
Abstract
Objective:
Irritable mood is common in children with attention-deficit/hyperactivity disorder. Research to date has primarily comprised cross-sectional studies; thus, little is known about the antecedents of irritability. Furthermore, existing cross-sectional studies generally focus on the association between irritability and comorbidities and do not examine broader aspects of functioning. Finally, previous research has neglected to include child-report of irritability. This study aimed to address these gaps using data from a longitudinal study of children with attention-deficit/hyperactivity disorder.
Method:
Children aged 5–13 years (mean = 10.2; standard deviation = 1.9) with attention-deficit/hyperactivity disorder were recruited from pediatric practices across Victoria, Australia. This study reports on those who had reached adolescence (12 years or older, mean = 13.8; standard deviation = 1.2) at the 3-year follow-up (n = 140). Internalizing and externalizing problems were measured using the Strengths and Difficulties Questionnaire. At follow-up, parent-reported and adolescent self-reported irritability was assessed using the Affective Reactivity Index. Parent and adolescent outcomes measured at follow-up included attention-deficit/hyperactivity disorder symptom severity, sleep, behavior and parent mental health.
Results:
Children with externalizing problems at age 10 had higher parent-reported irritability (β = 0.31, 95% confidence interval = [0.17,–0.45], p = 0.001) in adolescence. Cross-sectional analyses found that irritability was associated with increased attention-deficit/hyperactivity disorder symptom severity and sleep problems; poorer emotional, behavioral and social functioning; and poorer parent mental health.
Conclusion:
Our findings highlight the importance of assessing for and managing early conduct problems in children with attention-deficit/hyperactivity disorder, as these predict ongoing irritability which, in turn, is associated with poorer functioning across a number of domains.
Attention-deficit/hyperactivity disorder (ADHD) affects an estimated 5% of children worldwide (Polanczyk et al., 2007). Children with ADHD often have difficulties with emotional dysregulation and irritable mood (Shaw et al., 2014). Children with ADHD and high levels of irritability are more impaired than children with ADHD who do not have excessive irritability. In a sample of 500 clinically referred children with ADHD aged 6–18 years (mean [M] = 10.2; standard deviation [SD] = 3.2), Ambrosini et al. (2012) found that irritability was associated with comorbid depression and oppositional defiant disorder (ODD), as well as ADHD-combined type. Irritability has been defined as a mood that is characterized by a proneness to anger (Vidal-Ribas et al., 2016). While most people experience irritability at some point, high levels of irritability are pathological, and irritability is included in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) as a symptom of number of both internalizing and externalizing psychiatric disorders (American Psychiatric Association, 2013). It has been proposed that irritability specifically, and emotion dysregulation more broadly, is partially responsible for the high rates of comorbidities in children with ADHD (Shaw et al., 2014).
The few studies examining correlates of irritability in children with ADHD have found that irritability is associated with poorer global (Biederman et al., 2012; Mick et al., 2005) and social functioning (Biederman et al., 2012) and greater severity of ADHD symptoms (Ambrosini et al., 2012; Sobanski et al., 2010), while stimulant medication use has been found to reduce irritability levels (De la Cruz et al., 2015). Recently, a large community study reported 22% of 6- to 8 -year-old children with ADHD met criteria for comorbid disruptive mood dysregulation disorder (DMDD) (Mulraney et al., 2016), a new DSM-5 diagnosis characterized by severe emotional and behavioral problems with the hallmark feature of chronic irritability. In this sample, DMDD was associated with increased prevalence of ODD, conduct disorder and anxiety disorders. Mulraney et al. (2016) also reported that DMDD was associated with increased risk of engaging in bullying behaviors, poorer self-control and poorer family quality of life.
In the general population, irritability is associated with psychopathology (Copeland et al., 2015; Mulraney et al., 2014a; Stoddard et al., 2014), and longitudinal studies have found irritability to be independently predictive of internalizing disorders (Leibenluft et al., 2006; Stringaris et al., 2009). More broadly, irritability is associated with poor sleep (American Psychiatric Association, 2013). Parent- and child-reported irritability has also been associated with poor behavioral (Mulraney et al., 2014b; Stringaris et al., 2012), emotional (Mulraney et al., 2014b; Stringaris et al., 2012) and social functioning (Mulraney et al., 2014b). Rates of agreement between parent- and child-reported irritability range from moderate to good (r = 0.42–0.73) (Mulraney et al., 2014b; Stringaris et al., 2012), pointing to the need to collect data from multiple sources, although the majority of studies only measure parent-reported irritability. Wiggins et al. (2014) measured maternal depressive symptoms and child irritability at five time points from 1 year through to 9 years of age and found evidence of a bi-directional relationship between irritability and maternal depression. Child irritability at ages 3 and 5 predicted maternal depression at ages 5 and 9, while maternal depression at ages 1 and 3 predicted child irritability at ages 3 and 5.
In summary, longitudinal research in the general population has demonstrated that children with high levels of irritability are at greater risk of poor outcomes, and their parents have poorer mental health (Leibenluft et al., 2006; Stringaris et al., 2009; Wiggins et al., 2014). Associations exist for both parent- and child-reported irritability although there is only a moderate correlation between irritability symptoms reported by parents and children. Children with ADHD are more likely to experience high levels of irritability than the general population, yet research to date is predominantly cross-sectional. Thus, little is known about the antecedents of irritability for children with ADHD. Additionally existing cross-sectional studies have generally focused on the association between irritability and comorbidities and do not examine broader aspects of functioning that are relevant to young people such as school attendance. Finally, previous research has neglected to include child-report of irritability in children with ADHD. As such, it is important that a more comprehensive understanding is gained of the factors that are associated with and predictive of both parent- and child-reported irritability in children with ADHD.
This study aims to determine whether, in a sample of children with ADHD,
Child internalizing and externalizing problems predict adolescent irritability 3 years later;
Child (behavior, sleep, school attendance) and parent factors (parental mental health) are associated with adolescent irritability.
It is hypothesized that child internalizing and externalizing problems will predict ongoing parent- and adolescent-reported irritability 3 years later. It is further hypothesized that increased parent- and adolescent-reported irritability will be associated with poorer parent-, teacher- and self-reported emotional, behavioral and social functioning and with parent-report of poorer adolescent sleep and decreased school attendance.
Methods
Participants
Participants were adolescents drawn from a cohort of Australian children with ADHD diagnosed by a pediatrician. They were recruited at baseline aged between 5 and 13 years (M = 10.2; SD = 1.9) as part of the Attention to Sleep (ATS) study (Lycett et al., 2014) in 2010–2012, and a subsample (those who were at least 12 years at follow-up) have been followed up 2.9 (SD = 0.7) years later. Ethics approval was granted by the Human Research Ethics Committees of The Royal Children’s Hospital (#33206), the Victorian Department of Education and Training (#2013_002202) and the Catholic Education Office (#1958).
Eligibility and recruitment
Participants were originally enrolled in the ATS study, a longitudinal study investigating behavioral sleep problems in children with ADHD (Lycett et al., 2014). Briefly, 392 children recruited from 21 public and private pediatric practices, with an ADHD diagnosis from their pediatrician, which in accordance with national guidelines requires cross-situational impairment at kindergarten or school as well as home (National Health & Medical Research Council, 2012), who at recruitment met the full Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria for ADHD, as measured on the ADHD Rating Scale-IV (Dupaul et al., 1998), participated in the study. The study comprised children with a range of sleep problems from none to severe. Children with no/mild sleep problems (n = 148) and moderate/severe sleep problems (n = 244) were recruited, with the moderate/severe sleep problems group also participating in a randomized controlled trial (RCT) (Hiscock et al., 2015). Children were ineligible if (1) their primary caregiver did not have sufficient English language ability to take part or (2) if the child had an intellectual disability (IQ < 70) or a significant medical condition (e.g. cerebral palsy) that may have confounded outcomes. Once enrolled at baseline, parents completed a paper-based questionnaire and the Anxiety Disorders Interview Schedule for DSM-IV (Silverman and Albano, 2006) conducted by a telephone interview with a trained researcher to assess child comorbid mental health conditions.
For this study, invitation letters were sent to the 221 families from ATS who consented to follow-up and were at least 12 years old, of whom 140 (63%) participated. At follow-up, families were mailed a letter describing the study and inviting them to hear more about the study. Those who did not opt out after 10 working days were contacted by a member of the research team to discuss participation. Informed written consent was provided by the parent/guardian and adolescent. At follow-up, parents completed a short questionnaire, and in addition, the majority of adolescents (n = 122) also completed an online questionnaire. The questionnaires were completed by the parent and/or adolescent on their own, using a hand-held tablet. A researcher was present and provided assistance when needed. With parental permission, the adolescent’s teacher was also contacted and asked to complete an online questionnaire about the adolescent’s behavior at school.
Measures
All measures were collected at follow-up only unless otherwise specified.
The parent and adolescent self-reported Affective Reactivity Index (ARI) (Stringaris et al., 2012) was used to measure adolescent irritability (parent: α = 0.89; self: α = 0.85). The ARI comprises six items, measuring irritable behavior, including frequency, duration and threshold (e.g. ‘loses his/her temper easily’). Respondents rate each item using as 3-point Likert scale (0 = ‘not true’ to 2 = ‘certainly true’). Items are summed to give a total score (0–12), with higher scores indicative of chronic irritability. The ARI has good psychometric properties and is valid for use in children aged 5–17 years (Stringaris et al., 2012).
The ADHD Rating Scale-IV (DuPaul et al., 1998) was used to assess participant ADHD symptom severity. The scale has 18 items, assessing inattention and hyperactivity/impulsivity symptoms, as reflected in the DSM-IV (American Psychiatric Association, 2000). Parent (α = 0.90) and teacher (α = 0.95) versions were completed. Respondents rated behaviors exhibited by the child over the previous 6 months in the setting observed (home or classroom) on a 4-point scale from 0 = never or rarely to 3 = very often. A total symptom severity score was summed, with higher scores reflecting more severe symptoms.
Internalizing and externalizing problems were measured at baseline using the parent-reported emotional problems (α = 0.71) and conduct problems (α = 0.74) subscales of the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997). The SDQ comprises 25 items across five subscales (each with five items): emotional problems, hyperactivity-inattention, peer problems, conduct problems and prosocial behavior. Items are rated based on behavior over the previous 6 months, on a 3-point scale from 0 = ‘not true’ to 2 = ‘certainly true’. Cut points have been developed to indicate the presence of clinically significant symptoms, scores >4 are indicative of clinically significant emotional symptoms and scores >3 are indicative of clinically significant conduct problems. At follow-up, we report on the emotional (parent: α = 0.73; teacher: α = 0.78; self: α = 0.73), conduct (parent: α = 0.76; teacher: α = 0.74; self: α = 0.62) and peer problems (parent: α = 0.67; teacher: α = 0.77; self: α = 0.62) subscales.
Sleep problems were evaluated using the disorders of initiating and maintaining sleep (DIMS) subscale from the Sleep Disturbance Scale for Children (SDSC) (six items; α = 0.79). Parents reported on their adolescent’s sleep quality and sleep patterns around going to sleep and night-time waking over the past 6 months. The total score is summed for each item (1–5), and higher scores indicate more problematic sleep (Bruni et al., 1996).
School attendance was measured by asking parents and teachers the number of whole school days the adolescent has missed in the preceding 3 months. These questions are commonly used in school-aged children to measure days absent (Sciberras et al., 2010).
Comorbid disorders (internalizing and externalizing) were assessed at baseline, using the Anxiety Disorders Interview Schedule for DSM-IV (ADIS-C) (Silverman and Albano, 2006), a diagnostic interview assessing mental health disorders according to DSM-IV criteria. Children screened positive for a disorder if they met full criteria, and clinical impairment was indicated. Children were classified as having an internalizing problem if they screened positive for 2 or more anxiety disorders (e.g. specific phobia and generalized anxiety) or one mood disorder (e.g. dysthymia or major depression)—this approach provides high sensitivity and specificity for detecting internalizing comorbidities in children with ADHD (Mennin et al., 2000). An externalizing comorbidity was classified if they screened positive for conduct disorder or ODD.
Recent parent mental health symptoms were assessed using the 21-item Depression Anxiety Stress Scale (DASS-21) (Lovibond and Lovibond, 1996), which comprises three subscales: depression (α = 0.94), anxiety (α = 0.81) and stress (α = 0.89). Parents rate the extent to which they have experienced each symptom (e.g. ‘I find it difficult to relax’) over the past 4 weeks, on a 4-point scale from 0 ‘not at all’ to 3 ‘most of the time’, with higher scores reflecting poorer mental health (Henry and Crawford, 2005).
We also measured child age, gender and current ADHD medication use. Parent and family measures include parent education and family income. The Socio-Economic Indexes for Areas (SEIFA) Disadvantage Index was used as a measure of neighborhood disadvantage, with higher scores reflecting less disadvantage (M = 1000, SD = 100) (Australian Bureau of Statistics, 2008).
Statistical analysis
Descriptive statistics were used to examine sample characteristics at follow-up and to compare baseline sample characteristics between children who participated in the follow-up (participants) and those who did not (non-participants). Linear regressions examined whether clinically significant internalizing and/or externalizing problems at age 10 predicted parent-report of adolescent irritability at age 13 (Aim 1). Internalizing/externalizing problems were examined individually in univariate analyses, and then analyses were repeated in an adjusted model that accounted for ADHD symptom severity, ADHD medication use (yes/no), adolescent age and neighborhood disadvantage as these are all factors shown to be associated with child irritability (Ambrosini et al., 2012; Copeland et al., 2014; Dougherty et al., 2014). A second adjusted model was then conducted that took into account internalizing/externalizing problems at follow-up. A series of univariate linear regressions were conducted to determine the cross-sectional associations between parent-reported irritability and a range of adolescent and parent factors (Aim 2), and then analyses were re-run using an adjusted regression model to account for ADHD medication use, adolescent age and neighborhood disadvantage. For participants with self-reported data (n = 122), all analyses were repeated with adolescent self-reported irritability as the outcome. A sensitivity analysis found no effect of RCT group allocation on the results, so we did not control for RCT group status in our adjusted analyses. All analyses were conducted using STATA version 13.0.
Results
Sample characteristics
The sample characteristics are displayed in Table 1. The mean age of participants at follow-up was 13.8 years (SD = 1.1, range = 12.1–16.7 years), and 89% were male. Despite the majority of participants (72%) taking ADHD medication, ADHD symptoms were above the 90th percentile (DuPaul et al., 1998) (M = 31.0, SD = 9.7, range = 3–50). There was a moderate correlation of r = 0.43 (p < 0.001) between parent- and self-reported irritability, with parents reporting higher levels of irritability (M = 5.6, SD = 3.4) than adolescents (M = 3.5, SD = 3.0, p < 0.001). There was no difference in gender, baseline ADHD subtype, symptom severity or medication use, or comorbidities between participants and non-participants. Participants came from a higher socio-economic background, and their parents had fewer depressive symptoms than non-participants. Participants were also older than non-participants, although this is to be expected given that the follow-up only included those participants who were 12 years or older at that time point (see Supplementary Table 1).
Sample characteristics at follow-up.
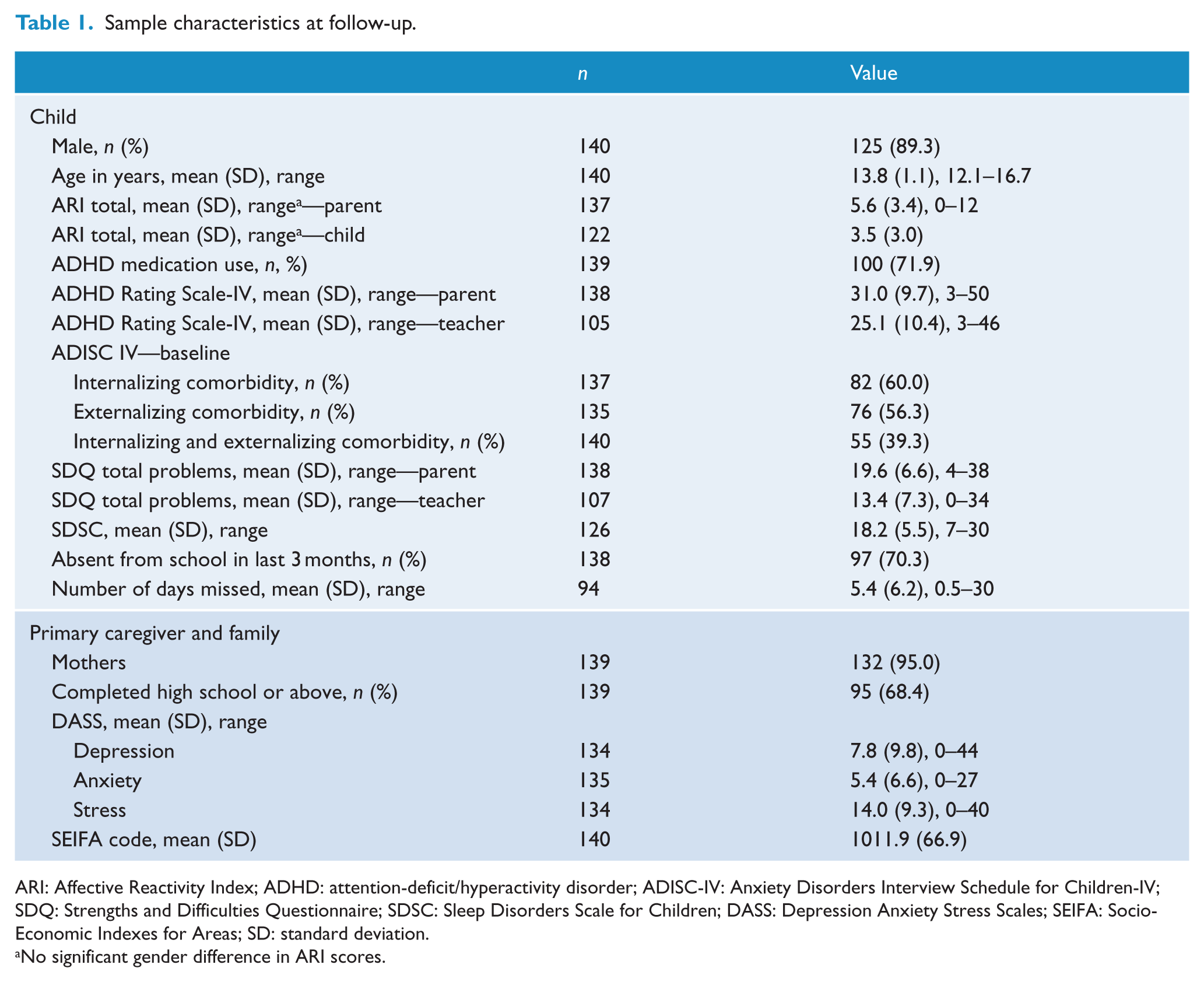
ARI: Affective Reactivity Index; ADHD: attention-deficit/hyperactivity disorder; ADISC-IV: Anxiety Disorders Interview Schedule for Children-IV; SDQ: Strengths and Difficulties Questionnaire; SDSC: Sleep Disorders Scale for Children; DASS: Depression Anxiety Stress Scales; SEIFA: Socio-Economic Indexes for Areas; SD: standard deviation.
No significant gender difference in ARI scores.
Comorbidity profiles predictive of irritability in adolescents with ADHD (Aim 1)
The presence of elevated externalizing problems (β = 0.31; 95% confidence interval (CI) = [0.17, –0.45]; p < 0.001) predicted parent-reported irritability even after adjusting for current externalizing problems, child age, ADHD medication use, ADHD symptom severity and neighborhood disadvantage (Table 2). Elevated internalizing problems and co-occurring internalizing/externalizing problems predicted parent-reported irritability in the first adjusted model (p < 0.001 and p = 0.001, respectively); however, neither of these associations remained significant once internalizing and externalizing problems at follow-up were added to the model. There was no relationship between internalizing or externalizing problems at baseline and self-reported irritability once the analysis accounted for the impact of confounders.
Relationship between internalizing and externalizing problems at age 10 and irritability at age 13 (Aim 1).
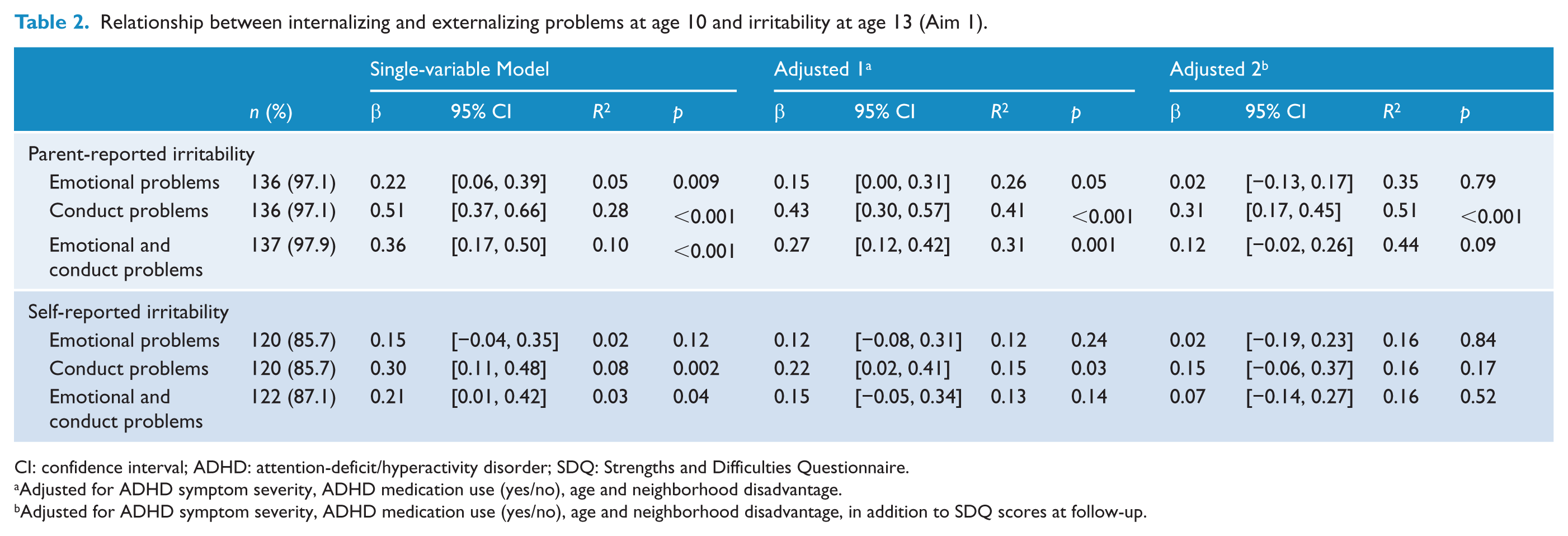
CI: confidence interval; ADHD: attention-deficit/hyperactivity disorder; SDQ: Strengths and Difficulties Questionnaire.
Adjusted for ADHD symptom severity, ADHD medication use (yes/no), age and neighborhood disadvantage.
Adjusted for ADHD symptom severity, ADHD medication use (yes/no), age and neighborhood disadvantage, in addition to SDQ scores at follow-up.
Correlates of irritability in adolescents with ADHD (Aim 2)
Parent-reported irritability was associated with increased ADHD symptom severity by both parent-report (β = 0.45; 95% CI = [0.30, –0.60]; p < 0.001) and teacher-report (β = 0.33; 95% CI = [0.16, –0.49]; p < 0.001) (see Table 3). Sleep problems, number of school days missed, and parent-, teacher- and self-reported emotional, conduct and peer problems were all associated with irritability. Higher levels of irritability were associated with increased parent stress (β = 0.37; 95% CI = [0.22, –0.53]; p < 0.001), anxiety (β = 0.23; 95% CI = [0.10, –0.38]; p = 0.003) and depressive symptoms (β = 0.37; 95% CI = [0.18, –0.56]; p < 0.001). All associations remained significant after adjustment for adolescent age, ADHD medication use and neighborhood disadvantage.
Child factors associated with parent-reported irritability (Aim 2).
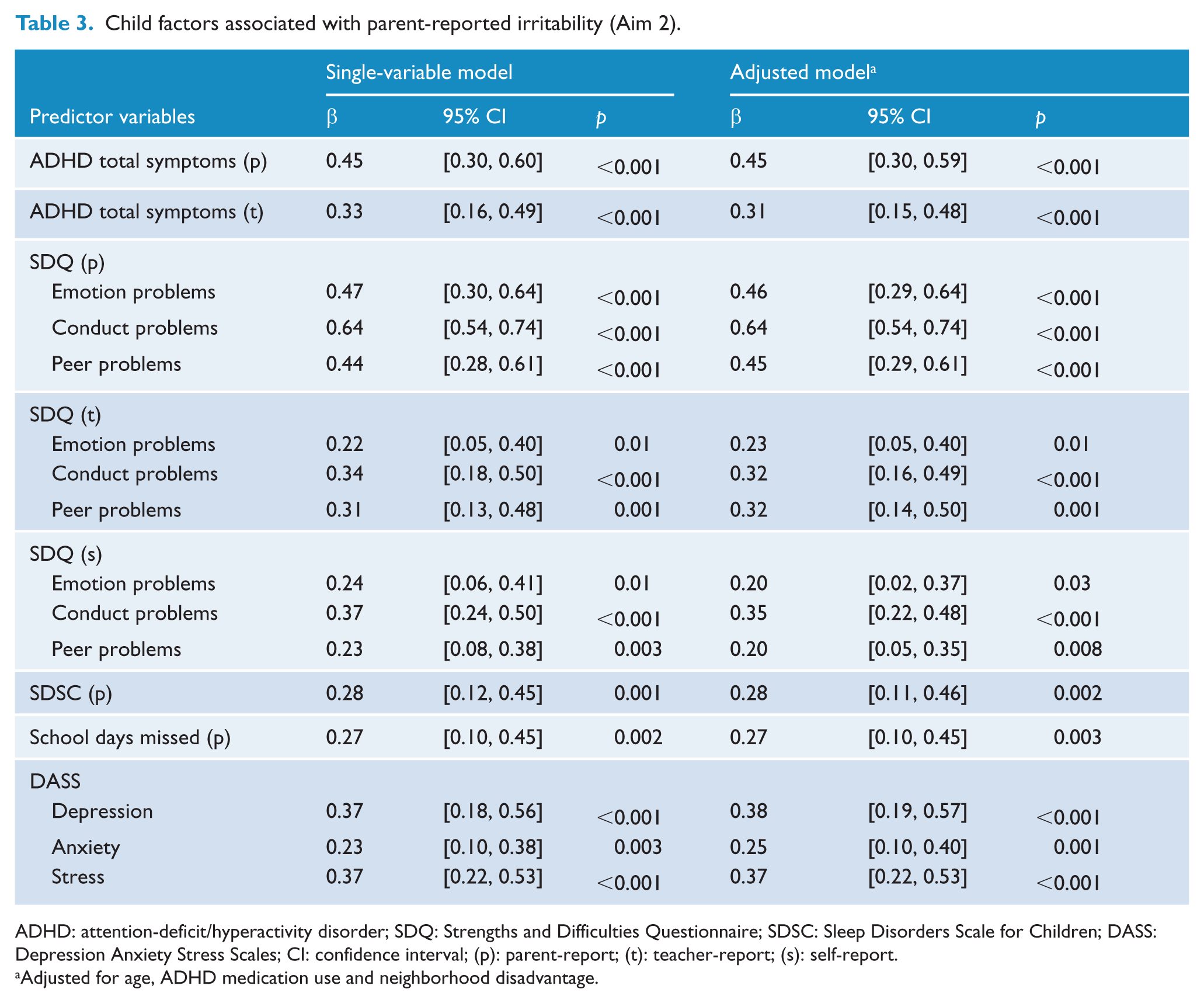
ADHD: attention-deficit/hyperactivity disorder; SDQ: Strengths and Difficulties Questionnaire; SDSC: Sleep Disorders Scale for Children; DASS: Depression Anxiety Stress Scales; CI: confidence interval; (p): parent-report; (t): teacher-report; (s): self-report.
Adjusted for age, ADHD medication use and neighborhood disadvantage.
When adolescent self-reported irritability was the outcome variable, there was no longer an association between irritability and ADHD symptoms, sleep or number of school days missed in adjusted analyses (see Table 4). Self-reported irritability was associated with increased parent- and self-reported emotional, conduct and peer problems and increased teacher-reported conduct problems.
Child factors associated with self-reported irritability (Aim 2).
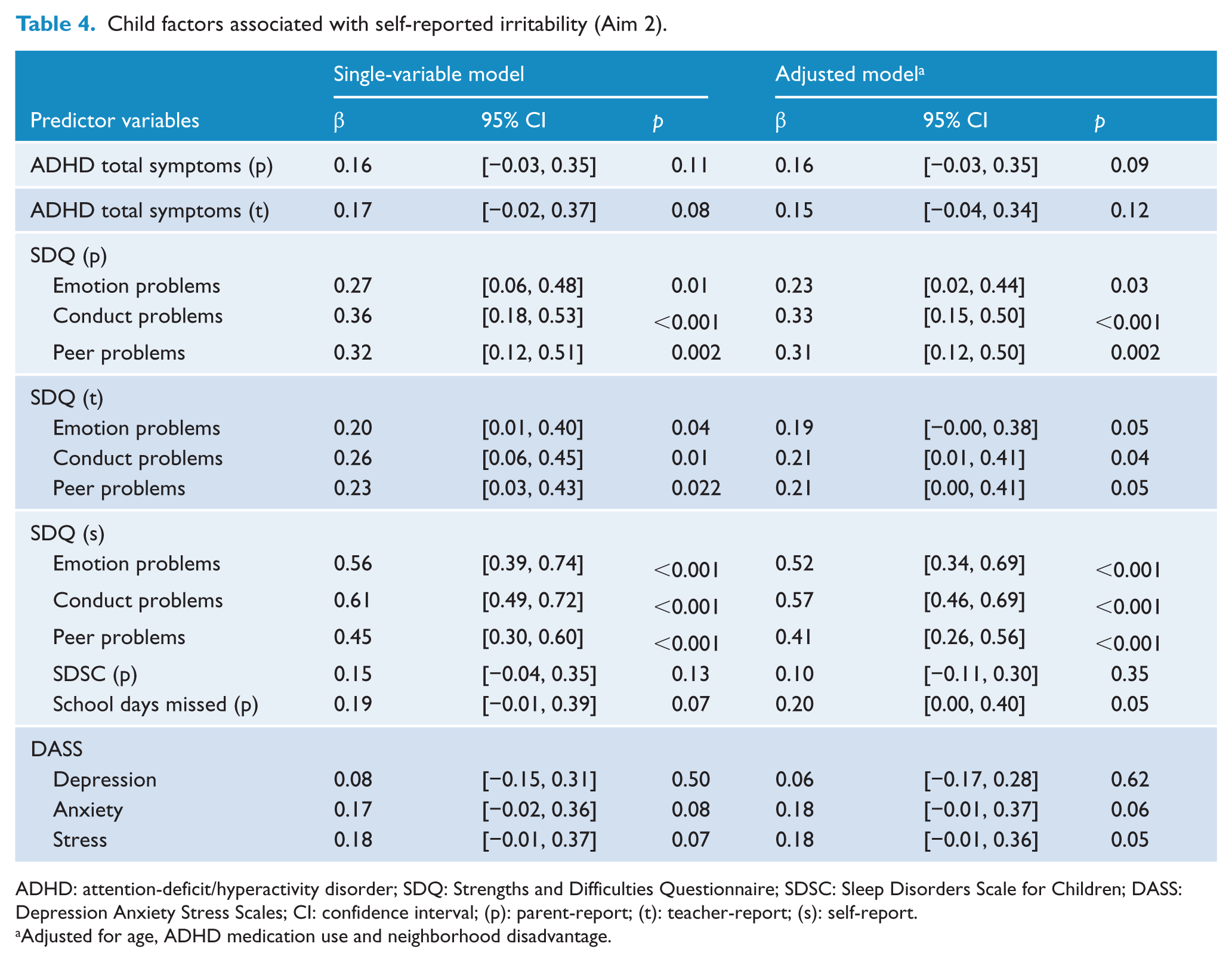
ADHD: attention-deficit/hyperactivity disorder; SDQ: Strengths and Difficulties Questionnaire; SDSC: Sleep Disorders Scale for Children; DASS: Depression Anxiety Stress Scales; CI: confidence interval; (p): parent-report; (t): teacher-report; (s): self-report.
Adjusted for age, ADHD medication use and neighborhood disadvantage.
Discussion
Within a sample of adolescents with ADHD, irritability was associated with increased ADHD symptom severity and sleep problems; poorer emotional, behavioral and social functioning; increased symptoms of depression, anxiety and stress in parents; and more school days missed. These associations were generally consistent for outcomes reported by parents, teachers and adolescents themselves demonstrating the pervasive impact that irritability has on functioning across multiple situations (e.g. at home, at school, with peers). The presence of externalizing problems at mean age 10.2 years predicted parent-reported irritability at 13.8 years.
In the general pediatric population, irritability is associated with both internalizing and externalizing disorders in cross-sectional studies but is predictive of only internalizing disorders in longitudinal studies (Leibenluft et al., 2006). In this study, we examined the converse of this relationship, i.e., whether internalizing and externalizing problems predicted later irritability. We found that the presence of an externalizing problem was predictive of irritability approximately 3 years later in children with ADHD. This is consistent with Okado and Bierman (2014) who found that early externalizing difficulties predicted mood dysregulation in adolescence. To our knowledge, this is the first study to examine whether early internalizing problems are an antecedent of irritability. We found that internalizing problems were predictive of irritability, but this relationship appears to be driven by the presence of persistent emotional problems from childhood to adolescence in this population as the relationship attenuated in the fully adjusted model.
Consistent with prior work, we found that irritability was associated with greater severity of ADHD symptoms (Ambrosini et al., 2012; Sobanski et al., 2010) and poorer social functioning (Mulraney et al., 2016). Consistent with findings in the general pediatric population, we also found that irritability was associated with poorer behavioral, emotional and social functioning. Wiggins et al. (2014) demonstrated that there is a bi-directional relationship between maternal depression and irritability in young children. Our results extend this by demonstrating a relationship between adolescent irritability and symptoms of parental depression, anxiety and stress.
A novel aspect of this study is the inclusion of adolescent self-reported irritability and behavior, and teacher-report of behavior, given that previous studies in ADHD samples have largely been restricted to parent-reported data (Ambrosini et al., 2012; Biederman et al., 2012; Mick et al., 2005; Mulraney et al., 2016). The findings from the self-report and teacher-report data echo the findings from parents; irritability is associated with a broad range of functional difficulties for young people with ADHD and those around them. When assessing symptoms such as irritability, which may not always manifest in a manner observable to parents, it is particularly important to include child self-report. The self-reported findings from this study are consistent with Mulraney et al.’s (2014b) reported association between irritability, emotional problems, conduct problems and peer problems and with Stringaris et al.’s (2012) findings of an association between irritability and emotional and conduct problems in children and adolescents. Given this and the well-established negative sequelae of irritability (e.g. suicide, Pickles et al., 2010; substance abuse, Copeland et al., 2014), it is clear that adolescents with ADHD and irritability are in need of treatment. However, currently there is little evidence to support specific treatments for irritability. Tourian et al. (2015) conducted a review of the literature regarding pharmacological treatment of DMDD. Given DMDD has only recently been defined, the authors extrapolated from treatment studies of severe mood dysregulation (which has been identified as an earlier version of DMDD) and treatment studies that report on key symptoms of DMDD such as temper outbursts and irritability. There is some evidence that methylphenidate in conjunction with behavior modification may improve irritability in children with ADHD (Pappadopulos et al., 2006). A number of studies have found atypical antipsychotics reduce irritability in the context of autism (Pappadopulos et al., 2006). However, the definition of irritability in autism is quite different from how irritability is defined in other populations. Typically, the Aberrant Behavior Checklist Irritability subscale is used to measure irritability in autism (Vidal-Ribas et al., 2016). This subscale includes items measuring self-harm and depression; thus, the results from these studies may not be comparable with other research. It may be that existing pharmacological and psychosocial interventions targeting emotional and behavioral problems may reduce irritability, but these are yet to be rigorously evaluated.
This study has several notable strengths. First, the sample was recruited from a number of pediatric practices across rural and metropolitan areas and as such is a good reflection of children being treated for ADHD by pediatricians in the Australian community. However, results may not generalize to children with ADHD who are not under the care of a pediatrician. Multiple informants (i.e. parent, teacher and child) were used to measure outcomes and predictors of interest, providing unique information from different perspectives and in different contexts. The longitudinal nature of the study allowed us to examine antecedents of irritability. Limitations include not having an assessment of irritability at baseline, as such it is not known whether the associations found are predictive or are continuations of patterns that existed, unmeasured, at baseline. Future research should measure irritability and associated constructs at multiple time points across childhood and adolescence to elucidate the nature of relationships over time. Only 35% of the original sample participated in the follow-up which may limit the generalizability of our results. We compared participants with non-participants on key baseline characteristics (e.g. ADHD symptom severity, socio-demographics) and found that non-participants tended to have parents with more depressive symptoms and come from lower socio-economic backgrounds (see Supplementary Table 1). As with the majority of research in ADHD there was a very strong gender bias in this study, our sample only included 15 girls at follow-up; thus, results may not generalize to girls. There is evidence to suggest that girls may experience irritability differently to boys (Vidal-Ribas et al., 2016) and that disruptive behavior disorders in girls are associated with multiple adverse outcomes (Molen et al., 2015). Future research should endeavor to include a greater number of girls with ADHD.
These findings have a number of important implications. The results clearly show that high levels of irritability, over and above ADHD symptom severity, have significant impacts on young people at home and at school, and on their parents. Given that early externalizing problems predicted irritability in young people with ADHD, early detection and treatment of comorbid disorders in ADHD may be a key way of reducing long-term irritability and its associated adverse outcomes. While there is significant work that needs to be undertaken to advance our understanding of how to manage comorbidities in ADHD, evidence is beginning to emerge of effective interventions. For example, Hiscock et al. (2015) demonstrated a behavioral intervention could improve sleep in children with ADHD and that the intervention also reduced ADHD symptom severity and behavioral difficulties. Similarly, a pilot study showed promising results in the treatment of comorbid anxiety with cognitive behavioral therapy in children with ADHD, with potential flow on effects to ADHD symptoms and broader functioning (Sciberras et al., 2015).The self-reported data in this study show that these adolescents recognize that their inability to control their irritability is severely impacting their life. This may be an opportune time to provide intervention. Finally, further research is required to determine whether current programs aiming to improve behavioral functioning in children and adolescents can also reduce irritability or whether more tailored approaches are required.
Conclusion
Emotional dysregulation and irritable mood are common in children with ADHD. This study supports previous findings that irritability in children with ADHD is associated with a range of poorer outcomes. A novel aspect of this study was that we examined whether internalizing and/or externalizing problems predicted irritability in adolescence, where previous research has focused on the converse relationship. Our findings highlight the importance of assessing for and managing comorbidities and emotional regulation in children with ADHD, as externalizing problems predict ongoing irritability which, in turn, is associated with poorer functioning across a number of domains.
Footnotes
Acknowledgements
Thank you to the families, teachers and schools for their participation in this study and to the Sleeping Sound with ADHD and Attention to Sleep research teams. Some study data were collected and managed using REDCap electronic data capture tools hosted at MCRI. REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been funded through a philanthropic grant from the Cripps Foundation, through the Murdoch Childrens Research Institute (MCRI). N.Z. is funded by an Australian Postgraduate Award and a studentship. E.S. and F.M. are funded by Australian National Health and Medical Research Council (NHMRC) Early Career Fellowships in Population Health (#1037159 and #1037449). H.H. is funded by an NHMRC Career Development Award (#607351). MCRI is supported by the Victorian Government’s Operational Infrastructure Support Program.