
Abstract
Objective:
Prisoners are at increased risk of both self-harm and suicide compared with the general population, and the risk of suicide after release from prison is three times greater than for those still incarcerated. However, surprisingly little is known about the incidence of self-harm following release from prison. We aimed to determine the incidence of, identify risk factors for and characterise emergency department presentations resulting from self-harm in adults after release from prison.
Method:
Cohort study of 1325 adults interviewed prior to release from prison, linked prospectively with State correctional and emergency department records. Data from all emergency department presentations resulting from self-harm were secondarily coded to characterise these presentations. We used negative binomial regression to identify independent predictors of such presentations.
Results:
During 3192 person-years of follow-up (median 2.6 years per participant), there were 3755 emergency department presentations. In all, 83 (6.4%) participants presented due to self-harm, accounting for 165 (4.4%) presentations. The crude incidence rates of self-harm for males and females were 49.2 (95% confidence interval: [41.2, 58.7]) and 60.5 (95% confidence interval: [44.9, 81.6]) per 1000 person-years, respectively. Presenting due to self-harm was associated with being Indigenous (incidence rate ratio: 2.01; 95% confidence interval: [1.11, 3.62]), having a lifetime history of a mental disorder (incidence rate ratio: 2.13; 95% confidence interval: [1.19, 3.82]), having previously been hospitalised for psychiatric treatment (incidence rate ratio: 2.68; 95% confidence interval: [1.40, 5.14]) and having previously presented due to self-harm (incidence rate ratio: 3.91; 95% confidence interval: [1.85, 8.30]).
Conclusion:
Following release from prison, one in 15 ex-prisoners presented to an emergency department due to self-harm, within an average of 2.6 years of release. Demographic and mental health variables help to identify at-risk groups, and such presentations could provide opportunities for suicide prevention in this population. Transition from prison to the community is challenging, particularly for those with a history of mental disorder; mental health support during and after release may reduce the risk of adverse outcomes, including self-harm.
Introduction
Self-harm is a global health problem (World Health Organization [WHO], 1993) and is one of the strongest predictors of subsequent suicide (Bergen et al., 2012). Incidence rates are higher in marginalised populations including people with previously diagnosed psychiatric disorders (Portzky et al., 2008), Indigenous populations (Luke et al., 2013) and people with low levels of education (Skegg, 2005), all of whom are substantially over-represented in prison settings (Australian Institute of Health and Welfare [AIHW], 2013; Fazel and Danesh, 2002). Self-harm has been studied extensively in adult prisoners and there is considerable evidence that the incidence of both self-harm (Hawton et al., 2013) and suicide (Fazel et al., 2005, 2011) is higher in prisoners than in the general population. Adults recently released from prison experience high rates of mental health problems, subjective distress and frequent comorbid injecting drug use (AIHW, 2013), and the period following release from prison is characterised by an even higher risk of death by suicide (Binswanger et al., 2007; Kariminia et al., 2007; Pratt et al., 2006; Spittal et al., 2014). Yet, despite the strong association between self-harm and suicide, almost nothing is known about the incidence, correlates or predictors of self-harm in adults recently released from prison.
There is evidence that ex-prisoners present frequently to the emergency department (ED) for a variety of reasons including interpersonal violence, intoxication and drug overdoses (Frank et al., 2013; Meyer et al., 2012). However, there are no published data relating specifically to ED presentations resulting from self-harm in this population. Some general population studies in this area have actively excluded prisoners due to data protection issues (Drew et al., 2006). Increasing knowledge in this area may assist in the identification of those at particularly high risk of premature death, including due to suicide, following release from prison (Bergen et al., 2012). The primary aim of this study was to estimate, using linked data, the incidence of ED presentations resulting from self-harm in a representative sample of adults following release from prison in Queensland, Australia. Secondary aims were to identify factors predictive of ED presentations for self-harm and to characterise these presentations in terms of the method of self-harm and mental health service use during and after each ED presentation.
Materials and methods
Participants
Participants in this study were adult prisoners who were recruited into the Passports study (Kinner et al., 2013, in press), a randomised controlled trial of an intervention designed to increase health-care utilisation for adults following release from prison in Queensland, Australia. To be eligible for inclusion in the study, participants were required to be within 6 weeks of expected release from their index incarceration (the episode of incarceration during which they were first recruited to the study and interviewed) and able to provide written, informed consent. A total of 1976 prisoners were screened for eligibility, of whom 1665 met eligibility criteria and 1325 (79.6%) were recruited. Of these, 665 (50.2%) were randomised to receive the intervention and 660 (49.8%) were randomised to the control condition. The sample was formally compared to the population of interest, and with the exception of the intentional over-recruitment of female participants (to improve power for sex-stratified analyses), the cohort was representative of the population of people released from prisons in Queensland during the study period. Full details of the recruitment methodology and cohort characteristics are provided elsewhere (Kinner et al., 2013).
Data collection
Baseline data were collected during structured face-to-face interviews that covered participants’ demographic and criminogenic characteristics as well as, among other domains, physical and mental health, self-harm history, alcohol, tobacco and other drug use prior to and during incarceration, and other health-related risk behaviours.
Data linkage
We used probabilistic data linkage with clerical review to link baseline data with correctional records and ED records in Queensland. Linkage was enhanced by the inclusion of all known aliases for participants, obtained from correctional records; this process has been shown to improve sensitivity without adversely affecting specificity (Larney and Burns, 2011). The Queensland Health Data Linkage Unit linked records from the state-wide Emergency Department Information System with participant identities to identify all ED presentations in the cohort in Queensland from 1 June 2002 to 31 July 2012. Variables obtained for each ED presentation included International Classification of Diseases (ICD) diagnosis codes assigned to each presentation, the date and time of each ED arrival and departure, the triage category, departure destination and free text which was post-coded to increase ascertainment of presentations involving self-harm and of those involving suicide/self-harm ideation. Queensland Corrective Services provided information on dates of entry to and release from prison for the cohort from 1 September 2008 to 31 December 2013, using deterministic linkage based on participants’ unique prisoner identification number. Secondary outcome and exposure variables were obtained through probabilistic linkage with a state-wide hospital admitted patient data collection (covering the period 1 July 1999 to 31 July 2012) and a state-wide community mental health service database (covering the period 1 September 2008 to 31 July 2012).
Coding self-harm events
In order to improve ascertainment of self-harm events, free text fields in ED records for study participants were screened for self-harm using a coding system adapted from a recent large-scale epidemiological study of self-harm (Moran et al., 2012) (see Supplementary Appendix 1). All ED presentations were coded as either ‘0 = Did not involve self-harm’ or ‘1 = Involved self-harm’, with the latter category comprising all ED presentations resulting from behaviours fitting into any one of five categories: (1) cutting/burning, (2) self-poisoning, (3) self-battering, (4) risk-taking or (5) other self-harm. In all, 10% of ED presentations were coded independently by two members of the research team (K.M. and R.B.), and based on the high level of agreement between raters (kappa = 0.96 for self-harm, kappa = 0.96 for self-harm/suicide ideation), the remaining records were coded by a single team member (K.M.).
Exposures
Exposure variables were derived from the baseline interview and measured by self-report unless otherwise stated. Demographic variables included age, sex, Indigenous status (Aboriginal or Torres Strait Islander vs other), relationship status (married or in a de facto relationship vs other), education (<10 years of education vs ⩾10 years of education) and sexuality (lesbian, gay, bisexual or transgender [LGBT] vs heterosexual). We manually coded the most serious offence pertaining to the participant’s index incarceration (linked from correctional records) as violent (including sex offences) or non-violent, using the Australian Standard Offence Classification (Queensland Supplement) (Office of Economic and Statistical Research [OESR], 2008). Mental health variables included a history of self-harm, attempted suicide, previous hospitalisation for psychiatric treatment and any previous ED presentations resulting from self-harm. Lifetime history of diagnosed mental illness was assessed by self-report using a question adapted from Australia’s National Health Survey (Australian Bureau of Statistics [ABS], 2008): participants were asked whether they had ever been told by a doctor, psychologist or psychiatrist that they had a mental illness.
Measures
The primary outcome was the number of presentations to any ED in Queensland resulting from self-harm after release from prison for their index incarceration. We considered only those ED presentations that occurred while the participant was residing in the community (i.e. not during a period of re-incarceration). We also investigated the following outcomes: the method of self-harm (as described in Supplementary Appendix 1), time of day of ED presentation, duration of stay in the ED (computed as the difference between time of arrival and time of departure from the ED) and length of time between release from prison and ED presentation. We also examined mental health service use during and after each ED presentation. This included referral to mental health services by ED staff, admission to hospital for psychiatric treatment within 2 days of the date of departure from the ED and use of public community mental health services during the ED stay and within 30 days of the date of departure from the ED. We excluded community mental health records in which the participant had no direct contact with a clinician or other employee, as some of these records denote administrative or other activities related to the client’s care but not directly involving the client.
Ethics and governance approvals
Ethics approval for the study was granted by The University of Queensland’s Behavioural and Social Sciences Ethical Review Committee (#2007000607) and the Queensland Department of Health Human Research Ethics Committee. All participants provided written informed consent prior to entering the study.
Statistical analyses
We first compared the demographic and criminogenic characteristics of participants who presented to the ED for any reason at least once during follow-up with those who did not present, performing chi-squared tests for differences in proportions. We used survival analysis to generate Kaplan–Meier plots and computed time to first ED presentation for self-harm and the crude incidence rate per 1000 person-years of such presentations according to baseline characteristics. Next, we estimated unadjusted incidence rate ratios (IRRs) for ED presentations resulting from self-harm using a univariate negative binomial regression model for each exposure variable. We then computed adjusted IRRs using a multivariate model that included all exposure variables. As we excluded ED presentations that occurred during periods of re-incarceration from the analyses, we used person-time in the community (follow-up time minus duration of any periods of re-incarceration) as the denominator when calculating crude and multivariate incidence rates. Finally, we calculated simple proportions describing the secondary outcome measures, using individual self-harm ED presentations as the unit of analysis. All analyses were performed using Stata version 13.1.
Results
Linked health records were obtained for 1315 (99.2%) participants, 1307 (98.6%) of whom were also linked to correctional records; all subsequent analyses were conducted on these 1307 participants. The median duration of community follow-up was 2.6 years per participant (interquartile range [IQR]: 2.0–3.1 years), for a total analysis time of 3192 person-years. Table 1 shows the number of participants who presented to the ED after release from index incarceration, disaggregated by whether the participant was residing in the community or prison and reason for presentation (all cause, self-harm ideation and/or actual self-harm). The crude incidence rate of ED presentations in the community for any reason was 1095 per 1000 person-years, compared with 212 per 1000 person-years in the general population during the same period (AIHW, 2012). A total of 885 (67.7%) participants made 3755 unique ED presentations following release from prison for their index incarceration. Among those who presented to the ED at least once, the median number of presentations was 3 (IQR = 1–5). Those who presented to the ED were more likely to be female, aged 18–39 years, LGBT, have had less than 10 years of formal education and have committed a violent offence.
Emergency department presentations following release from index incarceration.
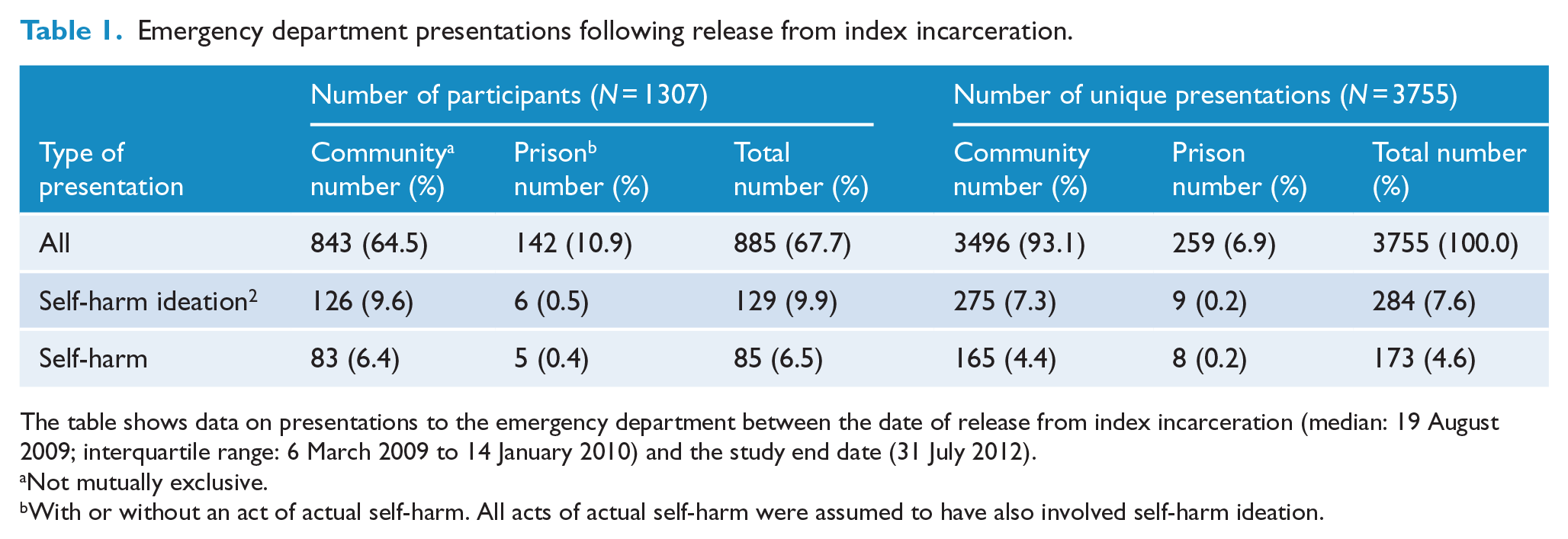
The table shows data on presentations to the emergency department between the date of release from index incarceration (median: 19 August 2009; interquartile range: 6 March 2009 to 14 January 2010) and the study end date (31 July 2012).
Not mutually exclusive.
With or without an act of actual self-harm. All acts of actual self-harm were assumed to have also involved self-harm ideation.
In all, 83 (6.4%) participants presented to the ED due to self-harm at least once during community follow-up, with 35 (2.7%) doing so within 1 year of release from their index incarceration (see Figure 1). A total of 165 (4.4%) ED presentations resulted from self-harm. There was no difference in the proportion of participants presenting to the ED due to self-harm between the intervention (42; 6.4%) and control (41; 6.3%) arms of the trial (χ2(1) = 0.01, p = 0.92). We therefore omitted the intervention variable from subsequent analyses to preserve statistical power.
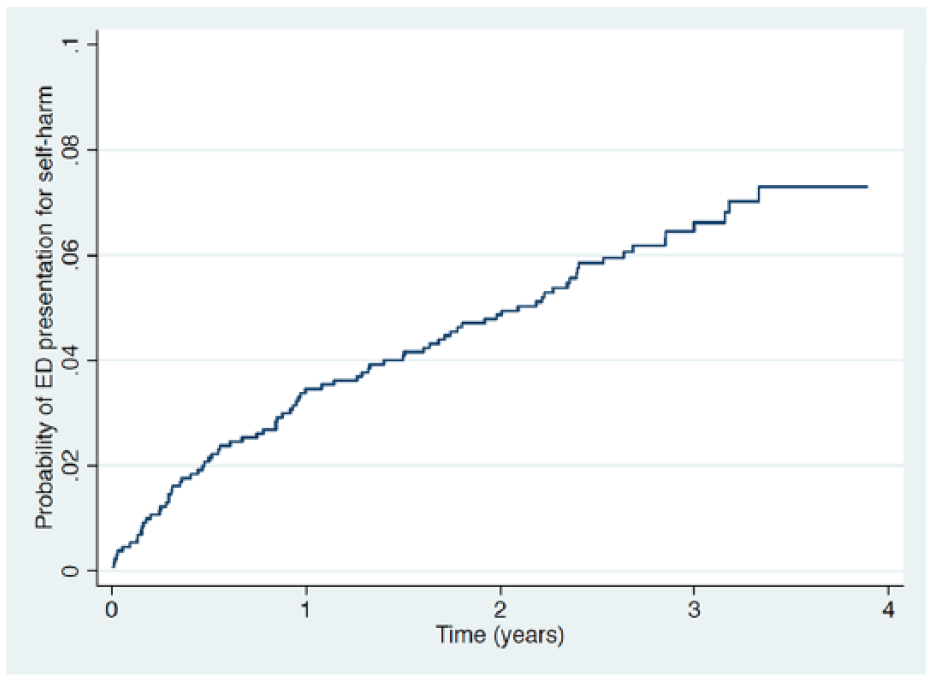
Probability of participants presenting to an emergency department for self-harm after release from prison.
Among the 83 participants who presented to the ED for self-harm, 8 (10%) first did so within 90 days of release and 27 (33%) first presented between 91 and 365 days after release. The remaining 48 (58%) participants first presented more than 1 year after release. In all, 49 (59%) presented on one occasion only, 20 (24%) presented twice and 14 (17%) presented three or more times. The maximum number of presentations for self-harm was 14, by one participant. Table 2 describes the baseline characteristics of participants and shows the number and rate of ED presentations resulting from self-harm according to these characteristics. The crude incidence rate of ED presentations for self-harm was 60.5 per 1000 person-years for females and 49.2 per 1000 person-years for males. In all, 32 (39%) ED presenters reported a history of self-harm at baseline interview, compared with 150 (12%) non-presenters (χ2(1) = 44.9, p < 0.001). Totally, 41 (49%) ED presenters reported a previous suicide attempt, compared with 236 (19%) non-presenters (χ2(1) = 42.2, p < 0.001). Just under half of participants who presented for self-harm following release from prison (48%) had been identified by prison staff as being at risk of self-harm in their correctional records.
Baseline characteristics of participants and number of ED presentations for self-harm (N = 1307).
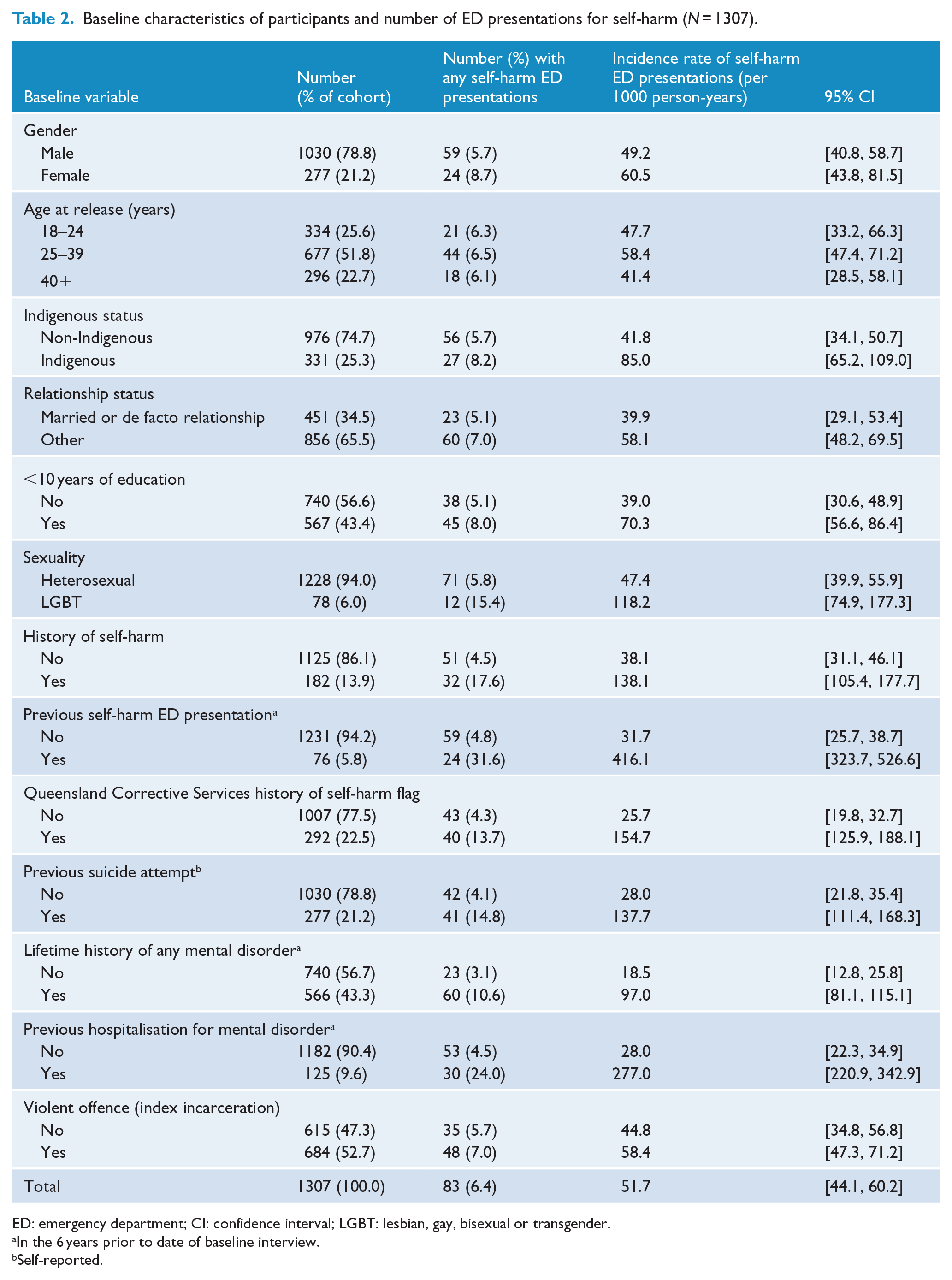
ED: emergency department; CI: confidence interval; LGBT: lesbian, gay, bisexual or transgender.
In the 6 years prior to date of baseline interview.
Self-reported.
Table 3 presents associations between exposure variables measured prior to release from index incarceration and the number of ED presentations resulting from self-harm after release. In adjusted analyses controlling for all other exposure variables, independent predictors of self-harm ED presentations included identifying as Indigenous, having been flagged by corrective services as being at risk of self-harm, having a history of mental illness, having a history of ED presentation due to self-harm and having previously been admitted to a hospital for psychiatric treatment.
Associations between baseline characteristics and ED presentations for self-harm (N = 1307).
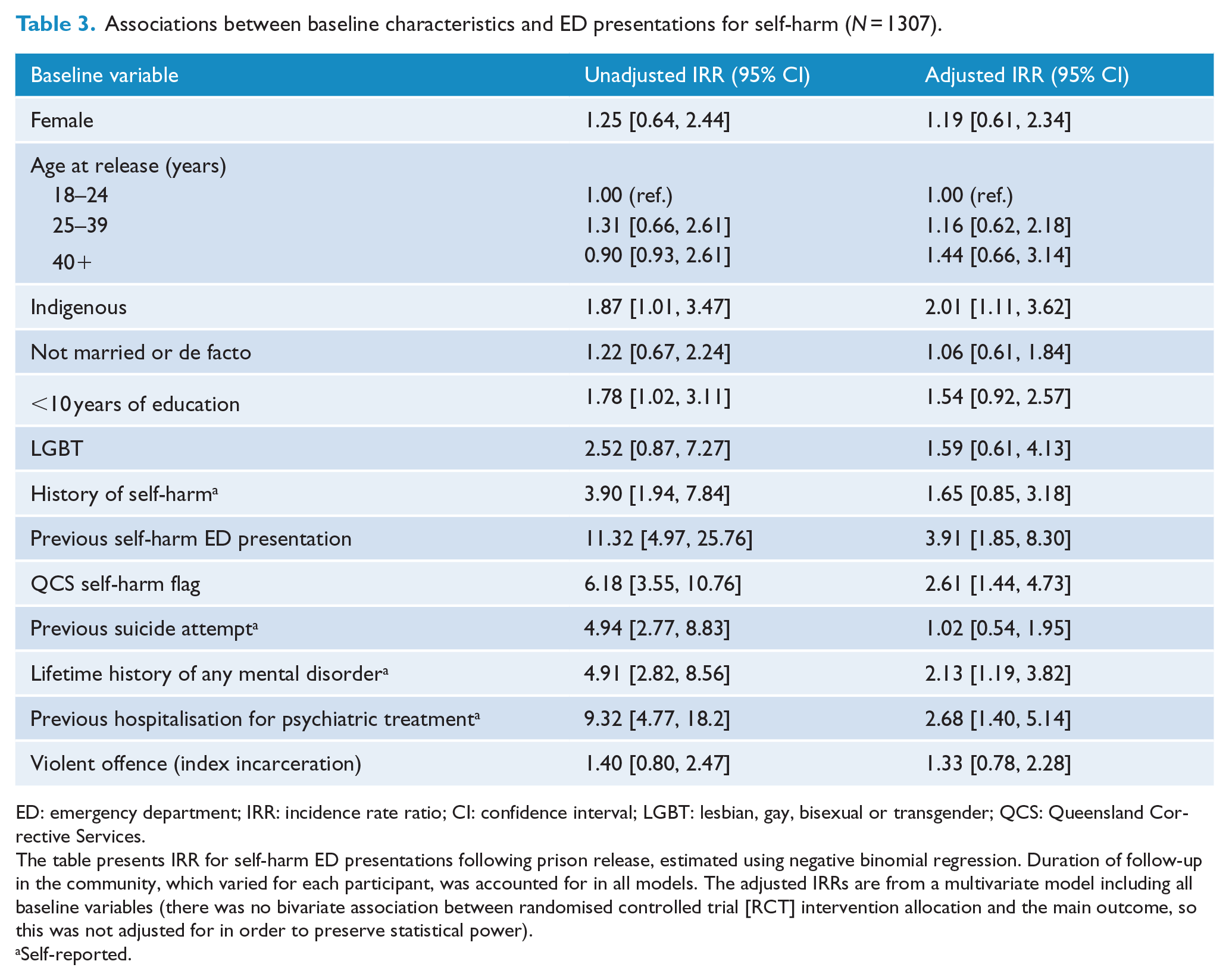
ED: emergency department; IRR: incidence rate ratio; CI: confidence interval; LGBT: lesbian, gay, bisexual or transgender; QCS: Queensland Corrective Services.
The table presents IRR for self-harm ED presentations following prison release, estimated using negative binomial regression. Duration of follow-up in the community, which varied for each participant, was accounted for in all models. The adjusted IRRs are from a multivariate model including all baseline variables (there was no bivariate association between randomised controlled trial [RCT] intervention allocation and the main outcome, so this was not adjusted for in order to preserve statistical power).
Self-reported.
Subsequent outcomes during and after ED presentations for self-harm
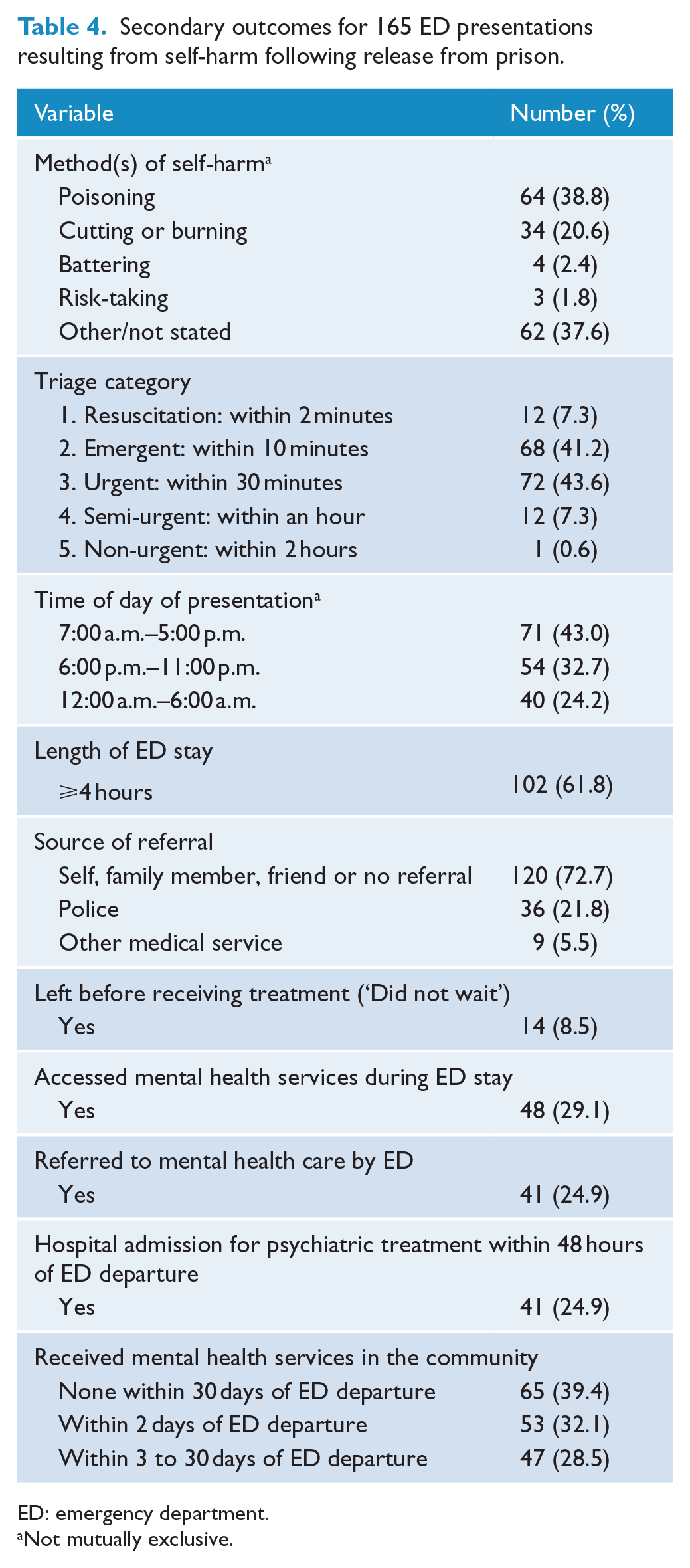
Table 4 describes contextual factors and mental health service use during and after ED presentations resulting from self-harm in the community. The most common method of self-harm recorded was poisoning and the highest proportion of presentations occurred between the hours of 7:00 a.m. and 5:00 p.m. In 65 (39.4%) self-harm ED presentations, participants had no contact with public mental health services either during their ED visit or within 30 days afterwards.
Secondary outcomes for 165 ED presentations resulting from self-harm following release from prison.
ED: emergency department.
Not mutually exclusive.
Discussion
In this study, we sought to estimate the incidence and identify predictors of ED presentations resulting from self-harm in a representative sample of adults following release from prison, and to characterise these presentations in terms of the method of self-harm used and rates of mental health service access after discharge from the ED. We found that about one in 40 participants presented to the ED as a result of self-harm within 1 year of release from prison and one in 15 presented for self-harm during follow-up. Self-harm was responsible for less than 5% of all ED presentations, yet this proportion was more than 10 times greater than that which has been reported in the general population (Drew et al., 2006). The incidence rate in our cohort was higher in women than in men and considerably higher in those with a prior history of self-harm or hospital treatment for a mental disorder. The most commonly recorded method of self-harm was poisoning, which is in line with findings from previous studies examining ED use in the general population (Centers for Disease Control and Prevention [CDC], 2001; Doshi et al., 2005). This suggests that the profile of self-harm among ex-prisoners may be comparable to that of the general population, although the incidence of such events is considerably higher in ex-prisoners. Interestingly, no spike in the incidence of ED presentations for self-harm was observed shortly after release from prison; instead, there was a relatively stable pattern of presentations over the first 12 months post-release. This suggests that presenting to the ED due to self-harm may be related less to the experience of being released from prison, or indeed the interface between prison and the community, and related more to the specific characteristics of this population or the circumstances in which they find themselves after release from prison.
There was no difference in the incidence of self-harm presentations between participants in the intervention and control groups of the original Passports trial. The aim of the trial was to increase access to health services, and it seems plausible that more contact with health services may have resulted in reduced rates of self-harm. However, few interventions have been shown to reduce self-harm (Dialectical Behaviour Therapy [Linehan et al., 1991, 2006] being one exception, although this intervention is specific to people with borderline personality disorder), and studies demonstrating a beneficial impact of increased health service contact on rates of self-harm are scarce. Contact with services may be a necessary but not sufficient condition for reducing self-harm in this population.
After adjusting for potential confounders, ED self-harm presentations were associated with being Indigenous, having a lifetime history of a mental disorder, having previously attended the ED due to self-harm, having previously been hospitalised for psychiatric treatment and having been identified by prison staff as being at risk of self-harm. Most presentations were between the hours of 7:00 a.m. and 5:00 p.m., and one in every 11 participants left the ED before receiving treatment, a proportion which was almost double that recorded in Australia in 2011–2012 (9% vs 5%) (AIHW, 2012). While patients who leave an ED without receiving treatment may not necessarily be at increased acute risk of mortality (Guttmann et al., 2011), patients who present to the ED following self-harm are already at considerably higher risk of further self-harm and eventual suicide (Crandall et al., 2006). This risk may be exacerbated further by not receiving timely medical and/or psychiatric treatment (Hickey et al., 2001).
Contact with mental health services
The high prevalence of psychiatric and substance use disorders in this population suggests that these issues should be considered during ED presentations and subsequent referrals (Doshi et al., 2005). However, in our study, fewer than 3 in 10 participants (29%) who presented to the ED due to self-harm received a mental health assessment. Despite being consistent with previous research (Hickey et al., 2001), this finding is extremely concerning as it is contrary to Australian national guidelines (Boyce et al., 2003). The Royal Australian and New Zealand College of Psychiatrists (RANZCP) states that patients presenting to the ED with evidence of self-harm should receive a comprehensive psychiatric assessment and that, where possible, this should take place in the ED (Boyce et al., 2003). The incidence of self-harm in the year following an initial ED presentation due to self-harm is significantly higher among those who do not receive such an assessment compared with those who do (Hickey et al., 2001; Shahid et al., 2009), further increasing both individual risk and health-care costs. Importantly, this suggests that it may already be ‘too late’ once an individual presents to the ED following self-harm, as these individuals should already have received mental health care following their release from prison. This is especially pertinent in light of our finding that those who presented to the ED following self-harm had elevated rates of mental disorder and that many had presented to the ED in the past following self-harm. Future studies examining the potential protective effects of mental health service contact prior to presenting to the ED for self-harm would further increase our understanding of this issue.
Strengths and limitations
Our study had several important strengths. First, these are the first published data examining self-harm in a sample of adults following release from prison internationally. Second, and unlike previous studies in which self-harm was measured exclusively by self-report, we used prospective ED data to capture self-harm events and, as such, had almost zero attrition. Third, our sample was large and broadly representative of adults being released from prison in Queensland across the study duration on a range of demographic and criminogenic variables (Kinner et al., 2013). Fourth, extensive data linkage combining survey responses with multiple administrative datasets allowed us to examine participants’ access to mental health services during and after discharge from the ED. Finally, we had access to state-wide data, and it is therefore likely that we captured a very high proportion of ED presentations (Spilsbury et al., 2015).
Our study also had some limitations. First, it is possible that eligible non-participants (i.e. those prisoners who declined to take part in the Passports trial) may have differed significantly on key demographic or outcome measures from those who chose to participate, and this may have impacted on the results obtained. Previous studies have reported that non-participants in health-related trials are more likely to be of lower socioeconomic status (i.e. worse living conditions, lower educational level and poorer employment status) (Drivsholm et al., 2006), to have a lower level of functioning (as measured by global assessment of functioning scores) (Rentrop et al., 2010), to have increased rates of substance misuse (Mansson et al., 1994) and to have poorer general physical (Bisgard et al., 1994) and mental (Haapea et al., 2008; Hansen et al., 2001) health than participants. It is therefore possible that potential participants who declined to be involved in the trial may have had poorer overall outcomes – including elevated rates of self-harming behaviour – than study participants. To the extent that this is the case, we would have under-estimated the incidence of self-harm in this population.
Second, it is possible that some participants may have presented to an ED as a result of self-harm outside of Queensland, and due to our data collection methods, such presentations would not have been captured. However, additional linked data relating to study participants indicate that fewer than 5% accessed health services solely outside of Queensland (mirroring recent research; Spilsbury et al., 2015), and as such, the number of ED presentations due to self-harm outside of Queensland is likely to be small. Third, it is possible that participants may have presented to a non-emergency health-care service or a primary or private health-care service only, leading to under-estimation of self-harm events. Fourth, participants who presented to the ED after self-harm and were correctly coded as such may have differed systematically according to their baseline characteristics from those who were incorrectly coded. This could have resulted in misclassification bias in our examination of baseline predictors of self-harm or selection bias in our descriptive analysis of contextual factors and mental health service use following individual self-harm ED presentations. Fifth, due to our data collection methods, we did not have access to private mental health-care data which may have been relevant to our findings. Finally, due to our data collection methods, we were unable to comment on the reasons why participants engaged in self-harm or on the possible links between self-harm, substance use and intoxication.
Clinical implications
The incidence rate of ED presentations for any reason in our sample was more than five times higher than that of the Queensland population during the same period (AIHW, 2012), a finding which is in line with previous research indicating that ex-prisoners represent a group with disproportionately high ED use (Frank et al., 2013; Meyer et al., 2012). Given this high presentation rate, it might be feasible to initiate a critical time intervention (CTI) for self-harm in ex-prisoners in the ED. CTIs have been shown to be feasible and potentially effective in preventing homelessness among mentally ill populations (Herman et al., 2011), and they may also improve continuity of care for recently released prisoners with mental health problems (Jarrett et al., 2012). On a similar note, almost half (48%) of participants who presented for self-harm following release from prison had been identified by a prison health staff member as being at risk of engaging in future self-harm. This also suggests that potentially valuable self-harm reduction strategies might be implemented while the individual is still in prison and/or at the point of release. Such interventions would need to explicitly focus on enhancing the support available during the vulnerable transitional period from prison to the community.
These are the first published data regarding self-harm in a sample of adults following release from prison. Ex-prisoners are a particularly challenging population to engage and retain in research, and the disclosure of self-harm remains highly stigmatising. It is perhaps for these reasons that, until now, little has been known about the incidence of self-harm following release from prison. Our study sheds important new light on this problem and demonstrates that, following release from prison, one in 15 ex-prisoners presents to the ED following episodes of self-harm. Such presentations could provide pivotal opportunities for suicide prevention in this population.
Footnotes
Acknowledgements
The authors wish to thank Queensland Corrective Services for assistance with data collection and Passports study participants for sharing their experiences. The authors also wish to thank Ms Katherine Mok (K.M.) for her assistance with data coding.
Declaration of Conflicting Interests
The views expressed herein are solely those of the authors and in no way reflect the views or policies of Queensland Corrective Services.
Funding
The Passports study was funded through an Australian National Health and Medical Research Council (NHMRC) Strategic Award (#409966) and Project Grant (#1002463). Rohan Borschmann is supported by an NHMRC Early Career Fellowship (#1104644). Stuart Kinner is supported by an NHMRC Senior Research Fellowship (#1078168).