
Abstract
Background and Aims:
Our understanding of patient pathways through specialist Alcohol and Other Drug treatment and broader health/welfare systems in Australia remains limited. This study examines how treatment outcomes are influenced by continuity in specialist Alcohol and Other Drug treatment, engagement with community services and mutual aid, and explores differences between clients who present with a primary alcohol problem relative to those presenting with a primary drug issue.
Method:
In a prospective, multi-site treatment outcome study, 796 clients from 21 Alcohol and Other Drug services in Victoria and Western Australia completed a baseline interview between January 2012 and January 2013. A total of 555 (70%) completed a follow-up assessment of subsequent service use and Alcohol and Other Drug use outcomes 12-months later.
Results:
Just over half of the participants (52.0%) showed reliable reductions in use of, or abstinence from, their primary drug of concern. This was highest among clients with meth/amphetamine (66%) as their primary drug of concern and lowest among clients with alcohol as their primary drug of concern (47%), with 31% achieving abstinence from all drugs of concern. Continuity of specialist Alcohol and Other Drug care was associated with higher rates of abstinence than fragmented Alcohol and Other Drug care. Different predictors of treatment success emerged for clients with a primary drug problem as compared to those with a primary alcohol problem; mutual aid attendance (odds ratio = 2.5) and community service engagement (odds ratio = 2.0) for clients with alcohol as the primary drug of concern, and completion of the index treatment (odds ratio = 2.8) and continuity in Alcohol and Other Drug care (odds ratio = 1.8) when drugs were the primary drugs of concern.
Conclusion:
This is the first multi-site Australian study to include treatment outcomes for alcohol and cannabis users, who represent 70% of treatment seekers in Alcohol and Other Drug services. Results suggest a substantial proportion of clients respond positively to treatment, but that clients with alcohol as their primary drug problem may require different treatment pathways, compared to those with illicit drug issues, to maximise outcomes.
Introduction
Data from the 2007 National Survey of Mental Health and Wellbeing indicate that 22.1% of Australians meet lifetime criteria for alcohol use disorders (Teesson et al., 2010), with 7.5% meeting lifetime criteria for illicit drug use disorders (Australian Bureau of Statistics [ABS], 2007). Importantly, an increasing international evidence base on the effectiveness of specialist Alcohol and Other Drug (AOD) treatment has emerged over the past three decades, including large multi-site outcome studies such as Project Matching Alcoholism Treatments to Client Heterogeneity (MATCH) (Project MATCH Research Group, 1997) and Combined Pharmacotherapies and Behavioural Interventions for Alcohol Dependence (COMBINE) (Pettinati et al., 1996) in the United States and National Treatment Outcomes Research Study (NTORS) (Gossop et al., 2000), Drug Treatment Outcome Research Study (DTORS) (Donmall et al., 2009), Drug Outcome Research in Scotland (DORIS) (McKeganey et al., 2008) and United Kingdom Alcohol Treatment Trial (UKATT) (UKATT Research Team, 2005) in the United Kingdom. Nevertheless, our understanding of pathways through the treatment system, and the cumulative impact of engaging with specialist AOD and non-AOD community services on treatment outcomes remains limited.
To date, there have only been two multi-site treatment outcomes studies conducted in Australia, both focussing on people who use illicit drugs. The first, the Australian Treatment Outcomes Study (ATOS), was a longitudinal study examining 825 heroin users in New South Wales, South Australia and Victoria attending Opiate Substitution Treatment (OST), Residential Rehabilitation (RR) and detoxification services, as well as 80 non-treatment needle-exchange consumers. Participant outcomes were assessed at 3, 12, 24 and 36 months and 11 years (Teesson et al., 2006, 2008, 2015). Key findings at 12-months were that 52% of detoxification, 63% of RR and 65% of OST clients reported past-month abstinence from heroin (14% continuous abstinence) with significant reductions in criminal behaviours, psychopathology, intravenous-related and physical health problems (Teesson et al., 2006).
The second major Australian study, ‘Methamphetamine Treatment Evaluation Study (MATES)’, examined 360 meth/amphetamine users in community-based detoxification or RR and 101 non-treatment quasi-controls. The study was conducted in Sydney and Brisbane with 3-, 12- and 36-month follow-ups. Continuous abstinence from methamphetamine was reported by 33% more among residential rehabilitation clients relative to the those receiving detoxification only or no treatment at 3 months but fell to just 14% more at the 1-year follow-up and 6% more at 3 years (McKetin et al., 2012).
Both ATOS and MATES highlight the complexity and severity of individuals presenting for specialist AOD treatment (e.g. drug dependence, poor psychological health), as well as the substantial improvement observed across multiple clinical and psychosocial domains following treatment. While desired outcomes from these two studies were associated with longer and more intensive treatment modalities (i.e. residential rehabilitation), cumulative time spent in multiple modalities (which could reflect periods of engagement, drop-out and re-engagement) was not. Research suggests outcomes are generally improved when there is continuity of care to address AOD problems across treatment types (e.g. ongoing support from counselling services following inpatient detoxification) (McLellan et al., 2000). There is increasing recognition that, like other chronic health problems (e.g. diabetes, asthma, schizophrenia), substance use disorders are best managed through continuing care models, involving ongoing monitoring and coordination between different services, rather than by an acute episodic treatment approach (Dennis and Scott, 2007; McKay et al., 2009; McLellan et al., 2000). Continuing care models have also been shown to be more cost-effective than acute treatment episodes (Popovici et al., 2008). The continuing care model in the United States, which involves general practitioner (GP) visits, ongoing AOD specialist treatment and support from psychiatric services (where needed) has been associated with positive substance use outcomes up to 9 years later (Chi et al., 2011; Chi and Weisner, 2008). Case management and active referral between AOD services are therefore likely to improve outcomes, but as identified in a recent systematic review, few high-quality studies on continuity of care exist (Lenaerts et al., 2014). The benefits of continuing care with Australian treatment seekers and how these vary by a client’s primary drug of concern (PDOC) have not previously been examined.
Treatment outcome research (predominantly US and UK studies) has focussed primarily on responses to isolated treatments or modalities (e.g. inpatient detoxification). These typically represent just one component of an individual’s care, which may include multiple modalities of treatment within AOD services (e.g. detoxification, counselling), with specialist AOD services being one component of a broader system that can include health, social and welfare services. Included in this broader system are informal sources of support that can contribute to the treatment journey such as mutual aid (e.g. 12-step programmes such as Alcoholics Anonymous and Narcotics Anonymous, or Self-Management And Recovery Training (SMART) Recovery). While there is evidence that mutual aid is associated with improved outcomes for clients with AOD issues (Kaskutas, 2009), its contribution to treatment success has received little attention in Australian treatment cohort studies. Consequently, the level of inter- and intra-sectorial integration, pathways of care and their relationship to outcomes remain poorly understood, despite recognition of the merits in adopting a broader systems perspective when examining the benefits of treatment (Babor et al., 2008). Understanding the combinations of service use and pathways of care to address clients’ multiple and disparate needs, and associated AOD outcomes, can inform the configuration of an effective treatment system.
Prior Australian treatment outcome research is limited to heroin and methamphetamine using cohorts. Problematic alcohol and cannabis users, however, represent 70% of all publicly funded treatment episodes in Australia (Australian Institute of Health and Welfare [AIHW], 2014), and it is essential that future AOD treatment outcome research incorporates these populations. Furthermore, few studies consider outcomes across substance types or in relation to poly-substance use which is common among treatment seekers (AIHW, 2014). The aim of this study was to examine substance use outcomes among clients attending AOD services in Victoria and Western Australia (WA), and to examine factors associated with these outcomes, including the PDOC, type and nature of AOD service use, other forms of service use and mutual aid engagement (i.e. the treatment pathway). The substance use outcomes of interest were: (1) treatment success – defined as a reliable reduction in the frequency of use/ abstinence from the PDOC, and (2) abstinence from all drugs of concern (DOCs). Specific research questions were: (1) Do outcomes differ between clients with a primary alcohol versus primary drug problem? (2) Are outcomes improved with continuity in specialist AOD treatment (i.e. referral to other AOD services)? (3) Are outcomes improved with engagement with non-AOD community services and mutual aid? And finally, (4) to what extent do treatment pathways that achieve positive outcomes differ between clients with a primary drug and alcohol problem?
Method
Design and procedure
The study was a prospective, multi-site treatment outcome study. Participants were recruited via clinicians from 21 different AOD specialist services across 37 different sites in Victoria and Western Australia (WA) between January 2012 and January 2013. In total, 1054 clients were referred to the study for screening, of whom 796 (75.5%) met inclusion criteria, provided written informed consent, and completed the baseline interview (see Figure 1). Inclusion criteria were: aged 18 and above, commencing a new treatment episode (primary index treatment [PIT]) within the previous month, and not having engaged in the same type of treatment in the three weeks prior to commencing the current treatment episode. Further details on baseline characteristics of the cohort and methodology of recruitment can be found in Lubman et al. (2014). The outcomes for 73% (585/796) of the sample were ascertained: 555 (70%) participants were successfully re-interviewed over the telephone approximately 12-months later (11 were deceased and 19 were incarcerated; see Figure 1). Ethics approval was provided by Eastern Health Research and Ethics Committee; E17/1112, Monash University Human Research Ethics Committee (201200020) and Curtin University (HR11/2012).
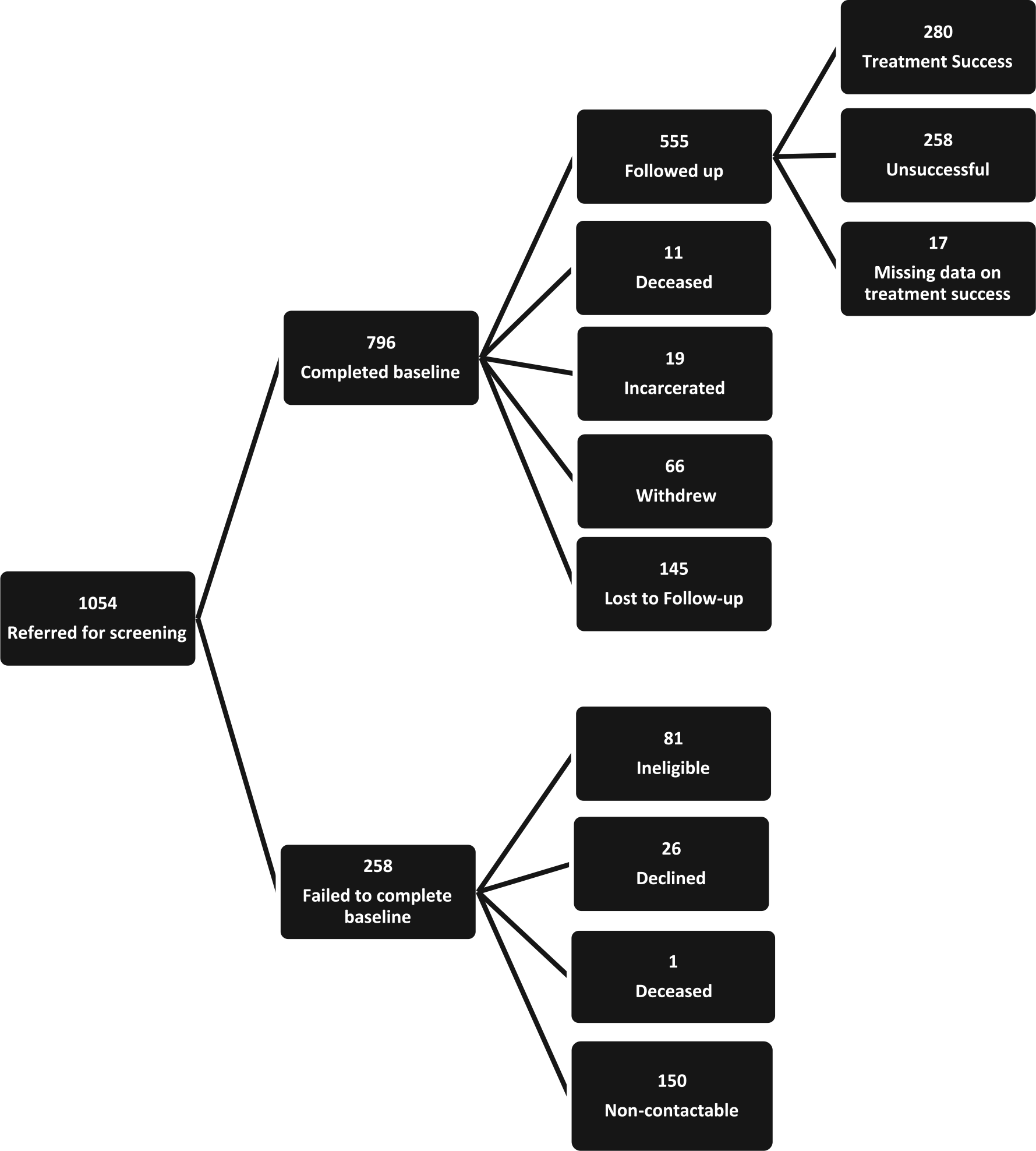
Participant flow through the study.
Sample
The baseline sample (n = 796) comprised 29 (4%) who had completed a comprehensive assessment, 146 (18%) receiving individual counselling, 24 (3%) receiving group counselling, 346 (43%) undergoing inpatient withdrawal, six (1%) undergoing home-based withdrawal treatment, 230 (29%) in long-term residential treatment such as residential rehabilitation or therapeutic communities and 15 (2%) commencing pharmacotherapy treatment. For the purpose of analyses, these treatment types were grouped into three PIT categories; 352 (44%) acute withdrawal (AW) (inpatient or home-based withdrawal), 214 (27%) outpatient services (OPS) (assessment, individual or group counselling and pharmacotherapy) and 230 (29%) long-term residential (RR) (e.g. residential rehabilitation, and therapeutic communities).
Measures
Participants completed a comprehensive interview at baseline and again at follow-up, using standardised instruments validated on Australian populations where available. The interview captured (1) demographic characteristics, (2) pattern of substance use, including frequency of use of all licit and illicit substances in the past 30 days using the ASSIST (WHO ASSIST Working Group, 2002) as well as primary and secondary DOCs, (3) problem severity using the Severity of Dependence Scale (SDS) (Gossop et al., 1995), (4) all service utilisation in the previous 12-months categorised using an adapted form of the Lifetime Drug Use History (LDUH) tool (Day et al., 2008), which examined: further specialist AOD (RR, OPS, AW); mutual aid (e.g. 12-step and SMART recovery); General Practitioner (GP) visits; acute health services (ambulance; hospital emergency departments [ED]; hospital inpatient services); and other community health/social/welfare services (including mental health services, legal aid, financial counselling, employment services, family/relationship counselling and housing). The tool was developed specifically to record number of visits and referral source for use of that service. Further (post-PIT) AOD service use was categorised as either ‘continuity of care’ (defined as further participation in post-PIT AOD treatment to which the participant was referred by the PIT or other AOD service, to reflect the process of active referral between AOD services that is considered a core component of the continuing care model) or ‘fragmented care’ (further AOD service attendance post-PIT, but without any referral from another AOD service). Treatment satisfaction was assessed using the Client Satisfaction Questionnaire (CSQ)-8 UK (Nguyen et al., 1983), a standardised measure of treatment satisfaction.
Following the National Institute on Drug Abuse consensus panel recommendations that either abstinence or reductions in frequency of use can represent clinically meaningful substance abuse treatment outcomes (Donovan et al., 2012), our primary outcome was achieving either a reliable reduction in the frequency (days) of PDOC use in the month prior to interview or abstinence from that PDOC. To address the issue of poly-substance use and the fact that the majority of the sample (61% for alcohol and 76% for drugs) had abstinence as their treatment goal, the secondary outcome of interest was abstinence from all DOCs.
Analyses
Distributions of continuous variables subject to between-group and/or repeated measures analyses (age, SDS score, CSQ-8 score) departed significantly from normality (Kolmogorov-Smirnov p < 0.001). Comparisons of baseline age and SDS score between those who were and were not followed up, and comparisons of CSQ-8 scores between those who did and did not complete their PIT, were therefore analysed with Mann–Whitney U tests. Between-group comparisons of categorical variables were conducted with Pearson χ2 tests, while changes in category sizes between baseline and follow-up were analysed with McNemar tests.
Reliable change criteria (RCC) for days of use of the PDOC were calculated using the Jacobson and Truax (1991) formula, in which the reliability of a measure and the standard deviation of the distribution of its scores at baseline is used to calculate the magnitude of change in an individual’s score that would be less than 5% likely to occur by chance in the absence of real change in the underlying construct. We used the intra-class correlation (ICC) values reported for inter-rater reliability of the near-identical days of use measures from the Australian Treatment Outcomes Profile reported by Ryan et al. (2014) for each PDOC, generating RCC for reduced frequency of use (days).
Logistic regression models were used to examine predictors of outcomes. To determine demographic and social disadvantage indicators to be controlled for in the final model, we first analysed a model predicting the primary outcome with only demographic and social disadvantage variables (age, gender, state of residence, being married or in a de facto relationship, on unemployment benefits, recent homelessness and education) entered as predictors. Since age was the only statistically significant predictor, it was added to the final model which also included substance use and treatment process variables (PIT type, PIT completed, continuity in AOD treatment [i.e. having an additional episode of AOD service use, following or concurrent with the PIT, to which the participant was referred to by the PIT or another AOD service], PDOC, use of community services [other than GP] and mutual aid attendance), while controlling for the interval between baseline and follow-up as predictors of outcomes. Additional univariate logistic regression models were tested in participants who engaged in mutual aid during the follow-up interval to examine associations between number of meetings attended and treatment success. All analyses were conducted using SPSS 22.0.
Results
Baseline characteristics
This paper describes the baseline characteristics and outcomes of the 555 participants successfully followed up (see Lubman et al. (2014) for a detailed description of the total cohort). At baseline, the most common PDOC was alcohol (49.4%), followed by meth/amphetamine (16.6%), opioids (15.9%), cannabis (15.3%) and other drugs (2.9%), with 51.7% of participants nominating at least one secondary drug of concern (SDOC). The sample was predominantly male, Australian-born and had a median age of 37.3 years (see Table 1 for a summary of demographics). Marginalisation and disability were common, with the majority neither in paid employment nor a stable relationship and with chronic medical conditions. The median drug dependence score on the SDS for their PDOC was 11, with 98.4% falling in the ‘probable dependence’ range (scoring >2) and 87.0% in the severely dependent range (scoring >6). As shown in Table 1, those with alcohol as their PDOC were older, more likely to be foreign-born and have an educational qualification, but were less likely to be male, to have SDOCs, to be receiving welfare benefits, to have experienced recent homelessness and to be experiencing legal problems than those with other PDOCs. The mean time between baseline and follow-up interviews was 380.3 (±71.8) days. Participants lost to follow-up were significantly younger (p < 0.001), more likely to have experienced recent (past 90 days) homelessness prior to intake (p < 0.01), be involved in the criminal justice system (p < 0.001) and have meth/amphetamine as the PDOC (p < 0.01), and were less likely to have been suffering a chronic medical condition (p < 0.05), relative to those successfully re-interviewed.
Baseline demographic and substance use characteristics of participants who completed follow-up assessment (N = 555).
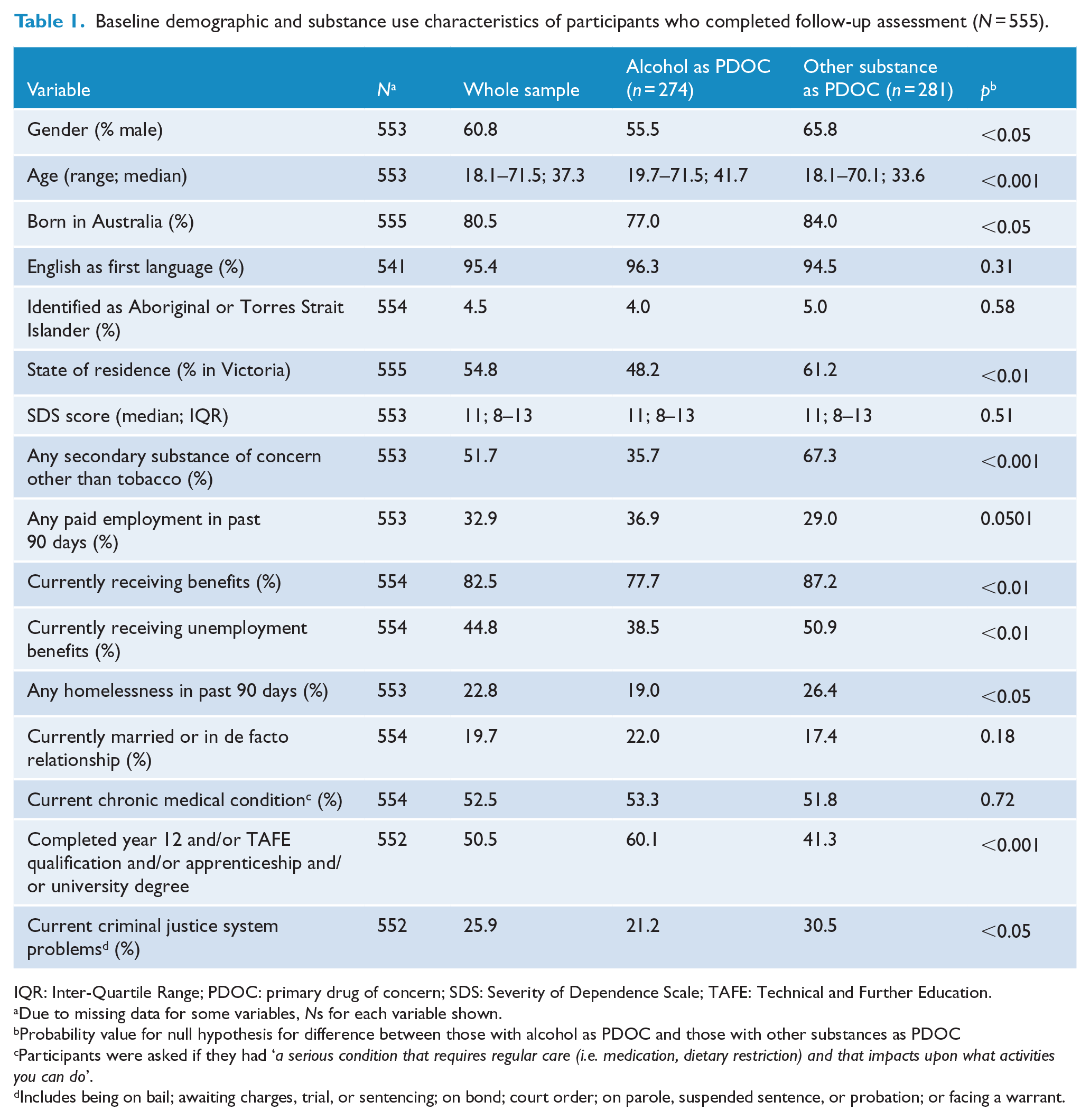
IQR: Inter-Quartile Range; PDOC: primary drug of concern; SDS: Severity of Dependence Scale; TAFE: Technical and Further Education.
Due to missing data for some variables, Ns for each variable shown.
Probability value for null hypothesis for difference between those with alcohol as PDOC and those with other substances as PDOC
Participants were asked if they had ‘a serious condition that requires regular care (i.e. medication, dietary restriction) and that impacts upon what activities you can do’.
Includes being on bail; awaiting charges, trial, or sentencing; on bond; court order; on parole, suspended sentence, or probation; or facing a warrant.
Service use
As a consequence of their severity and complexity, participants were engaged with a diverse range of services at baseline and most (68.8%) had received specialist AOD treatment in the year prior to the PIT. Table 2 shows changes in engagement with health (including acute services), social and welfare services in the year pre- and post-PIT. Approximately three-quarters engaged in further AOD specialist treatment post-PIT and reported using a non-AOD community service, with a significant 15.7% reduction (p < 0.001) in the proportion reporting use of acute services relative to baseline rates.
Use in the years before and after PIT of AOD specialist, community and acute medical service.
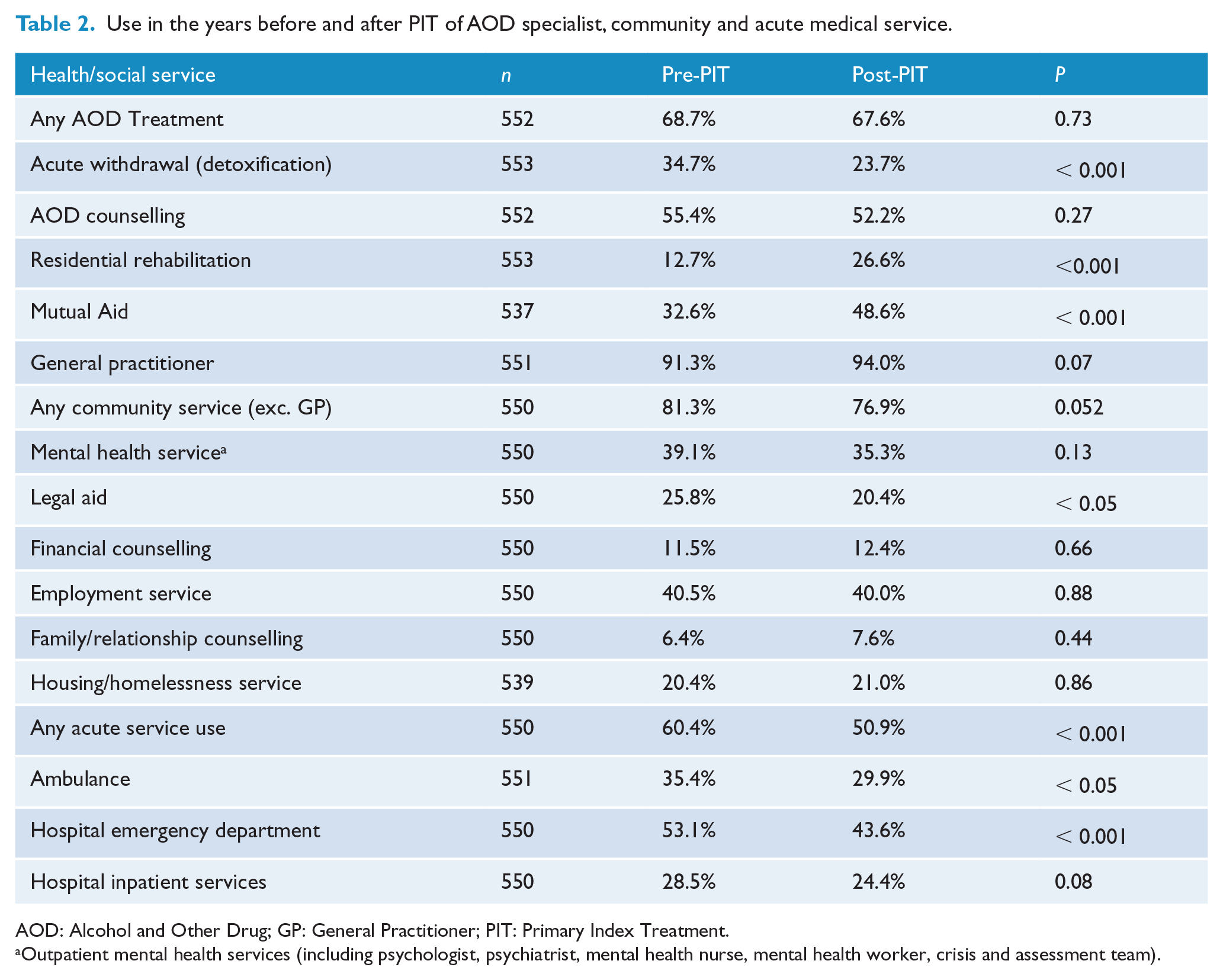
AOD: Alcohol and Other Drug; GP: General Practitioner; PIT: Primary Index Treatment.
Outpatient mental health services (including psychologist, psychiatrist, mental health nurse, mental health worker, crisis and assessment team).
Completion, duration and satisfaction with the primary index treatment
Almost two-thirds (65.6%) reported completing their PIT, with an additional 33 (6.0%) remaining in the PIT for the study duration. The median duration for those who had completed their PIT was 70 days for OPS, 7 days for AW and 70 for RR. Treatment satisfaction (a positive response to ‘Did you feel you successfully achieved what you wanted from treatment?’) was indicated by 77.3% of AW, 69.8% of RR and 62.3% of OPS participants. A Mann–Whitney U test revealed significantly higher scores on the CSQ-8 treatment satisfaction scale among participants who completed their PIT relative to those who left prematurely (median of 30 vs. 26 out of a possible 32; p < 0.001).
Primary outcome (treatment success)
Of those retained in the study, just over half (52.0%) of the cohort had reliably reduced the frequency of their PDOC (days in the month prior to interview) or had ceased using it (i.e. were abstinent in the previous month), and these participants were considered to be a ‘treatment success’. Rate of treatment success was highest when meth/amphetamine was the PDOC, followed by opioids, then cannabis, and was lowest for alcohol and ‘other drugs’ (see Figure 2 for rates of treatment success by PDOC). Taking a conservative approach and assuming those lost to follow-up had continued using, 35.9% of the entire baseline sample would be classed as treatment successes. The overall rate of abstinence 1 from the PDOC in the month prior to follow-up was 37.5% and highest when the PDOC was meth/amphetamine followed by opioids, ‘other drugs’, cannabis, and was considerably lower for alcohol (see Figure 2). Finally, 13.9% reported being continuously abstinent from their PDOC during the entire year between baseline and follow-up interview (26.1% when the PDOC was meth/amphetamine, 17.0% for opioids, 16.5% for cannabis and 7.7% for alcohol; p < 0.001).
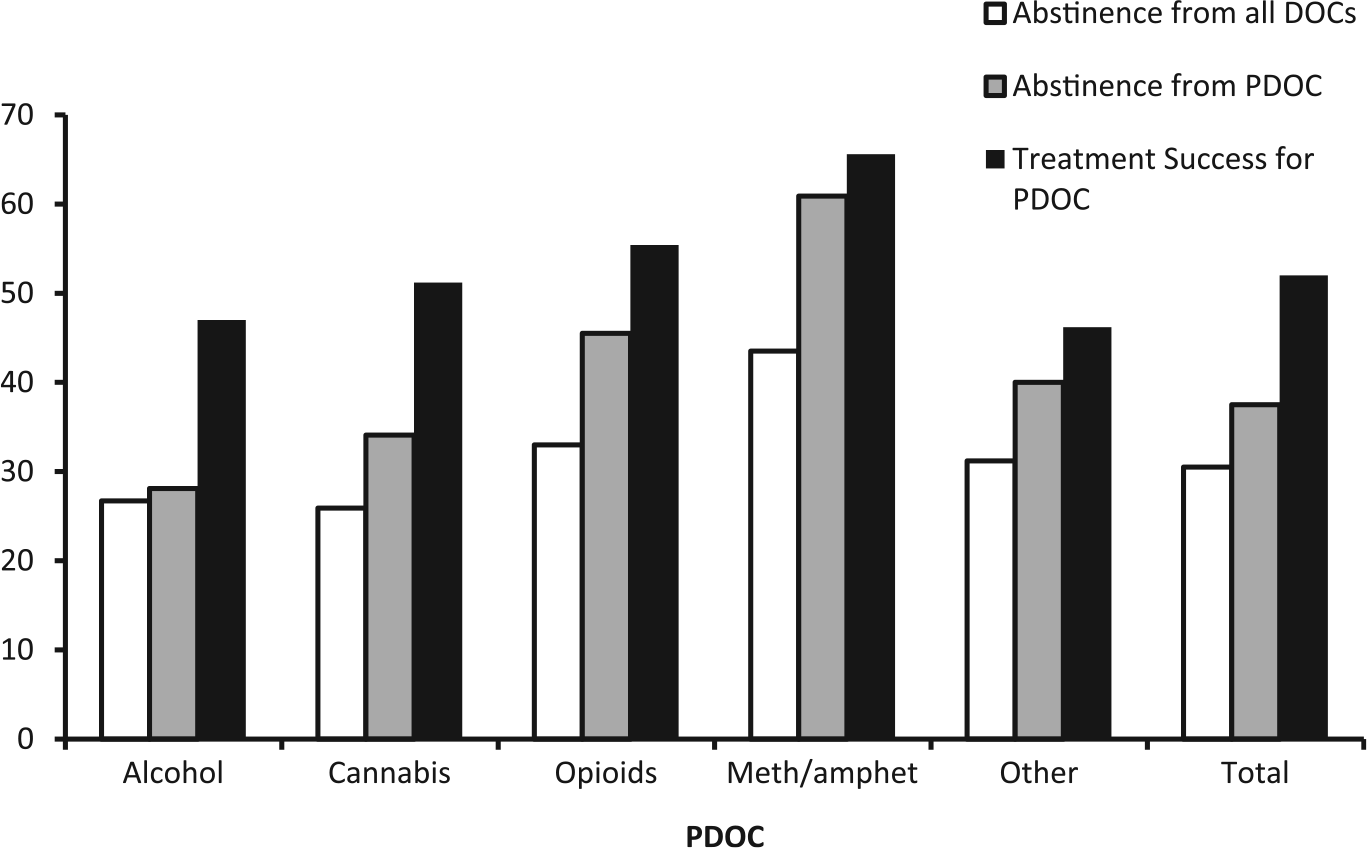
Percentage rates of abstinence from PDOC, all DOCs, and treatment success by PDOC.
Abstinence from all DOCs
Past-month abstinence from all DOCs (other than tobacco) was reported by 30.5% of the follow-up sample. Taking a conservative approach and assuming those lost to follow-up would not have been abstinent at follow-up, 21.3% of the entire baseline sample was abstinent from all DOCs. Only 4.3% reported being continuously abstinent from all alcohol and drug use (aside from tobacco) during the past year.
Impact of specialist AOD pathway and community service use on outcomes
Chi-square analyses indicated that participants who experienced continuity of AOD specialist services (n = 200) reported significantly higher rates of PDOC abstinence (38.2% vs. 25.2%, p < 0.01) and treatment success (61.0% vs. 44.0%, p < 0.001) than those who received fragmented AOD specialist treatment (n = 206). There were no significant differences in outcomes associated with use of community services in the past 12 months in the whole sample (all p > 0.05).
Predictors of treatment success (PDOC)
The preliminary model that only included demographic and social disadvantage indicators (gender, Australian state, education, not being married or in a de facto relationship, unemployment and recent homelessness) had a small but statistically significant predictive value for treatment success (Nagelkerke R2 = 0.04, χ2 = 18.17, p = 0.03), with age as the only significant individual predictor (OR = 0.98, p < 0.05), with younger participants more likely to achieve treatment success. Age was therefore entered as a predictor in subsequent regression analyses alongside treatment characteristics (e.g. PIT completion, PIT-type, continuity of specialist AOD care, community service use), PDOC and mutual aid attendance, controlling for follow-up interval.
In the first logistic regression analysis examining predictors of treatment success (see Table 3, column 1), the overall model was significant (Nagelkerke R2 = 0.12, χ2 = 49.4, [df = 12], p < 0.001). Relative to clients with alcohol as their PDOC, those with meth/amphetamine as the PDOC had more than twice the odds (OR = 2.2, p < 0.01) of being a treatment success. Completing the PIT almost doubled the odds (OR = 1.91, p < 0.01), while attending mutual aid increased the odds of being a treatment success by 72.0%.
Odds ratios for predictors of treatment success and abstinence from all DOCs.
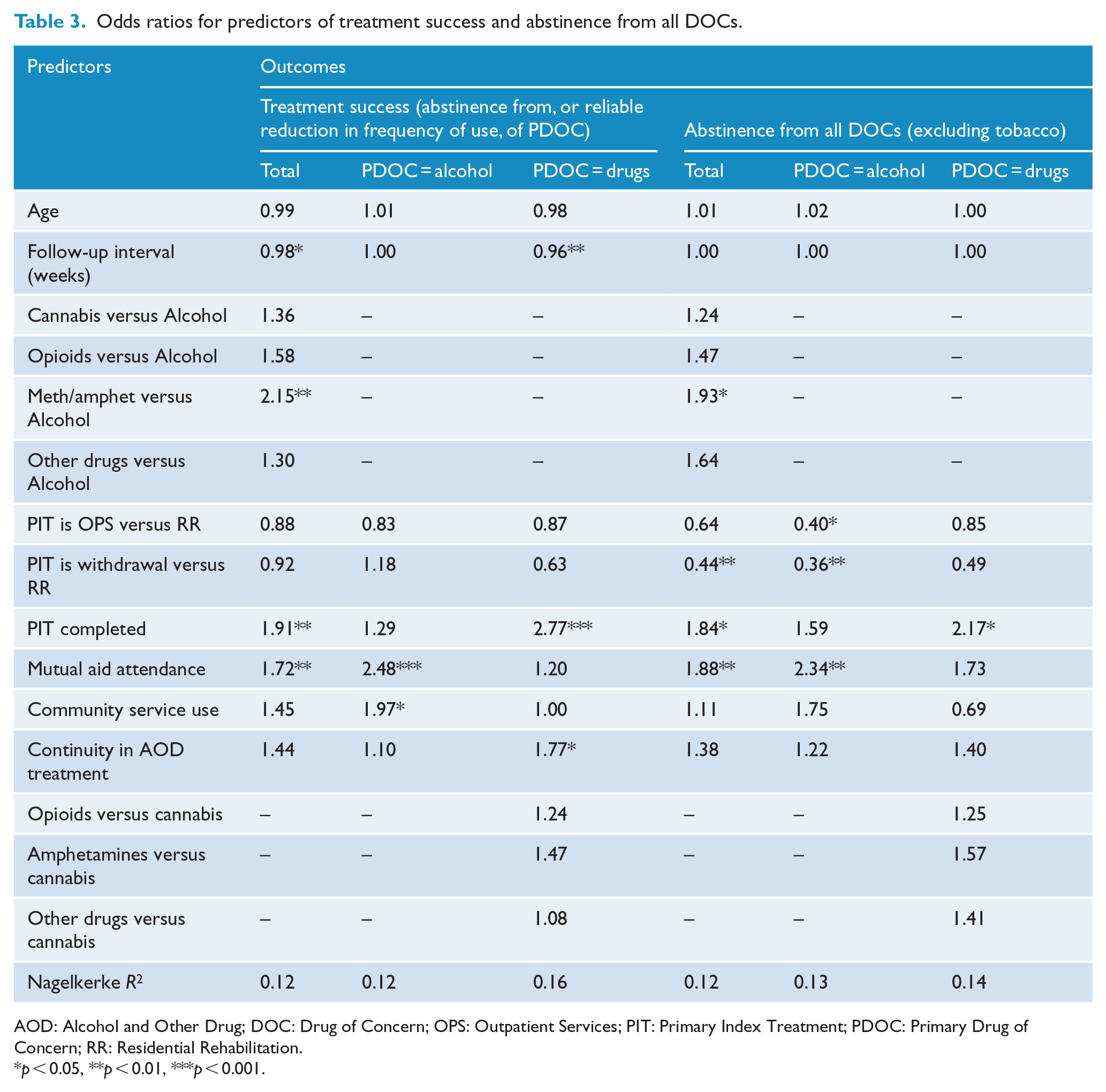
AOD: Alcohol and Other Drug; DOC: Drug of Concern; OPS: Outpatient Services; PIT: Primary Index Treatment; PDOC: Primary Drug of Concern; RR: Residential Rehabilitation.
p < 0.05, **p < 0.01, ***p < 0.001.
To explore possible differences between clients with primary alcohol problems and those with primary drug problems, the regression analysis was repeated separately for the two groups (see Table 3, columns 2 and 3). For clients with a primary alcohol problem, the model was significant (Nagelkerke R2 = 0.12, χ2 = 25.1 [df = 8], p < 0.01), but the only significant predictors were mutual aid attendance (OR = 2.5, p < 0.01) and engaging in community services (OR = 2.0, p < 0.05), which doubled (or more) the odds of treatment success. For clients with a primary drug problem, the model was also significant (Nagelkerke R2 = 0.16, χ2 = 34.5 [df = 11], p < 0.001), but only PIT completion (OR = 2.8, p < 0.01) and continuity in specialist AOD service use increased the likelihood of being a treatment success (OR = 1.8, p < 0.05).
Predictors of abstinence from all DOCs
Applying the above model to specifically predict abstinence from all DOCs (see Table 3, column 4), we found that the overall model was significant (Nagelkerke R2 = 0.12, χ2 = 47.20, [df = 12], p < 0.001). Relative to participants with alcohol as their PDOC, those with meth/amphetamine had nearly twice the odds of abstaining from all DOCs. Completing the PIT also almost doubled the odds, as did attending mutual aid. Having AW as the PIT relative to RR significantly reduced the odds of achieving abstinence from all DOCs, though continuity in AOD specialist care and community service use (excluding GPs) had no impact on this outcome. When analyses were restricted to participants with alcohol as their PDOC, mutual aid attendance became a stronger predictor (OR = 2.3) and RR as the PIT was superior to both AW and OPS as a predictor. In contrast, when restricted to clients with drugs as a PDOC, mutual aid attendance and RR as the PIT were both lost as predictors, while PIT completion became slightly stronger.
Association between mutual aid and outcomes
Since mutual aid attendance predicted treatment success in clients with a primary alcohol (but not drug) problem, this effect was explored further by examining the impact of frequency of meeting attendance among those with any mutual aid attendance. The most common forms of mutual aid among those who had attended at least one meeting in the past year (n = 267) were Alcoholics Anonymous (68%) and Narcotics Anonymous (67%), while 11% attended SMART recovery meetings and 5% reported attendance at ‘other’ recovery groups. Bivariate logistic regression analysis, with number of mutual aid meetings attended during the follow-up period as the predictor, showed that each mutual aid meeting attended increased the odds of treatment success by approximately 1% (OR = 1.01, p < 0.01). When the analysis was restricted to those with alcohol as their PDOC, this effect remained significant (OR = 1.01, p < 0.05), but when restricted to those with other drugs as their PDOC, this was non-significant (OR = 1.00, p = 0.07). Figure 3 shows that success rates for clients with a primary alcohol problem were substantially lower when there was little or no engagement in mutual aid, but increased to levels similar to those shown by clients with drugs as their PDOC with higher frequency of mutual aid engagement.
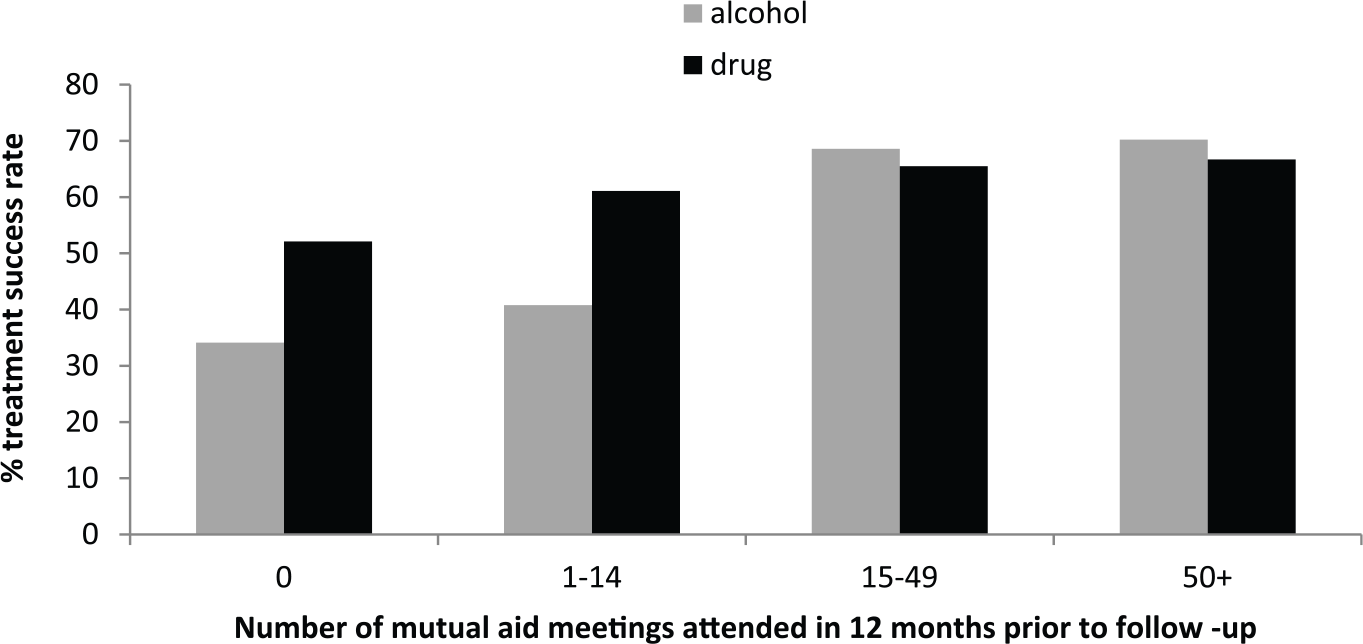
Relationship between number of mutual aid meetings attended and treatment success rates in clients with a primary alcohol or drug problem.
Discussion
This multi-site study examined treatment outcomes for clients with a broad range of PDOCs (including alcohol and cannabis), who were accessing AOD treatment across multiple service types. The study is unique in examining client engagement within the broader treatment and welfare systems, both in the year prior to and following study intake, and the relationship with treatment outcomes. Supporting earlier treatment outcome research, marked improvements in AOD use were observed at the 12-month follow-up with more than half of the sample substantially reducing the number of days they used their PDOC, and more than one-third reporting abstinence from their PDOC in the month prior to interview. Another strength of the study is its consideration of abstinence from all DOCs, an outcome achieved by over 30% of the retained sample. Substance use outcomes did not vary greatly by PDOC, but were best when meth/amphetamine was the PDOC and poorest with alcohol.
After controlling for the effect of multiple independent variables, completing the PIT predicted a higher likelihood of both outcomes, consistent with international literature that emphasises the importance of treatment retention and completion (Gossop et al., 2001; Simpson and Sells, 1990). Having a residential rehabilitation as the PIT predicted abstinence for the whole sample, but did not significantly predict treatment success when alcohol was the PDOC. Mutual aid attendance significantly predicted both outcomes, as did having a primary meth/amphetamine problem relative to alcohol.
Mutual aid attendance and community service engagement were significant predictors for clients with a primary alcohol problem, while PIT completion and continuity of specialist AOD care were significant predictors for those with a primary drug problem, with no predictor being significant in both groups. These findings support US data on the value of continuity in specialist AOD treatment and engagement with non-AOD community health and welfare services (Chi et al., 2011; Chi and Weisner, 2008); however, they suggest that specific components of this model may differentially benefit distinct substance-using populations. It is possible that characteristics associated with alcohol-dependent individuals presenting to treatment, such as older age, longer problem use histories and greater cognitive impairment (Stavro et al., 2013), as well as societal factors (e.g. the pervasive availability of alcohol and its greater social acceptability in comparison to illicit drugs) pose particular challenges for those with alcohol as their PDOC, despite lower levels of social disadvantage identified in the current sample. This may explain why engagement with community services and mutual aid significantly increased the likelihood of successfully responding to treatment, since they could offer the necessary support mechanisms to safeguard against the ubiquitous opportunities to consume alcohol in Australian society. Interestingly, engagement with community services and mutual aid failed to boost outcomes for clients with a primary drug problem who instead benefited from a more extensive or continuous AOD treatment pathway (completing the PIT and being referred onto further AOD treatment). This may reflect differences in perceived suitability of, or need for, specialist AOD treatment between clients with a primary alcohol or drug problem. Thus, failing to complete a treatment episode or the absence of continued AOD specialist care becomes more of a setback for clients with a primary drug problem who have fewer support options outside of specialist AOD services.
Since most long-term residential therapeutic care is abstinence-oriented, it was not surprising that having RR as the PIT was a significant predictor of abstinence from all DOCs, although this was limited to clients with a primary alcohol problem. This highlights the need to increase the availability and accessibility of RR, and is consistent with a growing international literature on the effectiveness of long-term residential care for achieving abstinence (e.g. Vanderplasschen et al., 2014). It is recognised that a period of residential stay can be a sufficient ‘turning point’ in a developmental recovery trajectory (Best, 2014). However, in light of its elevated cost and limited places, alternative, cost-effective models of care and integration within the community must also be identified. While again limited to clients with a primary alcohol problem, a dose-response effect of mutual aid engagement was observed whereby attendance at more meetings increased rates of treatment success. This is consistent with earlier research (Kaskutas, 2009) and supports an additive effect of treatment and mutual aid. These findings suggest alcohol-dependent clients require engagement with support beyond professional AOD treatment to enhance their treatment journeys and recovery pathways. The findings support the benefits of mutual aid engagement as a form of aftercare or as an adjunctive therapy (Kelly et al., 2013). It is important to recognise, however, that mutual aid attendance could simply reflect a greater motivation to overcome AOD problems rather than having a direct casual impact on outcomes.
There are a number of important limitations that must be considered when interpreting these results. While AOD treatment was found to be effective, it is important to note the absence of a no-treatment control group. Natural recovery is well-documented (Dawson et al., 2005), and may have led to some of the improvement. Moreover, patients are more likely to present for treatment at times of crisis, and substance use and other problems may naturally improve over time. Nevertheless, the finding that treatment type, treatment completion and referral pathways leading to continuity of AOD treatment influenced outcomes suggests that at least some treatment types and pathways have additional beneficial effects above any effects that would be expected in the absence of treatment. This is consistent with findings from MATES and ATOS, which both demonstrated superior outcomes among treated relative to non-treated drug-dependent individuals. Moreover, other factors associated with positive outcomes in the current study, such as engagement with wraparound community services and other forms of support (e.g. mutual aid), were significant after controlling for treatment intensity and duration, highlighting the important role of both specialist AOD and non-AOD support systems.
Since participants were not randomly assigned to different levels of predictors (e.g. randomised to PIT types or mutual aid), causal conclusions cannot be drawn definitively, as unmeasured confounding factors may explain some of the associations between predictors and outcomes. While the follow-up rate of 70% is acceptable, the outcomes of those who could not be re-contacted for interview, which could reflect greater instability and poorer functioning, are likely to be poorer and differences in the characteristics of those who were and were not followed up may have biased findings. A further limitation was that telephone interviews precluded the use of objective measures (breathalyser or urine analysis) to corroborate self-reported AOD use. Self-report is, however, well-established as an accurate method for capturing AOD use under conditions that were applied in this study (i.e. when confidentiality is guaranteed and when reporting to an independent researcher (Napper et al., 2010)).
Despite the aforementioned study limitations, the findings point towards a number of important implications for policy and practice. Given the increasing public concern around individual and community harms associated with meth/amphetamine use (Australian Crime Commission [ACC], 2015), the high rates of abstinence and reduced days of use among participants with a primary meth/amphetamine problem is encouraging, and highlights the importance of broadly promoting the effectiveness of AOD treatment to the community. Since completion of the PIT was a robust predictor of outcome among clients with a primary drug problem, it reinforces the importance of strategies to enhance treatment retention and satisfaction during treatment (Simpson, 2004).
Since greater continuity in AOD specialist treatment was also important, this calls for enhanced efforts around case coordination, regular reviews of client need and assertive and timely referral to appropriate services to aid transition through the AOD treatment system. In addition, as fragmented AOD treatment pathways were associated with poorer outcomes, methods to enhance retention and completion should be investigated. Indeed, our findings highlight the importance of funding models that promote continuity and service integration and facilitate treatment journeys that involve multiple treatment modalities and greater linkage to follow-up care.
Service providers might consider assertive linkage to supportive community groups, including but not restricted to mutual aid groups. These can offer a free and widely available form of aftercare which is important for chronic and relapsing conditions (O’Brien and McLellan, 1996). Referral from specialist AOD settings to community-based recovery-focussed organisations has proven effective in international research (Kaskutas, 2009; Manning et al., 2012; Timko et al., 2006), and is considered an important component of an integrated treatment system (White, 2009).
This study highlights the importance of treatment systems research that looks at treatment populations as they occur and considers the effectiveness of the AOD service sector within broader health and welfare systems. The study examines treatment outcomes as they occur within existing treatment services/systems including clients selected only by their willingness to participate and not by the rigorous clinical inclusion/exclusion criteria of randomised controlled trials (RCTs). Such naturalistic treatment outcome studies are needed to complement the already well-established tradition of controlled studies of particular treatment modalities, which by design provide limited information on the influence of context (e.g. setting, funding, workforce) and implementation challenges. Further investment in treatment systems research is essential for informing the design of the Australian AOD sector, and identifying the strengths and weaknesses of particular models of care.
Footnotes
Acknowledgements
We thank the participants, the treatment service staff that supported the project, and members of Alcohol and other Drugs Council of Australia (ADCA) for their support and expertise. We would like to thank other members of the research team who assisted with the project: Seraina Agramunt, Julia Butt, Sue Carruthers, Dina Eleftheriadis, Sarah Flynn, Jodie Grigg, Cherie Heilbronn, Barbara Hunter, Klaudia Jones, Shraddha Kashyap, Jessica Killian, Belinda Lloyd, Melaine McAleer, Terence McCann, Vijay Rawat and Terry Slomp. This work could not have been completed without the support of the Commonwealth Department of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Commonwealth Department of Health, Australia.