
Abstract
Objective:
To identify whether mindfulness-based stress reduction is effective in improving physical health outcomes for long-term physical conditions.
Method:
A systematic review of the literature (retrieved from MEDLINE, PubMed and PsycINFO).
Results:
Fifteen studies were included in the review. None of the studies assessed as having a low risk of bias demonstrated significant improvements in physical health status although there was some emerging evidence that mindfulness-based stress reduction may be useful in pain conditions. There was some preliminary evidence that it may also be effective in improving primary insomnia and irritable bowel syndrome. Small to moderate effect sizes were also found for asthma, pain, tinnitus, fibromyalgia and somatization disorders.
Conclusion:
Although there is some preliminary support for the use of mindfulness-based stress reduction in physical health conditions, further research is required before it could be considered an effective intervention for improving physical health outcomes.
Keywords
Background
It is now well established that people with serious mental disorders have higher rates of physical illness and are more likely to experience premature death than the general population (Scott and Happell, 2011; Thornicroft, 2011; Wahlbeck et al., 2011). Many long-term conditions particularly metabolic diseases, cardiovascular diseases, respiratory tract diseases and musculoskeletal diseases are more prevalent in people with serious mental disorders than in the general population (De Hert et al., 2011). Conversely, people with long-term physical conditions experience two to three times the rate of mental health problems than the general population (Naylor et al., 2012). The evidence suggests that at least 30% of all people with a long-term condition also have a mental health problem (Cimpean and Drake, 2011). It has also been estimated that 46% of people with a mental health problem have a long-term physical condition (Naylor et al., 2012). The causal relationship is likely to be bi-directional (Kiecolt-Glaser et al., 2002).
Health service delivery to people with long-term conditions and mental health problems is usually fragmented with primary care funded to treat the long-term conditions and psychiatric services funded to treat mental health problems (Crowe, 2014). The current disconnection between secondary care psychiatric services (which are focused on mental health outcomes) and primary care services, which are often not fully engaged in the physical health care of their patients with mental illness, needs to be addressed as a matter of urgency (Langan et al., 2013). Interventions that take a more integrated approach are obviously needed. Given the high rates of co-occurring long-term physical and mental conditions, they are increasingly likely to be the norm rather than the exception in the future. It is important therefore to identify interventions that may address both. It has been well established that mindfulness interventions are clinically effective for depression and anxiety (Hofmann et al., 2010; Khoury et al., 2013), but given the co-occurrence of these conditions with physical health conditions, are they also effective for physical symptoms?
Mindfulness
Mindfulness can be described as bringing one’s complete attention to the experiences occurring in the present moment, in a non-judgmental and accepting way (Kabat-Zinn, 1990). The original purpose of mindfulness in Buddhism—to alleviate suffering and cultivate compassion—suggests a central role for this practice in health care (Santorelli, 1998). Bishop et al. (2004) have proposed that irrespective of specific techniques mindfulness involves self-regulation of attention and orientation to experience. They describe it as a process that enables thoughts and feelings to be experienced as subjective (vs necessary) and transient (vs permanent).
An effect of mindfulness is that it may modulate subjective experience of pain and disability, thus helping people to cope better (Ludwig and Kabat-Zinn, 2008). It is a form of meditation practice, an attentional stance and a shift in attitude and perspective that allow the person to see her or his long-term condition in a way that is less anxiety-provoking (Kabat-Zinn, 2003). There are many ways that mindfulness may promote self-management of long-term conditions: decreased perception of pain severity; reduced stress, anxiety and depression; diminished need for medication; enhanced ability to reflect on choices; improved adherence to treatment; increased motivation for lifestyle change; enriched interpersonal relationships and social connectedness; and alterations to biological pathways affecting health such as the autonomic nervous system, neuroendocrine function and the immune system (Ludwig and Kabat-Zinn, 2008).
The practice of mindfulness has been integrated into several psychosocial interventions: acceptance and commitment therapy (ACT), mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR). The core conceptualization of ACT is that psychological suffering is generally caused by experiential avoidance and cognitive entanglement, and the resulting psychological rigidity leads to a failure to take needed behavioral steps in accord with core values to enhance well-being (Hayes et al., 2006). ACT is primarily focused on behavior change. MBCT was developed as a psychological relapse prevention treatment for recurrent depression (Segal et al., 2002). It focuses on teaching individuals to accept and observe rather than to react to automatic thoughts and feelings that maintain depression. MBSR was developed specifically to help people manage pain and the stress associated with long-term conditions (Kabat-Zinn, 2003).
This review focuses on MBSR because it does not assume behavior change is required as in ACT and has a broader focus than symptoms of depression as in MBCT. MBSR was developed by Jon Kabat-Zinn (1990), at the University of Massachusetts Medical Center. It is typically an 8-week 1-hour group training intervention with a 1-day workshop and an expectation of practice between sessions. The intervention uses three techniques: (1) body scan, where in a lying position participants are guided to place their attention non-judgmentally on each area of the body, (2) breathing practice and (3) mindful slow walking with focused attention on body sensation and/or breathing.
There is convincing evidence that MBSR can improve depressive and anxiety symptoms (Bohimeijer et al., 2009; Hofmann et al., 2010; Khoury et al., 2013); therefore, these outcomes and conditions were excluded from the review. We were interested in identifying whether MBSR could have a wider effect and also improve physical health outcomes in long-term physical conditions.
Method
A systematic review of the literature was conducted based on the Cochrane method for reviews (Higgins and Green, 2011): developing the review question and developing criteria for including studies (M.C., B.B.), searching for studies (M.C. and research librarian), selecting studies and collecting data (M.C., B.B. independently), assessing and addressing risk of bias in included studies/evaluation of quality (M.C., V.J.), analyzing data and meta-analysis (M.C.), presenting results (M.C.) and interpreting results and drawing conclusions (M.C., D.G., S.H.). Initials relate to the author responsible for each step.
Research question
Is MBSR an effective intervention for improving physical outcomes for people with long-term physical conditions?
Search strategy
Databases searched were Ovid (MEDLINE, and PsycINFO), PubMed and manual searching of reference lists from papers identified by electronic search. The following key words were identified in consultation with a research librarian:
Chronic disease;
Mindfulness;
Long-term conditions;
Intervention studies/or interventions.
Criteria for considering studies
Inclusion criteria are as follows:
Intervention studies;
Adult participants (aged >18 years);
Community-based;
MBSR intervention (or modification based on MBSR principles);
Participants have long-term physical symptoms and/or condition;
Physical health outcomes measured;
Published before August 2014.
Exclusion criteria are as follows:
ACT;
MBCT;
Hospital-based;
Non-English;
Psychiatric long-term conditions;
Depression and anxiety outcomes.
Assessment of relevance for inclusion
The abstracts of all studies identified by the search strategies were examined (n = 499). Those that reported intervention studies were selected for more detailed examination. The full-text versions of these studies were then obtained (n = 42; see Figure 1).
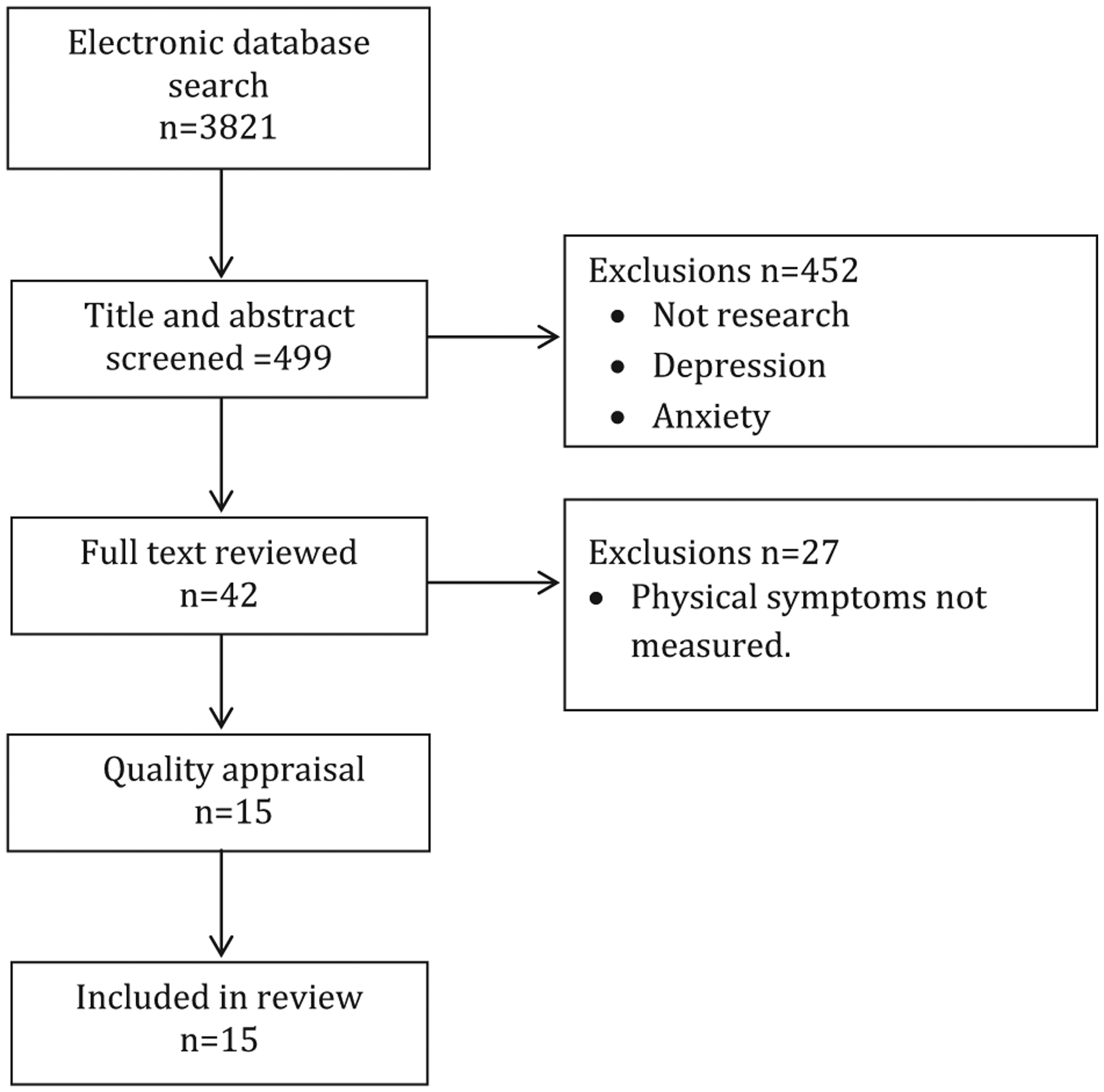
Flow chart of search process.
Assessment of risk of bias
Each randomized controlled trial (RCT) was assessed for risk of bias using the Cochrane Collaboration’s tool for assessing bias (Higgins et al., 2011):
Sequence generation;
Allocation concealment;
Blinding of participants;
Incomplete outcome data;
Selective outcome reporting;
Other sources of bias.
Studies were then assessed as low risk of bias, unclear risk of bias or high risk of bias.
Quality assessment
Assessing and addressing the risk of bias apply to RCTs; however, our review was not limited to these. Other studies that included physical health outcomes were also included and assessed using a dichotomous quality assessment of the following (Crowe et al., 2010):
Are the identified aims congruent with methodology and measurements?
Are sufficient details of treatment and control conditions reported?
Is the sampling method described, if relevant, and are patient demographic characteristics provided?
Have the measures used been validated?
Are there sufficient details of intention to treat and statistical analyses?
Are results presented with sufficient detail to assess significance (where appropriate)?
Do the conclusions reflect the results from the study?
Results
Fifteen studies met the inclusion criteria for this review. Ten studies were conducted in the United States, and the others were one each in the United Kingdom, Denmark, Germany, Hong Kong and Canada. There were 11 RCTs (Brown and Jones, 2013; Fjorback et al., 2013; Gardner-Nix et al., 2014; Gross et al., 2011; Morone et al., 2008; Mularski et al., 2009; Pbert et al., 2012; Plews-Ogen et al., 2005; Schmidt et al., 2011; Wong et al., 2011; Zernicke et al., 2013). The other four studies were pre- and post-test design. Most of the RCTs were not blinded, but there appears to be strong attempts at creating plausible controls in two (Plews-Ogen et al., 2005; Schmidt et al., 2011), while three other studies were not clear about blinding (Mularski et al., 2009; Pbert et al., 2012; Wong et al., 2011). Three RCTs used a wait-list control (Gardner-Nix et al., 2014; Morone et al., 2008; Zernicke et al., 2013): one used treatment as usual as the control (Brown and Jones, 2013), one used ‘enhanced’ treatments as usual (Fjorback et al., 2013) and one used medication as a control (Gross et al., 2011). Two studies employed a three-arm design: MBSR/massage/treatment as usual (Plews-Ogen et al., 2005) and MBSR/relaxation group/wait list (Schmidt et al., 2011). The others had active control arms: support group (Mularski et al., 2009), Healthy Living Group (Pbert et al., 2012) and an education program (Wong et al., 2011).
MBSR is designed to be delivered over 8 weeks and one study had an 8- to 12-week intervention duration (Gardner-Nix et al., 2014); however, most measured outcomes at 8 weeks apart from Fjorback et al.’s (2013) study that had a 15-month follow-up. Physical health status was an outcome in 13 studies with most studies using the Short-Form Healthy Survey 36 (SF-36; Ware et al., 1993) or its other versions. In all, 12 studies measured symptoms using a range of measures specific to the symptoms. Ten studies measured both physical health status and symptoms. Most studies excluded participants with psychiatric illnesses, but exclusion criteria for studies were not extensive (see Table 1 for details).
Study design characteristics.
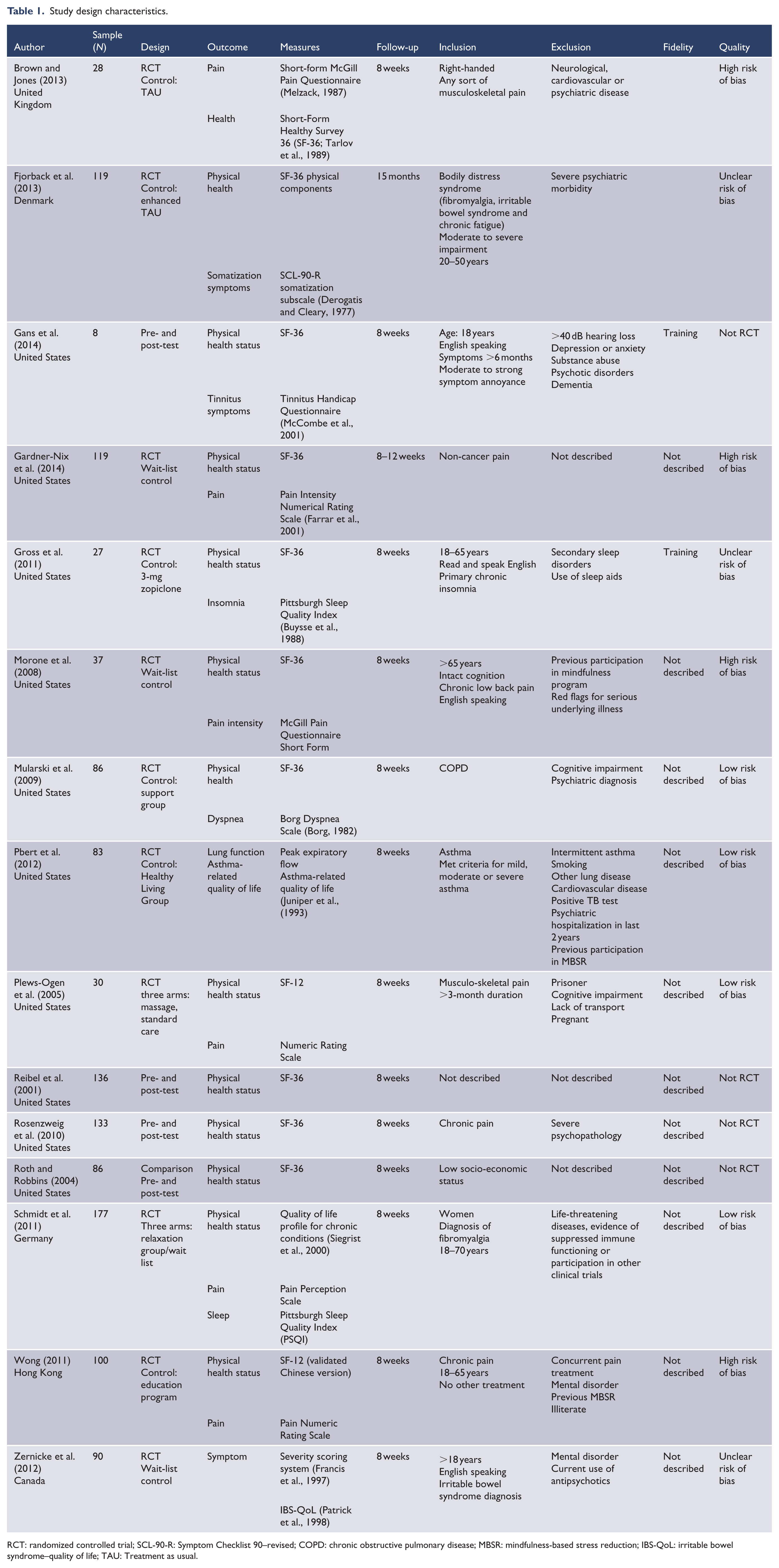
RCT: randomized controlled trial; SCL-90-R: Symptom Checklist 90–revised; COPD: chronic obstructive pulmonary disease; MBSR: mindfulness-based stress reduction; IBS-QoL: irritable bowel syndrome–quality of life; TAU: Treatment as usual.
Risk of bias
Four studies were assessed as having a low risk of bias (Mularski et al., 2009; Pbert et al., 2012; Plews-Ogen et al., 2005; Schmidt et al., 2011), three as having an unclear risk of bias (Fjorback et al., 2013; Gross et al., 2011; Zernicke et al., 2013) and four as having a high risk of bias (Brown and Jones, 2013; Gardner-Nix et al., 2014; Morone et al., 2008; Wong et al., 2011). Those assessed as having a high risk of bias provided inadequate reporting of randomization, allocation and were not blinded. The inability of participants to be blinded to the intervention was the main contributing factor in those with unclear risk of bias. No studies reported adequate fidelity checks for the intervention.
Patient characteristics
The participants had a range of physical conditions predominantly associated with pain, e.g., arthritis, chronic low back pain, fibromyalgia, migraine and also chronic obstructive pulmonary disorder, primary insomnia, hypertension, irritable bowel syndrome, asthma and tinnitus. The mean ages ranged from 38 to 75 years. Most were 45–55 years. Most participants were females; however, two studies had predominantly males (Gans et al., 2014; Mularski et al., 2009). Participants were predominantly described as White although eight studies did not report ethnicity (see Table 2 for details).
Patient characteristics.
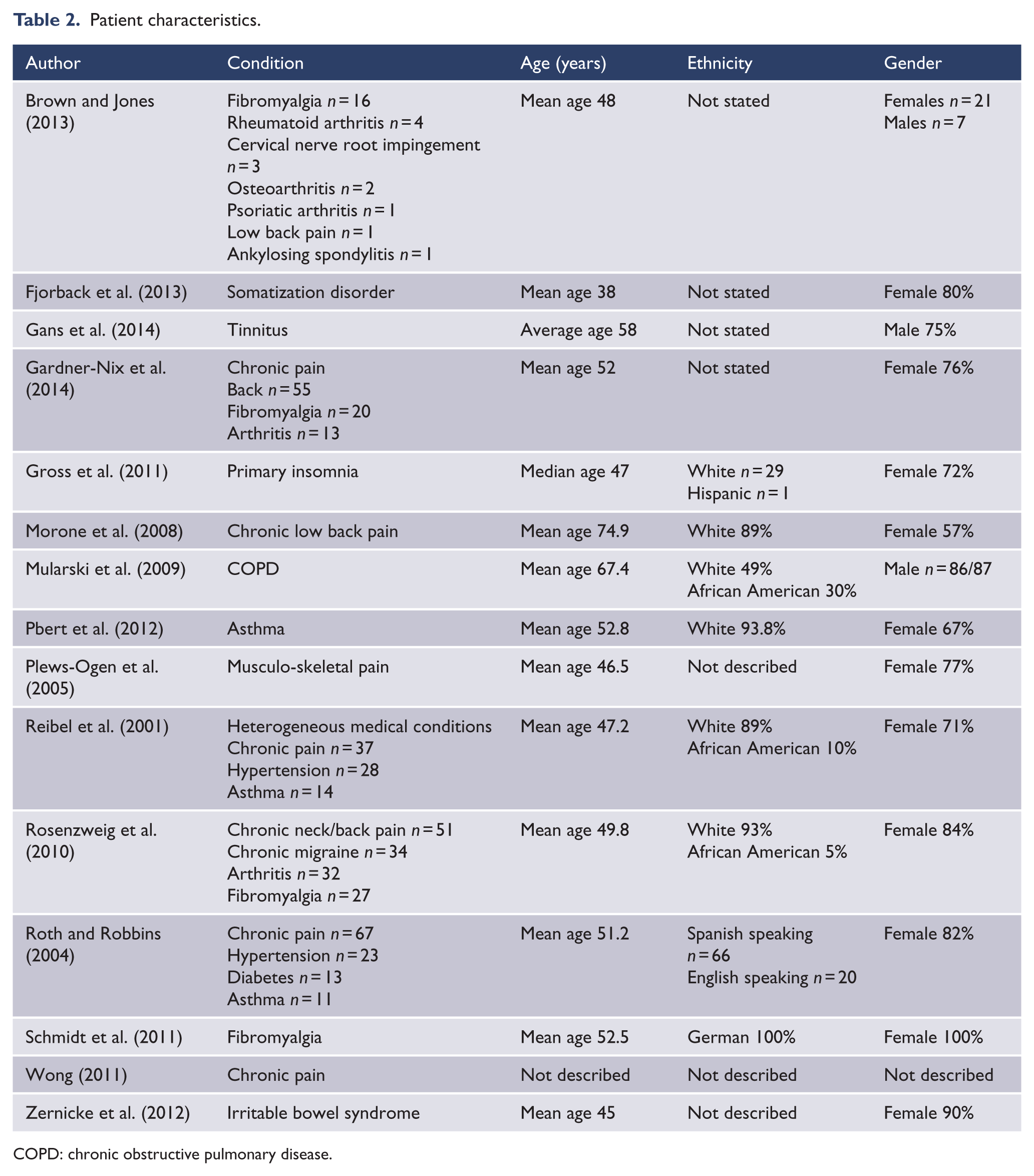
COPD: chronic obstructive pulmonary disease.
Physical outcomes
Most studies identified no significant improvements in physical health status apart from Morone et al.’s (2008), Rosenzweig et al.’s (2010) and Roth and Robbins’ (2004) studies. Two of the studies were able to demonstrate significant improvement in physical symptoms. Gross et al. (2011) demonstrated large statistically significant improvements in sleep, and Zernicke et al. (2013) demonstrated significant differences in irritable bowel syndrome symptom severity. Three studies demonstrated low to moderate effect sizes in symptom measures: a pilot study of tinnitus (Gans et al., 2014), asthma (Pbert et al., 2012) and some pain conditions (Reibel et al., 2001; see Table 3).
Results by outcome measured.
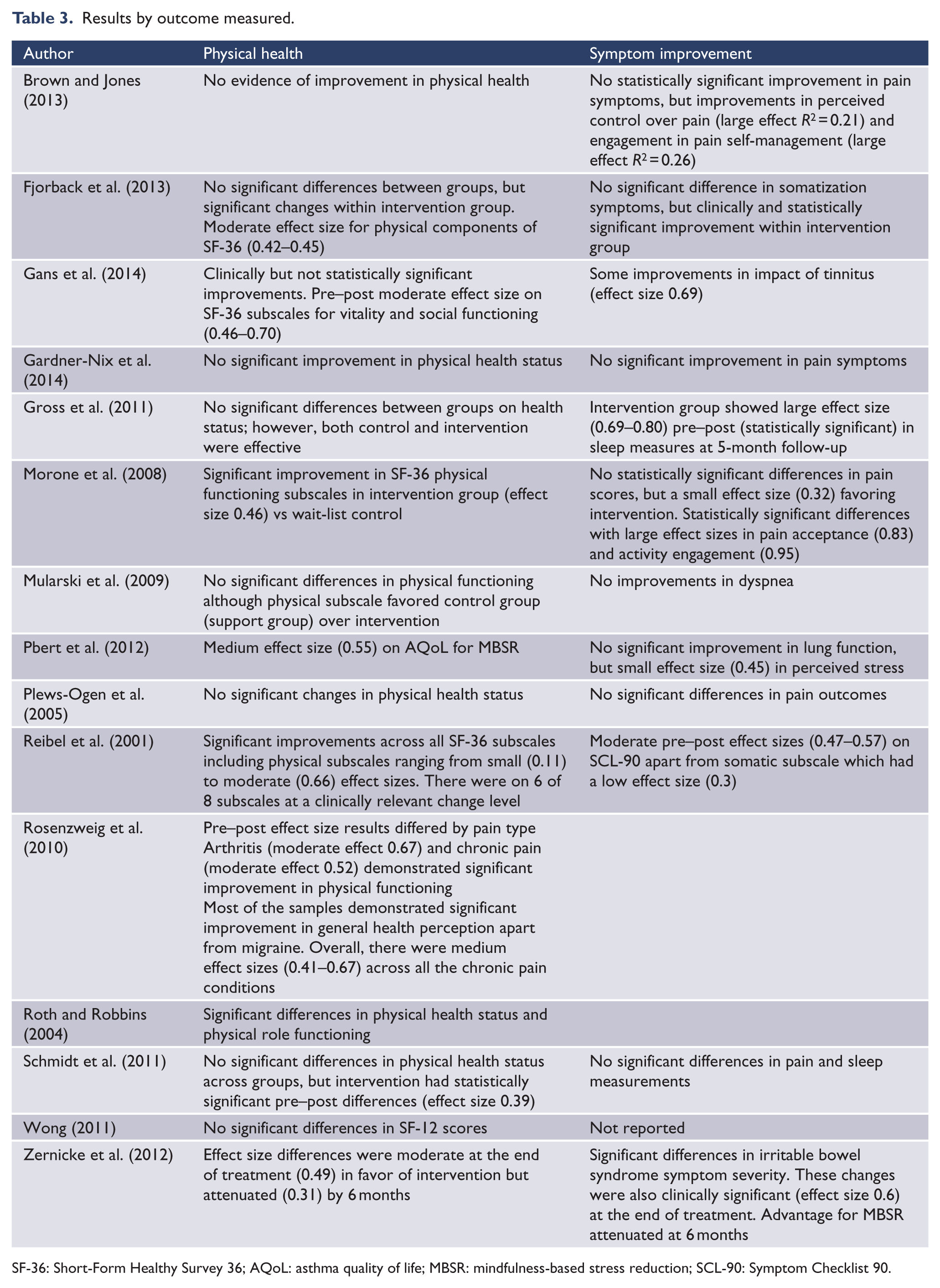
SF-36: Short-Form Healthy Survey 36; AQoL: asthma quality of life; MBSR: mindfulness-based stress reduction; SCL-90: Symptom Checklist 90.
None of the studies assessed as having a low risk of bias demonstrated statistically significant improvements in physical health status outcomes; however, some of the studies with an unclear risk of bias or which were of pre- and post-test design had small to moderate effect sizes. Pbert et al.’s (2012) study of asthma had medium effect sizes (0.55) in favor of MBSR; Schmidt et al. (2011) demonstrated statistically significant pre- and post-improvements in the MBSR group receiving treatment for fibromyalgia; and Fjorback et al.’s (2013) study demonstrated moderate effect sizes for somatization disorders.
Discussion
The potential for MBSR as an effective treatment for long-term physical conditions is only just beginning to be investigated with 80% of the trials in this review published in the last 5 years. Our review suggests that there is some emerging evidence that MBSR may be a clinically effective intervention for improving physical health status (functional health and well-being) in chronic pain conditions, irritable bowel syndrome, asthma, fibromyalgia and somatization disorders. There is also some emerging evidence that it may be effective for the treatment of symptoms of irritable bowel syndrome, insomnia, tinnitus and lower back pain. These improvements may relate to what Ludwig and Kabat-Zinn (2008) hypothesized as a modulation of the subjective experience of symptoms which enables better coping. While psychological symptoms were not the focus of this review, it is of note that most of the studies were able to demonstrate improvements in these subscales.
Another meta-analysis conducted by Grossman et al. (2004) that included a range of both physical and psychological conditions, both acute and long term, found a consistent and a relatively strong level of effect size across a range of very different conditions. They suggested that mindfulness training might enhance general features of coping with distress and disability in everyday life, as well as under more extraordinary conditions of serious disorder or stress. Support for the use of MBSR in clinical populations for people with co-occurring physical and psychological symptoms has been identified by Hofmann et al. (2010) who proposed that the effects of mindfulness therapies may not be diagnosis-specific but may address transdiagnostic processes occurring in multiple disorders. It may improve the experience of physical symptoms by improving the emotional and evaluative dimensions that underlie general aspects of well-being.
While there is a short history of studies of MBSR for physical outcomes and limited evidence of its effectiveness, there is increasing interest in its potential. Several studies have identified somatic responses during meditative practices (Jevning et al., 1996; Lou et al., 1999). Rosenkranz et al. (2013) used the Trier Social Stress Test involving the topical application of capsaicin cream to the forearm and found that following MBSR, participants had reduced stress-evoked cortisol levels, psychological distress, physical symptoms and a significantly reduced post-stress inflammatory response. Davidson et al. (2003) have also reported enduring brain and immune function effects following an 8-week mindfulness intervention. They found significant increases in left-sided anterior cortex activation, a pattern previously associated with positive affect along with increases in antibody titers to influenza vaccine. The magnitude of increase in left-sided activation predicted the magnitude of antibody titer rise to the vaccine. Creswell et al. (2012) found that in addition to reducing loneliness, MBSR was also found to downregulate pro-inflammatory gene expression and suggested that this may be the mechanism that reduces stimulated pro-inflammatory cytokine production found in a study of MBSR for people with breast or prostate cancers (Carlson et al., 2007). Gallegos et al. (2013) identified that following MBSR, older adults had higher post-treatment insulin-like growth factor-1 (IGF-1) levels and reduced antigen-specific immunoglobulin responses.
Research implications
Further well-designed trials of MBSR for long-term physical conditions that are adequately powered, have an active control and incorporate measures of treatment integrity are required to conclusively ascertain its effectiveness. Treatment integrity measures are needed to ensure that the intervention is delivered competently and demonstrates fidelity to the treatment manual. Further research into somatic changes associated with MBSR such as inflammatory markers, vital signs and brain and immune function is also required to add to the growing body of evidence of changes occurring at a biological level. The evidence base would also be improved if more follow-up studies were undertaken to ascertain whether any changes are enduring. Follow-up measures need to be conducted subsequent to conclusion of treatment although Khoury et al. (2013) found that follow-up outcomes at 3 months and 3 years (weighted mean values, 28.92 weeks) were largely similar to those at the end of treatment. It would, however, be useful to know whether this sustained improvement was due to on-going use of MBSR strategies.
It would be useful for consistent evaluation across studies if the SF-36 or SF-12 (Tarlov et al., 1989) was used to measure physical health status. The strengths of the SF-12 measure are its brevity and the availability of norms across medical conditions (Larson, 2002). The SF-36 provides more nuanced measurement and is relatively quick to complete. Symptom measures need to be disease-specific, but alongside objective measures such as lung capacity, blood pressure and pulse, it would be useful if well-established self-report measures were consistently used where relevant, e.g., Short-form McGill Pain Questionnaire (Melzack, 1987) and Pittsburgh Sleep Quality Index (Buysse et al., 1988).
The issue of choice of control group is somewhat more complex. In this review, four studies used treatment as usual or wait-list control, but six had active controls. MacCoon et al. (2012) have suggested that a well-designed control should include (1) a positive expectation for intervention success by both the therapist and the client, (2) a therapeutic relationship, (3) provision of a plausible therapeutic rationale and (4) some corresponding action for alleviation of symptoms (specific ingredients). However, the more active the treatment, the more difficult it is to detect differences as both groups improve. The other issue is that controls cannot always be blinded—patients will know what intervention they are receiving and could be expected to access the Internet or other resources to discover the likelihood of its efficacy. One control identified in this review that appeared to have all the necessary characteristics of an active control was the Healthy Living Group (Pbert et al., 2012) that was used for the treatment of asthma.
Clinical implications
MBSR provides those working with people with both mental health problems and long-term physical conditions a useful adjunctive intervention that has the potential to improve physical health and is acknowledged as improving psychological health. It is potentially a cost-effective intervention as MBSR is usually delivered in eight 1-hour sessions in a 1-day group format workshop. There are many supporting resources freely available on-line, in hard copy or in audio formats for little if any cost. Training in MBSR from recognized training providers would be a minimal requirement in order to deliver the intervention along with adequate regular supervision.
Future studies of MBSR for physical conditions could focus on clinical effectiveness to ensure the clinical utility of the intervention. March et al. (2005) have proposed that for trials to have practical utility in the clinical environment, they should have the following characteristics: (1) questions must be simple, clinically relevant and of substantial public health importance, (2) the trials are conducted in clinical settings, (3) study power is sufficient to identify small to moderate effect sizes, (4) patients must be randomly allocated, (5) there must be uncertainty over which treatment is preferable, (6) outcomes are simple and clinically relevant, (7) assessments must be simple and straightforward and interventions typical of everyday practice, and (8) subject and investigator burden associated with the research goals must be minimized.
Conclusion
MBSR is an intervention that integrates both physical and mental health. Further research into physical outcomes from MBSR is required before it could be considered an effective intervention for long-term physical conditions that frequently co-occur with psychiatric conditions. There is some evidence from this review that MBSR has a positive impact in reducing the daily impact of long-term physical conditions and that for some conditions such as primary insomnia an irritable bowel syndrome improvement in physical health status is reported after MBSR treatment. Further research is required into the effect of MBSR on long-term physical conditions and its physiological effects. Given the evidence from previous reviews for its effectiveness on the psychological effects of long-term conditions, it should be considered for use in clinical practice.
Footnotes
Declaration of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.