Henderson et al., 2003). There are a number of reasons for this, including the practical challenges of conducting high-quality research in the workplace and employers reluctance to await the outcome of research studies.
There is increasing consensus regarding the need for greater clarity on the framework for strategies workplaces should adopt for prevention and recovery of mental illness, and the evidence-base for these. In response to this, researchers in Australia (Harvey, Glozier) and the United Kingdom (Henderson) have gradually built a consensus framework of how the various types of interventions could be combined to create a more mentally healthy workplace. This framework is now being used by organisations such as the Australian National Mental Health Commission and the UK Chief Medical Officer in the guidance they are giving to employers and policy makers on workplace mental health. This Viewpoint article aims to present the current framework of how to create a mentally healthy workplace, outline the theoretical basis for this and to suggest evidence-informed strategies that could be implemented in practical applications of the framework.
A framework of how to create a mentally healthy workplace
The proposed framework of how a mentally healthy workplace can be created is illustrated in Figure 2. There are five broad workplace strategies that can be used to enhance employee mental health, namely:
Designing work to minimise harm;
Building organisational resilience through good management;
Enhancing personal resilience;
Promoting and facilitating early help-seeking;
Supporting recovery and return to work.
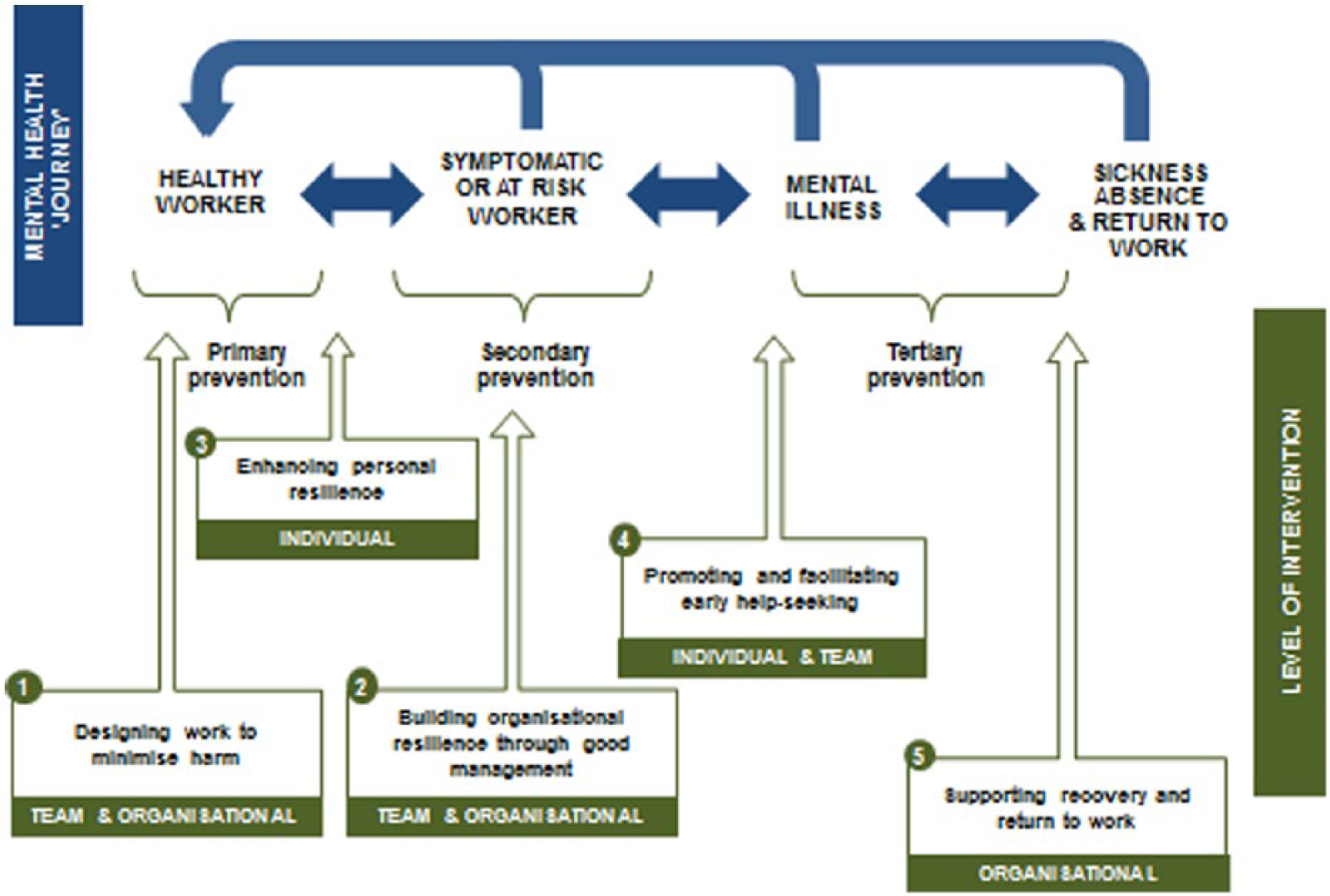
Diagram of the framework, outlining the mental health ‘journey’ of an employee and the five key workplace mental health strategies.
The first three strategies in the framework map onto concepts of universal and selective prevention, while the final two relate to indicated prevention and recovery. Reflecting this, the strategies presented are in accordance with earlier models of an employee’s mental health ‘journey’ showing the potential transition from a healthy worker to an ill worker requiring a period of sickness absence (Henderson et al., 2011). Additionally, the framework spans three levels of intervention, with mental health strategies that can be delivered on an individual, team and/or organisational level. The framework argues that optimal workplace mental health is best facilitated by the implementation of a mixture of preventative and reactive strategies delivered to the individual, team and organisational level. The framework draws on findings of recent reviews demonstrating empirically supported interventions workplaces can implement to assist in the prevention of common mental disorders (Mykletun and Harvey, 2012, Tan et al., 2014) and in facilitating symptom treatment, return to work and recovery in the workforce (Joyce et al., 2016, Modini et al., 2016).
Examining the evidence base for the framework
In order to provide an overview of the evidence supporting both the theoretical basis of the proposed framework and specific interventions that can map onto each of the five strategies, we conducted a narrative literature review. This was based on two previously published meta-reviews (Harvey et al., 2017; Joyce et al., 2016) together with separate searches using a variety of relevant keywords relating to the workplace (e.g. work, employment, job), interventions (e.g. training, change, resilience, intervention) and mental health or well-being outcomes (e.g. mental health, depression, anxiety, wellbeing, stress).
Both systematic reviews and original primary studies were included. Findings from reviews and higher-quality intervention studies were prioritised, however, results from observational studies were also considered.
To summarise the strength of evidence for various types of workplace intervention identified as examples within each strategy of the framework, we used a modified version of the United Kingdom Royal College of General Practitioners (UK RCGP) clinical guidelines. Four levels of research evidence were defined (Table 1), with strength of evidence indicated by a star rating system: strong, moderate, limited/contradictory or unknown.
Description of the strength of evidence adapted from the modified United Kingdom Royal College of General Practitioners (RCGP) clinical guidelines.
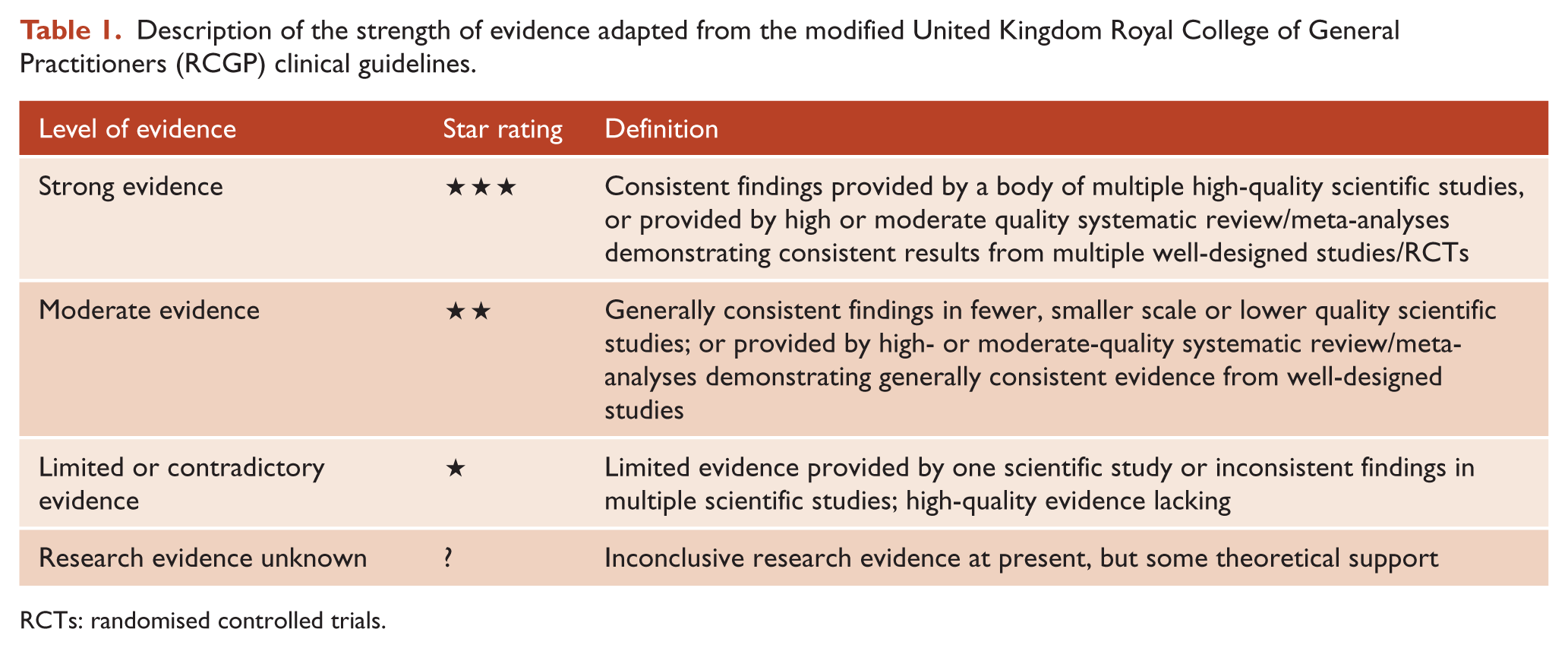
RCTs: randomised controlled trials.
Examples of workplace interventions under each strategy were identified. A summary of these is provided in Table 2, with the full reference details of the examples of relevant publications provided in a separate online supplement. While our review is not systematic or complete, we hope that identifying these key examples and the level of evidence associated with each assists both workplaces, clinicians and researchers when they consider the practical implications of our proposed framework.
Five workplace mental health strategies and examples of relevant studies, strength of evidence and level of intervention.
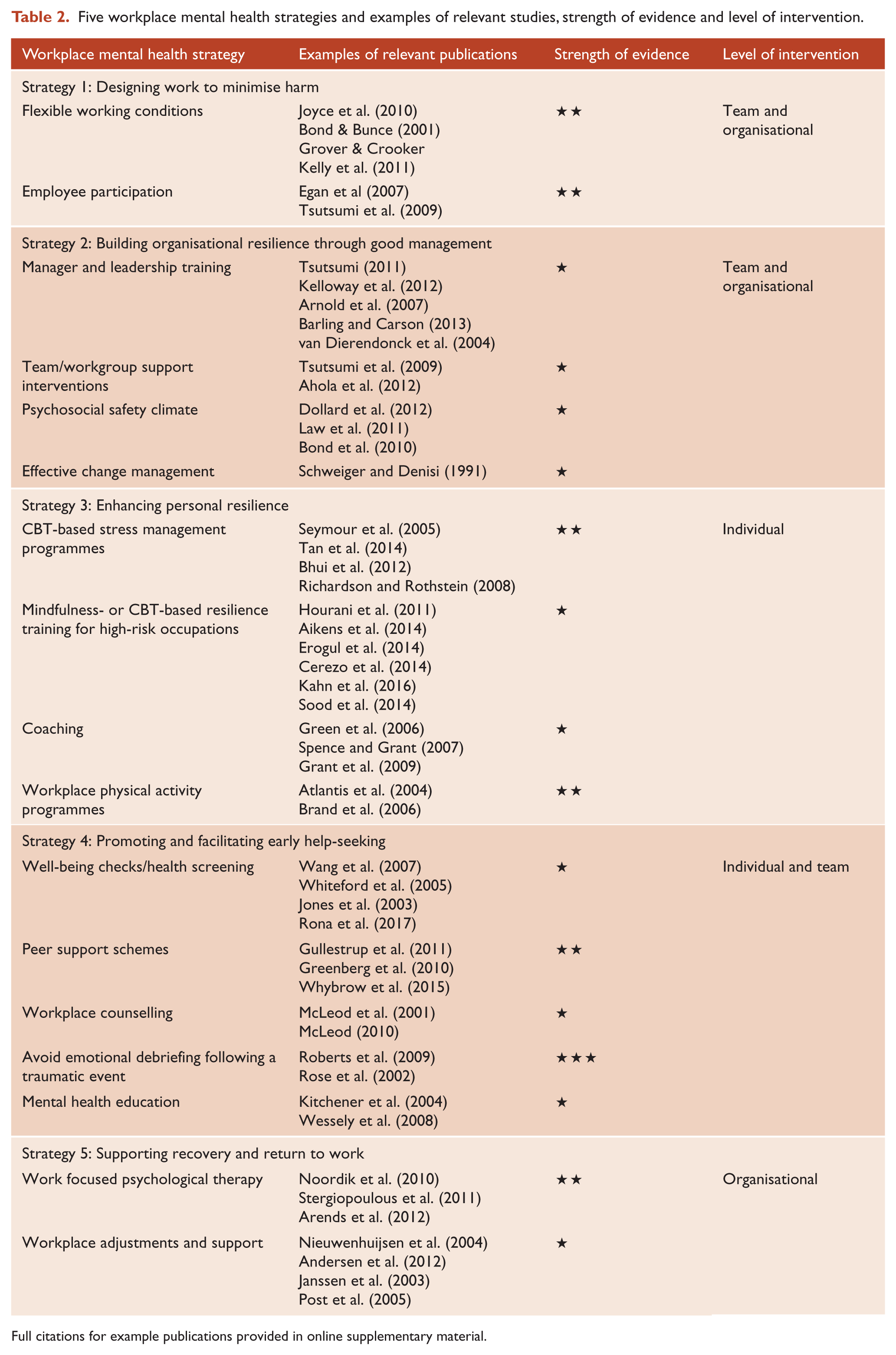
Full citations for example publications provided in online supplementary material.
A discussion of the evidence for the framework, and key findings and example interventions for each of the five strategies follows. In discussing the evidence for each type of intervention, it is important to note that there is a difference between the level of evidence for an intervention and the effect size of that intervention, meaning that those with the most evidence are not necessarily the interventions with the greatest effect.
Strategy 1: designing work to minimise harm
The first strategy refers to workplaces modifying job design and workplaces to reduce known risk factors for mental ill-health. Over recent decades, a range of work-based mental health risk factors have been identified from well-designed observation studies, including excessive job demands, limited job control, an imbalance between effort and reward, workplace trauma, bullying, role conflict and perceived injustice within an organisation (Harvey et al., 2017). Despite the range of potential risk factors, to date most intervention studies have focused on increasing employee control. The importance of employees perceived level of control over their working conditions and environment stems from Karasek’s Job Demand-Control-Support (JCDS) model. Interventions aimed at increasing employee control have tended to focus on the promotion of flexible working conditions or schemes designed to enhance employee participation in decision making.
Flexible working conditions★★
A Cochrane review examining the impact of flexible working conditions on mental health and well-being found that interventions which increased employee control and choice over their work patterns and shift schedules were likely to have a positive effect on their health (Joyce et al., 2010). A quasi-experimental study examining similar workplace strategies found that increased employee control was not only able to improve mental health, but also significantly reduced sickness absence among employees (Bond and Bunce, 2001).
Employee participation★★
There is also moderate evidence that increasing employee control via employee participation is effective in reducing symptoms of mental illness. A systematic review examined the impact of employee participatory strategies such as problem solving committees, education workshops and stress management committees (Egan et al., 2007). Although no randomised controlled studies were identified, the review showed promising evidence from controlled or comparison group interventions on anxiety and depression symptoms. There is also additional evidence from a more recent randomised controlled trial that examined the impact of a team participatory intervention on a healthy sample of Japanese workers (Tsutsumi et al., 2009).
Strategy 2: building organisational resilience through good management
While resilience can be defined in many ways, broadly speaking, resilience is the process of negotiating, managing and adapting to significant sources of stress, change, adversity or trauma. Various factors within the individual and their environment facilitate this capacity for adaptation and ‘bouncing back’ in the face of adversity and stress. In the proposed framework, resilience occurs at an organisational and an individual level. Strategies to enhance organisational resilience almost always require the involvement of leaders and managers.
Manager and leadership training★
While RCTs have shown that manager’s knowledge and confidence surrounding mental health matters in the workplace can be increased with training and that this is associated with reductions in subordinates’ levels of perceived stress, it remains unclear whether these changes translate into reduced mental health problems among these workers (Tsutsumi, 2011). Organisational psychology research has also found that the style of leadership shown by managers can have an impact on employee mental health, although such research is usually cross-sectional in design, and thus interpretations are based on inference. For instance, transformational leadership, a style that inspires meaning in the work of employees, is associated with employees’ psychological well-being (Kelloway et al., 2012). Other cross-sectional studies demonstrate how leadership training is associated with enhanced capability and behaviour, which have previously been found to predict employee well-being (Arnold et al., 2007; Barling and Carson, 2013; Kelloway et al., 2012; van Dierendonck et al., 2004).
Team/workgroup support interventions★
Perceived support within the workplace is an important predictor of individual resilience to stressful workplace exposures (Harvey et al., 2011b). There have been surprisingly few interventions developed and tested to enhance perceived support in the workplace, although one randomised control study found a 1 week workplace support group intervention reduced depression symptoms amongst workers (Ahola et al., 2012). While this, taken together with observational findings on the importance of workplace support provide some evidence for interventions aimed at enhancing perceived support within a team or workgroup, greater clarity is required regarding the possible benefits and what type of interventions (e.g. instrumental vs emotionally focussed) are most helpful.
Psychosocial safety climate★
There is growing evidence supporting further evaluation of strategies promoting a culture of psychological safety within the organisation, often termed a ‘psychosocial safety climate’ (PSC). PSC refers to the perception of appropriate balance between management concern for their workers’ mental health and productivity. To date observational evidence has suggested that employees working in organisations with a high PSC display better mental health (Dollard et al., 2012), and that PSC moderates the impact of bullying on posttraumatic stress symptoms (Bond et al, 2010). However, there is a lack of intervention studies examining whether enhancing PSC in isolation is an effective workplace mental health strategy.
Effective change management★
There is prospective observational evidence for the mental health benefits of effective management strategies during times of significant organisational change. A longitudinal field experiment compared employees who received open and realistic communication about their organisation’s merger, to employees who received limited information and found a reduction in psychological stress, uncertainty, and absenteeism in those who received the open communication (Schweiger and Denisi, 1991). However, despite such promising findings from nearly three decades ago, there has since been a lack of high-quality intervention studies examining the effect of such change management strategies on employee mental health.
Strategy 3: enhancing personal resilience
The third strategy involves improving employee mental health by enhancing an individual’s coping skills and personal resilience. This can be attempted via direct resilience training or programmes of lifestyle modification or other forms of coaching.
Mindfulness or CBT based resilience training for high-risk occupations★
The potential value of resilience in a psychological context lies in its potential as an internal resource that can mitigate the negative effects of stress or other mental health challenges. A number of prospective studies of high-risk workers, such as first responders, have found that standardised measurements of resilience, are independent predictors of future mental health problems (Wild et al., 2016). As a result, the majority of research on workplace resilience training interventions has been conducted with high-risk occupations, such as the military or emergency services. Reviews focused on the armed services have found some beneficial effects for resilience training such as pre-deployment cognitive behaviour therapy-based programmes or stress inoculation training (SIT) (Hourani et al., 2011). There are also a number of emerging randomised controlled trials of mindfulness-based resilience training programmes in other occupational groups that generally show positive effects on a number of employee well-being outcomes, including resilience (Aikens et al., 2014; Erogul et al., 2014). The majority of studies demonstrating an ability to shift levels of resilience use either cognitive-behavioural therapy or mindfulness techniques, with some evidence that a mixed intervention approach, incorporating both mindfulness and cognitive behavioural therapy, facilitates the greatest change in resilience levels (Cerezo et al., 2014; Kahn et al., 2016; Sood et al., 2014). The degree to which changes in an employee’s level of resilience, as measured by a resilience scale, are related to true protection against new onset mental disorder remains unclear.
Cognitive behavioural therapy (CBT) based stress management programmes★★
The World Health Organization defines work-related stress as ‘the response people may have when presented with work demands and pressures that are not matched to their knowledge and abilities and which challenge their ability to cope’. The relationship between perceived ‘stress’ in the workplace and risk of mental illness is complex, though there is evidence that perceived work stress can contribute to the development of mental health issues (Stansfeld and Candy, 2006). While the evidence for general workplace stress management programmes is mixed, the evidence is more consistent for stress management programme based on cognitive behavioural therapy (CBT) (Bhui et al., 2012; Richardson and Rothstein, 2008; Seymour and Grove, 2005; Tan et al., 2014).
Coaching★
While work-based coaching interventions have been subject to limited empirical evaluation, there are some small randomised controlled studies that have demonstrated improvements in well-being (Green et al., 2006; Spence and Grant, 2007) and reductions in depression and stress. However, there remains considerable variation in interventions examined. For example, an executive coaching programme for executives and senior managers based on a cognitive-behavioural solution-focused approach included one group half-day leadership training workshop and four individual executive coaching sessions over 8–10 weeks (Grant et al., 2009), a 10-week cognitive-based solution-focussed life coaching group programme for employees (Green et al., 2006) and group-based life coaching sessions delivered by peers or professional life coaches (Spence and Grant, 2007). Such variation in approach, delivery mode and target group means it has yet to be determined which form of coaching, if any, is most effective and for whom.
Workplace physical activity programmes★★
The positive effects of physical activity on mental health are well documented (Harvey et al., 2010), raising the possibility that interventions promoting physical activity in the workplace could help promote individual resilience. For example, a randomised controlled trial of a work-based 24-week aerobic and weight training programme resulted in a significant reduction of worker’s depression symptoms (Atlantis et al., 2004), while a 13-week off-worksite exercise programme found an improvement in overall psychological health for employees who received the intervention compared to controls (Brand et al., 2006).
Strategy 4: promoting and facilitating early help-seeking
Early help-seeking for mental health symptoms is still uncommon within the general community (Roness et al., 2005). There are a number of ways that workplaces can help to reduce the barriers to help-seeking, including offering well-being checks, peer-support programmes, psychoeducation and counselling services.
Well-being checks/health screening★
Although this approach is often promoted, the evidence for workplace health screening is mixed. A randomised controlled trial of screening for depression in a US workplace found that screening followed by an outreach and care management programme not only resulted in lower self-reported depression but also significantly higher job retention rates and increased number of hours worked (Wang et al., 2007). A similar model of early identification and help-seeking evaluated in Australia was found to be cost-effective with increased employee well-being (Whiteford et al., 2005). However, while these studies demonstrated screening interventions were able to identify individuals at-risk, a number of other large RCTs have failed to find any benefit to screening, even among high-risk populations (Rona et al., 2017). Any screening process also runs the risk of identifying false positives, causing unnecessary anxiety or stigma via falsely labelling temporary distress as an illness or sign of vulnerability. A recently developed prediction algorithm has demonstrated promise in the use of more complex models to identify individuals at-risk for onset of common mental disorders among working populations (Fernandez et al., 2017). Thus, optional wellbeing checks or screening backed up by appropriate responses to positive results may have an important role in promoting early help-seeking, but mandated screening is not without risks and overall benefits are yet to be definitively shown.
Peer support schemes★★
To date, peer support schemes have mainly been implemented in high-risk occupations such as emergency services, but there is increasing interest in their use in other work situations (Gullestrup et al., 2011). Peer support schemes involve providing additional mental health training to a selection of workers. These peer support workers are not expected to provide psychological assistance, but to instead provide more general support to other employees and to help identify those who might require professional assistance. Recently, a number of studies have examined the impact of such peer support schemes within the military, most notably the UK Armed Forces, and a number of other high-risk occupations. While the results of early RCTs failed to find peer support to be associated with reduced symptom levels (Greenberg et al., 2010), later non-randomised studies have shown a range of other potential benefits, including increased perceived support, reduced barriers to help seeking and possible reductions in sickness absence (Whybrow et al., 2015).
Workplace counselling★
Workplace counselling is a common intervention that provides psychological support services for employees, often as part of an Employee Assistance Program (EAP). Although these services are widely implemented in many large organisations, the overall evidence for their effectiveness is limited. In 2001, the British Association for Counselling and Psychotherapy published a report on workplace counselling which reported it to be an effective treatment for mental illness (McLeod, 2001). However, these findings were later found to be significantly compromised by the methodological limitations of the review (Henderson et al., 2003). Since then a further systematic review on the effectiveness of workplace counselling found some evidence for reducing psychological problems (McLeod, 2010); however, this was again largely limited to lower quality studies and weak assessment methods.
Avoid emotional debriefing following a traumatic event★★★
Psychological debriefing is an intervention that promotes emotional ventilation and detailed recollection after exposure to trauma, with the intention of reducing distress and psychiatric morbidity. While very popular and widely used, multiple randomised controlled trials and systematic reviews have now demonstrated that routine use of psychological debriefing is not only ineffective in reducing psychological injury such as post-traumatic stress disorder (PTSD), but it has the potential to be harmful by re-exposing the individual to traumatic memories (Roberts et al., 2009; Rose et al., 2002).
Mental health education of employees★
There are a variety of mental health education programmes offered in workplaces, though few have been formally evaluated. An exception to this is Mental Health First Aid, a training programme that helps individuals assist others who may be experiencing mental illness. A randomised control trial of Mental Health First Aid training found a number of benefits among employees, including improvements in mental health knowledge, stigmatising attitudes, confidence and provision of help to others (Kitchener and Jorm, 2004). Additionally, the intervention group displayed significantly greater improvement in their own levels of depression and anxiety symptoms. Such findings need to be balanced against other publications, which have argued that the evidence base for psychoeducation is yet to be established that psychoeducation may carry additional risks (Wessely et al., 2008).
Strategy 5: supporting recovery and return to work
The fifth and final strategy identified in the framework is based upon an increasing acknowledgement in the literature of the need for work-focused interventions in order to improve the occupational outcomes of those with mental illness. The term ‘recovery’ in respect to mental health is a hopeful concept that forms the basis of a recovery-oriented model of care widely implemented among mental health services internationally (Bellack, 2006).
Work focused psychological therapy★★
Programs focused on improving the occupational outcomes of mentally ill workers may not necessarily be conducted in the workplace, but they will need to be supported by the workplace if they are to be effective. There is now promising evidence that work-focused psychological interventions are effective at improving occupational outcomes for individuals with PTSD (Noordik et al., 2010; Stergiopoulos et al., 2011), obsessive compulsive disorder (OCD) (Noordik et al., 2010) and adjustment disorders (Arends et al., 2012 [see supplementary material]). A Cochrane review has also evaluated the effectiveness of interventions facilitating the return to work of individuals with adjustment disorders and found that problem solving therapy (PST) assisted individuals in achieving a partial return to work (Arends et al., 2012) sooner compared to treatment as usual.
Workplace adjustments and support★
Although there is limited high-quality evidence concerning specific workplace interventions that support the recovery of individuals with mental illness, a meta-synthesis of qualitative research found that strategies such as support from supervisors and colleagues, as well as workplace adjustments like partial sickness absence can facilitate return to work in those suffering common mental disorders (Andersen et al., 2012). Similarly, small-scale studies have suggested that supervisor support may be a potential determinant for increasing the likelihood of return to work among ill employees (Janssen et al., 2003; Nieuwenhuijsen et al., 2004; Post et al., 2005), although some failed to show any direct effects of positive supervisory behaviour on return to work outcomes (Nieuwenhuijsen et al., 2010). Guidelines based on a Delphi consensus study have now been developed to provide workplaces with assistance in managing the absence and supporting the return to work of employees suffering from common mental disorders (Reavley et al., 2012).
Conclusion
Mental ill health among the working population is an increasing public health problem. As a result, the workplace needs to be a key location for initiatives aimed at reducing the burden of mental ill health. There is great interest among employers and policy makers about how workplaces can be made more mentally healthy. However, to date, there has been very limited evidence-informed guidance on this topic.
In this article, we have proposed a framework of how the design, management, training, structures and processes of work might be modified to enhance employee mental health and wellbeing, a description of evidence supporting this approach, and identified gaps where intervention studies are required. While these findings demonstrate that there is much that workplaces can do to enhance the mental health and wellbeing of their employees, they also highlight the limitations of the currently available research. There is uncertainty about the role that broader contextual factors, such as compensation policy and access to services, may play in limiting the effectiveness of any changes in the workplace. In the future, cross-discipline collaboration will be needed to address these issues.
While each workplace needs to develop tailored solutions, the five strategy framework proposed in this review will hopefully provide a simple guide for employers and those advising them to use when judging the adequacy of existing services and considering opportunities for further enhancements. Collaboration between academics, employers and policy makers will be needed if workplaces are to fulfil their potential role in mental health promotion.
Footnotes
Acknowledgements
S.B.H. conceptualised and planned this article. The framework proposed was sequentially developed by S.B.H., N.G. and M.H. over a number of years. The literature search was conducted by L.T., S.J. and M.M. both K.P. and S.B.H. wrote the initial draft of this manuscript with all authors commenting on revisions. All authors have supported and approved publication of the final manuscript.
Declaration of Conflicting Interests
Samuel Harvey and Sadhbh Joyce are associated with the Black Dog Institute and Rawmind Coach, who deliver mental health interventions in the workplace.
Funding
This work was supported by funding from beyondblue with donations from the Movember Foundation, the Australian National Mental Health Commission and NSW Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.