
Abstract
Background:
The importance of social connectedness in supporting public mental health is well established. However, the reverse causal pathway (that psychological ill-health leads to reduced social connectedness) remains a dominant perspective among mental health practitioners. Our analysis aimed to provide a rigorous test of the directionality of this relationship.
Method:
A cross-lagged panel analysis of a large longitudinal national probability sample (N ≈ 21,227), the New Zealand Attitudes and Values Survey, was used to assess the bidirectional longitudinal relationship between social connectedness and mental health, controlling for baseline levels of both variables and demographics.
Results:
Social connectedness was found to be a stronger and more consistent predictor of mental health year-on-year than mental health was of social connectedness.
Conclusion:
These results further demonstrate how the psychological resources conferred by social connectedness can act as a ‘social cure’ for psychological ill-health, and provide the strongest evidence to date for the direction of this relationship in the general community.
Social connectedness is critical for good health. People with limited social connectedness have poorer mental and physical health, including increased depression (Cruwys et al., 2014a), and die earlier than those with strong social connectedness (for a meta-analysis, see Holt-Lunstad et al., 2010). There is widespread consensus in the public health and epidemiology literatures that social connectedness causally protects and promotes mental health (Kawachi and Berkman, 2001; Perkins et al., 2015). However, models that specify the reverse causal relationship are also common among clinicians; the loss of social connectedness is frequently described as a consequence of mental illness. Indeed, a key diagnostic criterion of major depressive disorder is that symptoms ‘
Social connectedness and mental health
The focal emphasis of research on social connectedness and mental health has differed somewhat between public health scholars, who have tended to emphasise social determinants of health (Almedom, 2005), and mental health researchers, especially clinical psychologists (Hirschfeld et al., 2000), who have tended to emphasise the consequences of mental ill-health (e.g. depression) for social functioning. In this section, we review each of these perspectives in turn.
Social connectedness as a protective and curative factor in mental health
Social capital is a multidimensional concept that includes both structural (‘objective’) and cognitive (‘subjective’) components (Berry and Welsh, 2010). As a social determinant of health, structural social capital (e.g. frequency of social participation, marital status) refers to material indicators of adequate social relationships. Much work has investigated its influence on both physical and mental health (e.g. Ding et al., 2015; Helliwell and Barrington-Leigh, 2012; Stafford et al., 2008). However, mounting evidence suggests that subjective appraisals of social relationships (which are our focus in this paper, e.g., self-reported social support or belonging), or ‘complex’ operationalisations of social capital (where both structural and cognitive elements are present), are more strongly associated with psychological health than purely objective measures (e.g. whether a person lives alone; Holt-Lunstad et al., 2010).
Many of the studies exploring the relationship between social connectedness and health have utilised controlled longitudinal designs in large, representative samples. For example, Luo et al. (2012) found that the subjective experience of loneliness (as distinct from objective social isolation) robustly predicted later onset of depressive symptoms and early mortality in a large nationally representative sample of older US adults. In a longitudinal study of Californian adults, Patterson and Veenstra (2010) found that chronic loneliness was associated with early mortality, which they argued could be explained by increased depression and maladaptive health behaviours. Yu et al. (2015) measured both cognitive and structural social capital and found that both predicted subsequent mental health in a multilevel cross-lagged longitudinal structural equation model. Finally, in a longitudinal study, Cruwys et al. (2013) found that older adults who made new social connections (by joining new groups) over 2 years were more likely to recover from depression (if initially depressed), and were less likely to develop depression (if initially not depressed).
A smaller number of experimental studies have also found that interventions which aim to improve social connectedness have benefits for mental health. For example, people with mental illness who joined recreational and therapy groups which target social isolation experienced clinically significant reductions in depression and anxiety symptoms (Cruwys et al., 2014b; Haslam et al., 2016).
In addition to the strong empirical case for the causal link from social connectedness to mental health, several theoretical frameworks also argue for this relationship. These include models which posit that social relationships fulfil a fundamental psychological need for belonging (e.g. Baumeister and Leary, 1995) and, more recently, the social identity approach to health (or the ‘social cure’ perspective, Jetten et al., 2012). This model states that our social relationships (and in particular, our social group relationships) act as psychological resources that protect one’s health, particularly in times of adversity (see, for example, Praharso et al., 2017; Seymour-Smith et al., 2017).
To summarise, the dominant public health and epidemiological perspective on social connectedness is that it is a resource (a form of capital) that an individual can draw upon in times of need, and which will protect their mental health.
Poor social functioning as a consequence of mental illness
In the clinical literature, however, social connectedness is usually operationalised as social functioning. This is an individual-level skill (or deficit): ‘the degree to which a person is able to fulfil various roles in different social environments’ (p.2913, Renner et al., 2014; Segrin, 2000). Social functioning is often explicitly specified as either a consequence of mental illness, or as a symptom of the condition itself. For example, the Diagnostic and Statistical Manual for Mental Disorders (DSM-5) specifies that a key criterion of depression is withdrawal from social situations, as well as a lack of interest or engagement in important social roles such as work or close relationships (APA, 2013). In a review of social functioning and depression, Hirschfeld et al. (2000) described the ‘enormous personal, social, and economic impact of depression, due in no small part to the associated impairments in social functioning, is often underappreciated’ (p. 268). Many other disorders are also formally described as impairing social functioning, including anxiety disorders, substance-related disorders and autism-spectrum disorders (APA, 2013). The implication of such diagnostic criteria is that reduced social connectedness is an outcome of the disorder (rather than, say, a risk factor).
The task of determining the direction of the causal relationship between mental health and social connectedness is further complicated by the use of social functioning as an indicator of successful remission from mental illness. For instance, Renner et al. (2014) found that social functioning improved in people with major depressive disorder after the administration of psychotherapy. Even when impaired social functioning has been found to predate clinical diagnosis, clinical researchers have often framed this as a premorbid (i.e. prodromal) symptom; an early warning sign of the onset of mental illness (particularly for schizophrenia and bipolar disorders; Addington et al., 2008; Cornblatt et al., 2007), rather than as a risk factor per se.
From a clinical perspective, then, social functioning is impaired by mental illness, is sometimes an early symptom of mental illness onset, and recovers as a consequence of effective treatment targeting the psychological disorder. The conceptualisation of social functioning as a criterion for recovery or remission (Zimmerman et al., 2006), however, makes it difficult to determine whether the catalyst in such studies is improvement in social connectedness or improvement in mental health.
Reciprocal relationships between social connectedness and mental health
In their systematic review of social capital and mental illness, De Silva et al. (2005) raised the possibility of a reciprocal relationship between the two constructs, highlighting the limitations of the predominantly cross-sectional evidence purporting a causal link and recommending further longitudinal research. To our knowledge, though, there are only two extant systematic investigations of the possible reciprocal relationships between social connectedness and mental health. Ding et al. (2015) conducted a lagged fixed effects regression analysis in Australian adults using the Household, Income, and Labour Dynamics in Australia Survey (HILDA). They found that structural social capital (operationalised as community participation) and mental wellbeing were positively and reciprocally related. Yu et al. (2015) conducted a multilevel cross-lagged structural equation analysis of mental and physical health and social capital (operationalised as loneliness, social participation and social networks) in British adults using the British Household Panel Survey. Their analysis found that social participation (membership in community groups and other organisations) was positively and reciprocally associated with mental health. Furthermore, reported loneliness was negatively, but not reciprocally, associated with mental health. In other words, Yu et al. (2015) found some evidence that subjective social capital (loneliness) was a stronger predictor of mental health than the converse. While both are strong studies, neither completely accounts for the bidirectional relationships between social connectedness and mental health. The study conducted by Ding et al. (2015) did not have a measure of wellbeing available at each wave of data, and so could not use a full crossover design at each timepoint. Furthermore, Yu et al. (2015) used general measures of wellbeing rather than clinically validated scales for assessing mental health in the general population. Most importantly, neither study was specifically designed to directly compare the strength of each directional relationship, which may limit their persuasiveness for sceptical clinicians.
The current research
In this study, we perform a robust test of the relationship between social connectedness and mental health in both directions, that is, (1) Does a lack of social connectedness lead to poorer mental health? and (2) Does poorer mental health lead to a lack of social connectedness? We extend previous work on bidirectional relationships between these constructs, proposing that both statements are true, but that social connectedness may be a stronger longitudinal predictor of mental health than mental health is of social connectedness. We made this prediction based on both on the emerging empirical evidence (e.g. Cruwys et al., 2013; Yu et al., 2015) and on the strength of theoretical models of this relationship, which have developed substantially in recent years (for a review, see Haslam, 2014). However, given the lack of comprehensive past comparisons, this was a tentative prediction.
We utilise the New Zealand Attitudes and Values Survey (NZAVS), which is a longitudinal survey of New Zealand residents that commenced in 2009. We chose this dataset due to its large size (N = 21,227 with at least two usable waves of data) and excellent wave-to-wave retention; for its inclusion of suitable measures of social connectedness (e.g. ‘I know that people in my life accept and value me’; included from Wave 1) and mental health (operationalized as distress using Kessler-6, e.g., ‘In the past 30 days, how often did you feel so depressed that nothing could cheer you up?’, included from Wave 2 (Kessler et al., 2003). We conducted a fully cross-lagged panel analysis of social connectedness and mental health for Waves 2–5 of the NZAVS, controlling for age, sex and local area socioeconomic deprivation (NZDep2006, Salmond et al., 2007). Constraints imposed on regression paths in this analysis allow us to test specific hypotheses regarding the relative strength of the longitudinal pathways between social connectedness and mental health.
Our specific hypotheses are as follows:
H1. Social connectedness at each wave will positively predict mental health at the following wave, consistent with the public health and epidemiological perspective
H2. Mental health at each wave will positively predict social connectedness at the following wave, consistent with the clinical perspective
H3. The relationship between social connectedness and lagged mental health will be stronger than the relationship between mental health and lagged social connectedness.
Method
Sample
The data were drawn from four consecutive waves (Wave 2, 2010, to Wave 5, 2013) of the NZAVS. The NZAVS is a nationally representative 20-year study of New Zealand adult residents that commenced in 2009, with participants randomly selected from the electoral roll. For Waves 2 to 5, wave-to-wave retention was approximately 80% (Dalby et al., 2015; Sibley, 2014a). A total of 21,227 unique participants had data from at least two waves available, which was our N for pooled effects (Sibley and Greaves, 2014).
Measures
Social connectedness
Social connectedness was modelled as a latent variable and measured with three manifest items, adapted from Cutrona and Russell (1987). Participants were asked how accurately these statements described them: ‘I know that people in my life accept and value me’, ‘I know that people around me share my attitudes and beliefs’, ‘I feel like an outsider’ (reversed). The response range was 1, very inaccurate, to 7, very accurate. Higher scores on the variable indicate feeling more socially connected
Mental health
Mental (ill-)health was operationalised as distress, and modelled as a latent variable and measured with six manifest items from the Kessler-6 scale (Kessler et al., 2003). The Kessler-6 scale is a set of six questions that were developed to screen for serious mental illness in the general population. The question stem ‘In the past 30 days, how often did …’ prefaced items about distress, e.g., ‘you feel so depressed that nothing could cheer you up?’, ‘you feel worthless?’. The response range was 0, none of the time, to 4, all of the time. Higher scores on this variable represent a greater degree of distress.
Control variables
Participant age in years at Wave 2, sex (0 = female, 1 = male), and socioeconomic status were included as time-invariant covariates in the main analysis. Participant socioeconomic status was derived from the average 2006 New Zealand Socioeconomic Deprivation Index score for all waves in which participants provided data (1 = most affluent, 10 = most impoverished, Salmond et al., 2007). This score is derived from aggregate census information about the relative affluence of each sub-neighbourhood geographic area (a ‘meshblock’ of approximately 80 people, Sibley, 2014b).
Statistical analyses
We conducted fully cross-lagged panel analysis to investigate the reciprocal causal relationship between social connectedness and mental health. Following Cole and Maxwell (2003) and Martens and Haase (2006), we conducted the analyses in several steps. First, we constructed and tested measurement models for each wave to confirm that social connectedness and mental health were empirically distinct constructs. Second, we tested autoregressive models separately for social connectedness and mental health, where the latent focal variable at each wave was regressed on the latent focal variable at the previous wave. The test of autoregressive models demonstrates the stability of the focal constructs across time. Third, we constructed a full cross-lagged model that combines both autoregressive models and adds cross-lagged paths between social connectedness and mental health. The fully cross-lagged model represents all reciprocal relationships across time and offers a test of H1 and H2. Finally, as a test of H3, we compared the fit of the fully cross-lagged model to an alternative model in which the bidirectional relationships were constrained to be equal.
Missing data, estimation and model fit
We used Full Information Maximum Likelihood (FIML) estimation for the focal structural equation analyses. FIML maximises the informational value of observed data including incomplete cases, which are common due to wave-to-wave attrition and booster sampling in longitudinal panel surveys such as the NZAVS. The FIML method produces less biased parameter and standard error estimates than listwise deletion or expectation maximisation (Enders and Bandalos, 2001), especially when the data are not missing completely at random, or a substantial proportion of the dataset is considered missing. FIML is as effective as multi-step methods such as multiple imputation (Newman, 2003; Wothke, 2000).
To evaluate and compare model fit, we used the chi-square goodness-of-fit statistic, the comparative fit index (CFI), the standardized root mean square residual (SRMR) and the root mean square error of approximation (RMSEA) and, as is convention for RMSEA, its 90% confidence interval (CI). For large and complex data sets, the chi-square statistic is less useful for evaluating fit due to the very high power to detect minor perturbations away from exact fit, but it is included here as convention. A CFI value above 0.95 indicates excellent fit compared to the null model, a SRMR value below 0.08 indicates excellent fit (Hu and Bentler, 1999), and an RMSEA value below 0.05 indicates good fit, where the 90% CI lower and upper bounds fall below 0.05 and 0.10, respectively (Chen et al., 2008).
Results
Descriptive statistics
Descriptive statistics for focal variables of distress and social connectedness, and correlations between summary measures of each variable, are presented in Table 1. At the whole-sample level, distress and social connectedness were descriptively stable across time. At Wave 2, participants’ average age was 44.67 years old (standard deviation [SD] = 14.66), and 62.04% (N = 14,273) described their gender as female. The average socio-economic deprivation for the sample was 4.90 (SD = 2.77).
Descriptive statistics and correlations for summary measures of distress and social connectedness.
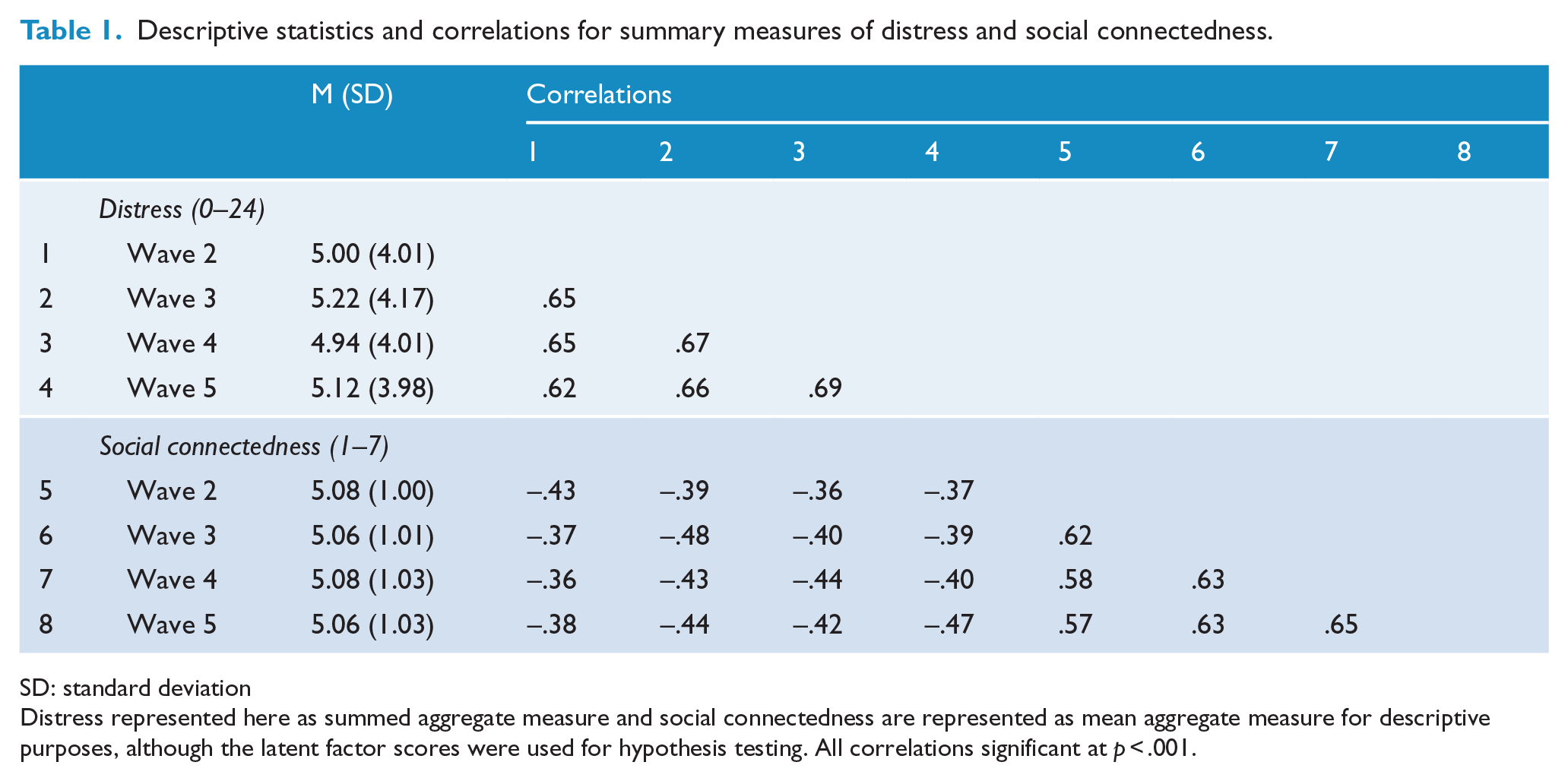
SD: standard deviation
Distress represented here as summed aggregate measure and social connectedness are represented as mean aggregate measure for descriptive purposes, although the latent factor scores were used for hypothesis testing. All correlations significant at p < .001.
Measurement and autoregressive models
A series of confirmatory factor analyses were conducted to evaluate and compare two possible measurement models for each occasion. The first model included two co-varying latent variables for each occasion: distress, manifested in the six observed variables, Kessler-1…Kessler-6 and social connectedness, manifested in the three observed variables, Social connectedness-1…Social connectedness-3. The second model for each occasion had a single latent variable, wellbeing, manifested in all nine observed variables. Across every wave, the two-factor model fit the data significantly better than the one-factor model, χ2difference(df = 1) = 462.65–1804.70, ps < 0.001.
An autoregressive model for distress regressed the latent variable of distress on each previous wave. The loading of each observed variable on the latent variable were constrained to be equal across the four waves (i.e. time-invariant factor loadings). The autoregressive model fit the data well, χ2(21516, df = 228) = 5286.63, p < 0.001, CFI = 0.96, SRMR = 0.07, RMSEA = 0.0321 (90% CI = [0.0314, 0.0329]). Standardised factor loadings ranged from 0.53 to 0.80. Standardised stability estimates ranged from 0.76 to 0.80.
An autoregressive model for social connectedness regressed the latent variable of social connectedness on each previous wave. As with mental health, factor loadings were constrained to be equal across waves. The autoregressive model fit the data well, χ2(21547, df = 39) = 182.14, p < 0.001, CFI = 0.995, SRMR = 0.06, RMSEA = 0.0131 (90% CI = [0.0112, 0.0150]). Standardised factor loadings ranged from 0.48 to 0.73. Standardised stability estimates ranged from 0.86 to 0.91. The good fit of the autoregressive models demonstrates the stability of each latent construct across time.
Cross-lagged models
Two fully cross-lagged models were tested. The first model (‘non-stationary model’) did not constrain the weighting of the structural paths over time, which allowed the magnitude of the bidrectional relationships between distress and social connectedness to vary across time. The second model (‘stationary model’) constrained lagged structural paths to be equal, to test whether the cross-lagged relationships between distress and social connectedness were invariant across time. Both models fit the data well (Table 2). A χ2 test revealed that constraining structural paths to be equal led to a small, but significant loss of fit, χ2difference(df = 8) = 34.14, p < 0.001, indicating that the reciprocal relationships between distress and social connectedness were not stationary over time. Thus, in order to demonstrate a robust test of H3, which also imposes additional path constraints, we summarise the path estimates of both models below.
Fit indices and statistics for structural equation models.
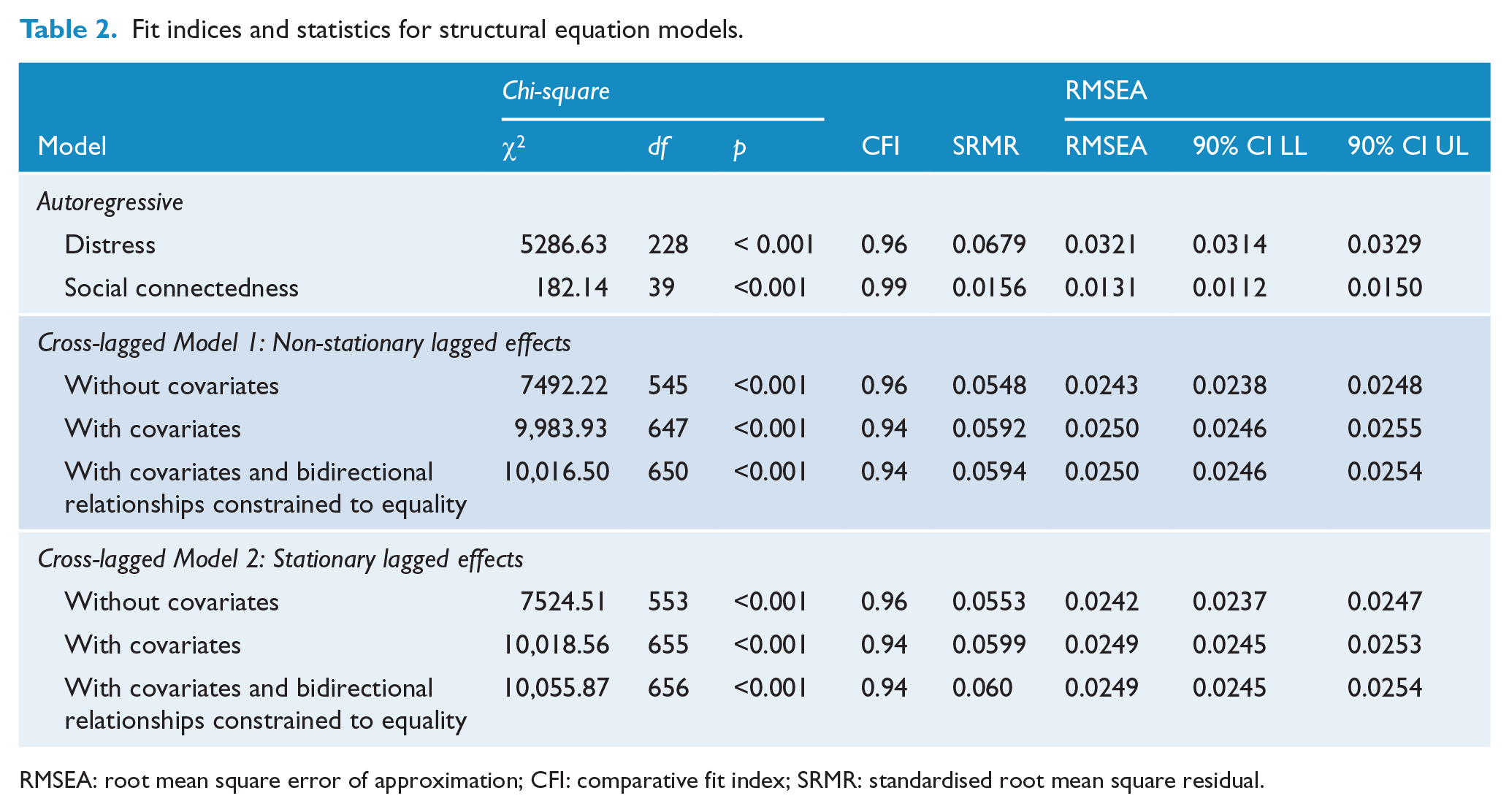
RMSEA: root mean square error of approximation; CFI: comparative fit index; SRMR: standardised root mean square residual.
Figure 1 provides an overview of the relationships in the non-stationary model. Social connectedness predicted decreased distress at every subsequent wave (BW2-W3 = −0.157, SE = 0.026, 95% CI = [−0.208, −0.107], BW3-W4 = −0.115, SE = 0.022, 95% CI = [−0.158, −0.072], BW4-W5 = −0.167, SE = 0.014, 95% CI = [−0.194, −0.140]) consistent with H1. Distress predicted decreased social connectedness at two of the three subsequent waves (BW2-W3 = −0.067, SE = 0.033, 95% CI = [−0.133, −0.002]; BW3-W4 = 0.013, SE = 0.029, 95% CI = [−0.045, 0.070]; BW4-W5 = −0.080, SE = 0.020, 95% CI = [−0.119, −0.041]) broadly consistent with H2. The model fit well (Table 2), and the pattern of relationships did not change when covariates of gender, sex, and deprivation were excluded from the model. To test H3, we tested a model in which the bidirectional relationships were constrained to be equal. This model had worse fit than the unconstrained model, χ2difference(df = 3) = 32.57, p < 0.001, suggesting that the reciprocal relationships between distress and social connectedness differed in magnitude.
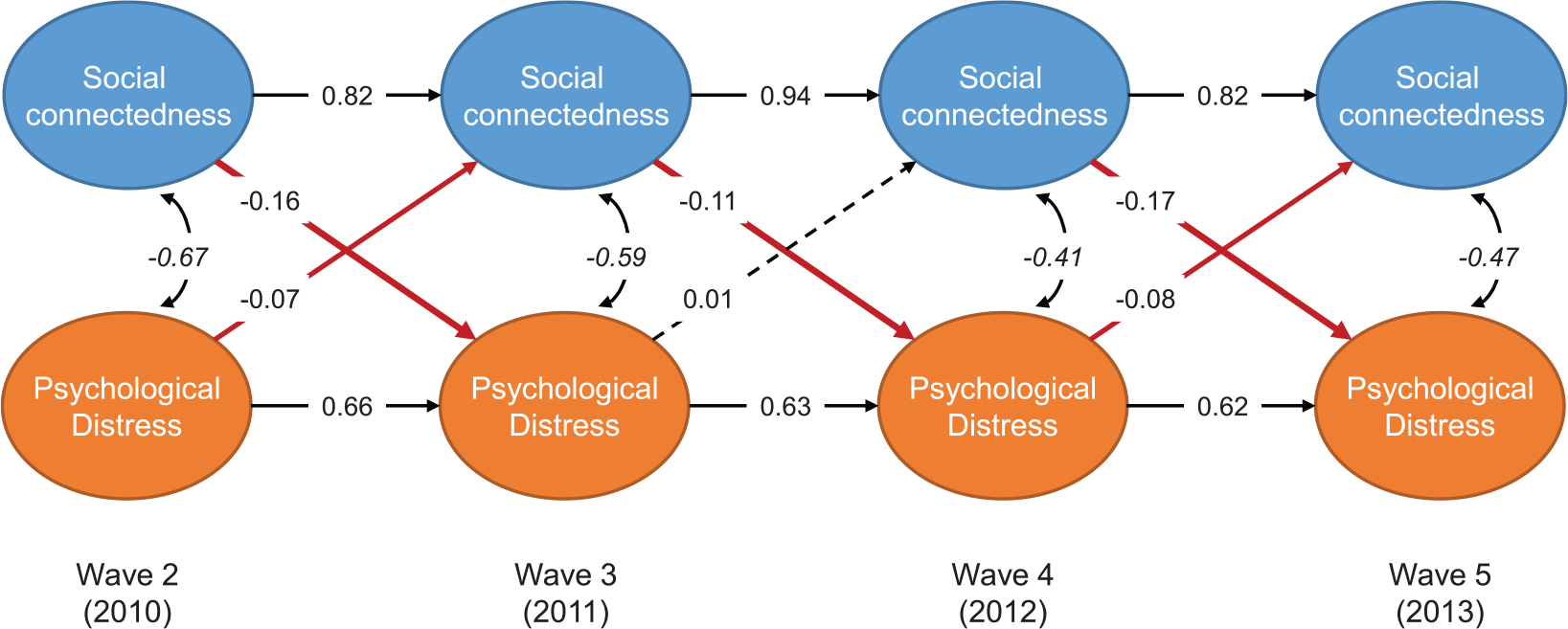
Non-stationary lagged effects cross-lagged analysis between distress and social connectedness.
Figure 2 illustrates the stationary model. Social connectedness predicted decreased distress at a one-year lag (B = −0.155, SE = 0.011, 95% CI = [−0.175, −0.134]) consistent with H1. Distress predicted decreased social connectedness at a one-year lag (B = −0.045, SE = 0.013, 95% CI = [−0.070, −0.020]) consistent with H2. The pattern of significant and non-significant relationships did not change when covariates of gender, sex and deprivation were excluded from the model. A model in which the bidirectional relationships were constrained to be equal fit worse than the unconstrained model, χ2difference (df = 1) = 37.31, p < 0.001, supporting H3 which stated that the reciprocal relationships are different in magnitude.
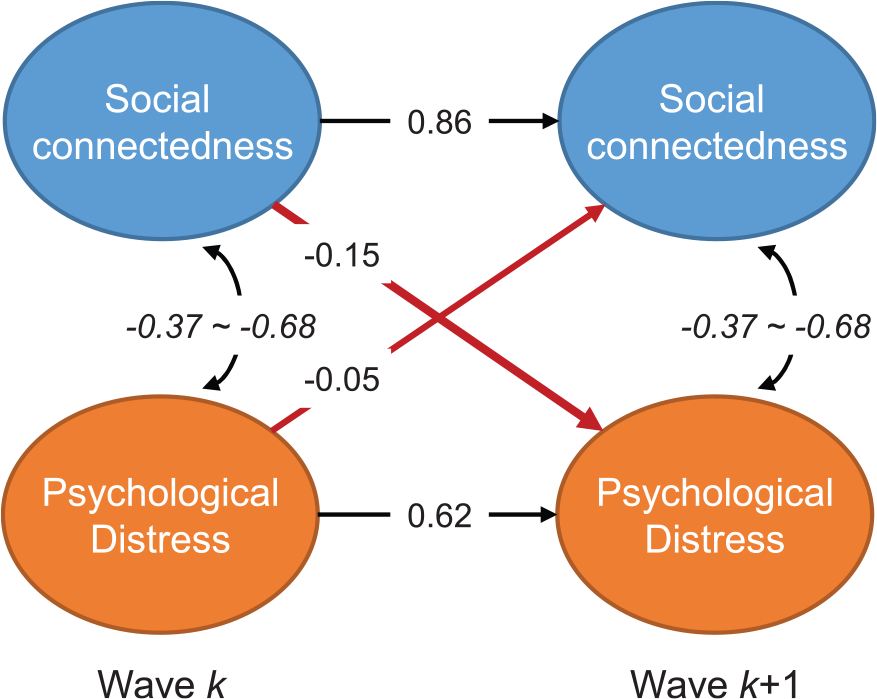
Stationary lagged effects cross-lagged analysis of distress and social connectedness.
Discussion
We investigated and compared the bidirectional relationships between social connectedness and mental health using a longitudinal nationally representative survey of New Zealand adult residents. The public health and epidemiological literatures state that social connectedness (usually operationalized with particular emphasis on subjective connection with others) promotes mental health, and thus we hypothesised (H1) that social connectedness would be positively associated with mental health (measured as lack of distress) one year later. In contrast, some clinical psychology and psychiatric literatures state that mental illness leads to reduced social connectedness (usually operationalised as impaired social functioning), and thus, we hypothesised (H2) that mental health would be positively associated with social connectedness at the following observation. Finally, drawing from the emerging work on social identity and health (Cruwys et al., 2013; Jetten et al., 2012), we tentatively hypothesised (H3) that social connectedness would be more strongly associated with subsequent mental health compared than the reverse.
All three hypotheses were supported: A cross-lagged panel analysis of Waves 2–5 of the NZAVS revealed that social connectedness and mental health were positively and reciprocally associated across time, and that social connectedness predicted subsequent mental health more strongly than mental health predicted subsequent social connectedness. Together, these results support a growing body of evidence that has demonstrated the importance of social connectedness in promoting and maintaining mental health in the general population (Cacioppo et al., 2006; Cruwys et al., 2014a; De Silva et al., 2005; Yu et al., 2015).
Implications for theory and practice
One barrier to advancing understanding of social connectedness (and its link to health) has been great diversity in the way this construct is conceptualised and measured. For instance, epidemiological research has often focused on more included both subjective and structural components of social relationships (e.g. Almedom, 2005; Ding et al., 2015), whereas clinical research has typically focused on self-reported impairment in one’s capacity to connect with others (APA, 2013; Evans et al., 2014). In the current paper, we measured social connectedness as the subjective appraisal of the quality and quantity of social relationships available to a person (consistent with Cruwys et al., 2014a). This was based on a constellation of recent work demonstrating that (1) it is the subjective experience of disconnection to others, not actual amount of contact with others, that is most debilitating for health (e.g. Luo et al., 2012; Sani et al., 2012); (2) recent large longitudinal analyses of similar research questions have focused on structural capital such as community participation (e.g. Ding et al., 2015); (3) the cognitive and structural components of social capital may be only weakly correlated (Giordano and Lindstrom, 2010); and (4) complex (multi-component) measures of social capital better predict health outcomes than structural measures alone (Holt-Lunstad et al., 2010). Nevertheless, it is possible that measures of social connectedness which aligned more closely with conceptualizations of social functioning or social capital may have led to different results.
Our conceptualisation of social connectedness is also consistent with theoretical work which has proposed that it is the subjective sense of connectedness to a group that is the ‘active ingredient’ in social relationships. This is what gives social relationships their power to promote and maintain mental health in depressed individuals (Cruwys et al., 2013), in the general population (Greenaway et al., 2015; Helliwell and Barrington-Leigh, 2012), and among people experiencing stressful life transitions such as retirement (Steffens et al., 2016). Furthermore, these results underline the point that it is subjective psychological appraisals that make social connectedness work to support and promote mental health in a community – simply ‘showing up’ at social and recreational events is unlikely to be sufficient to benefit wellbeing (Cruwys et al., 2014b). From this, we might infer that public health policies must target more than social participation in order to promote trust and social cohesion within a community (Giordano and Lindstrom, 2010).
The relationship between social connectedness and mental health has been discussed in the public health epidemiology literature several decades (for an interdisciplinary review, see Almedom, 2005; for a systematic review, see De et al., 2005). In some nations, public health policy has begun to incorporate lessons from this work by emphasising the importance of social relationships and social support for mental health and wellbeing (e.g. National Mental Health Commission, 2014). In medical and psychiatric settings, however, social functioning is often explicitly conceptualised as an outcome or indicator of mental ill-health, and thus is rarely considered a primary point of intervention or persisting risk factor for relapse (Backs-Dermott et al., 2010).
The tension between public health researcher and clinical practitioner perspectives on social connectedness and mental health may undermine efforts to create and promote effective mental health policy, and impede investigation of effective treatment for psychological disorders. The findings of the current paper move the field forward by demonstrating that while the relationship between social connectedness and mental health is reciprocal, social connectedness is particularly important in promoting mental health over time. These findings also support a growing movement in social psychiatry to attend to ‘horizontal epidemiology’, or the risk factors that are common across psychological disorders, rather than merely the (sometimes arbitrary) categorical boundaries between conditions (Cieza et al., 2015; Haslam, 2003). Interventions which focus on improving social connectedness, as an example of one ‘transdiagnostic’ risk factor, are likely to improve mental health now and in the future, regardless of current mental health status (see, for example, Haslam et al., 2016).
Strengths, limitations, and future directions
Methodologically, a strength of this paper is in its use of the NZAVS, a large national probability sample of New Zealand adults. Other work that has investigated social connectedness and health in panel and longitudinal data have employed subscales of the General Health Questionnaire (Yu et al., 2015) or items from the Medical Outcomes Study Short Form (Ding et al., 2015). In the current study, we assessed mental health using a validated measure of distress, the Kessler-6 scale (Kessler et al., 2003) and a measure of social connectedness that has its provenance in the psychological literature on belonging (Cutrona and Russell, 1987). Of course, it is possible that a measure of mental health that relied on strict diagnostic criteria may have yielded different patterns. However, previous studies have suggested that the pathway from social connectedness to mental health may be even stronger among vulnerable groups. For instance, Cruwys et al. (2013) found that joining social groups was particularly beneficial for people who had depression symptoms in the clinical range. Future work should test associations between social connectedness and diagnosed mental health conditions over time.
An additional possible limitation is suggested by the finding that the relationships between social connectedness and mental health may be non-stationary: when we constrained the cross-lagged relationships to be equal year-on-year, this led to a loss of model fit. One possibility that might explain the model instability is unmeasured exogenous variables. For instance, between Wave 2 (2010) and Wave 3 (2011), a magnitude 6.3 earthquake struck New Zealand South Island’s largest city of Christchurch, killing 185 people and causing widespread property damage, displacement and psychological trauma among residents (Osborne and Sibley, 2013). Although there were no mean differences in mental health or social connectedness across the whole sample between Waves 2 and 3, it is possible that the magnitude and direction of the relationship between social connectedness and mental health could have been affected by such a disaster.
Conclusion
In sum, this study provides the strongest evidence to date that social connectedness is a stronger predictor of subsequent mental health than the reverse. We investigated these reciprocal relationships over time in a nationally representative dataset of New Zealand adults (N ≈ 21,227). The findings speak to the value of interventions to improve social connectedness, such as facilitating engagement with existing group memberships and building new group memberships, for mental health. Furthermore, these results challenge mental health practitioners to conceptualise the social deficits in their patients as precursors, as well as symptoms or consequences of, mental illness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.