
Abstract
Objective:
In adolescents and young adults, depressive symptoms are highly prevalent and dynamic. For clinicians, it is difficult to determine whether a young person reporting depressive symptoms is at risk of developing ongoing mood difficulties or whether symptoms form part of a transient maturational process. Trajectory analyses of longitudinally assessed symptoms in large cohorts have the potential to untangle clinical heterogeneity by determining subgroups or classes of symptom course and their risk factors, by interrogating the impact of known or suspected risk factors on trajectory slope and intercept and by tracing the interrelation between depressive symptoms and other clinical outcomes over time.
Method:
We conducted a systematic review of trajectory studies conducted in cohorts including people aged between 15 and 25 years.
Results:
We retrieved 47 relevant articles. These studies suggest that young people fall into common mood trajectory classes and that class membership and symptom course are mediated by biological and environmental risk factors. Furthermore, studies provide evidence that high and persistent depressive symptoms are associated with a range of concurrent health and behavioral outcomes.
Conclusion:
Findings could assist in the formulation of novel concepts of depressive disorders in young people and inform preventive strategies and predictive models for clinical practice.
Introduction
Depressive disorders, including major depressive disorder (MDD) and dysthymic disorder (DD), are a leading cause of global burden of disease (Ferrari et al., 2013). While MDD is a relatively rare diagnosis in childhood, the incidence of the disorder rises rapidly during adolescence and early adulthood (Hankin et al., 1998; Lewinsohn et al., 1993, 1998). In all, 40% of MDD patients have suffered their first depressive episode by the age of 20 (Eaton et al., 2008), and 50% of patients experiencing MDD before the age of 18 will have further mood episodes in adulthood (Kessler et al., 2001). These numbers have provided an argument for early intervention strategies in MDD that can target symptoms early and prevent progression to a chronic illness stage (Allen et al., 2007). However, intermittent subthreshold depressive symptoms affect 10–20% of all young people (for review, see Wesselhoeft et al., 2013) and may represent a maturational process occurring in a developmental window similar to memory and fear development (King et al., 2013). Targeting evidence-based interventions to those most in need therefore remains a major challenge for clinicians and policy-makers (Jorm, 2015; Purcell et al., 2015).
Longitudinal studies tracking the fluctuations of depressive symptoms in young people over time provide an avenue toward a better understanding of the biological, psychological and social correlates of unfolding mood psychopathology. Generally referred to as ‘developmental trajectory research’, these investigations may also help untangle the considerable heterogeneity in the course of depressive symptoms among young people (Rhebergen et al., 2012). A developmental trajectory describes the course of a behavior or state over age or time. In mental health research, examples include symptom trajectories, organic trajectories (e.g. brain development) or functional trajectories (e.g. time spent in employment).
In this systematic review, we sought to identify publications that have used trajectory statistics to describe the course of mood symptoms over time in older adolescents and young adults, covering people aged between 15 and 25 years. We have focused on this age group because, compared to any other age, mood symptoms are most dynamic in late adolescence and early adulthood and surge to a peak between age 15 and 17 (Kessler et al., 2001). Additionally, in Australia and elsewhere, mental health services with a specific ‘youth’ focus are being developed that broadly cover the age range considered for this article (Brimblecombe et al., 2015; Rickwood et al., 2014). Our findings may be of specific interest to clinicians working in these services.
Method
We carried out a systematic review of the research literature.
Search strategy
We searched the MEDLINE and PubMed databases for articles published before 15 November 2015. The following search terms were entered: trajector* AND (child* OR adolescent* OR young people) AND (depressi* OR mood disorder* OR bipolar disorder*). Retrieved articles were subsequently screened by the authors for inclusion and exclusion criteria in three rounds, first by title, then by abstract and finally by full text content (Figure 1).
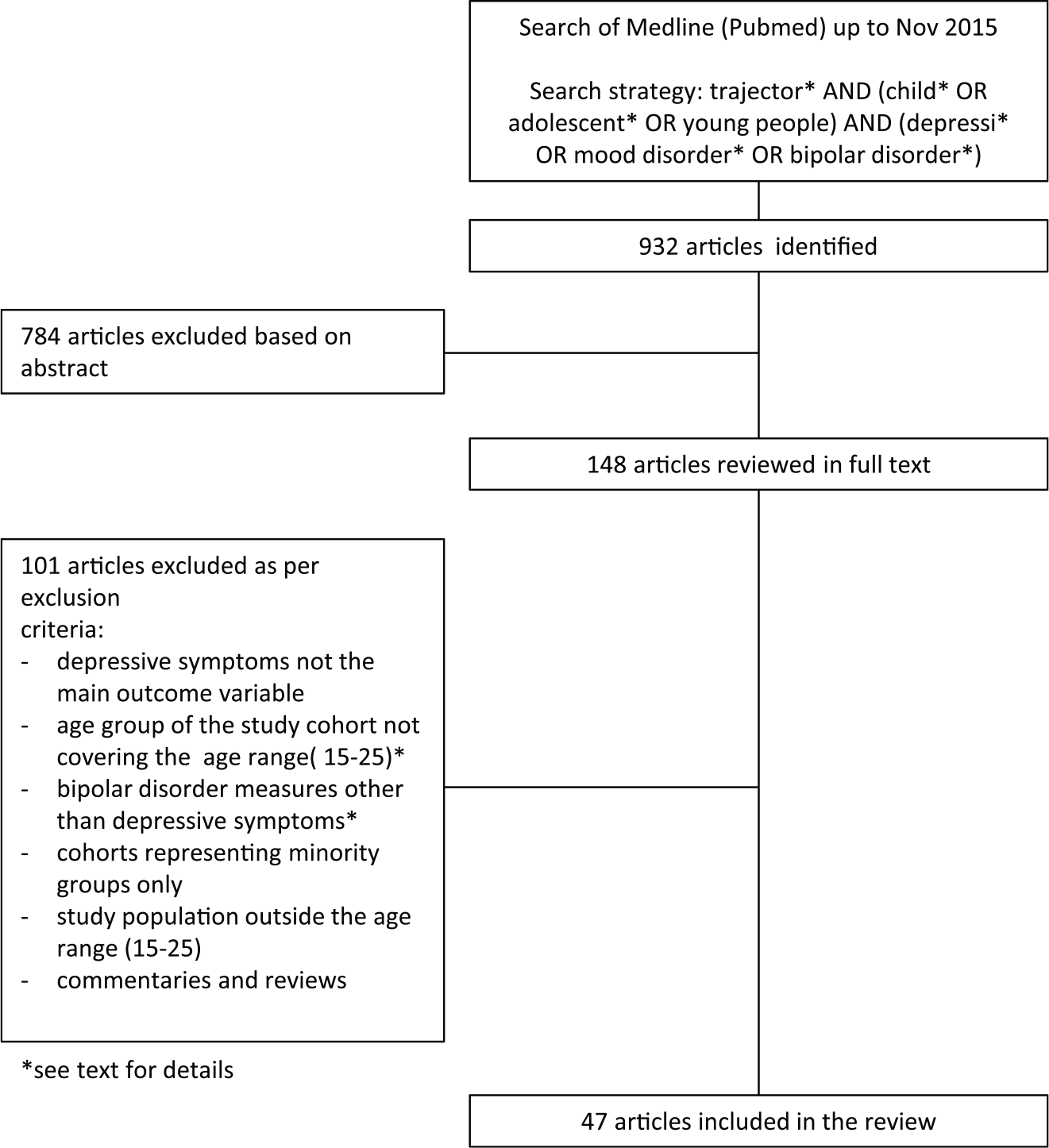
Flow chart of the systematic review process.
The initial PubMed search strategy yielded 932 findings. Following initial exclusion of articles not in English language or not thematically related to mood disorders/young people/mood trajectories, we took 148 articles forward for further analysis by abstract and full text. Of these, 47 articles were found to meet inclusion criteria and were ultimately considered for this review.
Criteria for considering studies
Inclusion criteria were as follows:
Age group of the study cohort predominantly falling into the age range 15-25;
Cohorts representative of a general population;
Depressive symptoms measured longitudinally as primary outcome variable;
Statistical trajectory analyses carried out.
Exclusion criteria were as follows:
Depressive symptoms not the main outcome variable;
Age group of the study cohort not predominantly falling into the age range 15-25;
Bipolar disorder measures other than depressive symptoms;
Cohorts representing minority groups only;
Study population outside the age range (15–25);
Commentaries and reviews.
Bipolar disorder was included in the initial algorithm in order to minimize loss to coverage, but articles reporting non-depressive symptoms were excluded from the review. In order to focus findings on studies examining depressive symptom trajectories in late adolescence and early adulthood in the general population, we excluded articles reporting on minority groups only. We excluded articles reporting age groups not covering the age range of interest (15–25) and commentaries and reviews. In order to be considered relevant for age range, a study had to cover at least 2 years of the lower end of the target range of interest (e.g. 15–17) or 5 years of the upper age range (i.e. 20–25 years)
Results
In total, 47 articles were included in the review (Tables 1–3). Thematically, the articles could be grouped as follows: (1) studies describing the number and shape of depressive symptom trajectories and describing risk factors for specific mood symptom trajectories (Figure 2(a), Table 1); (2) studies examining the contribution of specific and predefined risk factors to depressive symptom trajectories (Figure 2(b), Table 2); and (3) studies investigating trajectories concurrent with depressive symptoms (Figure 2(c), Table 3).
Studies describing the number and shape of depressive symptom trajectories and describing risk factors for specific mood symptom trajectories.
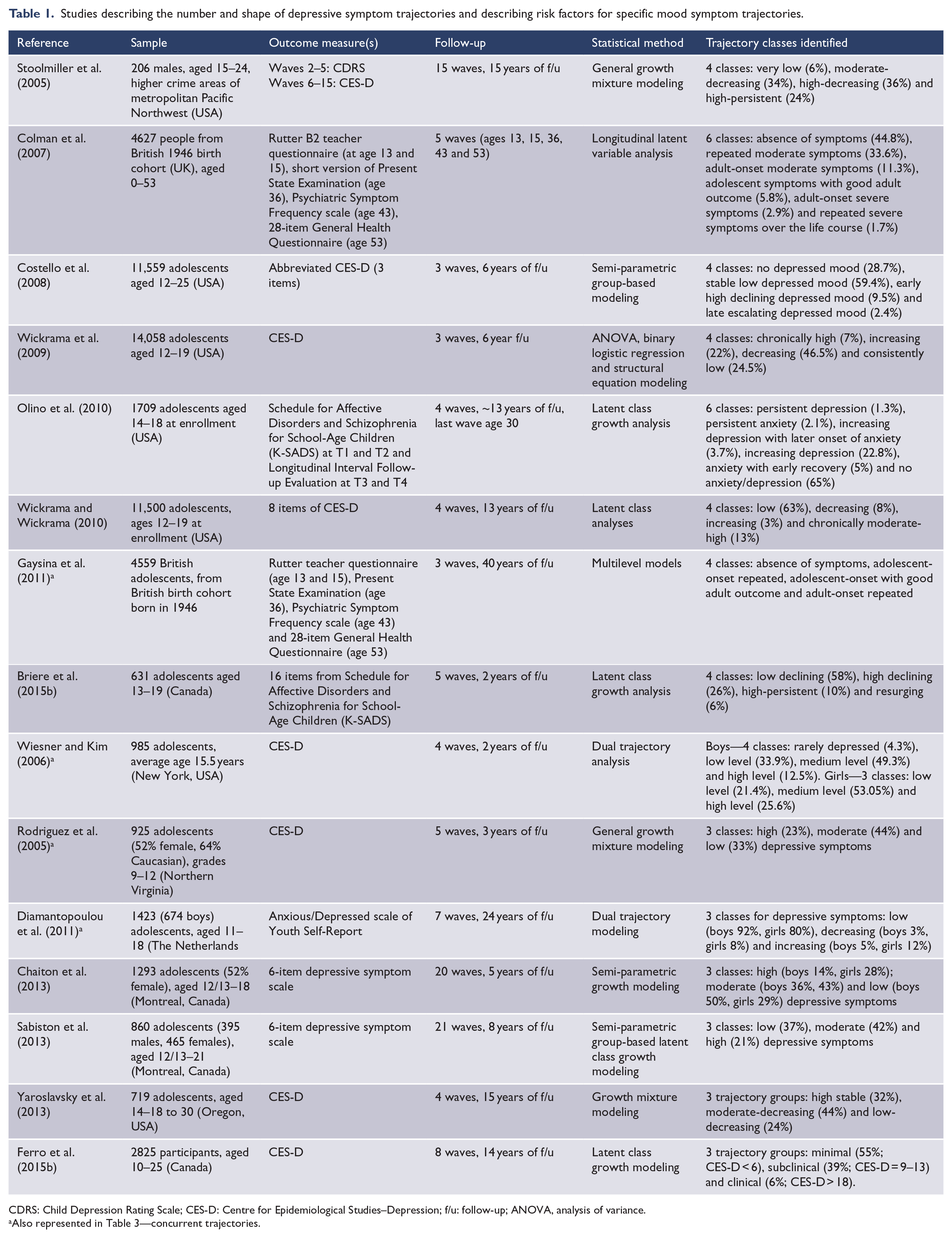
CDRS: Child Depression Rating Scale; CES-D: Centre for Epidemiological Studies–Depression; f/u: follow-up; ANOVA, analysis of variance.
Also represented in Table 3—concurrent trajectories.
Studies examining the contribution of specific and predefined risk factors to depressive symptom trajectories.
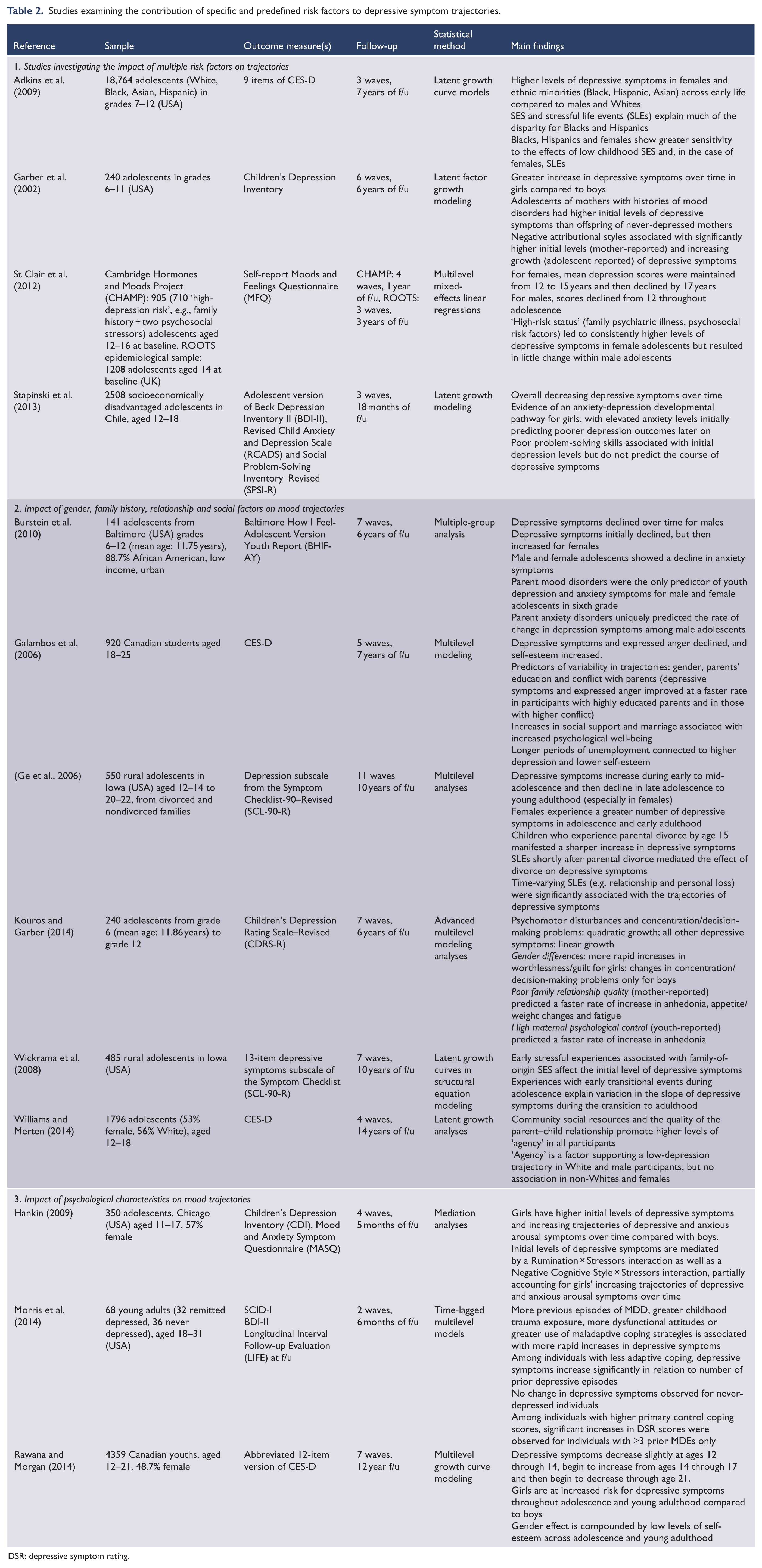
DSR: depressive symptom rating.
CES-D: Centre for Epidemiological Studies–Depression; f/u: follow-up; SCID-1, Structured Clinical Interview for DSM-IV Axis I Disorders; MDD, major depressive disorder; MDE, major depressive episode.
Studies describing concurrent trajectories of depressive symptoms and other longitudinally measured factors.
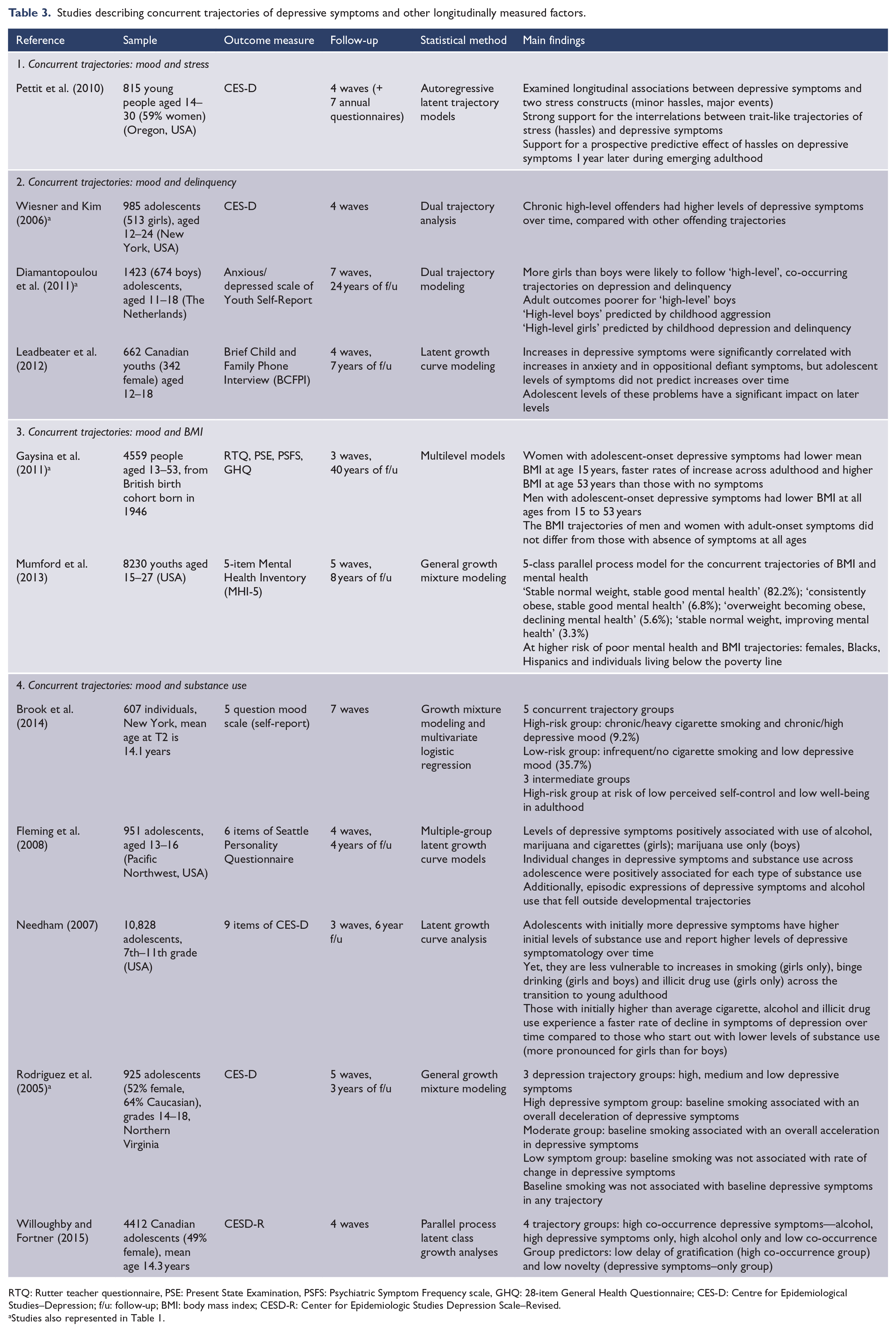
RTQ: Rutter teacher questionnaire, PSE: Present State Examination, PSFS: Psychiatric Symptom Frequency scale, GHQ: 28-item General Health Questionnaire; CES-D: Centre for Epidemiological Studies–Depression; f/u: follow-up; BMI: body mass index; CESD-R: Center for Epidemiologic Studies Depression Scale–Revised.
Studies also represented in Table 1.
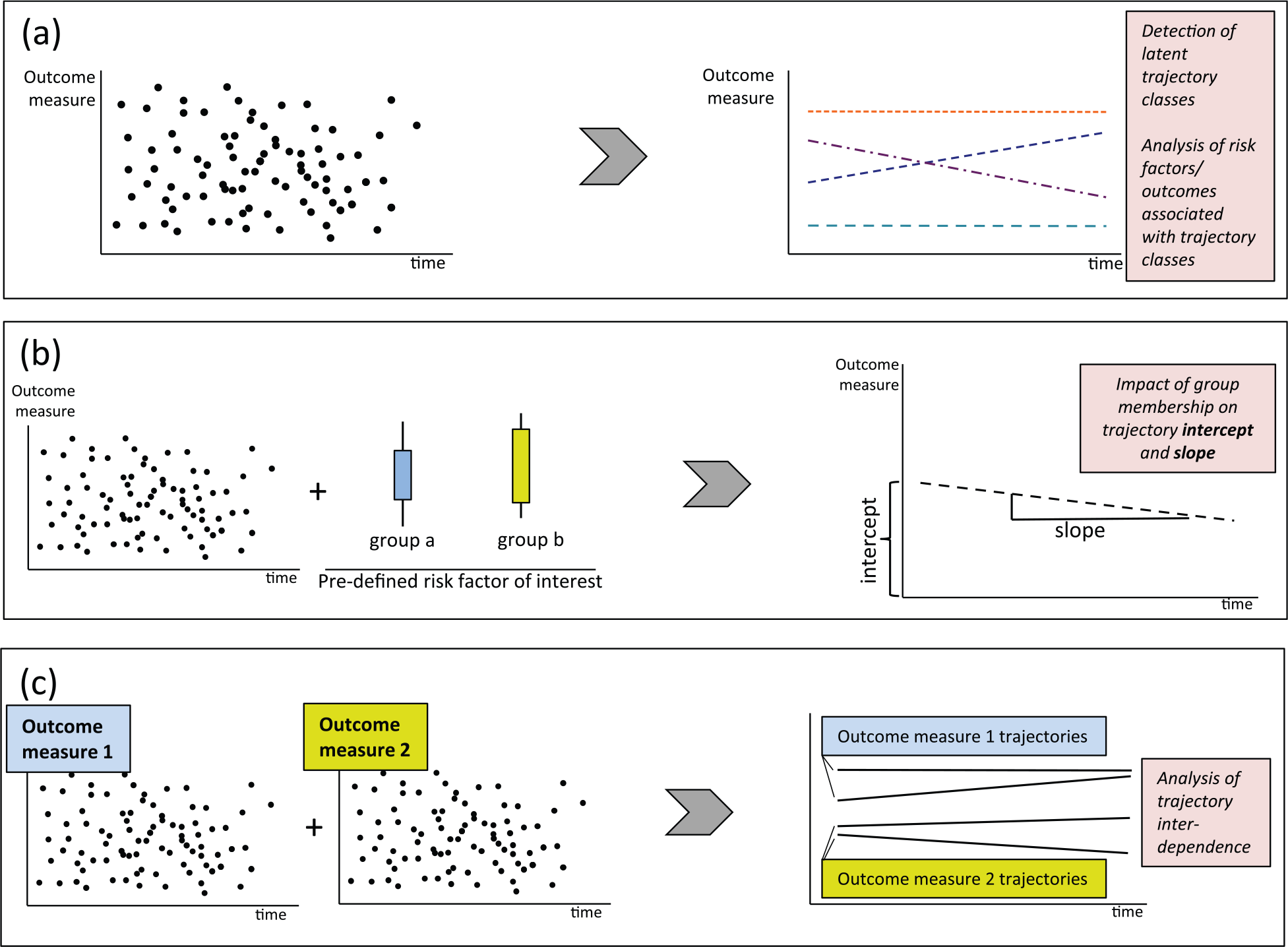
Three types of studies investigate depressive symptom trajectories in young people: (a) Data-driven driven studies that investigate whether trajectories of the outcome variable (e.g. a measurement of mood) can be statistically grouped. In a second step, studies often aim to identify predictor variables that put people at increased risk of belonging to a particular trajectory class. (b) Hypothesis-driven studies that define experimental groups a priori, according to characteristics of interest and depending on the original research question (e.g. female vs male). The impact of these dichotomies on the outcome variable of interest (e.g. depressive symptoms) at baseline (‘intercept’) and over time (‘slope’) is assessed. (c) Studies investigating the co-occurrence and interdependence of two outcome variables of interest over time (e.g. mood symptoms and substance use).
The first group of studies is data-driven and investigates whether trajectories of the outcome variable (here, a measurement of mood state) can be statistically grouped according to a ‘best-fit’ model (Figure 2(a)). These trajectory groups are then assigned descriptive labels, such as an ‘increasing’ group, a ‘decreasing group’ or a ‘no change’ group (Nagin, 1999). Often, predictor variables (e.g. age, gender, ethnicity) that put people at increased risk of following a particular trajectory are identified in these studies.
The second group of studies is hypothesis-driven and defines experimental groups a priori, according to risk factors of interest and depending on the original research question (Figure 2(b)). For example, predefined experimental groups may include ‘male’ versus ‘female’, or ‘Caucasian’ versus ‘Asian’. Then, the impact of these dichotomies on the outcome variable of interest (e.g. depressive symptoms) at baseline (‘intercept’) and over time (‘slope’) is assessed.
The third group of trajectory analyses investigates the co-occurrence and relationship of two outcome variables of interest over time (Figure 2(c)). For example, such a study may track the joint trajectories of depressive symptoms and anxiety symptoms and come to conclusions about their interdependence (Nagin, 2005).
As shown in Tables 1–3, there is some overlap between the areas since many studies investigating concurrent trajectories also provide separate information on depressive symptom trajectories alone. In the following sections, we describe the main findings identified by these three study types.
Studies describing the number and shape of depressive symptom trajectories and describing risk factors for specific mood symptom trajectories
Sixteen of the retrieved articles applied growth-modeling statistics to longitudinal depressive symptoms data, for the identification of distinct trajectories or ‘classes’ among participants over time (Table 1). It is notable that all but one of these identified analyses arrived at a statistically valid model describing distinct classes, supporting the idea that such a differentiation could represent a true phenomenon within the examined populations.
Shape of depressive symptom trajectories
Overall, the retrieved studies in Tables 1–3 confirm that mood and depressive symptoms are dynamic during emerging adulthood and that symptoms reach their peak around age 15–17 (e.g. Figure 3, Costello et al., 2008). This is consistent with previous literature, describing that depressive symptoms increase during early to mid-adolescence and then continuously decline in the transition from late adolescence to young adulthood (Ge et al., 2006; Rawana and Morgan, 2014) and further into the third decade of life (Pettit et al., 2010). There is evidence that females reach the depressive symptom peak slightly earlier than males (Edwards et al., 2014). Studies also concur that the peak occurs independent of trajectory group membership, indicating that even youths with overall low levels of depression experience an increase in symptoms at this age.
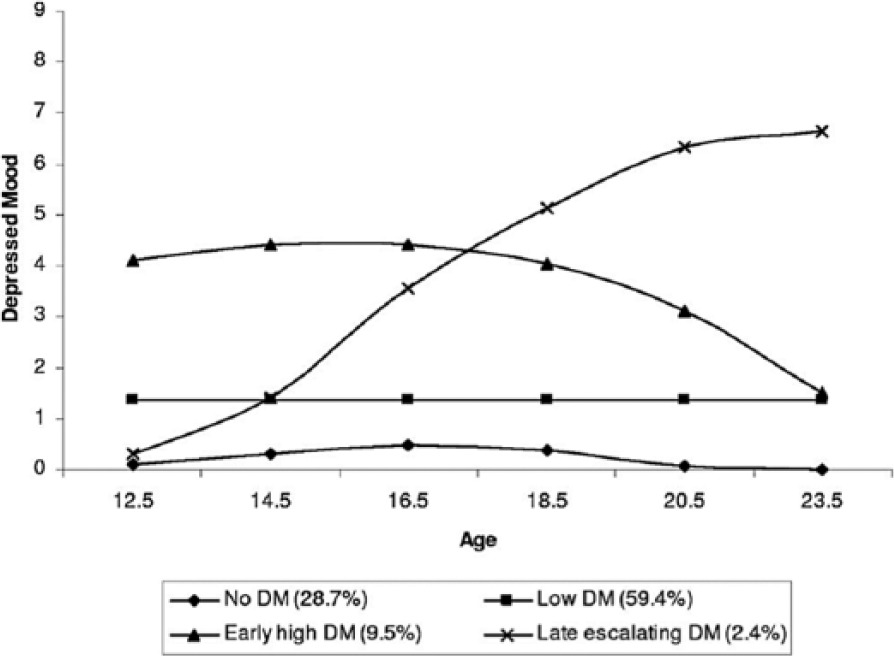
Example of depressive symptom trajectories calculated by a semi-parametric group-based method.
Studies differ considerably in their descriptions of the shape of identified trajectories. Whereas the majority of earlier studies found evidence for several cross-diagonal (i.e. distinctive upward or downward) curves (11 of 15 studies in Table 1; Briere et al., 2015a; Colman et al., 2007; Costello et al., 2008; Diamantopoulou et al., 2011; Gaysina et al., 2011; Olino et al., 2010; Stoolmiller et al., 2005; Wickrama et al., 2009; Wickrama and Wickrama, 2010; Wiesner and Kim, 2006; Yaroslavsky et al., 2013), some other recent analyses seem to support a model of increasing and then decreasing depressive symptoms across all groups in parallel trajectories (4 of 15 studies in Table 1; Chaiton et al., 2013; Ferro et al., 2015b; Rodriguez et al., 2005; Sabiston et al., 2013). On the basis of these latter studies, authors have speculated that a risk group for a young person is likely to be determined relatively early in adolescence, whereas the course of depressive symptoms throughout adolescence is primarily a function of normal youth development (Ferro et al., 2015b). Interestingly, studies that included a large number of young people from disadvantaged social backgrounds (e.g. ethnic minorities or socioeconomic disadvantage) were more likely to report cross-diagonal trajectory group studies that were more likely to report cross-diagnonal trajectory groups compared to studies that were more representative of the general population. One explanation for these cross-diagonal curves is that the presence or absence of severe and enduring psychosocial stressors could ‘shift’ people from a low-risk trajectory they would normally follow into a high-risk group, or vice versa.
Number of depressive symptom trajectories
The number of individual trajectories or ‘classes’ identified by the reviewed studies ranges between 3 and 6. The majority of studies (88%) report either 3 or 4 distinct trajectories. Notably, studies that recruited younger patients from the age of 10 to 12 years and followed them into late adolescence (Chaiton et al., 2013; Diamantopoulou et al., 2011; Ferro et al., 2015b; Sabiston et al., 2013; Yaroslavsky et al., 2013) tend to report fewer trajectories than studies that covered the course of depressive symptoms into middle adulthood (Colman et al., 2007; Costello et al., 2008; Olino et al., 2010; Stoolmiller et al., 2005). This discrepancy may reflect that younger samples have had less lived experience, and there had been a smaller passage of time in which patterns can emerge.
Two types of depressive symptom trajectories feature virtually in all of these studies. First, there is evidence for a class of individuals who experience only minimal depression throughout adolescence and early adulthood. Authors label this class variably as representing ‘no depressed mood’ (Costello et al., 2008), ‘absence of symptoms’ (Colman et al., 2007) or ‘stable low [symptoms]’ (Mezulis et al., 2014). In most studies, a large proportion of assessed subjects fall into this minimal depression class, typically between 40% and 55%. Second, most studies identified a group of patients suffering from consistently high depressive symptoms throughout adolescence and early adulthood. This class is labeled as ‘persistent depression’ (Olino et al., 2010), ‘high stable’ (Yaroslavsky et al., 2013), ‘high-persistent’ (Stoolmiller et al., 2005) or ‘chronically high’ (Wickrama et al., 2009) class. Compared to the low-depression class, there is more heterogeneity among studies with regard to the frequency of high-persistent symptoms in the study populations, ranging between 1.7% in a sample spanning age 13–53 years (Colman et al., 2007) and 32% in a study covering a narrower age range of 14–18 years (Yaroslavsky et al., 2013), with most studies reporting that about 5–15% of participants fall into this group. It is also notable that this high-persistent symptom group tends to show little variability over time in most studies (Stoolmiller et al., 2005).
Moreover, most studies come to the conclusion that there is at least one ‘intermediate’ group of young people with less severe depressive symptoms over time. These intermediate trajectories tended to be less stable than the high and low trajectory groups and often showed considerable positive or negative slope (variation) throughout the study period. Given the considerable heterogeneity between studies in describing the trajectory of this group (e.g. stable intermediate vs increasing vs decreasing), it is possible that external environmental factors play a more significant role in patients following these intermediate trajectories.
Studies examining the contribution of specific and predefined risk factors to depressive symptom trajectories
A considerable body of research has investigated the effects of specific, predefined risk factors on the longitudinal course of depressive symptoms in adolescents and young adults using statistical methods, including growth curve modeling, growth mixture modeling and structural equation modeling (Nagin, 2005). These studies do not directly identify ‘high’ or ‘low’ symptom trajectories and their risk factors. Rather, this type of analysis generates knowledge of the effects of known risk factors of risk status (i.e. cross-sectional diagnosis) on longitudinal disease activity. Table 2 lists the 22 studies identified for this review and summarizes their main findings.
Studies describing concurrent trajectories of depressive symptoms and other longitudinally measured factors
Thirteen of the articles identified for this review tracked the interdependence over time of depressive symptoms with other clinical or behavioral outcome measures, such as delinquency, anxiety and substance use (Table 3). This type of study addresses the problem that conventional reports of associations between two problem behaviors are typically represented by summary statistics (e.g. a correlation coefficient or an odds ratio is computed at each wave of assessment), which makes little use of information about group and individual developmental courses of the two constructs over time (Nagin and Tremblay, 2001). Moreover, summary statistics are unable to distinguish subgroups within the examined cohort and cannot reveal possible subgroup differences in the degree or developmental patterns of co-occurring problems. For example, associations may be very weak in some subgroups but much stronger for others. As a consequence, studies on co-occurring trajectory studies provide information on the associations between levels, concurrent change and episodic expressions of both phenomena, as well as the predictive relationships between level and growth (Fleming et al., 2008). Studies may yield important information for prevention programs tackling problem behaviors (e.g. crime prevention), enabling them to develop tailored strategies for identified subgroups that take co-occurring problems into account.
Risk factors for high depressive symptom trajectories and for elevated symptom intercept and slope
In the following section, we describe commonly identified biological, psychological and social factors that increase young people’s risk of belonging to a ‘high’ depressive symptom trajectory group (retrieved from studies represented in Table 1) and that influence the overall baseline level of depressive symptoms (intercept) and symptom development over time (slope) (Table 2).
Gender
Several studies have explored the impact of gender on depressive symptom trajectories and on trajectory membership in adolescence (Table 2). Overall, these investigations strongly suggest that young women and men differ considerably with regard to experiencing depressive symptoms during this life stage. Studies report that adolescent girls have overall higher symptom levels (Adkins et al., 2009; Ge et al., 2006) and a more pronounced increase in symptoms than boys from about age 12, peaking around age 17 (Burstein et al., 2010; Edwards et al., 2014; Garber et al., 2002; Hankin, 2009). In early adulthood, the gap between genders appears to narrow again, and some reports suggest that at age 25 the overall difference may no longer be statistically significant (Galambos et al., 2006). Interestingly, females show a sharper reduction in depressive symptoms between the age of 17 and 25 (Chen et al., 2011; Galambos et al., 2006; Stapinski et al., 2013). What also emerges is that well-established risk factors for depressive disorders, such as socioeconomic disadvantage and negative life events, have more profound effects on young females than males (Adkins et al., 2009; St Clair et al., 2012), particularly when they are amplified by personal psychological traits such as negative cognitive style and a tendency to ruminate (Hankin, 2009). On the individual symptom level, females may be more vulnerable to increases in ‘sad mood’, ‘sleep disturbance’ and ‘low self-esteem/guilt’, whereas males were found more susceptible to reductions over time in ‘concentration/decision-making’ (Kouros and Garber, 2014).
In support of these differences, many studies identified female gender as a risk factor for following ‘high’ depressive symptom trajectories (Costello et al., 2008; Ferro et al., 2015b; Yaroslavsky et al., 2013) (Table 1). However, some studies also indicate that more complex mechanisms may underpin these findings. For example, Mezulis et al. reported that female gender was a risk factor for a trajectory of increasing depressive symptoms between the age of 12 and 18, but not for a trajectory of early high and then decreasing symptoms. Olino et al. (2010) found that females were more likely to belong to classes characterized by fluctuations in the course of depressive and anxiety symptoms; however, sex differences were not observed in classes characterized by persistent depressive and anxiety disorders. Briere et al. (2015b) reported that male gender was the most informative prognostic factor of membership in a high-persistent depression trajectory, relative to other trajectories.
Interestingly, the adult clinical consequences of specific mood trajectory membership during adolescence appear to differ in males and females. One study found that adult emotional and behavioral wellbeing of adolescents on high-level trajectories was poorer for boys than for girls, despite the fact that more girls than boys were likely to follow high-level trajectories of depression (Diamantopoulou et al., 2011). Chaiton et al. (2013) reported that following a high-depression trajectory was a statistically significant independent predictor of depression, stress and self-rated poor mental health in young adulthood for both genders; however, only boys, but not girls, in the high trajectory group had a statistically significant increase in the likelihood of seeking psychiatric care. Therefore, while most studies concur that females are at higher risk of following high depressive symptom trajectories in adolescence and early adulthood, the long-term consequences of such a trajectory course could be more clinically and functionally damaging and disruptive in males.
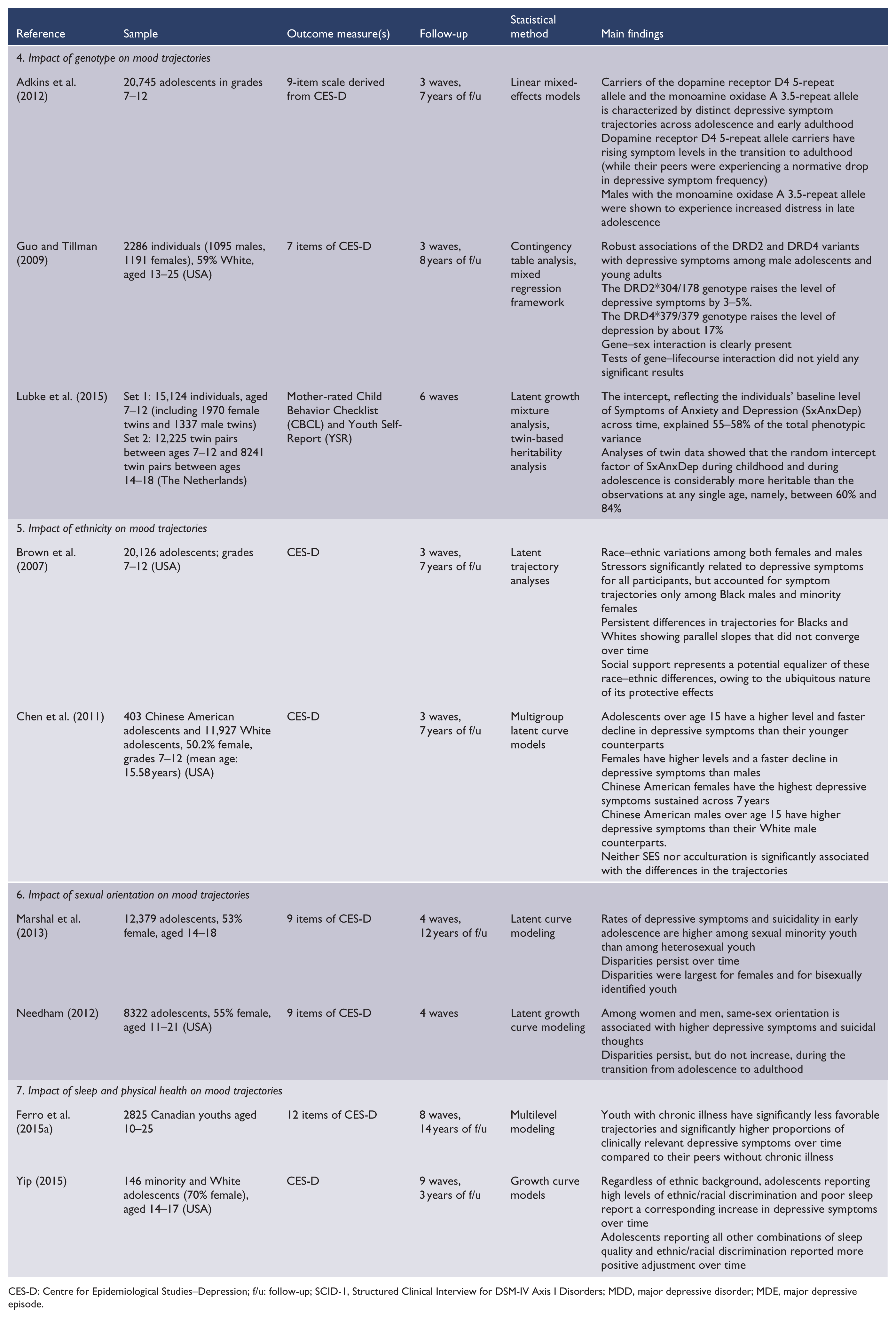
Genetic factors
Heritable factors are likely to contribute to depressive symptom trajectories in adolescents and young adults, and a number of studies have investigated these relationships in detail.
One study pointed to a heritability differentiation between mood and anxiety symptoms, as far as trajectory risk for the offspring was concerned: children of parents with depression were more likely to follow a high-depression trajectory, whereas offspring of parents with anxiety disorders tended to have a course characterized by anxiety disorders (Olino et al., 2010).
A specific heritability analysis of adolescents between the age of 14 and 18 found that the trajectory intercept factor (i.e. baseline stability) of depressive and anxiety symptoms is substantially more heritable than cross-sectional scores observed at any age, ranging between 72% (childhood) and 83% (adolescence) for males and 64% (childhood) and 84% (adolescence) for females (Lubke et al., 2015). In comparison, cross-sectionally assessed age-specific heritabilities ranged from 43% to 54% between the age of 7 and 18. The authors concluded that their findings support the existence of a latent genetic ‘intercept factor’ of depressive and anxiety symptoms that is less liable to measurement error and may therefore represent a reliable phenotype for further genetic studies. Furthermore, they concluded that three time points of measuring symptoms are sufficient to extract this highly heritable phenotype.
Three studies have specifically explored the impact of genetic variation on depressive symptom trajectories in young people. Taken together, these studies indicate that genetic variance could play a substantial role in determining the course of depressive symptoms in adolescence and young adulthood.
In young people aged 13–25, robust associations of genetic dopamine receptor D2 (DRD2) and dopamine receptor D4 (DRD4) variants with high depressive symptom trajectories among male adolescents from the age of 13 and among young adults of both genders aged between 24 and 26 were identified (Guo and Tillman, 2009). These genetic associations remained significant after controlling for a wide range of psychosocial parameters. The authors reported that the DRD2*304/178 and the DRD4*379/379 genotypes raised mean depressive symptoms by 3–5% and 17%, respectively.
In another sample of US high school students, an association between the relatively uncommon R5 allele of DRD4 and depressive symptom trajectories was described, for both males and females (Adkins et al., 2012). Individuals with any 5R alleles, representing 2.87% of the full sample, appeared to follow a unique trajectory with relatively low symptom levels through late adolescence, before experiencing rapid increases in early adulthood. Thus, carriers of the DRD4 5R appear to navigate their high school years with relative psychological ease compared to others, but begin to experience elevated distress as they transition into adult roles. In contrast, in males only, the 3.5R allele of the monoamine oxidase A (MAOA) variable number tandem repeat (VNTR) promoter was associated with higher symptom peaks in late adolescence and sharper declines of symptom intensity in early adulthood. Therefore, males with the 3.5 genotype appeared to have a particular stressful time during high school and the subsequent transition to adulthood, but converged with their peers in early adulthood.
Minority group membership
Minority group membership is regarded as a risk factor for many adverse mental health outcomes, including psychosis and MDD (Berger and Sarnyai, 2015; Ploderl and Tremblay, 2015). Several studies reviewed for this article set out to explore the impact of these social factors on depressive symptoms over time.
In the United States, several studies found that adolescents of Black, Hispanic and Asian minorities experience higher levels of depressive symptoms across early life compared to Whites (Adkins et al., 2009; Brown et al., 2007; Chen et al., 2011). Similarly, minority ethnicities increased the likelihood of following high-depression trajectories, compared to White Americans (Costello et al., 2008).
Potential mediators of these ethnic disparities have been identified. Two of the investigations reported that socioeconomic status (SES) and stressful life events (SLEs) explained much of the racial depressive symptom disparity, suggesting that minorities show greater sensitivity to the effects of low childhood SES (Adkins et al., 2009; Brown et al., 2007). In other studies, low socioeconomic status was independently associated with depressed mood trajectory groups in three studies (Costello et al., 2008; Ferro et al., 2015b; Wickrama et al., 2009). Additionally, Brown et al. (2007 reported that higher levels of maternal support were related to lower levels of depressive symptoms among all race–ethnic groups.
In one study, high levels of ethnic/racial discrimination combined with poor sleep were associated with a corresponding increase in depressive symptoms and lower levels of self-esteem over time, whereas other ‘combinations’ of sleep quality and ethnic/racial discrimination reported more positive adjustment over time (Yip, 2015). It is therefore possible that sleep disturbance and perhaps other indicators of general physical and mental wellbeing are an important mediator of the ethnicity–depression relationship.
Two studies investigated the impact of minority sexual orientation on depressive symptom trajectories and reported that the rates of depressive symptoms and suicidality in early adolescence were higher among sexual minority youth than among heterosexual youth. These disparities persisted over time as participants transitioned into young adulthood, but did not increase at older ages (Needham, 2012). The observed longitudinal disparities were largest for females and for bisexually identified youth (Marshal et al., 2013).
Psychological factors
One study identified high infant negative affectivity as a risk factor for both genders for increasing depressive symptom class throughout adolescence, whereas it was a risk factor for an early high symptom class only for boys. For girls, a high level of rumination was an additional risk factor for the early high symptom class (Mezulis et al., 2014). Lower self-concept was a risk factor for the high symptom classes in another study (Ferro et al., 2015b). Furthermore, negative cognitive style and a higher motivation to reduce symptoms were associated with elevated symptom trajectories (Briere et al., 2015b).
One study reported that initial levels of depressive symptoms were mediated by an interaction of rumination and stressors, as well as by an interaction of negative cognitive style and stressors (Hankin, 2009). The authors speculated that some of the well-documented sex differences in depressive symptom trajectories can be accounted for by particular cognitive vulnerabilities (particularly negative cognitive style and rumination) and stressors as risk mechanisms.
Another study investigated whether within-individual relations between depression vulnerability factors (childhood trauma, dysfunctional attitudes, maladaptive coping) and depressive symptom trajectories varied as a function of the number of prior major depressive episodes (MDEs) experienced in the lifetime of young people aged 18–31. Authors reported a significant interaction of ‘coping’ and the number of previous MDEs and time (Morris et al., 2014). Results indicated that among individuals with less adaptive coping (i.e. lower primary or lower secondary control coping scores), depressive symptoms increased significantly in relation to the number of prior depressive episodes.
Parental mental health and parent–child relationships
One study reported that the magnitude of parents’ depressive symptoms significantly discriminated a ‘high chronic’ symptom class from three lower symptom classes (Stoolmiller et al., 2005). Another study identified multiple parental transitions, negative life events and poor childhood academic achievements as risk factors for a high chronic symptom trajectory by one study (Stoolmiller et al., 2005).
In contrast, a two-parent family structure and feelings of connectedness toward parents were identified as protective factors against depressive symptoms, increasing the likelihood of following a low-depression trajectory (Costello et al., 2008).
Physical development and physical health factors
In a large 1946 birth cohort with mental health data spanning early adolescence to middle adulthood, Colman et al. found that heavier babies had a lower likelihood of elevated depressive and anxious symptom trajectories. Delays in first standing and walking were associated with subsequent higher likelihood of adverse depressive and anxious symptoms (Colman et al., 2007).
Two studies reported that chronic health conditions (Ferro et al., 2015b) and high volatility of physical problems over time (Wickrama et al., 2009) increased the likelihood of following high depressive symptom trajectories, highlighting the potential interactions between depression trajectories and physical health outcomes in adolescents and young adults. One study found that youth with chronic illness had significantly less favorable trajectories and significantly higher proportions of clinically relevant depressive symptoms over time, compared to their peers without chronic illness (Ferro et al., 2015a).
Lifestyle factors
‘Risky’ lifestyle factors between the age of 12 and 19, such as having multiple sex partners, having been arrested/having committed crime, being an excessive drinker, being a smoker and being unmarried, were identified as risk factors for chronically high, increasing and decreasing depressive symptom groups, compared with a consistently low trajectory group. In the same cohort, using alcohol, tobacco or other drugs on a weekly basis was a risk factor for high depressive trajectory groups (Costello et al., 2008).
Phenotype trajectories concurrent with elevated depressive symptom trajectories in young people
The most commonly investigated trajectories of developmental, clinical and behavioral phenotypes that concur with longitudinally assessed depressive symptoms in young people are described in the following section. Results are retrieved from studies listed in Table 3.
Phenotypes or phenomena that develop in parallel with depressive symptoms can be understood from two perspectives: first, as potentially causative factors (i.e. they promote the development of depressed mood) or, in reverse, as potential sequelae of longitudinally elevated depression scores. While studies investigating these parallel courses cannot give conclusive information about causation, they nevertheless provide important information on the potential usefulness of population-based or targeted interventions designed to address the (problem-) behavior in question.
Concurrent trajectories of mood symptoms and trauma/life events/stress
One study investigated the question whether exposure to major life events (e.g. illness, loss, trauma) and minor hassles (e.g. money problems, social difficulties, work or study pressure) coincides with an increase in depressive symptoms as people advance from adolescence (aged 14–18) into adulthood (age 30) (Pettit et al., 2010). The authors reported strong evidence for a bi-directional relationship between trait-like trajectories of stress (hassles) and the development or maintenance of depressive symptoms over time. Conversely, there were only weak to modest bi-directional relations between major life events and depressive symptoms when latent trajectories were taken into account. The authors therefore suggested that strategies for the prevention of depression in young adults might be most effective if they focus on coping and stress inoculation strategies for hassles in adolescents and young adults.
Concurrent trajectories of mood and delinquency/oppositional defiance
Three studies investigated the relationship between depressive symptoms and delinquent or oppositional defiant (OD) behaviors.
Two studies found that adolescents following a low-level trajectory of depression were most likely to also follow a low-level trajectory on delinquency. Vice versa, adolescents following a low-level trajectory on delinquency were most likely to also follow a low-level trajectory on depression (Diamantopoulou et al., 2011; Wiesner and Kim, 2006). Findings support the notion that depressive symptoms and delinquency do not develop in parallel across the entire population, but only in a subgroup of individuals, namely in those who display very high levels of these problem behaviors.
Studies differed in their conclusions of impact of gender on trajectory interplay. One study indicated that delinquent behavior was more predictive of depressive symptoms than vice versa for boys, whereas both problem behaviors were mutually predictive of each other for girls (Wiesner and Kim, 2006). In contrast, another study concluded that while high-depression levels appeared to always be related to high delinquency levels in both genders, high delinquency levels were more likely to be related to depression in girls than in boys (Diamantopoulou et al., 2011).
Another study tracked co-occurring trajectories of depressive symptoms, anxiety and OD behavior in a Canadian cohort aged 12–18 (Leadbeater et al., 2012). Authors reported that expressions of anxiety, depression and oppositional symptoms are distinctive within domains and invariant across time. Moderate correlations among adolescent levels for all symptom combinations were found, such that adolescents who started high in one domain were also consistently high in the others at each assessment point, suggesting that there is considerable consolidation of psychopathology and that this persists across the transition to young adulthood.
Concurrent trajectories of depressive symptoms and body mass index
Two studies investigated the concurrent trajectories of mood and body mass index (BMI). In the 1946 British Birth Cohort, Gaysina et al. reported that women with adolescent-onset elevated depressive symptoms had lower mean BMI at age 15 years, faster rates of increase across adulthood and higher BMI at age 53 years than those with no symptoms. Men with adolescent-onset mood symptoms had lower BMI than their low symptom peers at all ages from 15 to 53 years. The BMI trajectories of men and women with adult-onset depressive symptoms did not differ from those with absence of symptoms at all ages (Gaysina et al., 2011).
Another study of young people aged 15–27 in the United States found five profiles that characterize concurring depression and weight trajectories (Mumford et al., 2013). Black or Hispanic respondents had consistently greater odds of being in any class other than the normative reference class (‘stable normal weight, stable good mental health’—82% of the cohort). Males had higher odds of being in the ‘consistently obese, stable good mental health’ class (6.8% of the cohort) and lower odds of being in the ‘overweight becoming obese, declining mental health’ class (5.6%). Respondents reporting baseline income less than 100% of the poverty level had higher odds of being in classes of increasing obesity risks, with variations in mental health. Overall, the findings suggest that there is a detectable subgroup of young people who are particularly vulnerable to comorbid depression and obesity, supporting the idea that a ‘metabolic’ phenotype could exist among mood disorder patients (Mansur et al., 2015).
Concurrent trajectories of depressive symptoms and substance use
Five recent studies described co-joint trajectories of depressive symptoms and substance use, and aspects of their relationship in adolescents and young adults. Overall, this literature paints a picture of a complex rather than simplistic relationship between both phenomena. All studies reviewed here identified subgroups of 10–15% of youths in which consistently high levels of co-morbidity are seen (Brook et al., 2014; Fleming et al., 2008; Needham, 2007; Rodriguez et al., 2005; Willoughby and Fortner, 2015). For these ‘high-risk’ youths, the co-morbidity is either causally linked or co-mediated through common confounders. However, the available evidence indicates that for the majority of affected young people, depressive symptoms and substance use develop independently of each other.
Several studies identified a surprising impact of depression scores on substance use over time, indicating that while high initial depression scores in teenagers were associated with higher initial levels of substance use, they were also associated with decreased acceleration of substance use over time (Needham, 2007; Rodriguez et al., 2005).
Complementing these findings, another study reported that levels of substance use at age 14 did not predict change in depressive symptoms until age 18, nor did higher levels of depressive symptoms at age 14 predict greater increases in substance use. However, evidence was found for a positive association between episodic expressions of depressive symptoms and alcohol use that fell outside developmental trajectories (Fleming et al., 2008).
It is likely that the co-occurrence of depressive symptoms and substance use is influenced by other factors, such as psychological traits. In a recent study of 14- to 18-year-olds, high ratings on the ‘delay of gratification’ trait increased participants’ odds of belonging to a depressive symptoms and alcohol ‘low co-occurrence’ group, compared to high-risk groups, suggesting that difficulties in delaying gratification are a risk factor for both depression and substance abuse at this age (Willoughby and Fortner, 2015). In contrast, high ‘novelty seeking’ emerged as a risk factor for ‘high alcohol use only’ in boys, whereas low ‘novelty seeking’ in girls was associated with increased odds of being in the ‘depressive symptoms only’ group. The authors concluded that programs for adolescents that focus on improving delay of gratification and self-regulation in general may be particularly helpful not only for reducing co-occurring depressive symptoms and alcohol use but also for reducing at-risk depressive symptoms and alcohol use that occur independently of each other.
Discussion
Summary of findings
Overall, findings support a stress-vulnerability model for depressive symptom trajectories in young people.
We set out to review the current literature on mood symptom trajectories in young people aged between 15 and 25.
Our findings are summarized in Figure 4. We found strong evidence that depressive symptoms are not uniformly distributed across adolescent and young adult populations. Rather, young people follow distinct subgroups that are characterized by differential courses of depressive symptoms over time (Figure 3(a)). The majority of young people (60–80%) report consistently low levels of depressive symptoms with slight normative increases from early to late adolescence, peaking around age 17. In contrast, studies consistently point to a group, representing 5–12% of the population, who report ongoing high levels of symptoms. Between these extremes, intermediate trajectory groups are described, which are more variable across studies in terms of their shape and number, possibly depending on the specific characteristics of the population studied. For example, smaller studies involving minority groups have tended to identify higher numbers of distinct trajectories than larger studies more representative of the entire population (Figure 4(a)).
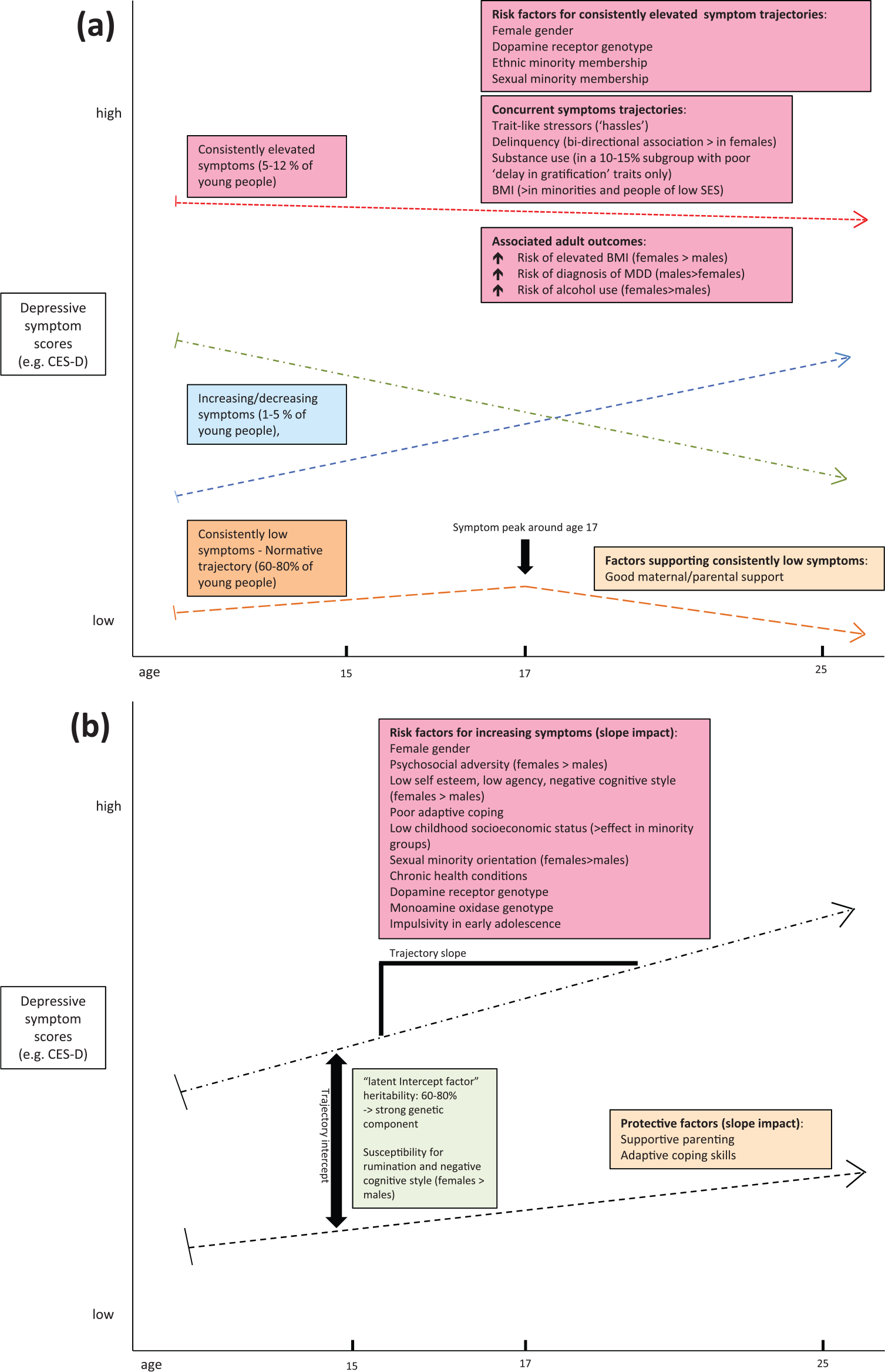
Summary of findings: (a) Studies report distinct latent trajectories of depressive symptoms in young people. Frequently identified latent groups include ‘consistently elevated symptoms’, ‘consistently low symptoms’ and ‘increasing/decreasing symptoms’. The total number of latent classes varies between studies. Frequently identified risk factors for the high and low symptom classes are summarized. (b) Frequently identified factors that impact baseline symptom levels (intercept) and direction of the trajectory curve (slope) are summarized.
Etiologically, the literature reviewed here supports a ‘stress-vulnerability’ model for depressive symptom trajectories in young people. Analyses of genetic heritability and specific genetic variants suggest a genetically mediated biological basis to experiencing higher-than-normal levels of depressive emotions over time, expressed as a ‘latent intercept factor’ (Adkins et al., 2012; Guo and Tillman, 2009; Lubke et al., 2015) (Figure 4(b)). When individuals with genetically determined vulnerability are exposed to certain internal or external environmental risk factors, their odds of experiencing chronically elevated levels of depressive affect are further enhanced. Internal risk factors appear to include sex hormones (testosterone may have a protective effect) and certain cognitive-psychological traits (e.g. ruminations or negative cognitive style). External factors seem invariably associated with some form of chronic psychosocial stress, as encountered by people of low SES, racial or sexual minority groups or by those reporting trait-like chronic ‘hassles’.
A subgroup of adolescents following high depressive symptom trajectories is additionally at increased risk of problem behaviors such as substance use or delinquency (Figure 4(a)). The interactions between depressive affect and these behaviors are complex and almost certainly involve mediating psychological traits such as novelty seeking and capacity for delayed gratification. Interestingly, the bi-directional links between high depressive symptoms and problem behaviors are overall more pronounced in females than in males, again suggesting mediating roles of sex hormones and possibly societal norms and expectations.
Some limited conclusions can be drawn from the reviewed literature about factors that are protective and that characterize people who follow the normative low symptom trajectory. Adequate parental support, intact family structures, advantageous SES and psychological traits such as adaptive coping have all been associated with the low symptom group. However, the literature reveals a bias toward exploration and description of high-risk outcomes and associated risks. Therefore, thorough examination of resilience factors is urgently required, particularly in those young people with a biological/genetic predisposition to high symptom trajectories.
Implications for clinical practice and research
Considering the strong evidence, reviewed here, for distinct latent classes of depressive symptom trajectories in adolescence and young adulthood and the equally strong evidence for a range of adverse health and behavioral outcomes for young people following consistently elevated depression trajectories, one might ask whether a shift in psychiatric nosology toward a ‘trajectory-centric’ understanding of mood disorders might be useful in this group. Current Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for MDD are based on cross-sectional assessments by clinicians combined with patients’ subjective recall of mood symptoms over the recent weeks. It is clear that such an approach has limited capacity to delineate the considerable heterogeneity in severity and outcome of depressive disorders, particularly in young people where symptoms are highly dynamic. Additionally, attempts to dissect MDD heterogeneity by symptom characteristics alone have been only moderately successful (Flint and Kendler, 2014). In this situation, a more systematic consideration of depressive symptom trajectories may offer a rewarding new avenue for clinical practice and research. A truly ‘longitudinal’ approach to assessment and diagnosis of mood symptoms may ultimately support a novel classification of MDD that may be better aligned with the underlying architecture of population heterogeneity, thereby representing a more valid target for causal enquiry into the roles of genes, environmental factors and their interaction (Colman et al., 2007). Assessment of symptom severity over time on a population level seems increasingly feasible with the advent and proliferation of personal health tracking devices. The suggestion that three measurements over time could be sufficient to detect a latent heritable ‘intercept factor’ is particularly encouraging in this context (Lubke et al., 2015). Future large-scale longitudinal studies should aim to sample a range of biological specimen and seek ‘deeper’ phenotypical assessment of participants to allow for a more comprehensive biopsychosocial characterization of ‘high’ and ‘low’ depressive symptom trajectory groups.
Furthermore, as described by our group before, Bayesian statistics offer relatively simple paradigms that can account for biological, social and psychological risk factors of individuals and that can produce improved predictions of an illness trajectory a patient is likely to follow (Clark et al., 2015, 2016; Schubert et al., 2015). If these tools can be successfully developed in the area of youth mental health, they would aid services in the provision of indicated prevention programs to high-risk individuals. At the same time, better reassurance could be provided to low-risk patients and their families to avoid the medicalization of normal developmental processes.
Limitations
The majority of studies reviewed here have relied on self-report of depressive symptoms. This approach may be problematic in young people who may be easily influenced in their answers or prone to under- or over-reporting. The use of clinician-rated questionnaires may have provided different results. However, given the high numbers of subjects enrolled in these studies, clinician interviews for each individual are hardly feasible.
Because these studies have investigated continuous symptom scores on mood questionnaires, it is difficult for clinicians to discern whether ‘high symptom trajectories’ were actually associated with the presence of a categorical diagnosis for MDD according to DSM criteria. Only one study in our dataset makes reference to this problem. Here, 29.2% of young men following a high-persistent symptom trajectory and 20% following a high decreasing trajectory had been diagnosed with MDD at age 26, compared to only 5.7% and 0% in moderate-decreasing and very low symptom classes (Stoolmiller et al., 2005). These numbers indicate that ‘high symptom trajectories’ may increase the risk of a DSM diagnosis of MDD, but also show that the relationship between ‘trajectory’ and ‘categorical’ concepts of depression is complex.
Another potential caveat of the studies reviewed here is that they investigated depressive symptoms without prior regard to specific symptom clusters that could underlie subtypes of depressive disorders. The stratification of study populations into these proposed subtypes, identified in adult populations using latent class analysis (Lamers et al., 2010; Li et al., 2014) or genetic linkage, could therefore substantially alter the findings reported in these articles.
Conclusion
A considerable body of large-scale investigations exists that describes the development of depressive symptoms over time in adolescent and young adult populations. The findings of these studies have the potential to serve as valuable guidance and starting points for clinicians, researchers and public health administrators in improving future strategies toward early intervention and indicated prevention in mood disorders in young people. Longitudinal assessment of mood symptoms in large samples also may help untangle the substantial clinical and biological heterogeneity that characterizes mood disorders.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.