
Abstract
Objective:
As there is growing evidence outlining varying degrees of social, economic and cultural changes among minority groups in China, there was a need to undertake research to determine whether modernization and urbanization of China has had an impact on the mental health of individuals from minority groups. In 1979, the Jino ethnic minority group was the last minority group to be designated a minority by the Chinese Central Government. As a direct result of the Chinese Government intervention, the Jino society began transitioning from a traditional rural lifestyle existence to that of a more modern urban lifestyle. Our objective was to explore whether changing social and economic influences had impacted the mental health of the Jino people.
Methods:
A longitudinal study over three decades was undertaken to determine the mental health of the Jino People.
Results:
From our initial study in 1979 and subsequent follow-up studies in 1989, 1999 and 2009, there were no significant changes found for 1-month prevalence, lifetime prevalence and prognosis for schizophrenia and mental retardation among the Jino population researched. For major depressive disorders, there were significant differences, suggesting a rising trend not only in 1-month prevalence but also in lifetime prevalence. We found significant differences had occurred over the three decades for alcohol abuse, alcohol dependence and Korsakov’s psychosis. At the same time, the annual suicide incidence had increased at least three times in 2009 compared to that of 1989.
Conclusion:
Results from our three-decade longitudinal repeated cross-sectional survey show that due to rapid social, economic and cultural changes among the Jino people, serious social and mental health problems such as alcohol-related disorder, suicide and major depressive disorders have increased.
Introduction
From early 1978, the Chinese Government began a program of rapid social and economic development leading to rapid changes in the modernization and urbanization of China. The success of China’s economic policies and the manner of their implementation have resulted in immense changes to Chinese society. Large-scale government planning programs alongside market forces have helped to minimize poverty. This unprecedented rapid development has also had a profound social and economic impact on many communities across the country. The social and economic development has had a particular significant impact on many of the 56 minority ethnic groups throughout China. These numerous ethnic groups share China’s vast lands. Most live in their individual communities, many of which are isolated although relationships between them have been formed over many years. Yunnan Province in China has the proud distinction of having the most ethnic minorities numbering 26 which make up about one-third of the province’s total population. One such minority group living in the Yunnan Province, Southwest of China is the Jino minority ethnic group. This group was the last minority group to be designated a minority by the Chinese Central Government in 1979 (Wan et al., 1981, 1982).
Up until the 1970s, the Jino people had lived a traditional isolated agricultural existence that revolved around low levels of productivity with quite poor methods of cultivation. In addition to this, they were often at the mercy of ruthless destructive forces of nature (Wan et al., 1981, 1982). Through the Chinese Government intervention, the Jino society began transitioning from a traditional rural lifestyle existence to that of a more modern urban lifestyle. This modernization and urbanization has had a gradual impact on the local people’s lifestyle and living standards, as well as their emotional, psychological and physical health (Li et al., 1994; Wan et al., 1981, 1982; Zhu et al., 1994).
Over the years, various scholars have described the lifestyle of Chinese without focusing on specific minority groups or their mental health issues. Li and Yang (1972) focused their research on personality factors of the Chinese people (Li and Yang, 1972). On the other hand, Kleinman and Lin (1981, 1982) went some way in looking at behavioral characteristics of Chinese people by studying normal and abnormal behaviors. However, research with its primary focus on mental health is lacking.
It is important to understand how rapid modernization and urbanization affect the interacting emotional and psychological aspects, behavior and lifestyle of an individual and group of people. At the same time, in order to bring about positive change, we must take the necessary steps to understand how rapid social and economic development influences the nature of stress over time. Equally important is the need to understand how change brought about by social and economic forces influences the manifestation of psychopathology.
There is evidence of the varying degrees of social and economic change occurring among minority groups (SH Bidisha et al., 2012). However, what is lacking is how the changes leading to modernization and urbanization of China have impacted the mental health of minority groups.
There are various ways to study mental health which has been influenced by social and economic changes. The most frequent methods are the cross-comparison of cultures and mental health in different samples or the intensive in-depth long-term exploration in a specific culture (Tseng and David, 1985).
We chose the latter by undertaking a repeated cross-sectional survey of a specific culture, the Jino people. In addressing issues relating to mental health changes within the Jino minority population, our study, the first of its kind, was initiated in 1979. This ongoing study has been undertaken at 10-year intervals spanning three decades.
Subjects and methods
Subjects
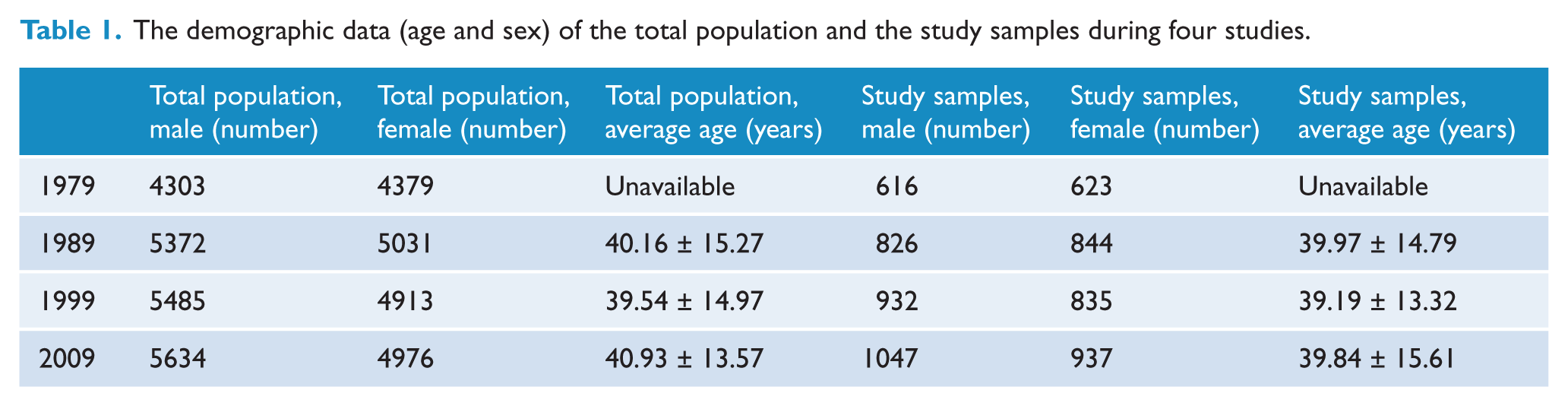
The Jino people totaling 12,108 reside in 46 unincorporated villages situated in the Jino Mountains (Li et al., 1994, 2008; Wan et al., 1982; Zhu et al., 1994) (2009 official census data). Due to factors of isolation and difficult terrain, two villages that were unreachable were excluded from this study. Data have been gathered from 44 villages using random cluster sampling. Table 1 shows the demographic data (age and sex) of the total population and the study samples during four studies undertaken.
The demographic data (age and sex) of the total population and the study samples during four studies.
Methods
Instruments
Socio-demographic information
Socio-demographic variables included gender, age, ethnicity, education level, occupational status, marital status, average annual income in the last year and self-report of adequacy of income.
Instruments used in this study
12-Item General Health Questionnaire
The 12-Item General Health Questionnaire (GHQ-12; Goldberg and Williams, 1988) was used in this study to determine possible disorders (or caseness). The validated Chinese version of the GHQ was also used in this study (Yang et al., 2003).
Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition Axis I Disorders
The study employed Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) criteria (American Psychiatric Association, 1994; First et al., 2002) for current (1 month) and lifetime prevalence of mental disorders. This assessment has been shown to be reliable and valid in China (Zhou et al., 1997). Interviewers (psychiatrists) who administered the screening instruments included common diagnoses listed in the fourth edition of Diagnostic and Statistical Manual of Mental Disorders (DSM). This allowed for the inclusion of not otherwise specified (NOS) categories of illness of subjects who displayed clinically significant symptoms combined with social dysfunction but who did not meet the full criteria for a specific disorder. Multiple current (1 month) and lifetime diagnoses ranked according to clinical importance were recorded during interviews.
Clinical Global Impressions Scale
The Clinical Global Impressions Scale (CGI) was first used in National Institute of Mental Health (NIMH)-sponsored clinical trials to provide a brief standard assessment of the clinician’s view of the patient’s global functioning (Guy, 1976). The CGI provides all available information, including knowledge of the patient’s history, psychosocial circumstances, symptoms, behavior and the impact of the symptoms on the patient’s ability to function. For the past three decades, the CGI has been shown to correlate well with standard, well-known research drug efficacy scales (Hamilton Rating Scale for Depression, Hamilton Rating Scale for Anxiety, Positive and Negative Syndrome Scale, Leibowitz Social Anxiety Scale, Brief Psychiatric Rating Scale, Scale for the Assessment of Negative Symptoms) across a wide range of psychiatric indications (Bandelow et al., 2006; Leucht and Engel, 2006; Leucht et al., 2005; Spielmans and McFall, 2006; Zaider et al., 2003). The CGI has been shown to be reliable and valid in China (Zhou et al., 1997). We used the Clinical Global Impression–Severity (CGI-S) and Clinical Global Impression–Global Improvement (CGI-I) to evaluate the function of patients. In the 7-point scale of CGI-S, 1 score was rated as normal. During our follow-up, for patients who were diagnosed previously, the score of 1 was considered equal to remission.
The Alcohol Use Disorders Identification Test
The Alcohol Use Disorders Identification Test (AUDIT) (Saunders et al., 1993; National Institute on Alcohol Abuse and Alcoholism, UDoHaHS, National Institute of Health, 2005) is a 10-item alcohol-screening questionnaire that was specifically designed to avoid cultural bias. The instrument had been validated (Li Bing, et al., 2003) and used in Chinese alcohol research (Guo et al., 2005).
Sampling, follow-up and screening
Following the initial survey in 1979, each additional survey included two parts: the follow-up and screening of the new onset patients.
Randomized cluster sampling methods were used to identify subjects. In each household, all male and female Jino subjects above 18 years of age who resided in the villages for at least 6 months of the year prior to the interview were identified. One was selected as the target subject by using a random numbers table. In the surveys carried out in 1979, 1989 and 1999, more than 15% of residents in each village were randomly selected (Li et al., 1994, 2008; Wan et al., 1982; Zhu et al., 1994).
In 2009, 1984 subjects were recruited from 44 villages accounting for 19% of the total population.
Subjects were classified into high-risk stratum, moderate-risk stratum and low-risk stratum for mental illness according to their GHQ scores (⩾4, 1–3 and 0).
All high-risk individuals along with a random selection of those at 10% of moderate, and 4% of low risk, were assigned to complete the face-to-face diagnostic assessment using the Chinese translation of the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders–4th Edition, Text Revision (DSM-IV-TR) Axis 1 Disorders (SCID-I-P).
In 2009, patients identified from the 1979–1999 interviews were followed up by using their medical records to help evaluate their prognosis.
Quality control
The studies had the support of the local Health Bureau and village committees. During the surveys, doctors from the local hospital and villages assisted in communications by using local dialect. The local hospital provided patient medical records for all subjects from the 44 villages.
In each survey, all interviewers including local doctors were trained by the same researchers three times, at weekly intervals before undertaking the initial and subsequent interviews. Diagnostic inter-rater agreement was at 0.79.
For the study, interviewers were divided into three groups consisting of two to four interviewers. Each group was supervised by an experienced psychiatrist with all questions given orally. Most of the respondents got the high school education and can speak mandarin, so at least approximately half the interviews were conducted in Mandarin. In situations where communication was difficult, mutual translation between Mandarin and local dialect was provided by a local guide or local doctors. We sourced one or two local guide(s) for each group of interviewers to assist in accessing a household. This study was approved by the Institutional Review Board of Yunnan Institute for Drug Abuse, Kunming, Yunnan Province, China (IRB 00002096). Oral informed consent was obtained before interviews.
Statistical methods
We described sample characteristics and prevalence estimates for mental diseases and other social phenomena. Cochran–Armitage trend test with z-score was used to compare trends of prevalence rates in three decades. Statistical significance was determined with an alpha level of 0.05. All calculations were carried out using SPSS 15.0
Results
Prevalence and prognosis of schizophrenia, mental retardation, major depressive disorder and alcohol-related disorders, 1979–2009
No statistically significant changes were found for 1-month prevalence, lifetime prevalence and prognosis for schizophrenia and mental retardation.
As shown in Table 2, there were significant differences for major depressive disorders, suggesting a rising trend not only in 1-month prevalence but also in lifetime prevalence.
Prevalence and prognosis of schizophrenia, mental retardation, major depressive disorder and alcohol-related disorders, 1979–2009.
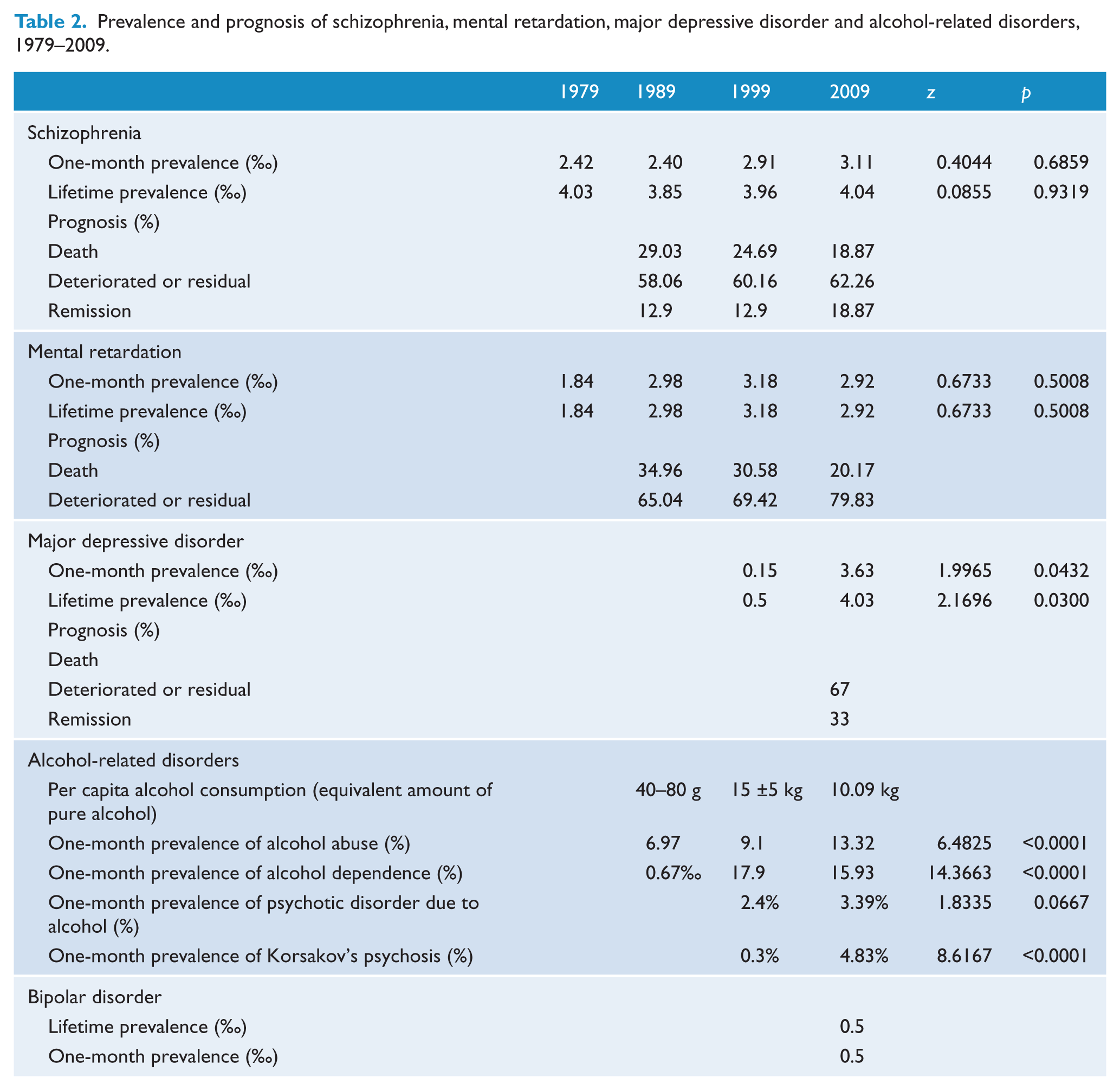
In 1979, people only drank alcohol during festival celebrations. Since 1989, except for psychotic disorder resulting from alcohol use, there were significant differences over the three decades for alcohol abuse, alcohol dependence and Korsakov’s psychosis. Various changes were observed for varieties of alcohol consumed. For example, in 1989 and 1999, local people preferred to drink white spirits; however, in the survey of 2009, people under 35 years of age preferred drinking beer more than white spirits when compared to older people.
Suicide incidence, 1979–2009
Prior to 1979, there were a total of 19 deaths due to suicide. However, in the following three decades, the suicide incidence changed significantly. The annual suicide incidence in Jino people increased at least three times (30.16/year/100,000) in 2009 compared to that of 1989 (9.61/year/100,000). The trend test showed there was a significant rising process (z = 10.708, p < 0.005).
Psychosexual disorder, divorce, crime, gambling and betting activities 1979–2009
For transsexual numbers, there was only one case from 1989 to 1999. In 2009, this had increased twofold.
Prior to 1979, there were a total of 31 divorces recorded; however, by the end of 2009, the divorce rate had gradually increased to 39.59/100,000. According to the National Statistical Report of Civil Affairs in 2009, the divorce rate among Jino people was lower than the national level (185/100,000) (Ministry of Civil Affairs of China, 2009). However, from 1989 to 2009, the divorce rate increased 2.8 times (14/100,000 and 39.59/100,000, respectively).
Crime incidence increased significantly in 1999 (35 cases, 30.82/year/100,000) when compared to that of 1989 (1 case, 7/year/100,000). In 2009, it decreased significantly to 28 cases (26.39/year/100,000).
Before 1999, there were few gambling and betting activities. However, in 2009, approximately 40% of local people in each village had purchased lottery tickets more than twice weekly.
Discussion
During our three-decade longitudinal study of the Jino ethnic minority people from 1979 to 2009, we found they have been exposed to the effects of rapid modernization and urbanization happening in China. Socially, in the Jino traditional culture where isolation is the norm, intermarriage with other ethnic minorities seldom occurred (Wan et al., 1981). We found that leading up to 1979, there were 510 marriages of which 10% were with other ethnic minorities. This social pattern has helped maintain various social and economic aspects of the Jino culture. However, rapid modernization and urbanization has directly affected the Jino people’s emotional and psychological health as well as aspects of their traditional lifestyle.
We found 1-month prevalence of schizophrenia in the Jino people changed from 2.42‰ to 3.11‰ over three decades from 1979. Small increases were found ranging from 4.03% in 1979 to 4.04% in 2009 for lifetime prevalence. However, these changes were not statistically significant. The prevalence of mental retardation mirrored a similar pattern but was lower than those found among the Han population in other Chinese provinces and cities (Cui et al., 2007).
Several researchers found that people with particular defining characteristics, living in areas where others do not share similar characteristics or where they are less common, had higher rates of mental illness (Wechsler and Pugh, 1967). Boydell et al. (2001) examined these findings with regard to ethnicity and found rates of schizophrenia increased as the proportion of ethnic minorities in the locality declined. This association was replicated by other researches (Veling et al., 2006). However, we did not find a similar phenomenon occurring in the Jino ethnic population. The difference could be due to the complexity in genetic etiology of schizophrenia; Hywel et al. (2005) reported some positive susceptible genes such as the Catechol-O-methyltransferase (COMT) could not be replicated in other ethnic groups (Hywel et al., 2005).
Although schizophrenia as a severe mental disorder was not as prevalent among the Jino people compared to other populations, its presence is cause for concern. From 1989 to 2009, the remission rate for schizophrenia increased from 12.90% to 18.87%. For the same period, 62.26% of patients had deteriorated or had residual symptoms. In our 2009 survey, only 14.6% of patients diagnosed with schizophrenia had been prescribed antipsychotic medication. The long treatment gap between onset and treatment for patients may account for the less than favorable prognosis. Others offer an alternative explanation saying people not treated are more likely to suffer prolonged illness, more marked symptoms and are less willing to accept support compared to treated individuals (Mao-Sheng Ran et al., 2009).
Several authors, on the other hand, have reported a more favorable prognosis for individuals with schizophrenia in low- and middle-income countries (Cohen et al., 2008). Our findings suggest the opposite conclusion. We believe that low economic development results in reduced mental health services leading to a negative prognostic outcome for patients. Consequently, there is a need to provide community awareness to identify the nature of the illness and for health professionals to pay closer attention to the diagnosis, treatment and prognosis of schizophrenia.
Alcohol production and consumption in China rapidly increased following the economic reform (National Bureau of Statistics of China, 1978, 2006). National and regional epidemiological studies over the past three decades have reported an increase in the prevalence of alcohol use disorders (Collaborating Research Group on Alcoholism and Related Problems, 1992; Hao, et al., 2004; Liu, et al., 1999; Zhang, et al., 2008). Our study found alcohol-related disorders increased due to increased alcohol consumption. Before 1979, the Jino people lived a very challenging lifestyle, often lacking adequate food and clothing as well as limited suitable housing conditions (Wan et al., 1981). Social drinking was predominately reserved for festival celebration. However, within a decade, the prevalence of alcohol abuse and dependence had exceeded that of major cities in China (Li et al., 1994). As early as 1999, pathological drinking, alcohol dependence, psychotic disorder and Korsakov’s psychosis had become a serious problem among the Jino population (Guo et al., 2005).
Although our study found alcohol dependence decreased marginally, various disorders due to alcohol consumption increased yearly. Individuals diagnosed as alcohol dependent or having chronic alcoholism before 1999 gradually developed a range of mental and physical disabilities. These included insomnia and hallucination along with several deaths linked to alcohol-related liver disease within the last decade. Family problems and conflicts were also on the increase due to increased alcohol consumption. During interviews, most young adults who were aware of the physical and psychological impairments caused by alcohol of others in their village preferred drinking beer, believing beer was not harmful to their health. The per capita daily consumption of beer is often 3.6–7.2 L.
‘Jino’ means ‘local people living a simple and uncomplicated lifestyle’. Only 19 cases of suicide were recorded before 1979. However, with the rapid social and economic changes, we found that within a decade, the annual incidence of suicide increased to 9.61/100,000 and within three decades to 30.16/100,000. These increases are higher than annual suicide rates recorded nationally (Phillips et al., 2002a). Reasons given by individuals surveyed for the increased suicide rate were deteriorating family relationships (46.9%), including spouse or parent–child relationship, persistent chronic physical diseases (12.5%) and alcoholism-related suicides (0.9%). These findings supported the hypothesis that acute stress and triggering life events resulting from social and economic change play an important role in the increased rate of suicide in rural China (Phillips et al., 2002b).
In 1999, the prevalence of major depressive disorder was 0.15%. Within a decade, this had increased to 3.63%, though still lower (6.1%) than in four provinces of China (Phillips et al., 2009). The increase of major depressive disorders in the Jino population may be due to the failure to recognize the disease in addition to the absence of antidepressants being prescribed. Interestingly, in a particular urban province in China, only 3.0% (1.6–4.9%) of outpatients were provided with antidepressant medication (Qin et al., 2008). The lack of recognition and treatment of major depressive disorders in the Jino population has resulted in 67% being left untreated. Efforts at reversing this finding should be long term, with a focus on the causation and treatment of depression to bring about a positive change.
The survey highlights increases in divorce, criminal activities, gambling and betting activities. Prior to 1979, 31 divorces were recorded. By the end of 2009, divorce had gradually increased to 39.59/100,000. The National Statistical Report of Civil Affairs in 2009 showed the divorce rate among Jino people was lower than the national level (185/100,000). However, from 1989 to 2009, the divorce rate had increased 2.8 times. Increases in criminal activities and gambling and betting activities were also above those for the corresponding period. The social shift mirrors the change of the Jino society and has had a profound negative impact on the lifestyle and psychological well-being of the Jino people. This is particularly so given that deteriorating family relationship was the main reason given during our study for the increased suicide rate within the Jino community.
Summing up, our three-decade follow-up study shows the rapid social, economic and cultural changes among the Jino people since 1979 have affected their mental health. Equally, we find in the same period serious mental health problems such as alcohol-related disorder, suicide and major depressive disorders have increased. Our finding of rapid social and cultural change leading to increased mental health problems seems to parallel the increases experienced by other Indigenous peoples (King et al., 2009).
During our survey, several people reported a range of physical symptoms; however, due to the lack of health services, diagnostic laboratory resources were not available to provide the necessary examinations to determine the accurate diagnosis of physical disease. Therefore, the diagnoses of somatoform disorders were not undertaken. Another limitation is that all instruments used in this study had been tested for validity and reliability in Chinese Han population but not with the Jino people using local dialect. Most respondents received high school education and could speak Mandarin. This allowed half of the respondents to be interviewed in the Mandarin language. For those whose communications were difficult, mutual translation between Mandarin and local dialect was provided by a local guide or local doctor trained by the researchers. Another limitation of the research was that persons above 18 years of age were surveyed; therefore, social and mental conditions of children and adolescents were unable to be compared. The lack of possible social determinants of mental health—such as migration, disruption of lifestyles, discrimination, disempowerment, cultural oppression and marginalization—could also be classed as a limitation in our study and should be addressed in future studies.
Despite these limitations, valuable information has been gained about the rapidly changing lifestyle of the Jino people. It is hoped our findings will be of practical use in developing mental health services and contribute to efforts designed to assist the Jino people to transition from a changing rural isolated lifestyle to a more modernized and urbanized inclusive healthy lifestyle.
Footnotes
Acknowledgements
We thank Prof. Glen. D. Edwards for his editing assistance. JianZhong Yang and ChuanYuan Kang contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been supported by Grants 81160170, 81460218 and 81660235 from the National Natural Scientific Foundation of China. These grants had no further role in study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.