
Abstract
Chronic conditions account for the majority of health care expenditure [1]. For these, the primary goal of treatment is to maximize function and wellbeing. Alcohol dependence is a chronic relapsing condition. Daily functioning, subjective and objective health status is often impaired during periods of heavy alcohol consumption and following treatment [2]. This reflects a variety of potential contributing factors, including poor emotional functioning, comorbid psychiatric conditions, alcoholinduced medical illness, altered socioeconomic status secondary to reduced work performance or job loss, social impairment and isolation. The relationship between changes in alcohol consumption which occur during rehabilitation and the participant's level of wellbeing has not been extensively explored.
In this study the treatment program used cognitive behaviour therapy (CBT), based on established principles of social cognitive theory. Cognitive behaviour therapy applied to alcohol dependence has been repeatedly demonstrated to be effective in reducing drinking in randomised trials [3]. The current program was developed to minimize patient drinking by improving management of life's stressors, including alcohol cues. In addition to coping skills training, CBT employs techniques of modelling, role-play and behaviour rehearsal to enable patients to develop an adaptive command of stressful situations [4–6].
Adjunctive pharmacological treatments for alcohol dependence are now available. Early clinical studies with naltrexone, a long-acting opiate antagonist, reported reductions in the number of drinking days and an increase in the rates of continuous abstinence [7], [8]. More recent meta-analysis of randomised controlled trials of naltrexone use in alcohol dependence treatment supports these findings [9]. Naltrexone has been reported of benefit when used in conjunction with CBT [10], [11] although one recent study which employed 12-step facilitation in patients with chronic severe alcoholism did not report an additional benefit with naltrexone [12].
In alcohol treatment evaluation, trials employing CBT and pharmacotherapy [10], [11] document abstinence or reduced drinking as the main outcome. They also report measures of compliance such as program attendance and improvement in biochemical measures. Less commonly, treatment outcome studies in alcohol dependence have directed attention toward the patient's self-reported level of health and wellbeing [13], [14]. This contrasts with other disease research where the patient needs to acquire skills in the management of their illness. Self-reported health-related quality indices are considered as a major outcome in addition to other widely used clinical response measures of survival or cure rates [15]. Recently, self-report outcome measures have been applied to funding allocation decisions and used in needs analysis for resource distribution in research, training and health care [16]. Few treatment studies of alcohol dependence have applied prospective measures to document these areas of potential change [17], [18].
In this study all patients began an outpatient 12-week CBT rehabilitation program. All were offered the option of adjunctive treatment with the anticraving agent naltrexone. Participants' health status and wellbeing was assessed using two instruments: The Rand Corporation medical outcomes short-form 36 health survey (SF-36) [19], and the General Health Questionnaire (GHQ-28) [20]. Treatments that recognize a central role for learned coping responses, if effective, should impact favourably on participant's subjective sense of wellbeing. One treatment objective was to determine whether changes in alcohol consumption were associated with subjective improvement. To capture these changes we compared pre- and post-treatment health status and wellbeing outcomes with published national, non-clinical, normative data. Whether the patient selection of naltrexone, in addition to CBT, distinctly enhances health status outcomes is unknown. This study considers if the patient's choice to include the adjunctive anticraving agent naltrexone further improved these psychosocial outcomes, above and beyond the impact of the CBT program alone in the treatment of alcohol dependence.
Method
Subjects
One hundred and thirty-six patients were consecutively treated for alcohol dependence. All patients provided written consent to participate in the study. This is an extension of a sample previously reported [11]. Of these, just over half (54%) chose CBT alone and declined medication (73 CBT only group). The remainder (63 naltrexone ++ CBT group) had naltrexone prescribed each clinic visit. A matched design was used. Each subject was individually paired by treatment condition (blind to outcome measures) on the following parameters: gender (male/female); age (0–19, 20–39, 40–59, 60–79); prior medically supervised detoxification (yes/no); alcohol problem severity (below 50th percentile/above 50th percentile of the brief Michigan Alcoholism Screening Test (bMAST).
With this approach 86 (43 naltrexone ++ CBT, 43 CBT-only) were matched. Where there was more than one possible match, a random selection option was employed using the Statistical Package for the Social Sciences (SPSS V.11). Patients who could not be paired on the entire individual matching parameters (n = 50) were not included. There wer 27 men and 16 women in each group.
The mean age amongst the matched naltrexone ++ CBT group was 39.72 ± 8.22 years compared with 37.40 ± 9.61 in the matched CBTalone group (F1,84 = 1.45, p = 0.231).
Inclusion and exclusion criteria
All patients were over the age of 18 years, fulfilled the DSM-IV criteria for alcohol dependence and recorded bMAST scores of ≥ 6 (range 0–29 scores, ≥ 6 associated with a high likelihood of alcohol dependence) [21]. All had sustained at least 3 days of alcohol abstinence. Exclusion criteria included current dependence on substances other than alcohol (except nicotine), current acamprosate, disulfiram, prescribed opioid or psychotropic medication use.
Treatment groups
Control (CBT-alone) subjects
All CBT-alone (control) subjects participated in an abstinence-based cognitive behavioural therapy (CBT) outpatient program without adjunctive medication (naltrexone). The program contained defined cognitive and behavioural components conducted by clinical psychologists. These components focused on four core areas: (i) identification and modification of alcohol expectancies; (ii) increasing drinking refusal self-efficacy skills; (iii) developing more effective coping strategies; and (iv) teaching problem-solving skills. Comprehensive supervision and training in-line with the treatment manual was provided to each therapist by a Doctoral level, senior psychologist (RY). The program included hourly therapy sessions weekly for the first 4 weeks. Patients were then seen fortnightly for the subsequent 8 weeks, completing 8 sessions over the 12 weeks of the program. Patients continued with the same therapist throughout the program.
Naltrexone (naltrexone ++ CBT) subjects
Naltrexone ++ CBT subjects were prescribed naltrexone 50 mg orally daily. Prescriptions were collected before each scheduled therapy session. These subjects received the same program as the CBT-alone group.
Measures
Psychosocial function
SF-36 Health Survey (SF-36) [19]: This is a generic 36-item self-report measure. It assesses subjective health status across eight dimensions: (i) physical functioning; (ii) role limitations (physical problems); (iii) role limitations (emotional problems); (iv) social functioning; (v) bodily pain; (vi) mental health; (vii) vitality; and (viii) general health perception. Raw scores are usually transformed to standard scores (0–100). Lower scores on the SF-36 subscales reflect poorer functioning.
General Health Questionnaire (GHQ-28) [20]: This is a domainspecific 28-item self-report measure designed to identify short-term changes in health perception. The GHQ-28 has four subscales measuring: (i) somatic symptoms; (ii) anxiety; (iii) social dysfunction; and (iv) depression. Higher scores on the GHQ-28 subscales reflect poorer functioning. Scoring the GHQ-28 followed the test manual recommendations (0, 0, 1, 1) using the Likert scale method. More complex scoring approaches have been developed, but offer little additional advantage [20], [22]. The clinically significant threshold score for psychiatric case identification or ‘caseness’ is 4/5 for the total scale [20]. For subscales analyses, a threshold of 1/2 has been recommended [23].
Measures of program compliance
Attendance and alcohol abstinence: The treating psychologist recorded attendance across each of the eight treatment sessions (12 weeks) for each patient. Alcohol abstinence was estimated by a combination of factors including: patient self-report (alcohol timeline followback [TFLB]) [24]; clinic visit alcohol breathalysation (BAL); monthly serum transaminases (aspartate aminotransferase, gamma glutamyl transpeptidase); and monthly serum carbohydrate deficient transferrin estimation [25]. If the patient failed to maintain abstinence, the week of breach was noted and days abstinent calculated. For the purposes of this study, withdrawal from treatment was classified as a failure to maintain abstinence.
Statistical analysis
Chi-square analyses were used with dependence severity/risk features and to determine if the proportion of program attendance and abstinence differed between treatment groups. Chi-square analyses were also employed for each GHQ-28 factor to examine proportions of caseness between treatment groups. Average days abstinent, by group, was calculated using ANOVA. Baseline treatment group differences on the primary dependent variables in this study (SF-36 and GHQ-28) were investigated through a multivariate analysis of variance (MANOVA) for all subjects who commenced the program, with separate analyses examining only the baseline data for those who completed. Changes in treatment group scores on the SF-36 and GHQ-28 subscales from initial assessment (baseline) to program completion (time 2) were analysed by repeated measures ANOVA. Ninety-five percent confidence intervals for national SF-36 and GHQ-28 normative data were calculated for comparison with pre- and post-treatment scores. All analyses were conducted using SPSS (V.11).
Results
Patient characteristics
Pre-treatment abstinence
Of the 86 patients, 88% reported < 7 days alcohol abstinence before joining the program and this did not differ significantly between both groups (83.7% naltrexone ++ CBT compared with 92.7% CBT-alone, χ2 = 1.51, p = 0.316).
Features of dependence severity and risk
Features of dependence severity and risk, by treatment group, are reported in Table 1.
Features associated with dependence severity
Program completion and abstinence by treatment group
The proportion of patients completing the 12-week program by treatment group, as defined by their attendance at each scheduled follow-up session, was determined by chi-square analysis. The attendance ratio was 31/43(72.1%) in the naltrexone ++ CBT group and 23/43(53.5%) in the group selecting CBT-alone. The difference in the attendance ratio between the two groups was not significant (χ2 = 3.19, p < 0.074). However, this result does represent a trend toward the naltrexone ++ CBT group having a higher proportion of patients attending the program to completion. An increased sample size may have moved this trend to a statistically significant result.
The proportion of patients within the two treatment groups that remained abstinent across the 12-week program was also determined by chi-square analysis. Program withdrawal prior to completion was recorded for the purposes of this study as a failure to maintain abstinence. Only one subject's CDT status was inconsistent with their selfreport and was recorded as a breach of abstinence. The abstinence ratio was 25/43(58.1%) in the naltrexone ++ CBT group and 15/43(34.9%) in the CBT-alone group. The difference in proportions between the two groups was significant (χ2 = 4.67, p = 0.031). The average number of days abstinent over the 12-week (84-day) program duration for the naltrexone ++ CBT group was 61.21 (± 30.13) and for the CBT-alone group 38.58 (± 29.51), representing a statistically significant difference between groups (F1,84 = 10.32, p = 0.002).
Baseline SF-36 and GHQ-28 scores
All Participants pre-treatment MANOVA revealed no significant differences across the SF-36 (Hotelling's T2 = 0.167, F8,77 = 1.248, p = 0.206) and GHQ-28 (Hotelling's T2 = 0.253, F4,74 = 1.43, p = 0.212) subscales between the subjects in the naltrexone ++ CBT and CBT-alone groups.
Program completers
Of the 54 patients who completed (31 naltrexone ++ CBT, 23 CBT-alone) the treatment program, there were no significant multivariate differences between treatment groups on baseline SF-36 (Hotelling's T2 = 0.253, F8,45 = 1.43, p = 0.212) or GHQ-28 (Hotelling's T 2 = 0.112, F4,49 = 1.37, p = 0.257) measures.
Using the baseline cut-off of 1/2 [23] for the completers, there were no significant treatment group differences in ‘caseness’ across all the GHQ-28 subscales: somatic symptoms (CBT ++ naltrexone = 61.3%%, CBT-alone = 69.6%, χ2 = 0.396, p = 0.529); anxiety (54.8%, 68.6%, χ2 = 1.21, p = 0.272); social dysfunction (48.4%, 60.9%, χ2 = 0.827, p = 0.363); and depression (48.4%, 30.4%, χ2 = 0.828, p = 0.184).
SF-36 and GHQ-28 changes across program duration
To investigate if there were changes in SF-36 and GHQ-28 subscales over the duration of the treatment program, including possible differential responses in relation to treatment condition (CBT ++ naltrexone vs. CBT-alone), repeated measures ANOVA s were conducted.
SF-36 changes across program duration and treatment group differences
Within the sample that completed the program, there were significant increases (improvement) in scores on the SF-36 subscales of: physical functioning (F1,52 = 8.70, p = 0.005); role limitations (physical problems), (F1,52 = 21.85, p < 0.001); bodily pain (F1,52 = 15.37, p < 0.001); general health perception (F1,52 = 13.81, p < 0.001); social functioning (F1,52 = 41.68, p < 0.001); role limitations (emotional problems) (F1,52 = 81.98, p < 0.001); and mental health (F1,52 = 33.77, p < 0.001) was observed for both treatment groups. There was no overall reported improvement in vitality (F1,52 = 2.14, p = 0.149).
When treatment groups were examined across program duration, the CBT-only group showed greater improvement than the CBT ++ naltrexone group on the SF-36 subscales of general health perception (F1,52 = 4.10, p = 0.048) and vitality (F1,52 = 5.55, p = 0.022). There were no significant treatment group differences reported on the SF-36 subscales of; physical functioning (F1,52 = 2.77, p = 0.102); role limitations (physical problems) (F1,52 = 2.77, p = 0.102); bodily pain (F1,52 = 0.950, p = 0.334); social functioning (F1,52 = 0.527 p = 0.471); role limitations (emotional problems) (F1,52 = 1.26, p = 0.268); and mental health (F1,52 = 0.634, p = 0.430).
Figure 1 summarizes pre- and post-treatment SF-36 scores with the naltrexone ++ CBT and CBT-alone subjects in relation to observed normative data. The normative data was extracted (age and gender data collapsed to obtain mean scores) from a study [26] on a non-clinical sample of 12 793 adults sampled from the same Australian state as the patients in this study. Confidence internals (95%) were calculated from this normative sample. All of the mean pre-treatment SF-36 subscale scores for both the naltrexone ++ CBT and CBT groups (except naltrexone ++ CBT vitality [mean = 69.71, CI = 63.93–64.61]) fell below the lower confidence interval limit. Apart the mean naltrexone ++ CBT groups' vitality score, all of the SF-36 subscales improved by the 12-week assessment, with subscales of physical functioning, physical problems, bodily pain in both treatment groups and general health perception and vitality in the CBT group falling within or above the normative upper confidence internals. The subscales of social functioning (mean N = 73.26 [CBT] = 76.17, CI = 86.26–86.94), emotional problems (mean N = 72.45 [CBT] = 83.77, CI = 87.03–87.93) and mental health (mean N = 75.90 [CBT] = 73.68, CI = 79.62–78.18), while showing improvement from pre-treatment did not fall within the 95% normative confidence intervals. The general health preception subscale in the CBT-only group also fell below confidence internals (mean = 67.67, CI = 72.70–73.40).
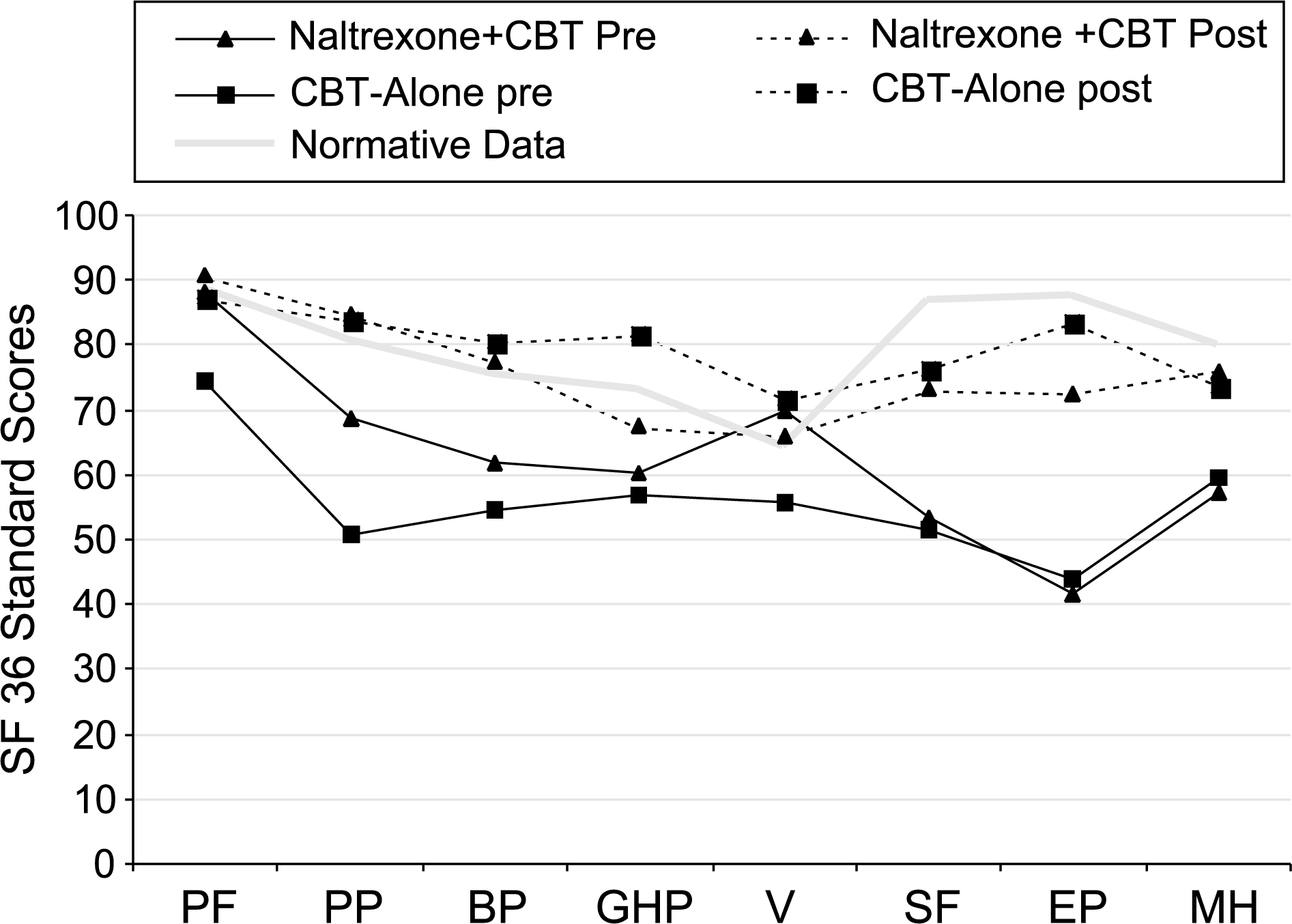
Pre- and post-treatment SF-36 scores by treatment condition.
GHQ-28 changes across program duration and treatment group differences
Within the sample that completed the program, a significant decrease (improvement) in scores on the GHQ-28 subscales of: somatic concerns (F1,52 = 21.93, p < 0.001); anxiety (F1,52 = 30.49, p < 0.001); social dysfunction (F1,52 = 16.43, p < 0.001); and depression (F1,52 = 11.67, p < 0.001), was observed upon program completion for both treatment groups. The CBT-only group showed more improvement on the GHQ-28 anxiety subscale, than did the CBT ++ naltrexone group (F1,52 = 4.65, p = 0.036). There were no treatment group differences in the degree of change across GHQ-28 subscales of: somatic concerns (F1,52 = 1.62, p = 0.208); social dysfunction (F1,52 = 0.191, p = 0.664); and depression (F1,52 = 0.304, p = 0.584).
Figure 2. summarizes pre- and post-treatment GHQ-28 scores with the naltrexone ++ CBT and CBT-alone subjects in relation to observed normative data. Australian GHQ-28 normative data was obtained from a sample of 2051 South Australian subjects [23]. Confidence internals (95%) were calculated form this normative sample. All of the mean pre-treatment GHQ-28 subscale scores for both the naltrexone ++ CBT and CBT-alone groups fell below the lower confidence interval limit. Each of the GHQ-28 subscales improved by the 12-week assessment, with the subscales of somatic concern, anxiety, social dysfunction and depression (naltrexone ++ CBT only) falling within or above the normative upper confidence internals. Within the CBT-only group, the depression subscale, while showing improvement from pre-treatment, did not fall within the 95% normative confidence intervals (mean = 0.73, CI = 0.17–0.24).
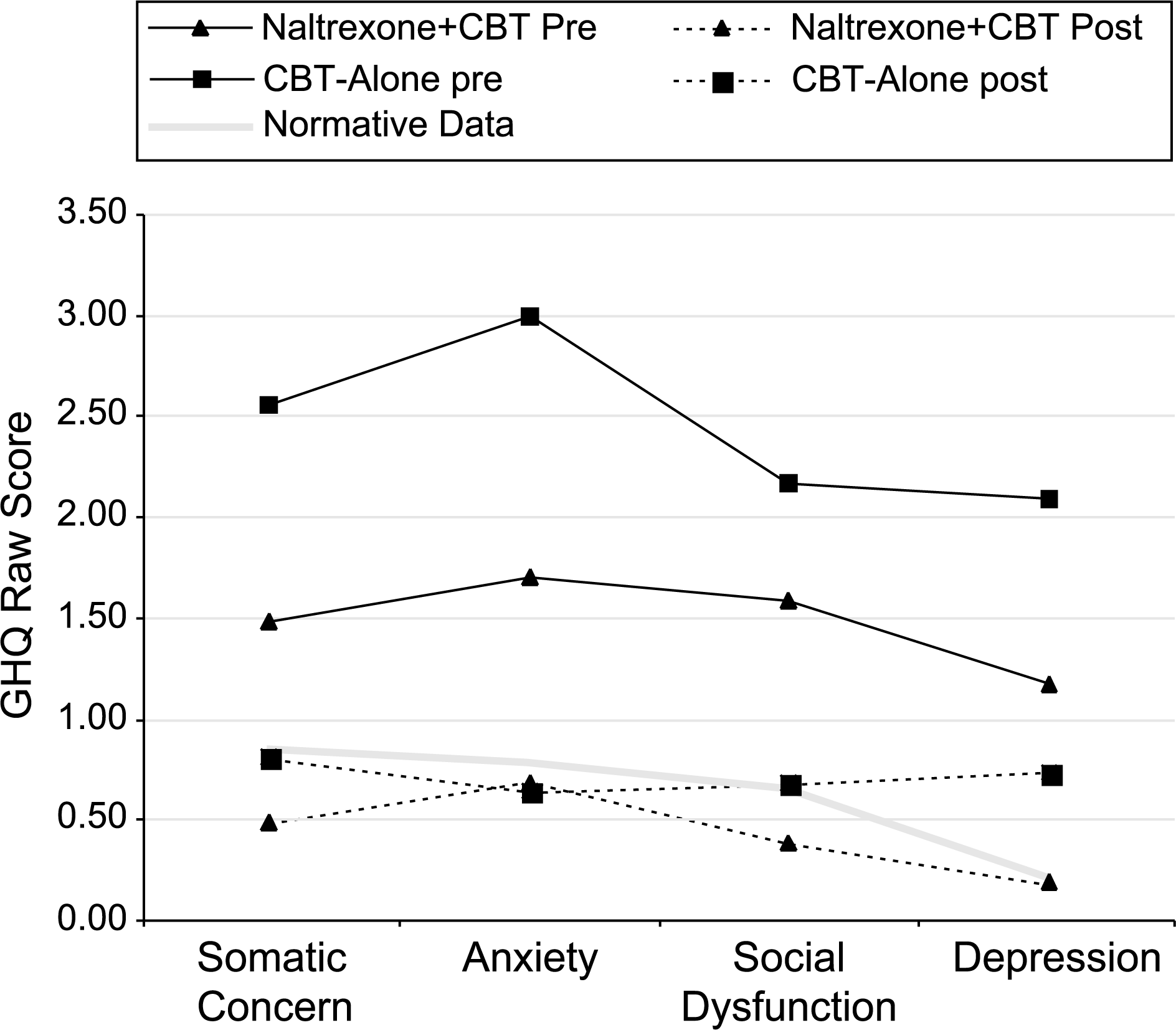
Pre- and post-treatment GHQ-28 scores by treatment condition.
Discussion
One objective of this study was to establish if participants in this treatment program reported improvement in subjective measures of health status and wellbeing. Where health status measures have been applied to patients with alcohol dependence they rate poorly when compared with normative data [18], [27], [28]. As a global measure, the SF-36 Health Survey has been among the most widely used and well-validated in medical research [29]. Our study participants confirm poorer self-report health status and diminished subjective wellbeing in comparison with available national normative data. At baseline, seven of the eight parameters measured (physical functioning, physical problems, bodily pain, subjective health perception, social functioning, emotional problems and mental health) showed a considerable departure from the Australian norms, as evidenced by falling well below 95% confidence intervals.
The SF-36 can also be applied longitudinally to provide an indicator of treatment effectiveness [27]. No individual patient in either treatment group reported a deterioration in health status. Patients who completed the 12-week program, irrespective of treatment group, reported, on average, significant improvement in most of the SF-36 domains (other than vitality in the CBT-only group). Notably, the physical SF-36 domains showed most improvement, all within or above 95% confidence intervals. The value of comparison with national data in this study is that it tracks the movement of program completers from levels of quality of life consistent with a displaced pre-treatment group to approximating those of the population amongst whom they live, posttreatment. This is consistent with treatment benefit.
Alcohol dependence is also associated with diminished mental health functioning, particularly mood and anxiety disorders [30]. The GHQ specifically targets short-term changes in mental health [20] and has been demonstrated as both an efficient and reliable instrument in an Australian setting [31]. It also has been validated as a longitudinal measure of change [32]. Pre-treatment, all of the GHQ-28 subscales of somatic concerns, anxiety, social dysfunction and depression fell significantly below national normative data. Following the 12-week abstinence-based program, all GHQ-28 subscales (apart from depression in the CBT-alone group) fell within or above 95% confidence intervals. These are target areas for CBT and is similarly associated with treatment benefit.
A further objective was to assess whether the addition of the anticraving agent naltrexone could be demonstrated to improve these health status perceptions and sense of wellbeing. For the naltrexone-treated group improvement was less marked on the SF-36 and GHQ-28 subscales. Some of these differences may reflect the participant's self-selection bias. As naltrexone had only recently become available, initial media coverage attracted patients, some were self-referred and highly motivated. By contrast, others referred for rehabilitation through established channels were often less well informed and when offered naltrexone, were guarded or ambivalent about its use. Pre-treatment, the naltrexone group had overall lower (better) average GHQ-28 scores and higher (better) average SF-36 scores than the CBTalone group. Although these pre-treatment differences did not reach statistical significance, the degree of improvement across the treatment program was less marked for the naltrexone-treated subjects. Both treatment groups reported similar SF-36 and GHQ-28 scores post-treatment. Pharmacological factors may have also contributed to poorer post-treatment functioning. The reported new-onset adverse clinical events with naltrexone treatment include nervousness (3.8%), fatigue (3.6%) and anxiety (2%) [33]; however, it is not possible to separate psychological from pharmacological effects.
Our findings should be interpreted with caution. The SF-36 measures how people feel (perception) about their health (physical and mental) while the GHQ-28 is designed to identify short-term changes (‘state over the past few weeks’) in mental health or psychological wellbeing. Important as improvement in perceived health is, this does not always translate into objective improvements in quality of life [14]. However, perceived health has been found to be strongly associated with health care utilization, morbidity and mortality [34]. Equally, the design employed is quasi-experimental in that patients chose between CBT ++ naltrexone or CBT-alone but this reflects the realities of clinical practice. Attrition from substance dependence treatment programs is a welldocumented clinical reality. Here, we report only the health and wellbeing outcomes of those who completed the 12-week program. An additional limitation is the unavailability of follow-up data for those lost to attrition.
Rehabilitation for alcohol dependence is more than the removal of alcohol from patient's lives. The initial success establishing abstinence over the short-term is less likely to be maintained unless there are clear incentives to continue an alcohol-free lifestyle. Enhancing adaptation and coping skills are important components. In this study those who successfully achieved alcohol abstinence and were retained in a CBT program, recorded substantial subjective improvement and approximated reported Australian normative data. As this represents an appropriate outcome parameter in health care in other chronic disorders, it warrants more widespread application to addiction treatments. Adjunctive naltrexone use improved program compliance and abstinence rates but was not demonstrated to enhance patient wellbeing beyond CBT alone.
These improvements in subjective health status and mental health wellbeing occur rapidly, within the first three months of therapy. If confirmed, they have important implications for allocation decisions in health resourcing for the treatment of alcoholism.
Footnotes
Acknowledgements
This study was supported through internal funds.