
Abstract
Objective:
The current study examined whether trauma characteristics such as the type and number of traumatic events were associated with three suicidal behaviours (i.e. ideation, plan and attempt) after adjusting for sociodemographic factors, post-traumatic symptoms and history of psychiatric disorders.
Method:
Data came from the 2007 Australian National Survey of Mental Health and Wellbeing (N = 8841). Respondents were asked about exposure to 28 traumatic events that occurred during their lifetime. Suicidal behaviours were measured using three statements about whether the person ever seriously thought about or planned or attempted suicide.
Results:
Sexual violence and exposure to multiple traumatic events were particularly associated with suicidal behaviours. The presence of the emotional numbing symptom cluster and co-occurrence of three psychiatric disorders (major depressive disorder, alcohol use disorder and substance use disorder) also increased the odds of suicidal behaviours. Analysis of age of onset revealed that the mean age of traumatic exposure was earlier than the age at which suicidal behaviours emerged.
Conclusions:
The current study is the first to demonstrate that sexual violence and exposure to multiple traumatic events are associated with suicidal behaviours in a representative sample of Australian adults. The results underline the potential benefits of thorough assessment of trauma history, post-traumatic symptoms and history of psychiatric disorders and their additive contribution in suicide risk among trauma victims. These findings can be used by clinicians and researchers for early intervention programmes.
Suicide is a major public health concern. The World Health Organization (WHO) reported that approximately 804,000 people die by suicide each year worldwide; this number represents a yearly suicide rate of 160 per million, while the rate of attempted suicide is 10–20 times higher (WHO, 2014). The alarming prevalence of suicide underlines the need for carefully designed prevention efforts, focusing on suicidal ideation, suicide plan and suicide attempt, as these non-fatal suicidal behaviours are major predictors of subsequent suicide deaths (Overholser et al., 2012). There are a number of other well-established risk factors for suicidal behaviours. These include sociodemographic factors such as younger age, being divorced or separated, low educational level, low income level (Borges et al., 2006; Li et al., 2011), presence of mood disorders (Li et al., 2011; Miret et al., 2013), drug and alcohol use disorders (Bohnert et al., 2010) and comorbidity of mental disorders (Nock et al., 2010). Likewise, several studies reported a strong association between the history of traumatic life events/post-traumatic symptoms and suicidal behaviours (Panagioti et al., 2009, 2012). Thus, there is solid evidence that the relationship between trauma and suicidal behaviours can be affected by various factors such as type of trauma, number of trauma, type of traumatic symptoms and related psychiatric disorders. However, few studies have investigated the aforementioned factors collectively in a coherent and cohesive framework.
Trauma-related characteristics and suicidal behaviours
Several studies in the last two decades have examined whether different types of traumatic events are related to suicidal behaviours or whether this association is limited to certain types of trauma. A review of the association between post-traumatic stress disorder (PTSD) and suicidal behaviour suggested that a personal feeling of responsibility and the preventable nature of trauma – the main characteristic of interpersonal trauma – may be the essential factors related to suicidality (Panagioti et al., 2009). A cross-national epidemiological study conducted in 21 countries highlighted that the majority of traumatic experiences were correlated with lifetime suicide ideation and suicide attempt, with sexual and interpersonal violence displaying the highest odds ratios. In multivariate analysis, after taking into account the co-occurrence of different traumatic events, fewer associations between traumatic events and suicidality were observed. However, sexual and interpersonal violence remained robust predictors of suicidality (Stein et al., 2010). Consistent findings are reported in active military members (Belik et al., 2009) and high-risk clinical samples such as patients diagnosed with mood disorder and substance use disorders (SUDs) (Evren and Evren, 2005; Oyefeso et al., 2008). Another important trauma-related variable is history of multiple traumatic events. The dose-response hypothesis suggests that exposure to multiple traumatic events may lead to an increase in suicidal behaviours. The association between the number of traumatic incidents and suicidal behaviours has been reported in a number of studies based on large community samples and nationally representative samples (Belik et al., 2007, 2009; Stein et al., 2010). Moreover, this association remains robust even several years after the trauma (Jankovic et al., 2013).
PTSD, trauma-related symptoms and suicidal behaviours
Individuals who are exposed to traumatic events are at risk of experiencing distress and heightened psychopathology, most notably PTSD, which is defined by a range of symptoms including re-experiencing, avoidance, cognitive and mood alternations, and hyperarousal. These symptoms must be present for at least one month duration and with impaired functioning (American Psychiatric Association, 2013). The presence of trauma-related symptoms, rather than the experience of traumatic events, is underlined as the principal factor associated with suicidal behaviours. Studies have highlighted the association between partial PTSD (defined by the number of present PTSD symptoms compared to the full diagnostic algorithm) and suicidal behaviours (Marshall et al., 2001; Sacks et al., 2008), as well as fully diagnosed PTSD and suicidal behaviours (Wilcox et al., 2009). However, more recent studies have reported that the PTSD symptom clusters may differ in their association with suicidal behaviour. For instance, a study of American war veterans with a PTSD diagnosis reported that the cognitive-affective alterations symptom cluster of major depression disorder (MDD) and the numbing symptom cluster of PTSD were associated with increased suicidal ideation (Guerra and Calhoun, 2011). Another study examined suicidal ideation among veterans diagnosed with PTSD as a result of sexual trauma experienced during military service. Taking into account the presence of MDD in a multivariate regression model, only the hyperarousal symptom cluster was associated with suicidal ideation (Surís et al., 2011). In the same vein, in a community sample of trauma-exposed Israeli men, hyperarousal symptom cluster was associated with higher scores in a suicide risk scale and avoidance symptom cluster was negatively associated with suicidality (Ben-Ya’acov and Amir, 2004). Although in the earlier edition of Diagnostic and Statistical Manual of Mental Disorders (DSM) (American Psychiatric Association, 1994) avoidance and numbing symptoms were grouped in a single criterion (criterion C), prior studies indicate differential roles of these symptoms in suicidal behaviours (Panagioti et al., 2009). This is in line with the four-factor model proposed by King et al. (1998) where the criterion C symptoms were divided into two factors indicating avoidance and numbing. This division has been used in the latest version of DSM (American Psychiatric Association, 2013).
History of psychiatric disorders, trauma and suicidal behaviours
Comorbidity is frequently reported among PTSD patients. Epidemiological research from the United States indicates that approximately 75% of respondents with PTSD reported a history of other psychiatric disorders, with anxiety and mood disorders as the principal co-occurring psychiatric conditions (Kessler et al., 2005). A recent French study highlighted that the presence of comorbid mental disorders moderates suicidal behaviours among trauma victims (Afzali et al., 2015). MDD, alcohol use disorder (AUD) and SUDs are frequently reported as major correlates of suicidal behaviour among trauma victims. The significant role of MDD in suicidal behaviours among trauma victims and PTSD patients has been highlighted in clinical samples with primary PTSD (Sacks et al., 2008; Tarrier and Gregg, 2004), clinical samples with primary depression (Oquendo et al., 2005) and large samples with a history of trauma such as veterans and refugees (Jankovic et al., 2013; Surís et al., 2011). In the same vein, the role of SUDs and AUD in suicidal behaviours among trauma victims and PTSD patients has been highlighted in clinical samples with primary PTSD (Guerra and Calhoun, 2011; Harned et al., 2006), clinical samples with primary substance use (Dore et al., 2012) and large samples with a history of trauma such as veterans (Price et al., 2004).
Objectives
There are a number of significant gaps in our knowledge about the relationship between traumatic events and suicidal behaviours. Although the association between some trauma-related characteristics and suicidal behaviours is well-established, to the best of our knowledge, the collective role of trauma-related characteristics, PTSD symptom clusters and major mental disorders is unclear. Information on this relationship would yield important insights into the magnitude of association between each of aforementioned factors and suicidal behaviours, along with the extent of their additivity. The current study is the first to use data from a large nationally representative Australian survey to address these factors in a comprehensive and coherent framework. Specifically, this study’s foci were
To examine whether trauma type is associated with suicidal behaviours (defined by suicide ideation, plan, attempt) after adjusting for sociodemographics, exposure to other traumatic events and the number of traumatic events;
To evaluate the possible role of particular PTSD symptom clusters beyond the type and the number of trauma;
To evaluate the possible role of psychiatric disorders beyond trauma and trauma-related symptoms.
Method
Study sample
Data for the current study were derived from the 2007 Australian National Survey of Mental Health and Wellbeing, a nationally representative survey of adults aged between 16 and 85 years. Data were collected via computer-assisted personal interviews conducted by trained staff from the Australian Bureau of Statistics. The sample excludes those residing in hospitals, nursing homes and jails and those living in remote and sparsely populated areas of Australia. A total of 14,805 individuals were initially selected to participate in the survey. Of those, 8841 (60%) completed the full survey. Oversampling of older and younger age groups was conducted to ensure greater representation of these traditionally under-represented groups. A comprehensive description of the sampling procedures and the study design can be found elsewhere (Slade et al., 2009).
Assessment
Traumatic events
All respondents were asked about their lifetime exposure to trauma, using a comprehensive list of traumatic events. Respondents were able to endorse multiple traumatic events, allowing examination of the impact of each type of traumatic event and, independently, the number of traumatic events. If respondents nominated more than one traumatic event, they were asked to indicate which event they considered to be most traumatic and the remaining PTSD module was administered with reference to this event. For the purposes of this study, and in line with literature (Stein et al., 2010), we combined traumatic events into four conceptually related categories: sexual violence (rape, sexually assaulted), physical violence (physically assaulted by partner, physically assaulted by stranger, physically abused as a child by parents, threatened with a weapon and kidnapped), non-interpersonal (life-threatening car accident, other life-threatening accident, natural disaster, exposure to toxic chemical substance) and unexpected death of loved one.
Suicidal behaviours
Respondents were asked to read statements related to suicidal ideation, plan and attempt. First, lifetime suicidal ideation was assessed by the statement ‘you seriously thought about committing suicide or taking your own life’ (Statement A). Respondents were subsequently asked ‘Did Experience A ever happen to you?’ Lifetime suicide plan was assessed by the statement ‘you made a plan for committing suicide’ (Statement B). Lifetime suicide attempts were queried by the statement ‘you attempted suicide’ (Statement C). Only those who reported suicidal ideation were asked about suicide plan or attempt. Consequently, the analyses of suicide plans and attempts focus only on the sub-sample of ideators, which avoids the problem of accounting for shared variance with suicidal ideation when examining risk factors for suicidal behaviours (May et al., 2012).
Mental disorders
Detailed information concerning mental disorders was gathered using a modified version of the World Mental Health Composite International Diagnostic Interview (Kessler and Ustün, 2004). Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) PTSD symptoms were organized into four clusters: re-experiencing, avoidance, numbing and arousal. DSM-IV criteria were used to generate lifetime diagnoses of MDD, AUD (combination of alcohol abuse and alcohol dependence) and SUD (combination of substance abuse and substance dependence).
Age of onset
In line with other studies (Belik et al., 2007) and to test the directionality of observed effects, separate paired samples t-tests were used to ensure that the worst traumatic event occurred significantly earlier than the mean age of onset of suicidal behaviours among the sub-samples of respondents who endorsed the experience of a trauma and each of the suicidal behaviours (ideation, plan and attempt). Bonferroni adjustments were applied to account for multiple comparisons (control for Type I error rate). Also as a sensitivity analysis to ensure the robustness of our results, all analyses were rerun excluding respondents who reported onset of suicidality before onset of trauma.
Analytic strategy
Appropriate estimation procedures were applied to all data analyses using Jackknife Replicate Weights provided by the Australian Bureau of Statistics to ensure representativeness of the data to the Australian population. The regression analyses were based on the weighted sample, which takes into account nonresponse and provides estimates that are generalizable to the Australian population. The ‘survey design with replicate weights’ (svrepdesign function) in the ‘survey’ package in R was used to obtain design-based variance estimation to calculate standard errors required for data with a complex sampling design. Hierarchical logistic regression models were estimated using the svyglm function to explore the relationship between type and number of traumatic events, PTSD symptoms, history of psychiatric disorders and suicidal behaviour after adjusting for age and sex. We analysed three dependent binary variables in separate analyses: suicidal ideation, suicide plan among ideators and suicide attempt among ideators. For each dependent variable, the independent role of trauma-related predictors, PTSD symptoms and history of psychiatric disorders was investigated in three steps. The first step focused on dependent variables regarding the type of trauma (i.e. sexual violence, physical violence, non-interpersonal and unexpected death of loved one) and number of traumatic events. The second step focused on dependent variables regarding the four groups of PTSD symptoms (i.e. re-experience, avoidance, numbing and arousal). The third step comprised information on history of three major related psychiatric disorders (i.e. MDD, AUD and SUD).
Results
Sample description
Four types of trauma were investigated. The most commonly reported trauma was the death of a loved one, reported by 1561 respondents (17.7% of the total sample), followed by physical violence reported by 1014 respondents (11.5%). Noninterpersonal trauma was reported by 937 respondents (10.6%), and 754 (8.5%) reported the experience of sexual violence. Lifetime suicidal ideation, plans and attempts were reported by 1252 (14.2%), 386 (4.4%) and 328 (3.7%) respondents, respectively. A history of lifetime trauma was reported by 692 respondents with suicidal ideation (55.5%), 240 respondents with suicide plan (62.7%) and 221 respondents with suicide attempt (68.0%). Among those with history of suicidal ideation, 581 respondents (84%) reported the experience of the worst traumatic event prior to their suicidal ideation. In this sub-sample, results of Bonferroni-adjusted paired samples t-tests showed the significant precedence of the age of the worst traumatic event (M = 23.17, standard deviation [SD] = 14.4) compared to the age of initial suicidal ideation (M = 27.40, SD = 13.7). Among those with history of suicidal plan, 213 respondents (89%) reported the experience of the worst traumatic event prior to their initial suicidal plan. In this sub-sample, results of Bonferroni-adjusted paired samples t-tests showed the significant precedence of the age of the worst traumatic event (M = 20.21, SD = 12.6) compared to the onset of suicide plan among ideators (M = 27.40, SD = 14.0). Among those with history of suicide attempt, 192 respondents (87%) reported the experience of the worst traumatic event prior to their initial suicide attempt. In this sub-sample, results of Bonferroni-adjusted paired samples t-tests showed the significant precedence of the age of the worst traumatic event (M = 19.74, SD = 11.7) compared to first suicide attempt among ideators (M = 24.84, SD = 11.0). These results provide some confidence about the directionality between the experience of traumatic events and subsequent suicidal behaviours.
Multivariate associations of trauma, PTSD symptoms and history of psychiatric disorders with lifetime suicidal behaviours
Table 1 presents adjusted odds ratios (AOR) and their confidence intervals (CI) from the hierarchical logistic regression models for the three outcomes after taking into consideration the effects of sex and age. Results concerning the effects of sex and age indicated that respondents who were younger and female had significantly higher odds of reporting a suicidal attempt, ideation and plan. In the hierarchical logistic regression, the first step comprised information on the type and number of traumatic events, the second step comprised information on the four groups of PTSD symptoms, and the third step comprised information on the three major related psychiatric disorders (MDD, AUD and SUD).
Results from hierarchical logistic regression models for three suicidal behaviours.
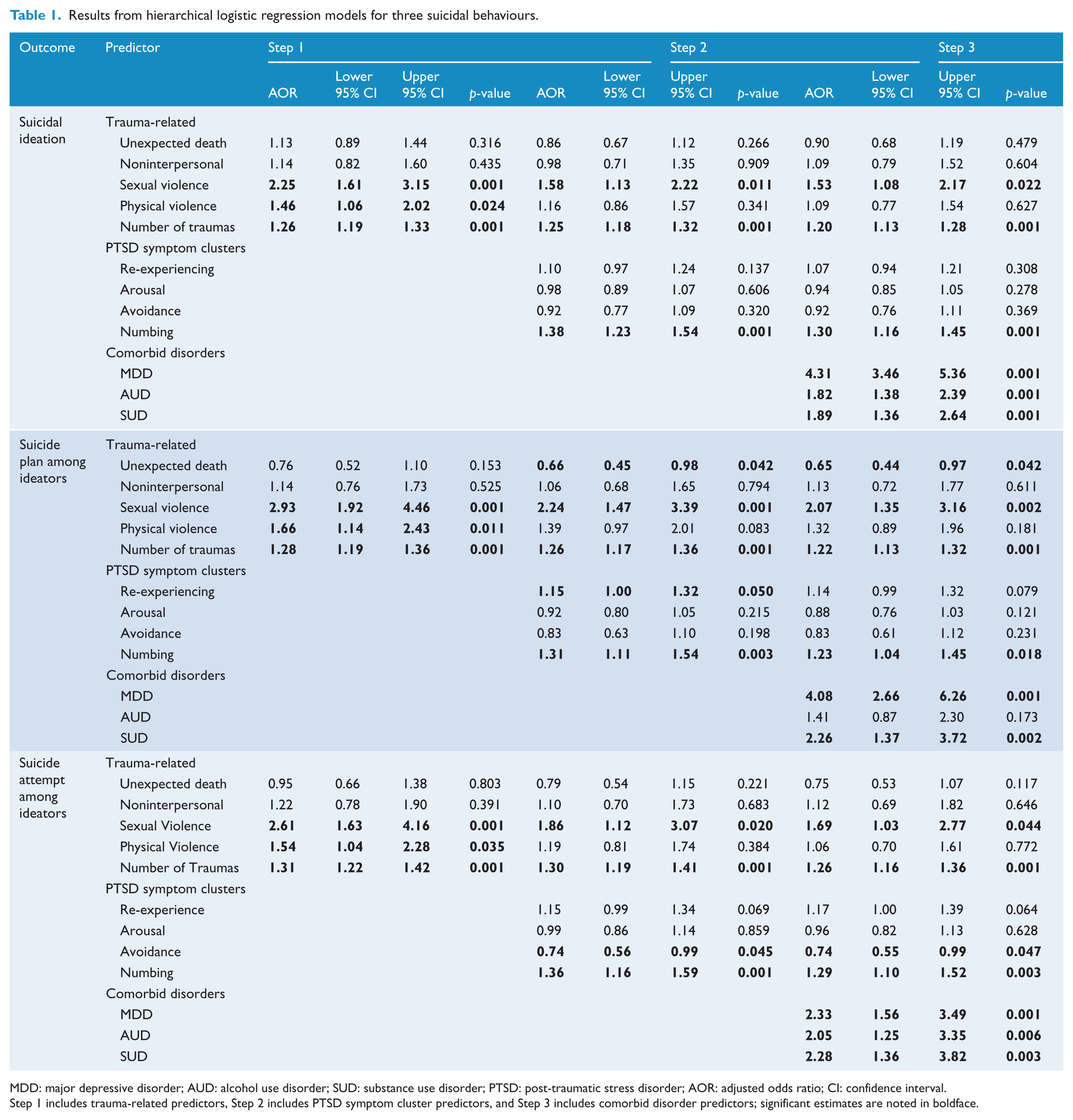
MDD: major depressive disorder; AUD: alcohol use disorder; SUD: substance use disorder; PTSD: post-traumatic stress disorder; AOR: adjusted odds ratio; CI: confidence interval.
Step 1 includes trauma-related predictors, Step 2 includes PTSD symptom cluster predictors, and Step 3 includes comorbid disorder predictors; significant estimates are noted in boldface.
In the first step, after taking into account the effects of co-occurring traumatic events and the number of traumatic events, a significant association was observed between sexual violence and suicidal ideation (AOR = 2.25, 95% CI = [1.61, 3.15], p < 0.001), suicide plan among ideators (AOR = 2.93, 95% CI = [1.92, 4.46], p < 0.001) and suicide attempt among ideators (AOR = 2.61, 95% CI = [1.63, 4.16], p < 0.001). Furthermore, significant associations were observed between physical violence and suicidal ideation (AOR = 1.46, 95% CI = [1.06, 2.01], p < 0.05), suicide plan among ideators (AOR = 1.66, 95% CI = [1.14, 2.43], p < 0.05) and suicide attempt among ideators (AOR = 1.54, 95% CI = [1.04, 2.28], p < 0.05). Finally, significant relationships were observed between number of traumatic events and suicidal ideation (AOR = 1.26, 95% CI = [1.19, 1.33], p < 0.001), suicide plan among ideators (AOR = 1.28, 95% CI = [1.19, 1.36], p < 0.001) and suicide attempt among ideators (AOR = 1.31, 95% CI = [1.22, 1.42], p < 0.001).
After introducing PTSD symptom clusters into the models, the AORs remained significant only for sexual violence and the number of traumatic events across the three outcomes. Also, significant associations were observed between emotional numbing symptoms and suicidal ideation (AOR = 1.38, 95% CI = [1.23, 1.54], p < 0.001), suicide plan among ideators (AOR = 1.31, 95% CI = [1.10, 1.54], p < 0.01) and suicide attempt among ideators (AOR = 1.36, 95% CI = [1.16, 1.59], p < 0.001). Moreover, the presence of avoidance symptoms decreased the odds of suicide attempt among ideators (AOR = 0.74, 95% CI = [0.56, 0.99], p < 0.05). These results remained consistent after the introduction of psychiatric disorders into the model.
Finally, in the third step, after addition of three psychiatric disorders to the models, significant associations were observed between MDD and suicidal ideation (AOR = 4.30, 95% CI = [3.46, 5.36], p < 0.001), AUD and suicidal ideation (AOR = 1.82, 95% CI = [1.38, 2.39], p < 0.001), as well as SUD and suicidal ideation (AOR = 1.89, 95% CI = [1.35, 2.64], p < 0.001). In the same vein, significant associations were observed between MDD and suicide attempt among ideators (AOR = 2.33, 95% CI = [1.56, 3.49], p < 0.01), AUD and suicide attempt among ideators (AOR = 2.05, 95% CI = [1.56, 3.49], p < 0.01), as well as SUD and suicide attempt among ideators (AOR = 2.28, 95% CI = [1.36, 3.82], p < 0.01). Sensitivity analysis indicated that these results remained robust after excluding respondents who reported onset of suicidality before onset of trauma.
Discussion
To our knowledge, the current study is the first to use a representative national sample to examine the association between suicidal outcomes, trauma-related characteristics, PTSD symptom clusters and psychiatric disorders. The current study adds to a nascent literature regarding the contribution of sexual violence and interpersonal violence to suicidal behaviours. The number of traumatic events emerged as a significant predictor, regardless of trauma type. Concerning the role of traumatic symptoms, the emotional numbing cluster was related to different types of suicidal behaviours. Re-experiencing symptoms were related to suicide plan, while the presence of avoidance symptoms reduced the odds of a suicide attempt. Finally, a history of psychiatric disorders significantly increased the odds of suicidal ideation and suicide attempt after taking into consideration type of traumatic events, number of traumatic events and traumatic symptoms.
When comparing the models before and after adjustment for traumatic symptoms and psychiatric disorders (i.e. MDD, AUD and SUD), the reduction in odds ratios indicates that psychopathological variables accounted for a significant portion of the association between trauma type and suicidal behaviour. It is noteworthy that there was less attenuation of the odds ratios for the number of traumatic events than other trauma-related variables. While these findings suggest psychiatric disorders partially account for the effects of specific traumas on suicidality, sexual violence remained a robust predictor of suicidal ideation and behaviours. The prominent role of sexual and physical violence is consistent with prior findings concerning higher rates of suicidality among victims of interpersonal trauma (Belik et al., 2009). Some authors suggest that the preventable nature of interpersonal trauma and feelings of personal responsibility potentially contribute to suicidality among interpersonal trauma victims (Hiley-Young et al., 1995; Panagioti et al., 2009). Other studies have found that sexual and interpersonal violence remain significantly associated with suicidal behaviour after accounting for sociodemographic characteristics and other forms of psychopathology (Belik et al., 2009; Stein et al., 2010).
The dose-response hypothesis suggests that exposure to multiple traumatic events may lead to an increase in suicidality. A review of clinical and epidemiological studies focusing on the association between trauma and suicidality reported that frequency of suicide attempt is associated with the number of lifetime traumatic events (Panagioti et al., 2009). This association has been reported in a number of studies based on large samples of adults (Jankovic et al., 2013), adolescents (Plener et al., 2011) and clinical samples (Blaauw et al., 2002). The present study lends further support to this hypothesis.
The role of emotional numbing and re-experiencing symptoms in suicidal behaviours has long been highlighted (Ferrada-Noli et al., 1998). A more recent study of a sample of American war veterans with a PTSD diagnosis also reported that the cognitive-affective symptom cluster of MDD and the emotional numbing symptom cluster of PTSD were associated with suicidal ideation (Guerra and Calhoun, 2011). These results can be interpreted in light of the interpersonal theory of suicide (IPTS). The IPTS identifies two explanatory factors of suicidal desire, namely, thwarted belongingness (i.e. social isolation) and perceived burdensomeness (i.e. feeling that one is a liability to others). However, an individual must possess not only suicidal desire but also the acquired capability for suicide (i.e. lowered fear of death and elevated physical pain tolerance) to engage in the suicidal behaviour (Van Orden et al., 2010). Prior findings indicate that emotional numbing symptoms such as loss of interest, being emotionally distant and emotional numbing might lead to the feeling of thwarted belongingness (Davis et al., 2014). The negative association between the presence of PTSD avoidance symptoms and suicide attempt could be explained by the protective nature of avoidance symptoms. More specifically, in the context of IPTS, avoidance could be negatively associated with the acquired capability for suicidal behaviour (Zuromski et al., 2014).
A growing body of research has highlighted the significant role of MDD in suicidality among trauma victims and PTSD patients. A meta-analysis examined the intervening role of depression in the association between PTSD and suicidality by testing the association between depression severity levels and the effect sizes of the association between PTSD and suicidality in different studies. Results of this meta-regression revealed a relation between depression severity and the magnitude of the association between suicidality and PTSD (Panagioti et al., 2012). Several explanations can be considered regarding the impact of depression in the PTSD/suicidality association. The first interpretation relies on the aggravating effect of depression on PTSD considering the overlap between two disorders. Second, depression severity may act as a mediating factor in the PTSD-suicidality association. Third, both PTSD and depression may play independent roles in the emergence of underlying suicide-related processual component such as feelings of hopelessness, emptiness and entrapment. Our results highlight that despite the overlap between PTSD numbing symptoms and MDD symptoms (Elhai et al., 2008, 2011), they have an additive role with regard to the different suicidal behaviours which is consistent with the underlying processual component hypothesis (Panagioti et al., 2013). These transdiagnostic processes are also implied in the association between AUD/SUD and suicidal behaviours. The important role of feelings of hopelessness and entrapment in the association between PTSD symptoms and AUD has also been highlighted (Blume et al., 2009). Likewise, in the context of IPTS, prior studies indicate that both AUD and SUD are significantly associated with thwarted belongingness and perceived burdensomeness (Conner et al., 2007; Darke et al., 2007; Lamis and Malone, 2011).
These findings should be considered in light of the following limitations. First, our data examined the presence of non-fatal suicidal behaviours but not suicide. Although non-fatal suicidal behaviours are reported as important risk factors of suicide deaths, some differences exist between fatal and non-fatal suicidal behaviours (DeJong et al., 2010). Therefore, the current findings may not be generalizable to individuals who die by suicide. Second, although the diagnosis of mental disorders established by lay interviewers using the Composite International Diagnostic Interview (CIDI) has been demonstrated to be reliable, they may not match the accuracy of clinician-based assessment (Haro et al., 2006). Third, the cross-sectional nature of our data does not permit causal inferences and assessment of psychopathological variables and temporal sequencing relied on retrospective reports, which are vulnerable to recall bias. Longitudinal research is necessary to further investigate the relationship between trauma-related variables, psychiatric disorders and suicidal behaviours. Fourth, the current study used DSM-IV criteria and did not take into consideration the changes that were made to the PTSD diagnostic criteria in DSM-5. Fifth, the survey did not comprehensively assess traumatic experiences in the early stage of life such as childhood sexual trauma and childhood interpersonal trauma that happened outside the household. Therefore, our results are unable to distinguish the differential role of childhood and adulthood trauma with respect to suicidal behaviours. Our findings provide an impetus for further research investigating the associations between trauma-related variables, PTSD symptoms, and psychiatric disorders using the new diagnostic criteria. Further research is also needed to evaluate the underlying processual mechanisms such as feelings of hopelessness, entrapment, thwarted belongingness, and perceived burdensomeness to clarify the link between trauma-related variables, psychiatric disorders, and suicidal behaviour.
Notwithstanding the above limitations, strengths of this study include the use of a large representative national sample of adults, along with the investigation of the role of type of trauma, number of trauma, PTSD symptom clusters, and the presence of other psychiatric disorders in a coherent and cohesive framework. To our knowledge, the current study is the first to present a comprehensive analysis of these three major factors associated with suicidality among trauma-exposed individuals. Although prior studies investigated the role of each factor separately, the current study provides important insights concerning the magnitude of association between each of aforementioned factors and suicidal behaviours, along with their additivity. Our results highlight the potential benefits of the comprehensive assessment of the three aforementioned risk factors for examining suicide risk among trauma victims. The use of epidemiological data overcomes some inherent problems with clinical samples. Clinical samples typically display a restricted range of symptomatology and motivation towards treatment, which hampers generalizability. In contrast, epidemiological samples present a more complete picture of the spectrum of symptoms in the population.
In closing, the findings of this study indicated that exposure to interpersonal violence was associated with suicidal thoughts and behaviours. After adjusting for previously identified correlates, sexual violence remained a significant predictor of suicidality. These findings have important implications. From a policy perspective, initiatives to increase public awareness about the traumatic effects of interpersonal violence as well as prevention of sexual and interpersonal violence holds promise for reducing, at least in part, suicidal behaviours. From a clinical perspective, this study highlights the need for a thorough assessment of trauma history, traumatic symptoms (specifically emotional numbing symptoms) and history of psychiatric disorders among trauma-exposed individuals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.