
Abstract
The association between medical illness and psychiat-high in some illnesses. Thus, in asthma, anxiety disorder ric and psychological morbidity was noted even in his-has been quoted as between twice and eight times more torical times [1, 2] and this was taken up by the common than in the general population [16] and the rate psychoanalysts of the last century [3–13]. More recent of depression after stroke is up to 60% [17]. Current and more systematic work has confirmed the increased paradigms include cognitive distortion [18], lack of incidence and prevalence of emotional disturbance social support [19] and what Toombs has called the comorbid with medical illness [14, 15]. This is especially ‘unshareability’ of illness [20].
It would seem then that psychotherapy might have an important role in the treatment regimen of the medically ill. However with the expectation of a clear evidence base for all interventions [21], the need for studies of adequate methodological quality in the area has become paramount.
This overview attempts to delineate issues of importance, as well as to provide a review and critique of some of the studies of psychotherapy for patients whose primary illness is physical in nature.
Method
The overview was conducted based on the following premises:
Psychotherapy is a form of communication between therapist and patient, informed by a theoretical base and with the aim of relieving or treating emotional distress or morbidity. Massage therapy, hypnosis, writing therapy and biofeedback have been excluded. Education and behavioural training are only included where a psychotherapeutic component is integral or added. Thus teaching of breathing techniques alone would be excluded, whereas breathing training as part of a cognitive behavioural treatment is included. To enable the literature to be properly understood, only English language studies have been included. So-called functional disorders, such as irritable bowel, chronic pain, chronic fatigue and pseudoseizures, are not regarded as primarily physical illnesses and are therefore excluded.
The data bases searched were MEDLINE, PsycINFO, Cochrane DSR, ACP Journal Club and DARE, using terms for the various illnesses plus ‘Medical Illness’, ‘Chronic Illness’ and ‘Physical Illness’ combined with ‘Psychotherapy’. However, because of the very broad extent of the field being studied, systematic inclusion of all relevant work was impossible.
Results
Illnesses selected for psychotherapy
There is a considerable difference in the frequency with which psychotherapy is used from one illness to another.
This is illustrated in Table 1. It is immediately apparent that the increased level of interest in one illness over another is mostly haphazard. For example, the extensive literature on breast cancer lies in contrast to a virtual absence in the field of bowel cancer. In the field of transplant medicine, the high level of analytic interest in the early years [22, 23] has been only sporadically matched more recently in renal [24] and lung transplants [25], despite a high level of recognized need [26–28]. There is also a surprising dearth of work in the field of neurological illness [29–35].
Randomized controlled trials of psychotherapy medical illness
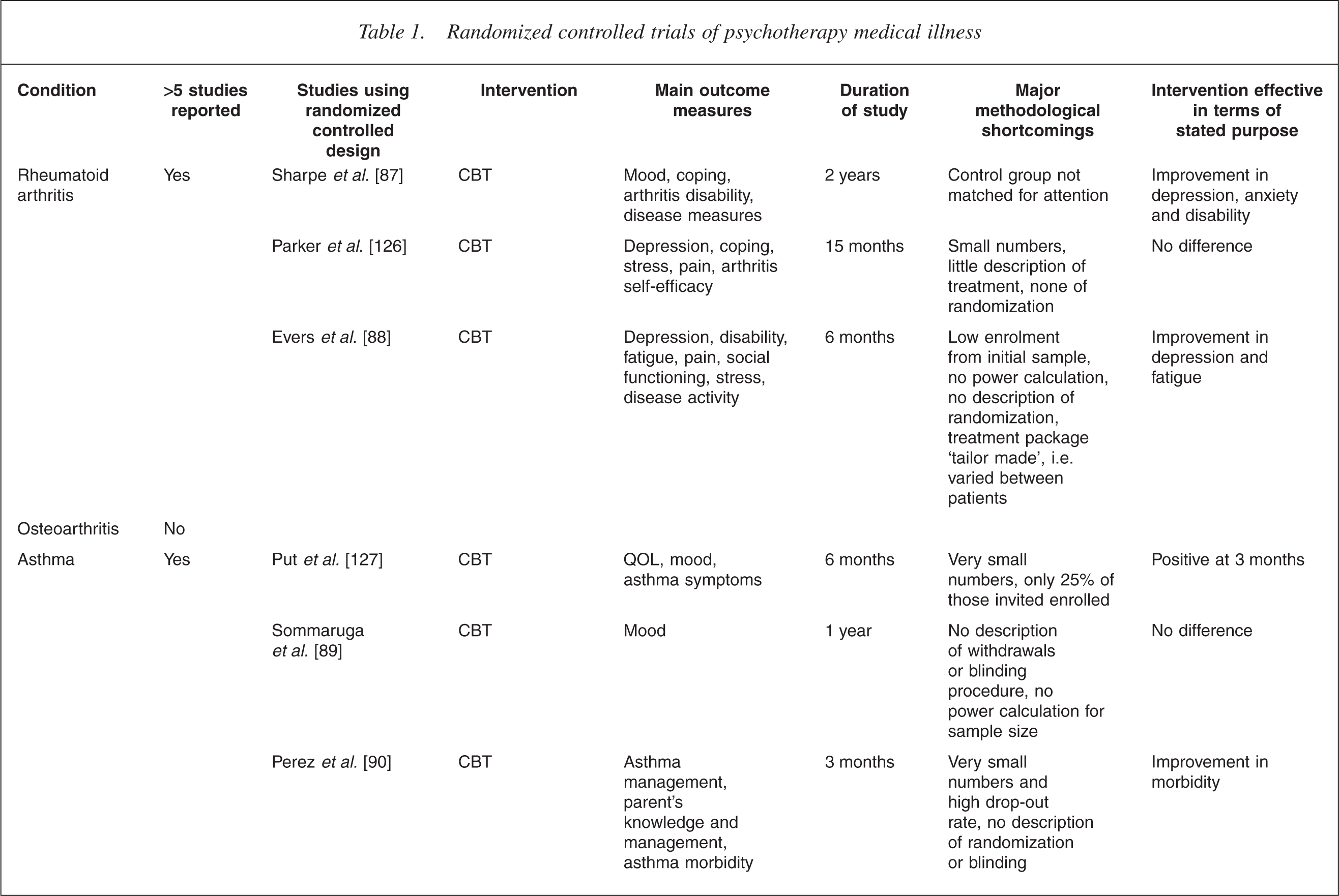
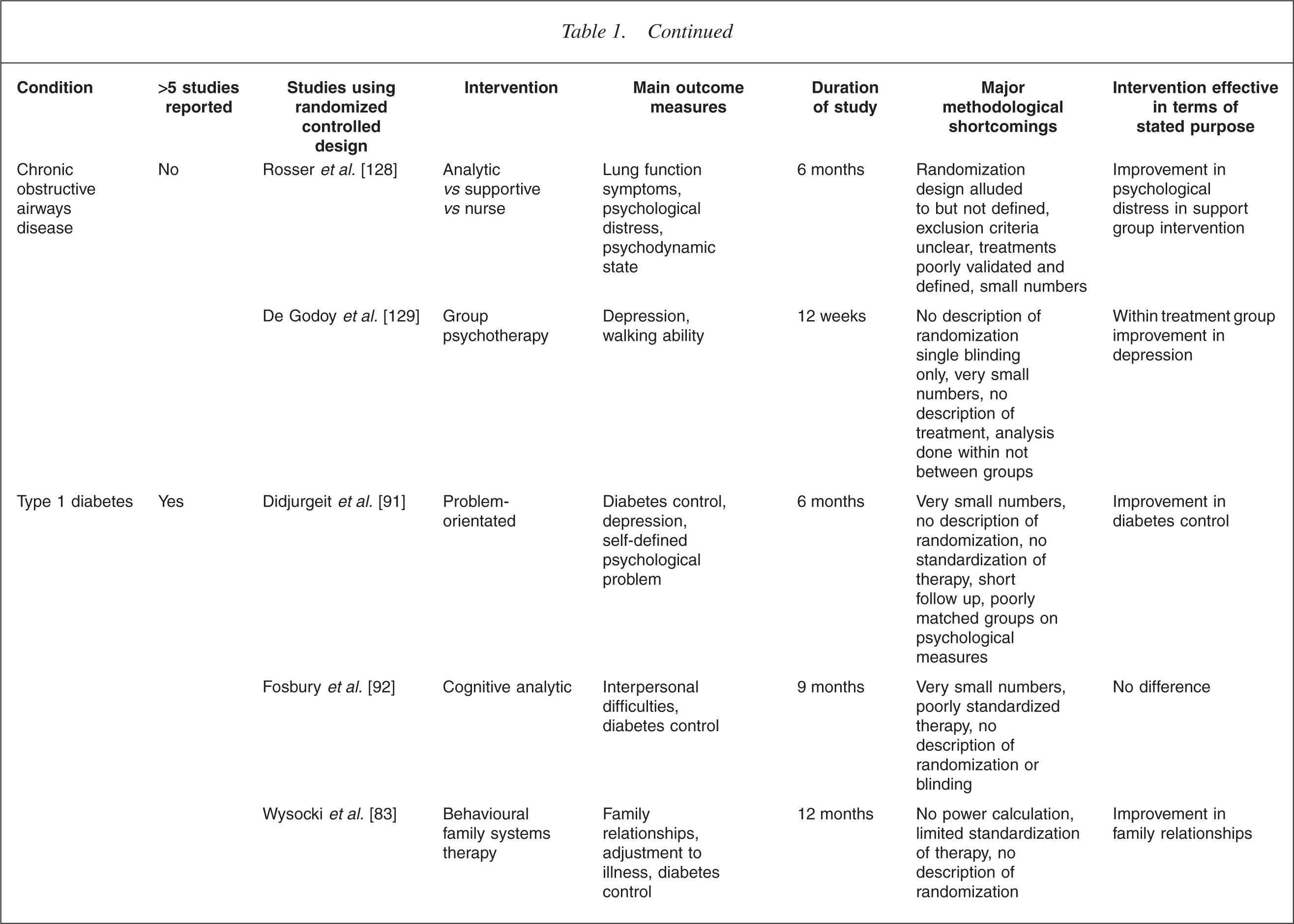
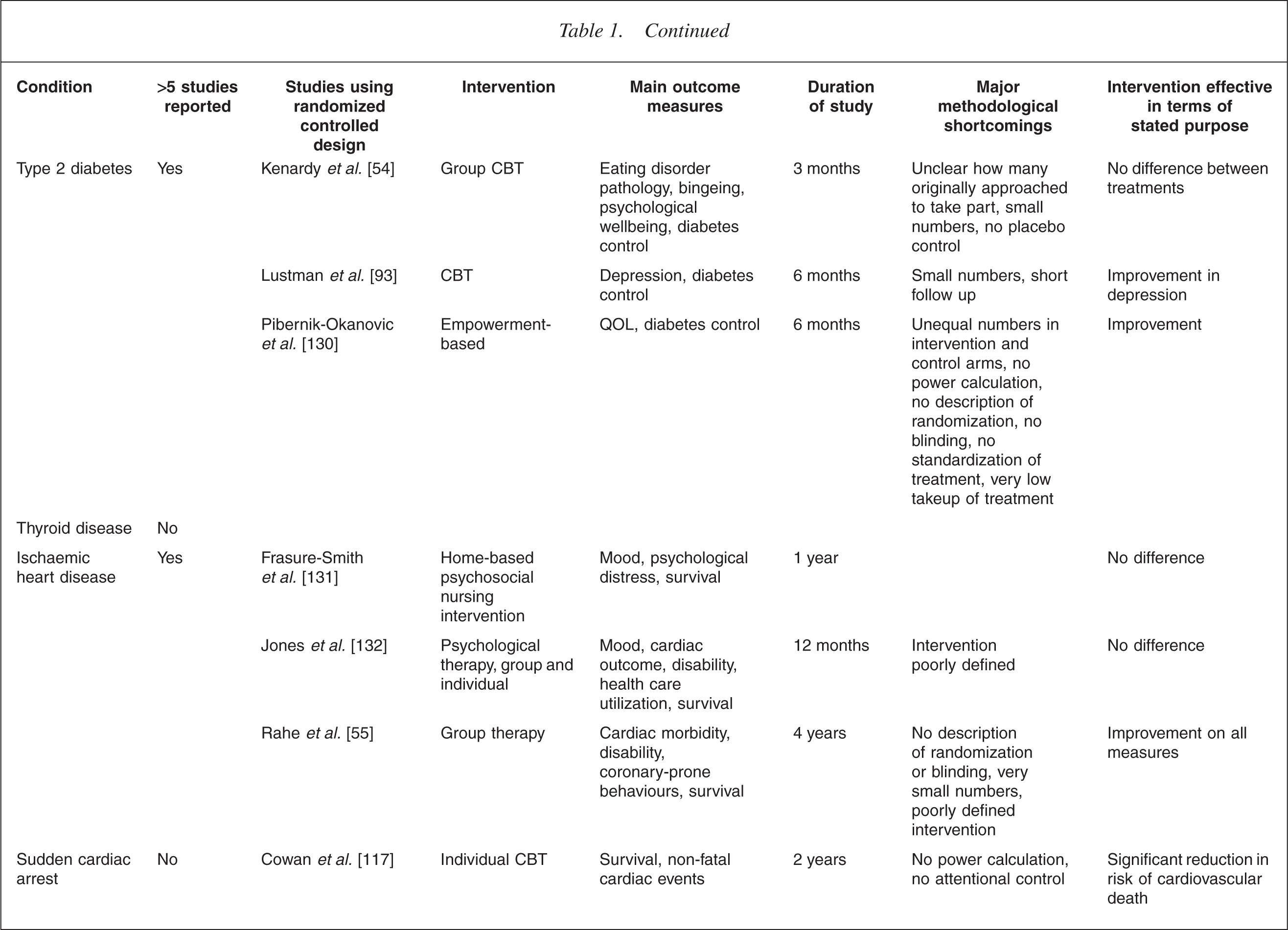
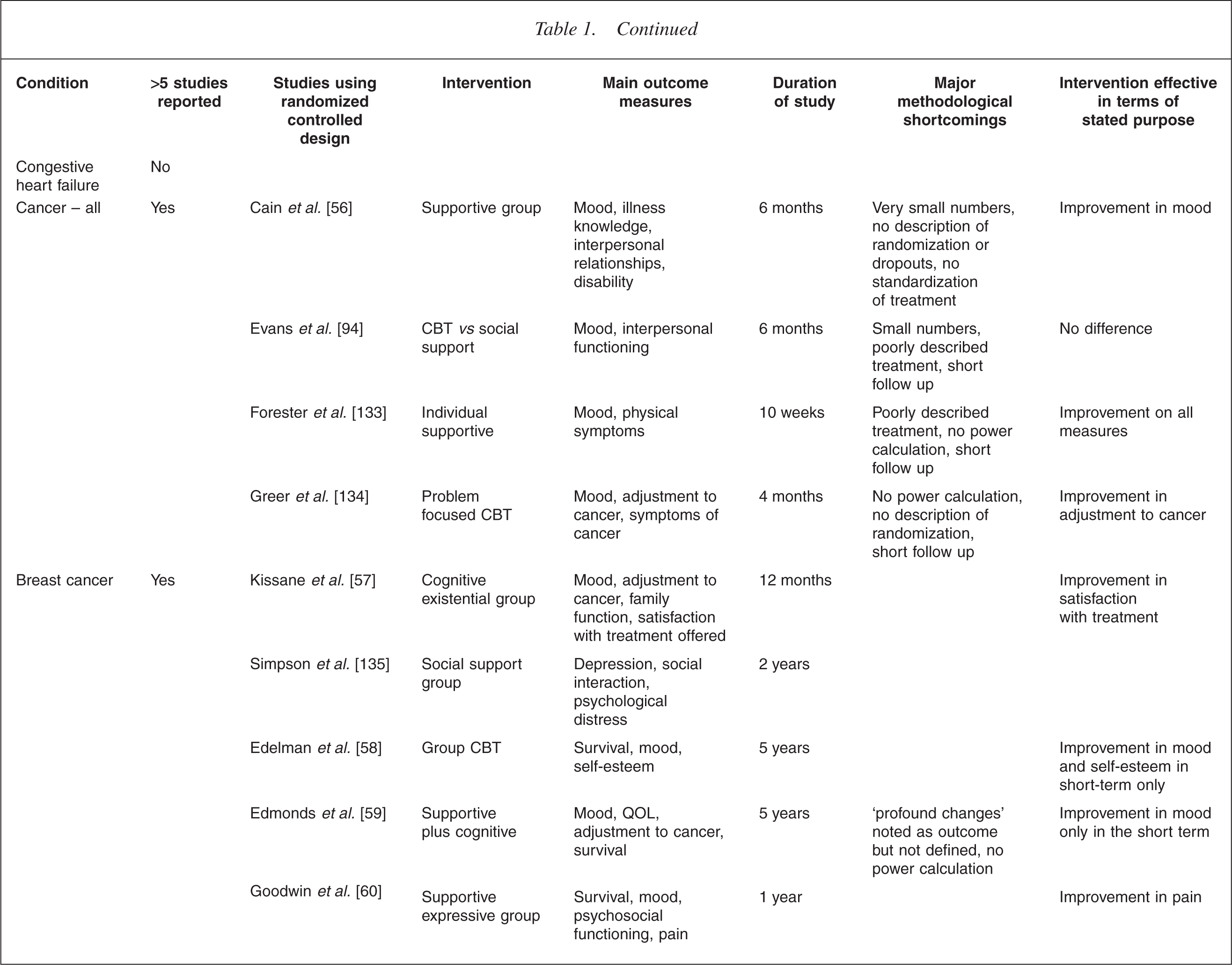
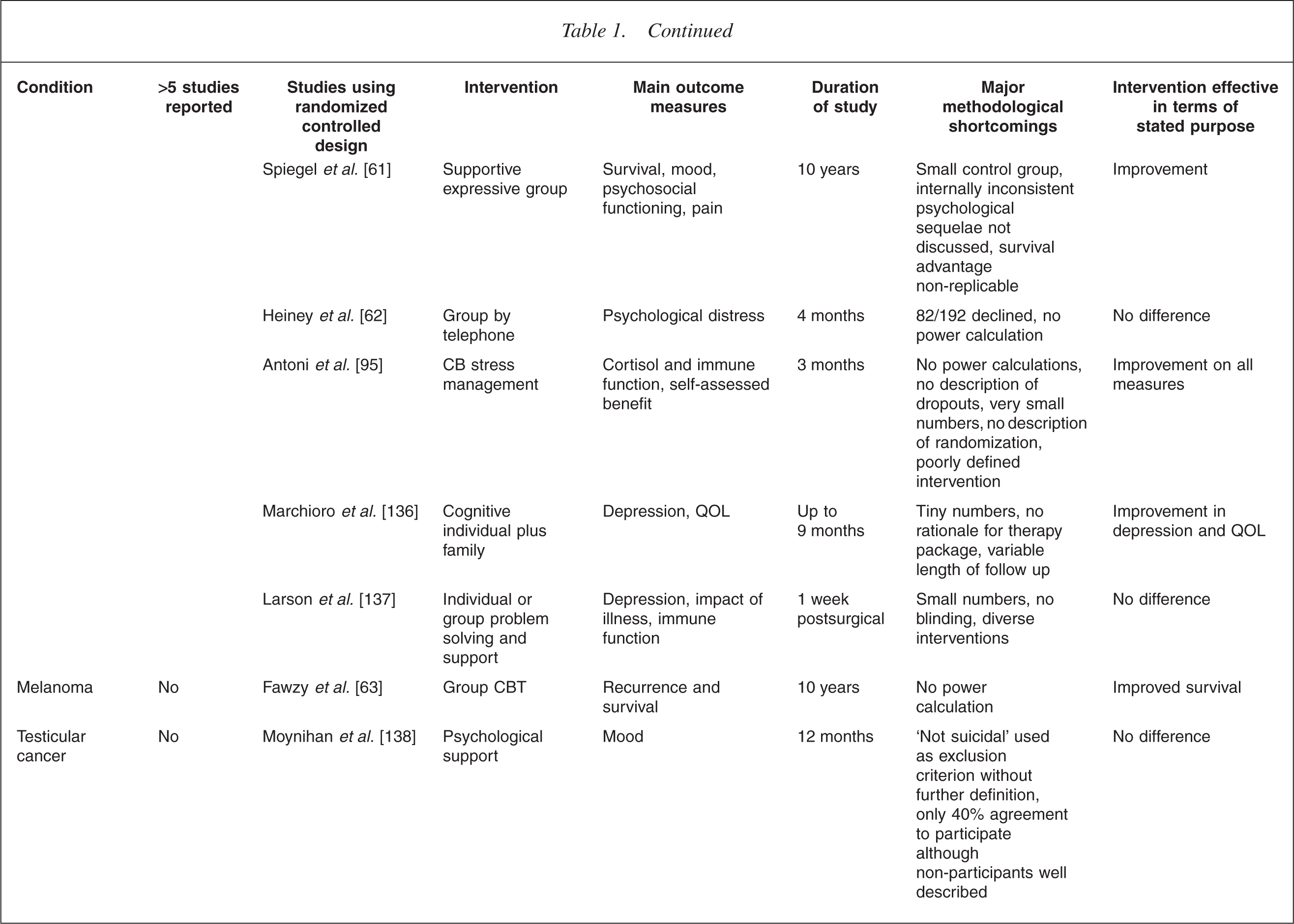
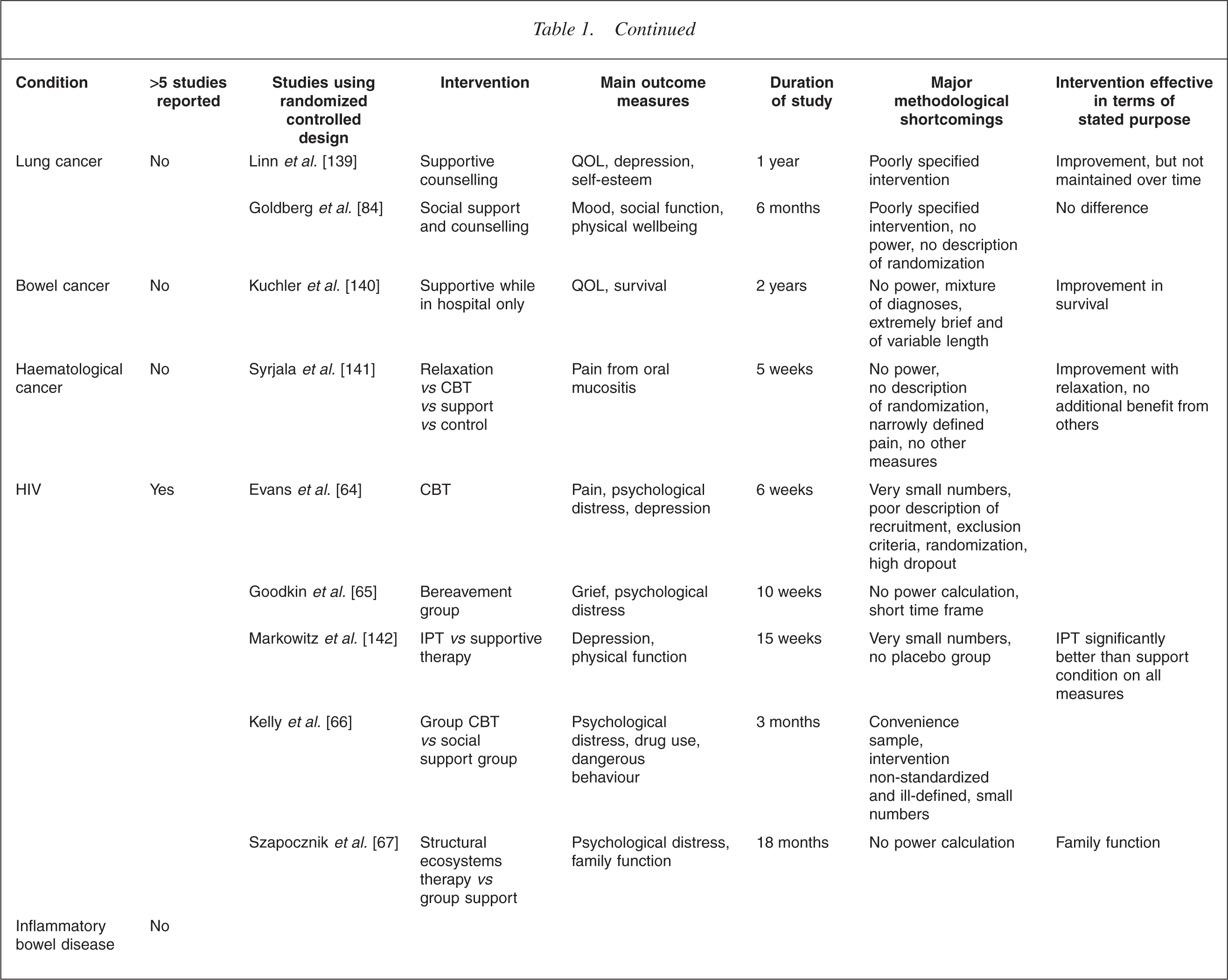
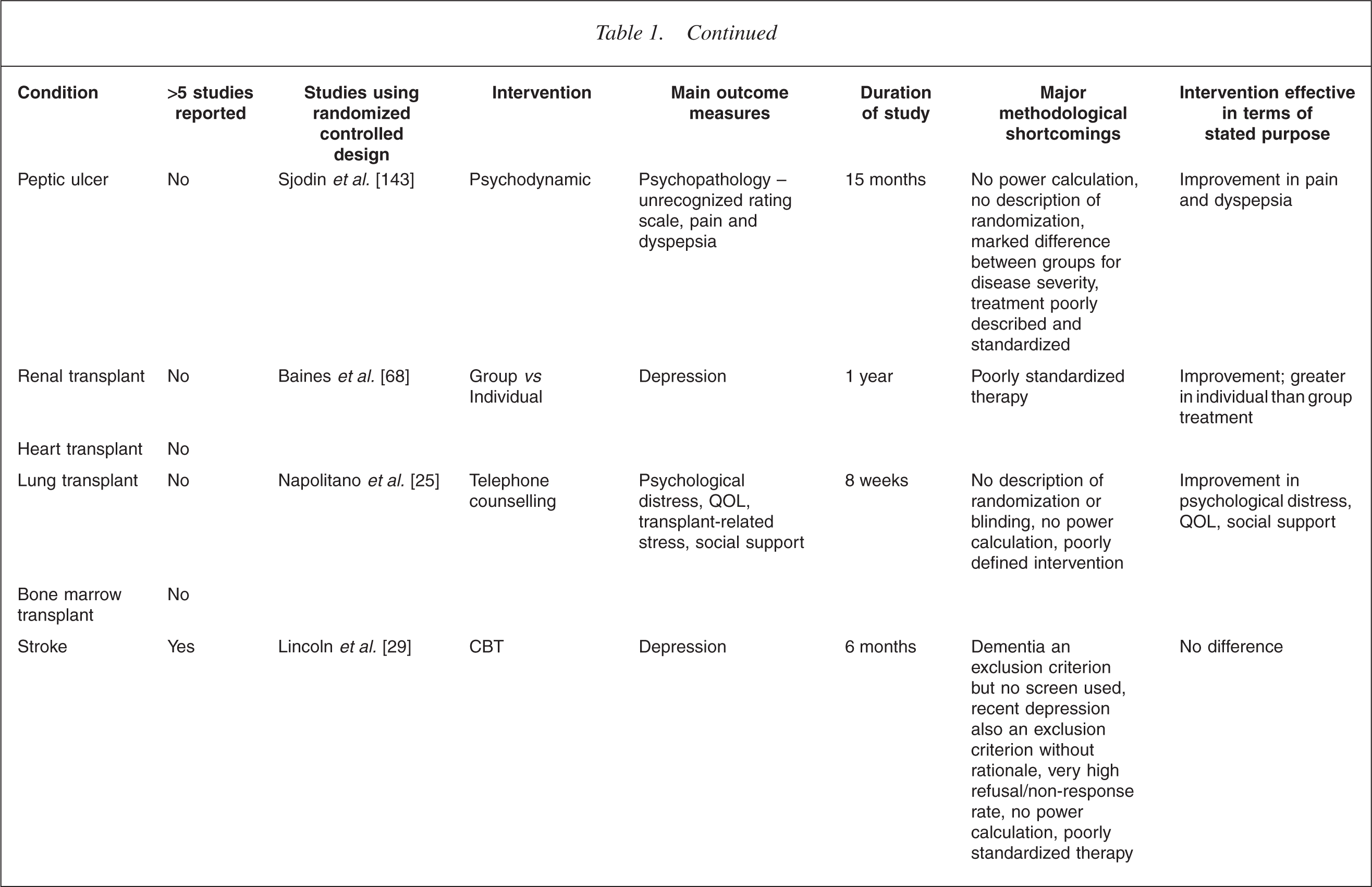
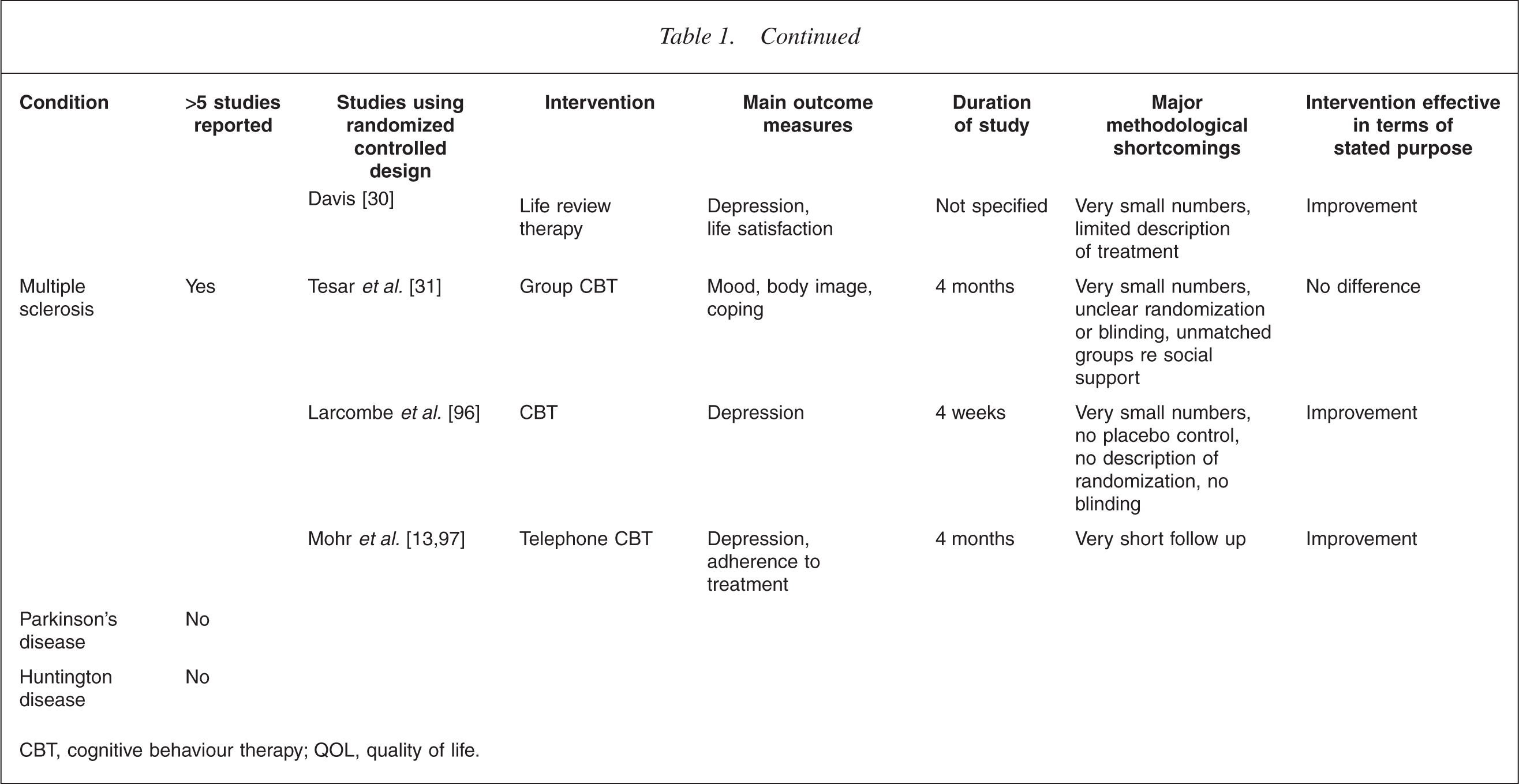
CBT, cognitive behaviour therapy; QOL, quality of life.
Finally, the need for specific studies looking at the psychotherapeutic needs of children and adolescents has been only partially recognized [36–39].
Outcome measures selected
In what remains a superb review, Fries describes five domains in which an outcome measures choice must be made [40]. Of these, the two of most relevance to chronic physical illness are the choice between use of numeric as opposed to more subjective variables, and how long a timeframe will be used. Exclusion of the patient experience in favour of ‘hard’ measures leads to the error described by Kleinman [41] of confusing the priorities of doctors with those of patients; using a short timeframe is virtually meaningless in the timeframe of an illness which may span a lifetime.
There are two main categories of outcome. The first relates to psychological factors such as depression or anxiety, coping, social interaction, self-esteem or quality of life. Despite the clear expression from patients that such subtle issues as body image, sexuality and selfesteem have considerable impact on their wellbeing [42, 43], the difficulty in valid measurement means that they are rarely included. The second concentrates on disease markers including self-management, physical functioning and survival.
Table 1 summarizes the outcome measures used in controlled studies.
Interventions
The most basic issue to be considered in terms of interventions is whether the medically ill require different treatment from the medically healthy in any way [44, 45]. Clearly, good doctor–patient communication is an essential starting point for any psychosocial intervention, though often not achieved [46, 47]. Without understanding their illness, it is impossible for patients to begin problem-solving, or developing coping strategies, much less managing the process of grieving and coming to terms with their altered selves and lives – the essential tasks of managing illness.
Minden in her excellent review of psychotherapy in multiple sclerosis [48] raises a number of points, suggesting that different techniques may be required. She notes that there are often distinguishing features in the treatment of the medical patient, from the referral which may come from the doctor rather than the patient, to concerns relating to whether the therapist comprehends the particular issues raised by illness. Furthermore, the frame may need major adaptation to the specific, and changing, needs imposed by sickness and disability. There is also the issue of which patients in the end follow through with psychotherapy, and which drop out, or choose not to have it, and which groups of patients may need special treatment of one kind or another to prevent this. In the only study found which looks systematically at this question [49], the only predictor of dropout was depression – a finding with worrying implications.
The earliest kind of intervention used for physically ill patients was, as described above, psychoanalysis. Its claims to success were almost entirely based on case reports [8, 10, 13, 50].
Surprisingly, despite its promising results in functional bowel disease interpersonal psychotherapy has rarely been studied [51–53].
Group psychotherapy, providing a chance to share experience, has obvious advantages and has been frequently used, either in a supportive or a cognitive behaviour therapy format [9, 31, 32,54–82]. Family therapy and therapy for family members acknowledges the burden illness places on carers [9, 76, 78,83–86].
In the realm of individual therapy, cognitive behavioural therapy has emerged as promising, relating both to the need for patients to assimilate considerable amounts of information, and the relative ease of standardizing the therapy for research purposes. Interventions target coping, stress management, education and interpersonal support [29, 38, 57, 58, 66, 70, 78, 79, 83,87–105].
Finally, there has been the recent development of existential and spiritually based psychotherapy. This draws from the work of existentialists like Victor Frankl [106] and attempts to explore possible personal meanings that may be found in illness [77, 107, 108].
Methodological issues
Psychotherapy research is a challenging endeavour [21, 109] and the presence of physical illness creates another level of complexity [81,110–112].
The most fundamental issue is the choice of patients to enrol. In the physically ill, except where depressive or anxiety disorders are being treated, there are no clear parameters for who should be offered psychotherapy. Perhaps because of this, the takeup of an offered psychological intervention is low and dropout is high [81], even where patients had initially expressed a need for such a service [113, 114]. Those who do use such therapy are mostly white, educated and middle class, making generalizability questionable [114]. The second major shortcoming relates to sample size. This has been almost uniformly too low, and rarely determined by power calculations. For example, a review of psychotherapy for adults with asthma [115] found only one study with a sample size of over 100. This study in fact used only music therapy [116] rather than psychotherapy as defined in this paper. Methods of randomization and blinding are often not specified and sometimes clearly inadequate. Finally, variations in factors such as medication and other comorbid medical conditions makes the construction of control groups problematic.
Studies using survival as the main outcome measure have been particularly difficult to interpret. For example, the study of a cognitive intervention in survivors of sudden cardiac arrest, showed a significantly reduced mortality of 86% in those receiving therapy despite no measured difference in most of the psychosocial variables measured [117]. Other claims to effects on survival have proved impossible to replicate [60, 118]. Table 1 presents a summary of some of the more prominent examples of randomized controlled research in the area, providing a snapshot of the issues described above.
Discussion
This review has covered a large and complex area, and in doing so has necessarily summarized and abbreviated many issues. Capturing all articles in the field was impossible. The decision to include only psychotherapy as narrowly defined, left out some interesting and useful work using educational interactions or relaxation methods. The exclusion of non-English papers introduced a bias away from psychoanalytically based therapies. However, some conclusions do emerge.
First, it is still not clear who will warrant psychotherapeutic intervention. Certainly, patients with anxiety or depression deserve the same level and quality of care whether or not they have comorbid medical illnesses [104,119–122], and this implies the need for better understanding of these disorders by the health-care team; currently recognition is low [119, 121]. However, the need for psychotherapy for the purposes of emotional adjustment in the absence of psychiatric illness has not yet been established. The diagnosis and ongoing trajectory of illness create a variety of psychological challenges to patients [120], but there is no clear understanding of how to separate out the groups of patients who might benefit from psychotherapy from those who will do perfectly well with standard care alone. Bereavement research shows that most people will grieve normally, with only a subgroup developing pathological responses requiring treatment [85, 123]. By analogy, it is likely that most people confronting the various losses created by illness will manage using their own resources.
Second, there must be a systematic attempt to find which interventions work, with attention to the question of which components may constitute the ‘active ingredient’ [124, 125] and whether these therapies need to be disease-specific, or whether they can be generalized from one illness to another.
Third, to determine the effectiveness of interventions, greater attention will need to be paid to the economic feasibility of introducing interventions in the medical setting. Brief therapies administered by members of the medical health team show promise as being accessible and attractive enough to become part of the repertoire of treatments. Group interventions, for which the evidence base is beginning to emerge, provide advantages at an economic level.
Increasingly, it seems unlikely that illness can be cured or survival lengthened simply by tending to the psyche – the ‘fool's gold’ of some research [71]. Attempts to demonstrate this have been too patchy, and too difficult to replicate.
In summary, the case for psychotherapy as an automatic adjunct to medical treatment has not yet been established. Nor is there sufficient evidence that psychotherapy can play a meaningful role in indices of survival. However, in the presence of the high levels of psychiatric illness and psychological distress accompanying physical illness, there is urgent need for well-designed and methodologically sound studies addressing the question of which interventions should be directed to whom and how they are best delivered.