
Abstract
Objective:
One of the main characteristics of social anxiety disorder is excessive fear of social evaluation. In such situations, anxiety can influence gaze behaviour. Thus, the current study adopted virtual reality to examine eye gaze pattern of social anxiety disorder patients while presenting different types of speeches.
Methods:
A total of 79 social anxiety disorder patients and 51 healthy controls presented prepared speeches on general topics and impromptu speeches on self-related topics to a virtual audience while their eye gaze was recorded. Their presentation performance was also evaluated.
Results:
Overall, social anxiety disorder patients showed less eye gaze towards the audience than healthy controls. Types of speech did not influence social anxiety disorder patients’ gaze allocation towards the audience. However, patients with social anxiety disorder showed significant correlations between the amount of eye gaze towards the audience while presenting self-related speeches and social anxiety cognitions.
Conclusion:
The current study confirms that eye gaze behaviour of social anxiety disorder patients is aversive and that their anxiety symptoms are more dependent on the nature of topic.
Introduction
A marked characteristic of social anxiety disorder (SAD) is fear of negative evaluation by others in social or performance situations. In such situations, socially anxious individuals draw attention away from external cues and instead attend to internal cues (Clark and Wells, 1995; Rapee and Heimberg, 1997). This contributes to persistence of fear because doing so prevents extinction by denying future opportunities to experience the feared cues in the absence of the unconditioned stimuli. Avoidance of eye contact plays a critical role in this process (Clark and Wells, 1995; Horley et al., 2004; Öhman, 1986). It may help socially anxious individuals alleviate immediate anxiety. However, in the long term, extinction of fear is unlikely, as avoidance of eye gaze would be perceived negatively by social interaction counterparts (Alden, 1992; Meleshko and Alden, 1993). For example, a person who avoids making an eye contact during a conversation may give an impression to the conversation partner that the person is hesitant to engage in the interaction. This may lead the partner to be unfavourable and this would in turn provoke further social anxiety. In addition, it is possible to miss positive feedback from interaction counterparts, which may help the person to overcome anxiety (Lowe et al., 2012; Schneier et al., 2011).
Existing literature well illustrates eye gaze behaviour of individuals with SAD. Vigilance-avoidance hypothesis predicts that patients with SAD quickly direct gaze towards emotional stimuli and, at the same time, quickly disengage from them (Mansell et al., 1999; Mogg et al., 2004; Weeks et al., 2013). Eye tracking studies using facial stimuli have demonstrated that individuals with SAD show less fixation on the facial area (Moukheiber et al., 2010), particularly avoiding the eye region (Horley et al., 2003, 2004). Such behavioural pattern becomes more evident as emotional intensity of the stimuli increases (Mogg et al., 2007).
Gaze aversion is more likely when social-evaluative threat is imminent (Garner et al., 2006). Indeed, research has shown that socially anxious individuals make less eye contact during conversations (Baker and Edelmann, 2002). They also exhibit hyperscanning, spend more time fixating at regions not occupied by the audience (Chen et al., 2015) while presenting a speech. In situations that require social interaction, interestingly, research has shown that performance of individuals with SAD may depend on task demand. In a study that compared performance in conversation and speech, SAD patients showed a performance deficit only during conversations. Performance in speech presentation did not show an actual deficit; however, patients had a distorted view that their performance was not satisfactory (Rapee and Lim, 1992; Voncken and Bögels, 2008). A possible explanation would be that conversation requires more complex, subtle reactions to the counterpart than presenting a speech.
While literature on performance of individuals with SAD in public speaking is accumulating, the current study attempted to examine how speech type influences gaze behaviour of individuals with SAD using virtual reality (VR). Use of VR for treatment of various psychiatric disorders has been proven effective (e.g. Emmelkamp et al., 2002; Garcia-Palacios et al., 2002; Rothbaum et al., 2006) and SAD is no exception (e.g. Anderson et al., 2013). The current study hoped to acquire a strict control over exposure to feared situation by using VR. In addition, unlike previous studies that focused only on audience’s facial expressions, this study introduced a more real-world scenario by emphasising audience’s actions and attitudes (e.g. signs of boredom and careful listening). Finally, two types of speeches – prepared speeches on general topics and impromptu speeches on self-related topics – were used in the study. The hypotheses were that self-related, impromptu speeches are more likely to produce aversive eye gaze because they involve self-disclosure. In contrast, preparation would help them alleviate their anxiety, thus resulting in better speech performance.
Methods
Participants
A total of 130 subjects (51 healthy controls [HCs] and 79 patients with SAD) were recruited from the local community. They were screened using the following self-reported questionnaires: Liebowitz Social Anxiety Scale (LSAS, Liebowitz, 1987), Social Interaction Anxiety Scale (SIAS, Mattick and Clarke, 1998), Social Phobia Scale (SPS, Mattick and Clarke, 1998), Beck Depression Inventory (BDI, Beck et al., 1961) and Fear of Negative Evaluation Scale (FNE, Leary, 1983). Patients with SAD had to meet the following inclusion scores in order to participate in the study: LSAS ⩾ 30, SIAS ⩾ 34 or SPS ⩾ 24. HCs had to meet the following inclusion scores: LSAS < 30, SIAS < 34, SPS < 24 and FNE < 48. Additionally, they self-reported that they and their family have no history of psychiatric conditions. All participants, regardless of the group, had to satisfy BDI < 21 to exclude current depressive disorders. In an additional clinical interview by a trained psychiatrist, patients were diagnosed with SAD using Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) criteria (Table 1). Patients with a psychiatric diagnosis other than SAD and HCs with any psychiatric diagnosis were excluded from the study. All participants provided written informed consent. The experimental procedure was approved by the institutional review board of Gangnam Severance Hospital.
Demographic and clinical characteristics of participants.
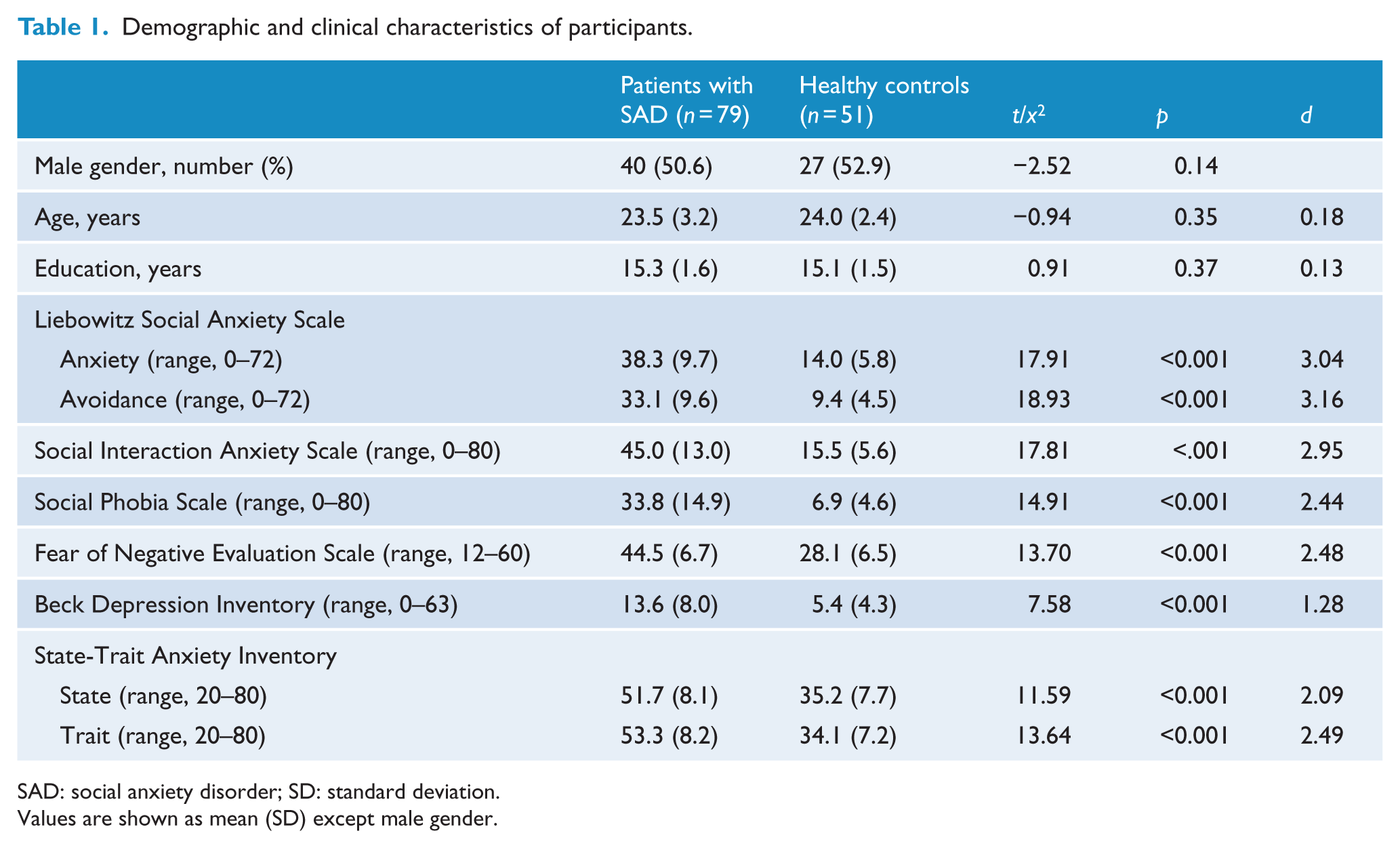
SAD: social anxiety disorder; SD: standard deviation.
Values are shown as mean (SD) except male gender.
Apparatus
The VR scene used in the experiment had seven people sitting in a seminar room. The scene resembled a typical lecture hall environment. Some of them were hard listeners; they took notes and looked at the speaker throughout the speech, while some of them were not; they showed signs of distraction. These include yawning, talking to others, answering phone calls and looking at the clock (Figure 1). The scene included a relatively large area not occupied by the audience, in order to capture reduction in the amount eye gaze towards the audience in an attempt to avoid them by looking at an empty spot.

The audience display presented during the experiment. The area indicated by the red line shows the region of interest.
The VR device used in the experiment includes a head mounted display (HMD, eMagin Z800 3DVisor), a motion tracker (Intersense InterTrax2) and an eye tracker (Arrington Research ViewPoint EyeTracker Systems). The motion tracker was attached to the HMD, allowing the scene orientation to change in synchrony with head movement. The eye tracker recorded participants’ eye movements at a sampling rate of 60 Hz. Calibration was done before the experiment. Participants were asked to look at 12 pre-defined locations in their field of view. When necessary, re-calibration was performed by displaying five fixation points for 6 seconds before the start of each speech presentation. A reference map was created using pre- and post-calibration results and gaze modification was performed on every task by correcting for translations and rotation angles.
Procedure
Participants filled out the State-Trait Anxiety Inventory (STAI-State and STAI-Trait, Spielberger et al., 1983). They were then briefly informed about the experimental procedure.
The task was to present speeches on each of the following six topics: low birth rate, environmental pollution, my strengths and weaknesses, friends I like and dislike, my family and my hobbies. The first two general topics were prepared speeches and the rest were self-related, impromptu speeches. For the topics in the self-related condition, upon receiving a topic, participants had to begin presenting immediately. For the topics in the general condition, participants were given a four-page article on each topic. They were given enough time to read the articles and prepare for speeches.
After preparation, participants began presenting each topic for 2 minutes. The order of the topics was randomly assigned. Their speech was recorded for post-evaluation. They were notified of the remaining time 30 seconds before the end. The recorded speeches were evaluated by an assistant who is blind to the purpose and design of the experiment. The evaluation criteria included the following: fluency, presentation style and content of the speech. The speeches were rated on a 5-point scale. Total scores range from 0 to 48; higher scores indicate better speech performance.
Eye gaze data analysis
The amount of eye gaze was computed using MATLAB. Eye gaze data were first corrected for head motion. The amount of eye gaze was computed by counting the number of fixations at a particular point and translating it into duration. A larger value indicates that more gaze was directed towards the selected area. The region of interest (ROI) was defined by dividing the entire scene into a 60 x 45 grid and selecting areas that were occupied by the audience (Figure 1).
Statistical analysis
The basic structure for the statistical analysis followed a 2 × 2 mixed design, with speech type (self-related, impromptu vs general, prepared) as a within-subjects variable and participant group (HCs vs SAD patients) as a between-subjects variable.
Eye gaze data and self-reported scores or speech performance evaluation for each group were subject to a correlation analysis. Correlations were computed separately for each group, while controlling for BDI scores. Partial correlations were conducted in order to rule out possible effects of depressed mood, for which there was a significant difference between the two groups.
Results
Speech performance evaluation
Data from seven SAD patients were missing because their speech recordings were not saved properly. A total of 51 HCs and 72 SAD patients were included in the analysis. The main effect of speech type was significant, F(1, 121) = 32.68, p < 0.001,
Scores from speech performance evaluation.
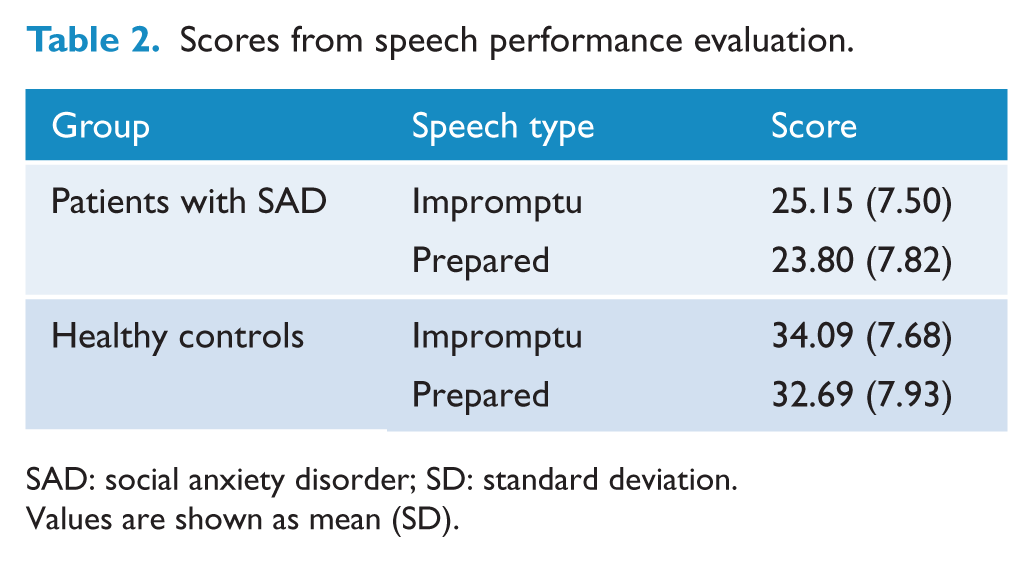
SAD: social anxiety disorder; SD: standard deviation.
Values are shown as mean (SD).
Amount of eye gaze
Eye gaze data from one HC and two SAD patients were excluded due to poor recording quality. The main effect of participant group reached a marginal significance, F(1, 125) = 3.88, p = 0.051,
Importantly, the interaction between the two factors was significant, F(1, 125) = 5.71, p = 0.018,
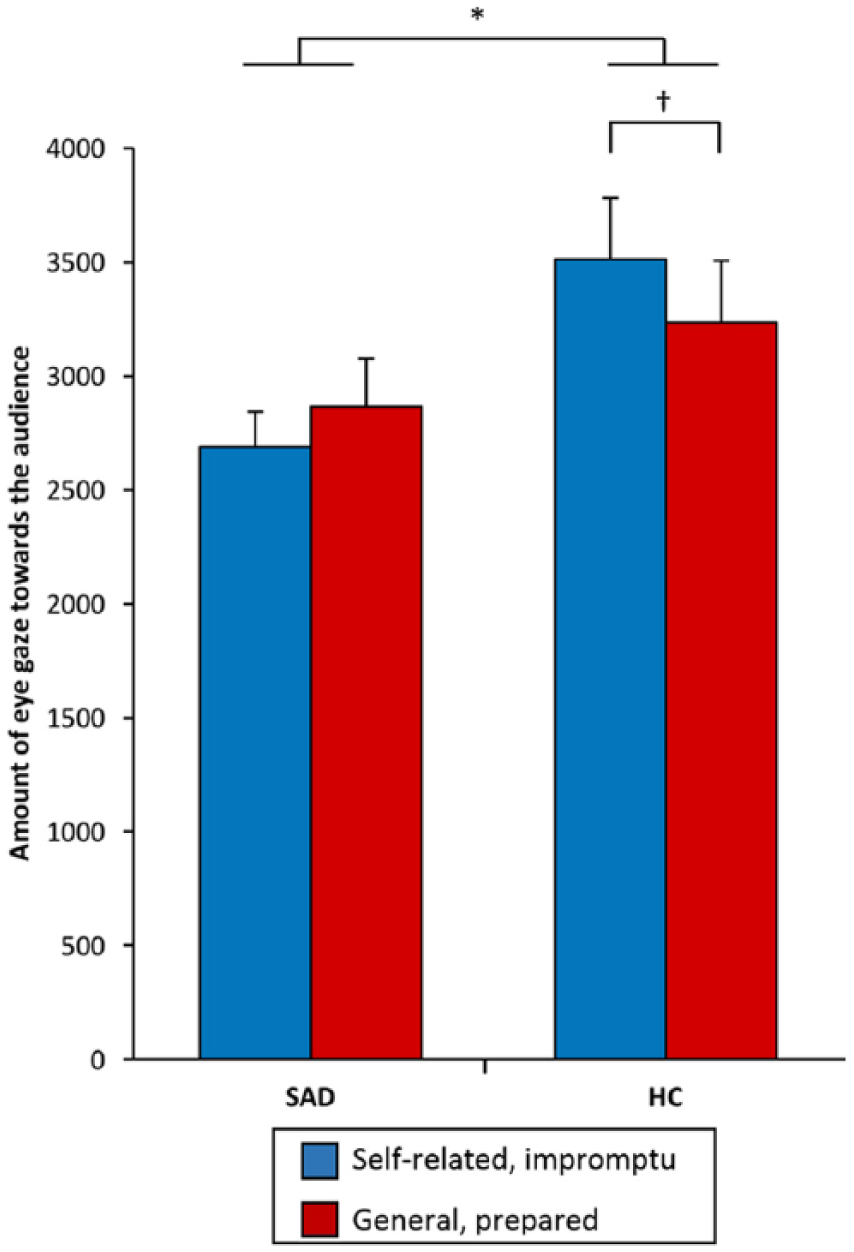
Amount of eye gaze of patients with social anxiety disorder (SAD) and healthy controls (HC) as a function of speech type. Error bars represent standard errors of the mean.
Correlation analyses
A total of 50 HCs and 70 SAD patients were included in the analysis. There was a significant correlation between the amount of gaze towards the audience while giving self-related speeches and FNE scores in SAD patients, r = −0.28, p = 0.022. The amount of gaze towards the audience while presenting general topics significantly correlated with STAI-State and STAI-Trait scores, r = −0.24, p = 0.043 and r = −0.30, p = 0.013, respectively (Figure 3). All other correlations were not significant. No significant correlations were found in HCs.
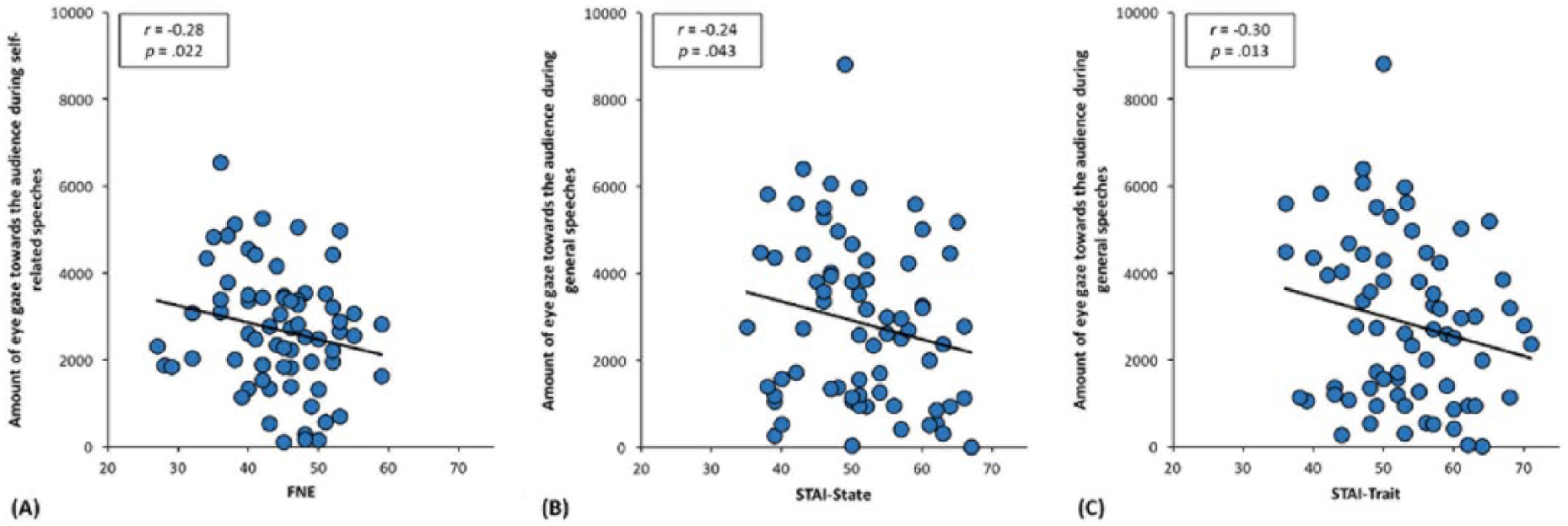
Correlations between the amount of eye gaze and FNE and STAI in patients with social anxiety disorder (SAD). (A) Amount of eye gaze towards the audience while presenting impromptu speeches was inversely correlated with FNE scores in patients with SAD. (B) Amount of eye gaze towards the audience while presenting prepared speeches was inversely correlated with STAI-State and STAI-Trait in patients with SAD. Values in the dashed box represent correlation coefficients and p-values.
Discussion
The current study compared eye gaze allocation of HCs and SAD patients while they presented different types of speeches. Results revealed that overall, SAD patients looked at the audience less than HCs. SAD patients showed no difference in the amount of eye gaze between self-related and general speeches. Speech performance evaluation scores indicated that SAD patients performed worse than HCs. Correlation analysis found significant negative correlations between the amount of eye gaze towards the audience and FNE and STAI-State and STAI-Trait scores. These trends were only evident in SAD patients.
SAD patients did not demonstrate a difference in the amount of eye gaze as a function of speech type. However, they generally looked less at the audience than HCs when presenting speeches. This confirms typical characteristics of SAD patients, that they avert eye gaze away from the audience in order to alleviate anxiety (Weeks et al., 2013). In addition, when they encounter a feared social situation, their internal anxiety symptoms are activated. Therefore, attention is drawn away from external social information and allocated more to internal negative thoughts (Clark and Wells, 1995; Lowe et al., 2012). Such engagement in internal negative thoughts would distract them from improvising and recalling what they had prepared. It also prevents them from taking in positive feedback from the audience, which can help them reduce anxiety (Lowe et al., 2012; Schneier et al., 2011). This result supports Clark and Wells’ (1995) cognitive model of SAD. Attending to internal cues in an attempt to avoid negative evaluation from the audience results in avoidance of eye contact, which in turn elicits negative evaluation from the audience and contributes to persistence of fear.
Perception and evaluation of external cues significantly influence how individuals evaluate their behaviour and adjust it accordingly. Rapee and Heimberg (1997) stated socially anxious individuals show hyper-vigilance for negative feedback on their behaviour, such as yawning and frowning, and tend to detect negative cues earlier than those without anxiety (Schulze et al., 2013). Detection of such external cues may aggravate the situation as it orients individuals’ attention to their mental representation of self to the others, physical and cognitive symptoms. This is supported by the results from the current study; high FNE score in SAD patients correlated negatively with the amount of eye gaze to the audience. Individuals with high cognitive symptoms of social anxiety show more apprehension, and early detection of negative feedback from the audience may lead SAD patients to further avoid making an eye contact with the audience.
Although SAD patients’ amount of eye gaze did not differ, it had correlations with self-reported scores. The amount of eye gaze towards the audience when presenting general, prepared speeches negatively correlated with STAI-State and STAI-Trait scores. When presenting self-related, impromptu speeches, the amount of eye gaze negatively correlated with FNE scores. Given that self-related speeches required participants to talk about themselves and that general speeches involved social issues, the results implies that SAD patients may have been affected more by the type of topic rather than the type of speech.
The self-presentation theory of social anxiety states that anxiety arises when an individual is motivated to make impressions on others, but doubts success in making desired impressions and imagines unfavourable evaluations from others (Schlenker and Leary, 1982; Strassberg et al., 1988). In the current study, SAD patients were forming impressions especially when presenting self-related, impromptu speeches via self-disclosure. Doubts on their ability, expectations about negative evaluations together with their general tendency to talk less (Daly et al., 1995; Pilkonis, 1977) and unwillingness to disclose themselves (Jones and Briggs, 1984; Snell, 1989) may have led them to feel more anxious. As a result, they were less likely to make eye contacts with the audience and this has been reflected in the negative correlation between FNE scores and the amount of eye gaze during self-related, impromptu speeches.
On the other hand, the amount of eye gaze towards the audience during general, prepared speeches negatively correlated with STAI-State and STAI-Trait scores. This implies that SAD patients did not perceive presenting general, prepared speeches as anxiety-provoking because it did not involve self-disclosure as much as presenting self-related, impromptu speeches. Therefore, scores that reflect general anxiety like STAI-State and STAI-Trait would have been able to capture their state better than scores specific to social anxiety.
Uncertainty theory predicts that speakers would look more at the audience when presenting prepared speeches because preparation helps them reduce uncertainty about factors such as wording and content (Witt and Behnke, 2006). However, contrary to this idea, the current study showed that HCs made less eye contact with the audience while presenting general, prepared speeches. There are two possible explanations for this. First, topics for prepared speeches generally required precise knowledge about them. If participants did not have any knowledge on the topic, it is possible that they did not find preparation useful; uncertainty would be likely to persist and presenting speeches would still be difficult. Results of the post-speech performance evaluation support this account. Scores for general, prepared speeches for both groups were lower than those for self-related, impromptu speeches, possibly because topics for general, prepared speeches were innately more difficult. Uncertainty imposed by difficulty of speech topics was not overcome by granting extra time for preparation and it may have been greater than uncertainty experienced when extemporaneously composing content during impromptu speeches. Second, HCs may have looked at the empty area in order to facilitate recalling what they have prepared. Averting eye gaze away from the audience helps to disengage from environmental stimulation. This facilitates cognitive processing and hence speech performance is enhanced (Glenberg et al., 1998).
The current study has several limitations. First, speech topics varied across different speech type, which may have hindered an accurate assessment of speech types. Second, preparation styles were not carefully controlled, which could have introduced variances. Indeed, there are studies that suggest performance in public speaking is closely related not just to the amount of time but also how a speaker prepares for it (e.g. Menzel and Carrell, 1994). Third, social anxiety scores for HCs were seemingly high. However, given the socially inhibited nature of Asian cultures, HCs tend to show high social anxiety scores and scores in the current study were similar to those in other studies. For example, the mean LSAS scores of HCs reported in other studies include Talati et al., 8.1; Sladky et al., 5.3; and Pujol et al., 11.8; cf. Liu et al., 20.0; and Ding et al., 19.2 (Ding et al., 2011; Liu et al., 2015; Pujol et al., 2013; Sladky et al., 2012; Talati et al., 2013). Finally, the way the ROI was defined – dividing the virtual scene into a 60 × 45 grid and selecting relevant blocks – did not allow a separate analysis to be conducted as a function of attitude of the audience. Given the volume of literature that suggests different gaze patterns depending on the audience characteristic, the current study would have been able to provide richer implications if other analyses could be conducted.
In summary, the results of the current study demonstrate that individuals with SAD show an aversive eye gaze behaviour and their anxiety symptoms are more dependent on the nature of topic. Future studies should concentrate on how the nature of topic and eye gaze behaviour are related, with a more refined experimental design that allows separation of audience characteristics.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (2014R1A1A1004553) and the Aspiring Researcher Program through Seoul National University (SNU) in 2014.