
Abstract
Background:
Bipolar disorder is a common chronic illness characterized by high levels of morbidity and all-cause mortality. Lithium is one of the gold standard mood stabilizer treatments, but the identification of good, partial and non-responders in clinical settings is inconsistent.
Methods:
We used an established rating scale (the Alda scale) to classify the degree of lithium response (good response, partial response, non-response) in a large, multicentre clinically representative sample of well-characterized cases of bipolar disorders I and II. Next, we examined previously reported clinical predictors of response to determine which factors significantly differentiated between the three response groups.
Results:
Of 754 cases, 300 received lithium, for at least 6 months, as a treatment for bipolar disorder (40%). Of these cases, 17% were classified as good response, 52% as partial response and 31% as non-response. Lifetime history of mixed episodes (p = 0.017) and alcohol use disorders (p = 0.015) both occurred in >20% of partial response and non-response groups but <10% of good response cases. Family history of bipolar disorder I was of borderline statistical significance, being more frequent in the good response group (38%) compared with the non-response group (18%). There was a trend (p = 0.06) for bipolar disorder II to be associated with non-response.
Conclusions:
Only three factors previously identified as predictors of lithium response significantly differentiated the response groups identified in our sample. Interestingly, these factors have all been found to co-occur more often than expected by chance, and it can be hypothesized that they may represent a shared underlying factor or dimension. Further prospective studies of predictors and the performance of the Alda scale are recommended.
Introduction
Bipolar disorder (BD) is a common chronic illness characterized by a high risk of mood recurrences, with 80% of patients experiencing a relapse within 2 years of an index mood episode (Goodwin and Jamison, 2007; National Institute for Health and Care Excellence [NICE], 2014). The disorder is also characterized by high levels of physical comorbidity, premature death and a high risk of suicide, with a 6- to 10-fold increased risk compared to the general population (Hayes et al., 2015). Unsurprisingly, BD is ranked as one of the 10 most burdensome disorders worldwide (Collins et al., 2011; Lopez and Murray, 1998). Despite these levels of morbidity and all-cause mortality, several longitudinal observational studies have shown that prophylactic treatment, especially with lithium, can reduce relapse, suicide and premature death rates and improve functional outcomes compared to no treatment or sub-optimal treatment (Müller-Oerlinghausen et al., 1994). Furthermore, in clinical settings, lithium remains a gold standard treatment with a significantly greater reduction in recurrence rates, regardless of the polarity, relative to placebo or to other anticonvulsant mood stabilizers (BALANCE Investigators and Collaborators et al., 2010; Geddes et al., 2004; Severus et al., 2014). Lithium is the only mood stabilizer that has been shown empirically to be associated with a reduction in the risk of suicide in patients with BD (Cipriani et al., 2005; Goodwin et al., 2003).
Although lithium appears to be a highly efficacious treatment for BD in research settings, response rates to lithium prophylaxis in clinical practice are highly variable between individuals. Rybakowski et al. (2001) reported that about 30% of individuals treated with lithium are classified as excellent responders (e.g. demonstrating a total absence of affective episodes over a 10-year period of lithium prophylaxis), while Grof et al. (2002) noted that the response rate may be increased further in first-degree relatives of lithium responders. However, the corollary is that, in day-to-day clinical practice, about 30% of cases are partial responders (prescription of lithium is associated with some improvement) and up to 40% of BD cases are lithium non-responders (i.e. the introduction of lithium does not modify the course of the disease) (Baldessarini and Tondo, 2000; Garnham et al., 2007). Given these findings, there have been some efforts to identify the personal and clinical characteristics of individuals who are more rather than less likely to respond to lithium prophylaxis.
Studies that attempt to identify clinical factors associated with good outcome following the introduction of lithium prophylaxis have produced conflicting results. Two of the most quoted predictors of Good Response (GR) are the history of prophylactic response to lithium in first-degree relatives and the episodic course of the disorder with remission between episodes (Grof et al., 2002). Other clinical predictors have also been proposed such as bipolar subtype, number of mood episodes prior to the introduction of lithium, age at onset, episode index polarity, rapid cycling, comorbidities (personality, substance use or anxiety disorders) and the presence of atypical features of depression. However, in an extensive review of 43 studies and 42 clinical variables, Kleindienst et al. (2005) were only able to identify five potential predictors of clinical response to lithium. The two predictors of GR to lithium treatment were episodic illness pattern characterized as ‘mania-depression-interval’ (or MDI) and older age of onset of BD; the three predictors of poor response were higher number of pre-lithium hospitalizations, an episodic pattern of ‘depression-mania-interval’ (or DMI) and a continuous cycling pattern. The authors noted that all these findings should be interpreted with caution, as there were inconsistencies in how lithium response was defined in the different studies. Moreover, subsequent studies have not replicated these findings. For example, Garnham et al. (2007) reported that lithium responders were more likely to have an early rather than later age of onset, to have an episodic illness pattern (but did not report any differences between MDI or DMI) and to meet diagnostic criteria for BD I. Pfennig et al. (2010) found that the probability of recurrence in lithium-treated patients was negatively associated with the presence of mood-incongruent psychotic symptoms, inter-episode residual symptoms and rapid cycling. Kessing et al. (2011) found that excellent lithium responders were characterized by few earlier psychiatric hospitalizations, a manic index polarity of BD and lower levels of somatic comorbidity.
Overall, there is some agreement about the proportion of cases who are likely to show a GR (about 30%), but there is uncertainty about the putative predictors of this desired outcome. This issue has been compounded by two factors: the heterogeneity in the definition or measurement of lithium response and the lack of clinical representativeness and/or small size of study samples. These issues have been partially resolved by the introduction of the ‘Retrospective Criteria of Long-Term Treatment Response in Research Subjects with Bipolar Disorder’ (also referred to as the Alda scale) (Grof et al., 2002). The Alda scale has been used in several studies by Grof et al. (2002), Duffy et al. (2002) and Garnham et al. (2007) and has recently been shown to have moderate but substantial inter-rater agreement and reliability in a study of over 1000 cases recruited from 29 centres participating in the Consortium on Lithium Genetics (ConLiGen) network (Manchia et al., 2013). We therefore employed this assessment measure to a representative clinical sample of adult cases of BD I and II who had been prescribed lithium by clinicians at one of four clinical services located across France. In this study, we examined the demographic and clinical characteristics associated with membership of one of three previously defined lithium response categories, namely, GR, Partial Response (PR) and Non-Response (NR) (Grof et al., 2002; Manchia et al., 2013).
Methods
Ethical approval was granted by an institutional review board for a programme of research on BD, and all participants gave written informed consent for their de-identified data to be used in the research programme, which included a range of projects including database studies.
Sample
The original research sample comprised participants who were recruited between 1995 and 2008 from four French university affiliated departments of psychiatry (Paris XII, Bordeaux, Marseille and Nancy). The inclusion criteria were that the person (a) was aged ⩾18 years; (b) had a mood disorder that met Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) criteria for BD I or BD II (American Psychiatric Association, 1994); (c) currently met criteria for euthymia, which was operationalized as having scores <5 on both the Montgomery–Åsberg Depression Rating Scale (Montgomery and Asberg, 1979) and the Bech Mania Rating Scale (Bech et al., 1978); and (d) was willing and able to give written informed consent.
Assessments
Cases meeting the above inclusion criteria were assessed by psychiatrists trained in the use of the French version of the Diagnostic Interview for Genetic Studies (DIGS), which is the equivalent of the Structured Clinical Interview for DSM-IV, lifetime version (SCID-1) (Nurnberger et al., 1994). The schedule (supplemented by additional questions as appropriate) was used to record key socio-demographic, family, clinical and treatment history variables in a research database.
For the purposes of the current study, we identified BD cases who were prescribed lithium as a prophylactic treatment for at least 6 months. The records of these cases were then rated using the Alda scale (Grof et al., 2002) by a psychiatrist (C.B.-P.) who had participated in the ConLiGen reliability study (Manchia et al., 2013). The Alda scale was specifically developed to allow retrospective evaluation of prophylactic treatment response in naturalistic conditions; it comprises two subscales (A and B). The A scale score (range: 0–10) derives from items that quantify the degree of improvement due to lithium treatment (e.g. reduction in the frequency of recurrences, reduction in residual symptoms, etc.). The B scale includes five criteria (each rated 0–2, with a higher score being more negative) that represent factors that undermine the likelihood that the observed improvement is really due to the introduction of lithium. The five potential confounders incorporated in the B scale are as follows: the number of episodes before receiving lithium (B1), the frequency of episodes before receiving lithium (B2), the duration of lithium treatment (B3), the compliance during periods of stability (B4) and the use of additional medication during the period of stability (B5). The total score (TS) on the Alda scale is obtained by subtracting the B score from the A score; any negative score (i.e. the B scale score exceeds the A scale score) is recorded as 0. For the purposes of this study, we used the three reported categories of response: NR (TS < 2), PR (TS = 2–6) and GR (TS ⩾ 7).
Many of the variables recorded in clinical case notes (e.g. pre- and post-lithium recurrence rates) are used to rate the A and B scale scores for the Alda scale, so the between-group comparisons we report here focus on those characteristics that were not already utilized to make the Alda rating, but that have been identified as potentially important in predicting likelihood of response to lithium in previously published studies. These included age at onset of BD and polarity of first episode, duration of illness prior to lithium, subtype of BD, lifetime history of mixed episodes, psychotic symptoms, rapid cycling, suicide attempts, anxiety disorders, alcohol or substance use disorders (AUD and SUD), seasonal illness pattern and family history of BD I or II.
Statistical analysis
Mean and standard deviations (SDs) and frequency data including number (N) and percentages (%) were calculated for each response category. These data take into account any missing information (so each comparison gives the number of cases with available data). Non-parametric descriptive statistical tests (χ2 and Mann–Whitney U tests) were used to compare the GR, PR and NR groups. All analyses were performed using the SPSS software package, version 20, and as all variables for the comparison were selected a priori, we set statistical significance at p < 0.05 for all tests.
Results
Of the 754 cases in the research database, 300 had been prescribed lithium for at least 6 months (40%).
The study sample comprised 121 (40%) males and 179 (60%) females. Their mean age was 45.4 years (SD 13.2 years), and the mean age at onset of BD was 25.8 years (SD 10.4 years). In all, 240 cases (80%) met criteria for BD I, while 60 cases (20%) met criteria for the BD II subtype. The cases had experienced a mean of 8.5 BD episodes (SD 8.2), of which 4.9 (SD 5.1) were depressive, 3.2 (SD 4.3) were manic and 0.2 (SD 0.4) were mixed episodes. Individual had been ill for about 10–12 years prior to the introduction of lithium.
As shown in Table 1, 17% of the sample was classified as GR, 52% as PR and 31% as NR. Neither current age nor gender was associated with response category. Family history of BD I was reported in 252 cases and was of borderline statistical significance, being more frequent in the GR group (17 out of 45 patients: 38%) compared with the PR (40 out of 131 patients: 31%) and NR groups (14 out of 76 patients: 18%); there was a non-significant trend (p = 0.06) for BD II to be associated with NR. Only two other factors differed significantly between the three groups: lifetime history of mixed episodes (p = 0.017) and AUD (p = 0.015); these problems both occurred in >20% of PR and NR groups but <10% of GR cases.
Clinical characteristics of groups categorized by Good Response (GR), Partial Response (PR) and Non-Response (NR) to lithium (see text for details).
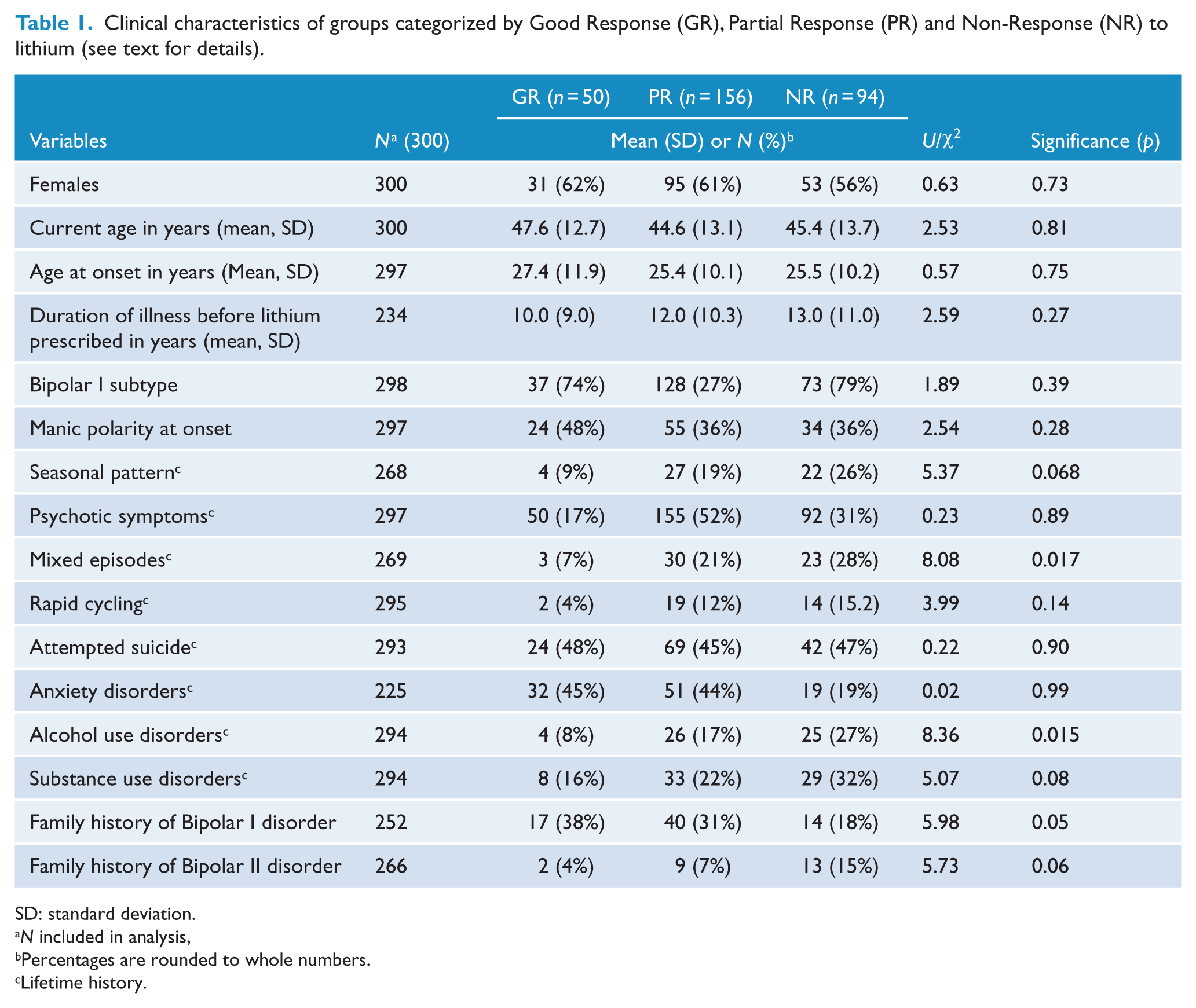
SD: standard deviation.
N included in analysis,
Percentages are rounded to whole numbers.
Lifetime history.
There were no statistically significant differences between group with regard to mean age at the onset of BD, or duration of illness prior to lithium, the characteristics of the clinical presentation (bipolar subtype, onset polarity, history of seasonal illness pattern, rapid cycling, psychotic symptoms, suicide attempts) or the lifetime history of other psychiatric comorbidities (anxiety disorder or SUD).
Discussion
Our main objective was to identify clinical factors associated with different levels of lithium response in a large, clinically representative sample of patients with BD. We identified 300 well-characterized cases of BD I and II who were prescribed lithium, for at least 6 months, at four French centres, making this one of the biggest independent studies of this issue. Of the previously purported predictors of lithium response, only three clinical factors differed significantly between the three predefined response groups: family history of BD I, lifetime history of mixed episodes and lifetime history of an AUD. Furthermore, the findings on family history of BD I should be treated with caution as data with regard to this variable were missing in 17% of the sample and the statistical significance was borderline (p < 0.05) and not corrected for multiple testing.
The finding that lifetime history of AUD and lifetime history of mixed episodes were both more common in groups associated with lower response or NR to lithium concurs with previous studies. For example, the response rate to lithium prophylaxis has been shown to be poorer in patients with BD and AUD (Frye and Salloum, 2006; Tohen et al., 1990). The mechanism of this ‘lithium resistance’ is unexplained, but there are a number of hypotheses. First, inadequate adherence may impact the response to lithium, and it is well known that individuals with AUD and SUD often show lower adherence rates than other patient populations (Aagaard and Vestergaard, 1990; Teter et al., 2011). However, other evidence indicates that lithium adherence in BD cases with comorbid AUD does not necessarily improve response. For example, patients with BD and comorbid AUD often have a younger age at onset for BD (Feinman and Dunner, 1996; Winokur et al., 1998), a higher risk of self-harm, more severe symptoms and more frequent episodes (O’Connell et al., 1991; Tohen et al., 1990) and more rapid cycling and mixed episodes (Carvalho et al., 2014); all of these characteristics may be associated with poorer response to lithium. Furthermore, in animal studies, a recent study has demonstrated that alcohol and lithium have opposing effects on behavioural circadian rhythms (Nascimento et al., 2015).
In line with our findings, previous studies have reported poorer lithium response in BD cases with a lifetime history of mixed episodes (Fountoulakis et al., 2012). Relatively few studies have investigated the long-term medication in patients with mixed episodes, but several suggest that lithium may be less effective for these patients than some of the other mood stabilizers such as valproate (Fountoulakis et al., 2012; Freeman et al., 1992; Montgomery et al., 2000; Yatham et al., 2013).
Finally, it is noteworthy that family history of BD I, AUD and mixed states often co-occur, and thus, the three predictors we have identified may represent different aspects of some underlying genetic or pathophysiological mechanism. A family history of BD has been noted as a predictor of response to lithium in several studies (Grof, 2010; Maj et al., 1985; Mendlewicz et al., 1973), although it is not always clear whether the important element is subtype of BD (I or II), family history of lithium response (i.e. pharmaco-genetic aspects) or the pattern of illness in familial cases (such as offspring presenting with a more classic ‘Kraepelian’ form of manic depression). However, studies have also noted that alcohol misuse, especially in males with BD, is often more frequent in those with family history of BD (Frye et al., 2003), and AUD appears to increase the risk of syndromal or sub-syndromal mixed states (Paykel et al., 2006).
Several limitations of this study must be acknowledged. The major weakness is the retrospective nature of the assessment of lithium response. Of course, to a certain extent, this is the only way to estimate the overall response to lithium in a large clinical sample. However, a prospective study with contemporaneous recording of clinical data pre- and post-lithium prescribing would allow more detailed analysis of other potentially important predictors and reduce any false-negative results that could have occurred in our study because of random missing data (that may have reduced the statistical power of some of our analyses or between-group differences). This would be especially helpful in assessing each of the B scale items and would offer a more reliable measure of the impact of fluctuating levels of mediation adherence and/or variations in therapeutic levels of lithium to be monitored. In this study, we note that only 4% of our cases (N = 11) had a high score on the ‘compliance item’ (B4 item score of 2). However, this does not mean that all other cases had good compliance throughout. Likewise, missing information from case notes can hamper accurate assessment of B scale items, such as detailed recordings of nature and severity of comorbidities and their treatments.
On a positive note, this study identifies several new lines for future research on predictors to lithium response, such as clarifying the nature of familial response (and the best element to choose to predict benefit from lithium) and the inter-relationships between the most robust predictors we found. In addition, it is clear that while the A and B subscales of the Alda scale are admirably pragmatic and make ‘clinical sense’, our experience of applying the scale to large clinical samples leads us to believe that there may be some benefit in reviewing the performance of the scale in more detail to determine whether further refinements could improve its ability to identify valid clinical phenotypes of lithium response for use in genetic and other studies (Schulze et al., 2010).
Conclusion
In our large French sample of individuals with BD I and II who received lithium for at least 6 months and who were characterized for lithium response using the Alda scale, we observed three factors associated with lithium response: family history of BD I, lifetime history of mixed episodes and lifetime history of an AUD. These three characteristics, previously identified as predictors of lithium response in the literature, have also been found to co-occur more often than expected by chance and may represent a shared underlying factor or dimension. Future prospective studies should test the positive and negative predictive value of this cluster of characteristics on lithium prophylactic response. Another finding, albeit weaker, is still noteworthy, namely that family history of BD I appeared to be associated with improving response, but family history of BD II showed a trend in the opposite direction – suggesting the need to explore these separately rather than as a single construct.
Footnotes
Acknowledgements
S.S., F.B. and P.A.G. were involved in the design and planning of the study. S.S., F.B., P.A.G. and J.S. identified the hypotheses for the current study. C.B.-P. undertook the lithium response assessments using the Alda Scale. S.S. carried out the literature review and drafted the main sections of the manuscript. S.S., P.A.G. and J.S. undertook the statistical analyses. S.G., J.P.-K., J.-M.A., C.H., B.E., M.L. and F.B. were responsible for the recruitment. F.B., B.E. and M.L. were, respectively, principal investigator and scientific coordinators of the research project. F.B., P.G. and J.S. assisted S.S. in writing the preliminary draft. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.S., C.B.-P., J.P.-K. declare that there is no conflict of interest. P.A.G. has received travel awards or financial compensation from AstraZeneca, Lundbeck, Menarini France and Otsuka. S.G. has received honoraria and financial compensation as independent symposium speakers from AstraZeneca, Bristol Myerrs Squib and Otsuka. J.-M.A. has received research support and has acted as consultant and/or serves on a speaker’s bureau for Bristol-Myers Squibb, Eli Lilly, Lundbeck, Otsuka, Takeda, Novartis, Pfizer, AstraZeneca, Servier and Sanofi-Aventis. C.H. has received honoraria and financial compensation as independent symposium speakers from AstraZeneca, Bristol-Myers Squibb, Otsuka. M.L. reports personal fees from Servier outside the submitted work. B.E. has received honoraria and financial compensation as independent symposium speakers from Lundbeck, AstraZeneca, Bristol-Myers Squibb, Otsuka and Servier. F.B. has received honoraria and financial compensation as independent symposium speakers from Sanofi-Aventis, Lundbeck, AstraZeneca, Eli Lilly, Bristol-Myers Squibb and Servier and has received peer review research funding from French Ministry of research, Assistance Publique – Hôpitaux de Paris, the National Institute for Research (INSERM) and the NARSAD. J.S. is a visiting professor at Diderot University. J.S. has received grant funding from the Stanley Foundation (for work on lithium and medication adherence), from the Medical Research Council UK (including for projects on actigraphy and bipolar disorders) and from the Research for Patient Benefit programme UK (PB-PG-0609-16166: Early identification and intervention in young people at risk of mood disorders). The FondaMental foundation has received funding from Sanofi-Aventis (sponsorship of the Psy COH BP cohort project), Roche Laboratory (sponsorship of the Autism InfoR cohort), Otsuka and Lundbeck laboratories (FondaMental Conferences), Eli Lilly & Co. (FondaMental PhD grant) and Servier (FondaMental Post Doctoral grant).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by INSERM and Assistance Publique des Hôpitaux de Paris (Research Project number C0829 and P111002, Ethics Approval number IDRCB2008-AO1465-50).