
Abstract
Objective:
Research has suggested that sexual minority young people are more likely to have depressive symptoms or depressive disorder, but to date most studies in the field have relied on convenience-based samples. This study overcomes this limitation by systematically reviewing the literature from population-based studies and conducting a meta-analysis to identify whether depressive disorder and depressive symptoms are elevated in sexual minority youth.
Method:
A systematic review and meta-analysis were conducted and informed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement to determine if rates of depressive symptoms or depressive disorder differ for sexual minority youth, relative to heterosexual adolescents. MEDLINE, PsycINFO, EMBASE and ERIC databases were searched. Studies reporting depressive symptom data or the prevalence of depressive disorder in population-based samples of adolescents, which included sexual minority youth and heterosexual young people, were included in the review. A meta-analysis was conducted to examine differences between groups.
Results:
Twenty-three articles met the inclusion criteria. The proportion of sexual minority youth in the studies ranged from 2.3% to 12%. Sexual minority youth reported higher rates of depressive symptoms and depressive disorder (odds ratio = 2.94, p < 0.001 and standardized mean difference, d = 0.39, p < 0.001) in comparison to heterosexual young people. Female sexual minority youth were more likely to report depressive symptoms when compared to male sexual minority youth (standardized mean difference, d = 0.34, p < 0.001). Limitations included variations in how sexuality was operationalized and how depressive symptoms or depressive disorder was measured.
Conclusions:
There is robust evidence that rates of depressive disorder and depressive symptoms are elevated in sexual minority youth in comparison to heterosexual young people. Despite the elevated risk of depressive symptoms or depressive disorder for sexual minority youth, the treatment for this group of young people has received little attention.
Introduction
Depressive symptoms are common among young people, and depressive disorder is a major risk factor for youth suicide (Malhi et al., 2015; Thapar et al., 2012). Depressive disorder is also costly at a societal (Murray and Lopez, 2013) and at an individual level (Brière et al., 2015; Fergusson and Woodward, 2002). As a group of young people, sexual minority youth (i.e. lesbian, gay and bisexual [LGB] individuals, those that are not exclusively heterosexual, and people not sure of their sexual attractions) are thought to be at an increased risk of depressive symptoms (Marshal et al., 2011). It has been hypothesized that sexual minority youth are more likely to have depressive symptoms or depressive disorder because of the stress of being in a group that is in the minority and because of the stigma, discrimination and victimization they experience as a result of homophobic and biphobic cultures (Bariola et al., 2016; Denny et al., 2016; Meyer, 2003). If this is so, then targeted interventions that address mistreatment such as bullying, which has a sizeable impact on adolescent mental wellbeing (Ford et al., 2017), as well as focusing on depression in this group is warranted.
It is important to consider how sexuality is defined because this requires an appreciation of certain developmental factors. For instance, adolescents in high-income countries mostly report not having had sexual intercourse (Clark et al., 2013), as such using sexual behaviour as the primary means of determining adolescent sexuality is limited. Sexual identity labels, such as lesbian, gay, bisexual and straight/heterosexual are frequently used by adolescents (Russell et al., 2009), yet many young people who are not exclusively heterosexual do not identify as lesbian, gay or bisexual (Mikulsky, 2005; Russell et al., 2009). Various reasons could account for this. For example, many of those who will eventually describe themselves as lesbian, gay or bisexual may not yet have ‘come out’ to themselves or others (Savin-Williams, 2001) and some may instead prefer terms like ‘queer’ or ‘questioning’ (Russell et al., 2009). Complexities linked to the challenges associated with defining sexuality may be one of the reasons why terminology like ‘sexual minority people’ or ‘sexual minority youth’ appears to have become fairly commonplace in the peer-reviewed literature.
Most research in the area of sexual minority youth and mental ill-health has relied on non-random samples of adolescents (Lucassen et al., 2011; Safren and Heimberg, 1999). As a result, the true proportion of sexual minority youth in the overall adolescent population and the risk of depressive disorder and depressive symptoms in sexual minority youth have been unclear. Non-random samples drawn from LGB community events, online sources and help-seeking organizations (e.g. counselling services) are useful, in that the surveys used can be designed specifically with sexual minority individuals in mind (e.g. they can more easily include detailed questions focused on homophobia and biphobia). Moreover, recruiting in this way is also an effective way of increasing a study’s sexual minority sample size (Morris et al., 2015; Swannell et al., 2016). But utilizing convenience-based samples (which typically lack a heterosexual comparison) presents major difficulties in establishing whether sexual minority individuals experience elevated rates of depressive symptoms and depressive disorder in comparison to their heterosexual peers (Cochran and Mays, 2006). For instance, participants recruited from LGB community events and networks have been found to be disproportionately drawn from specific demographic groups (e.g. white and male) (Cochran and Mays, 2006; Goldbach et al., 2014), and are thought to have different psychological profiles than sexual minority individuals not involved in the LGB community (Meyer and Wilson, 2009). Furthermore, in systematic reviews that combine convenience- and population-based samples, the proportion of sexual minority youth in the overall population cannot be determined, and when these estimates are presented they are understandably wide-ranging (i.e. 6–100% of a study’s cohort) (e.g. Goldbach et al., 2014; King et al., 2008; Marshal et al., 2011; Plöderl and Tremblay, 2015). A previous systematic review reporting a greater risk of depressive symptoms or depressive disorder and suicide in sexual minority young people included both population-based studies and convenience-based samples of sexual minority and heterosexual youth (with a sample mean age of ⩽18 years) (Marshal et al., 2011). In our systematic review and meta-analysis, we have focused only on population-based studies of adolescents (defined below).
Methods
We have conducted a systematic review informed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher et al., 2009). We used the Joanna Briggs Institute Prevalence Critical Appraisal Tool (Munn et al., 2014) to determine the quality of the studies, and we have carried out a meta-analysis of results.
Inclusion criteria
Publications were included if they:
Were population-based studies on depression (including depressive symptoms, depressive disorder or dysthymia) in which the size of the population could be determined and was deemed representative of a wider population in which there was no inherent selection bias towards including or excluding sexual minority young people, or sub-groups of these young people (e.g. school cohorts, birth cohorts and area cohorts);
Included prevalence statistics, symptom scores or data comparing sexual minority individuals and heterosexuals on depressive symptoms or depressive disorder;
Were studies conducted with sexual minority and heterosexual adolescents (in which sexuality was a variable);
Were published in the English-language.
Exclusion criteria
Publications were excluded if they
Utilized convenience or clinic/clinical-based sampling methods;
Were studies where adolescent data were not presented separately from adult data (or only adult data were provided);
Were opinion pieces or commentaries;
Were treatment studies (including case studies);
Were theoretical pieces (i.e. the publication did not contain original data).
When there were multiple publications from the same dataset, each study was subjected to the inclusion and exclusion criteria, after which five studies remained (from a total of 26 studies). Of the five studies, three were from the National Longitudinal Study of Adolescent Health project (Add Health), and two were from the Youth’2000 project. In order to not over-represent these datasets (Liberati et al., 2009), the relevant data from the study were extracted across the available papers and presented as one study in this review (i.e. Williams and Chapman, 2011).
Search strategy
We searched the following databases: PsycINFO (1806 to October 2015), Medline (1946 to October 2015), ERIC (1965 to October 2015) and EMBASE (1980 to October 2015). Relevant subject headings and key search terms with the appropriate truncation (i.e. $) were used, specifically: ‘homosexual$’ or ‘Homosexuality’ or ‘Sexual Orientation’ or ‘Sexual Behavior’ or ‘Lesbianism’ or ‘Homosexuality, Female’ or ‘Bisexuality’ or ‘Male Homosexuality’ or ‘Homosexuality, Male’ or ‘Homosexuality (Attitudes Toward)’ or ‘Gay’ or ‘same sex attract$’ or ‘queer’ AND ‘depress$’ or ‘Major Depression’ or ‘Depressive Disorder’ or ‘Depressive Disorder, Major’ or ‘Depression’ or ‘Depression (Emotion)’ or ‘major depressive disorder$’ or ‘Dysthymia’ or ‘Dysthymic Disorder’.
Study selection
The initial search revealed a total of 2691 articles. Of these, 518 studies were discarded as duplicates. The titles and abstracts of the remaining 2173 studies were examined by M.L., and 1859 were excluded because they did not meet the criteria (see Figure 1). A researcher and R.S. randomly selected and reviewed 109 papers identified by the search strategies (i.e. 5% of the papers) and independently concluded that 94% (n = 103) of the abstracts were suitable, but queried the exclusion of six abstracts. These were reviewed by another researcher who agreed with M.L.’s decisions for five out of the six abstracts. The sixth was excluded. The full text of the remaining 314 citations were examined in more detail, and it was determined that 291 did not meet the inclusion/exclusion criteria. No new articles were found by searching the reference lists of the articles included in the review. Data extraction was carried out by M.L. and checked by R.S.
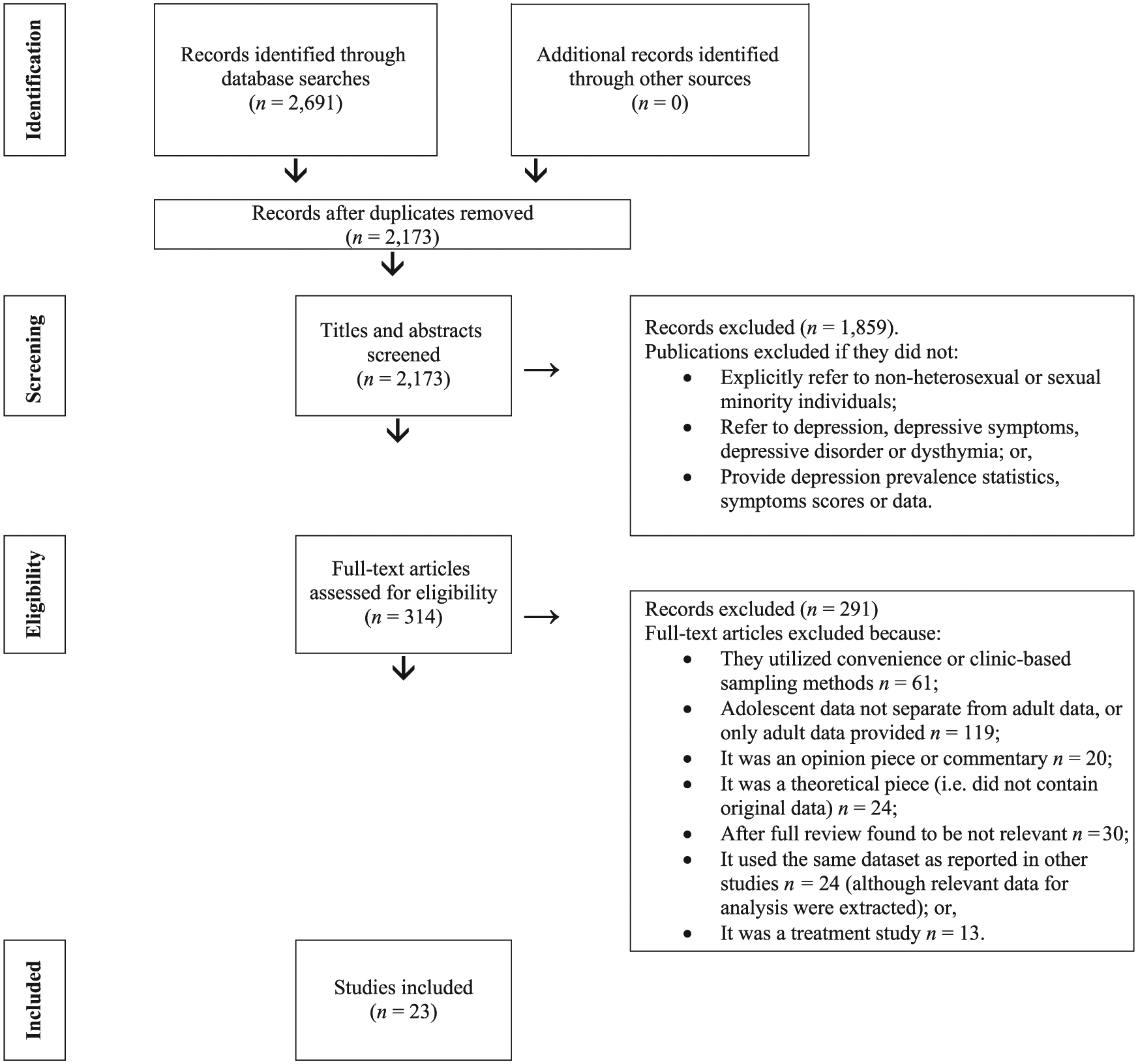
PRISMA flow diagram depicting the flow of information through the stages of the systematic review.
Meta-analysis methods
The overall effects for depressive symptoms and depressive disorder results were estimated in the studies that provided the relevant data (of note, studies 2, 7, 15 and 19 were excluded as the required data were not reported). This was done by combining weighted effects across all studies. Due to methodological diversity in the studies (i.e. variations in how sexuality and depressive symptoms or depressive disorder were assessed), statistical heterogeneity was anticipated, and therefore a random effects model was employed. The extent of heterogeneity in the results across studies was summarized as the I2 statistic. Different scales were used across the studies to report depressive symptoms; therefore, these are summarized in the meta-analysis using standardized mean differences (Cohen’s d). Sub-group analyses were conducted to compare: male sexual minority with female sexual minority youth and LGB youth with young people questioning their sexuality, as there were more than three studies available which allowed for these comparisons to be made. The meta-analysis was undertaken using RevMan5.
Results
Twenty-three studies met the inclusion criteria (see Table 1).
Summary of included studies (ordered by year of publication).
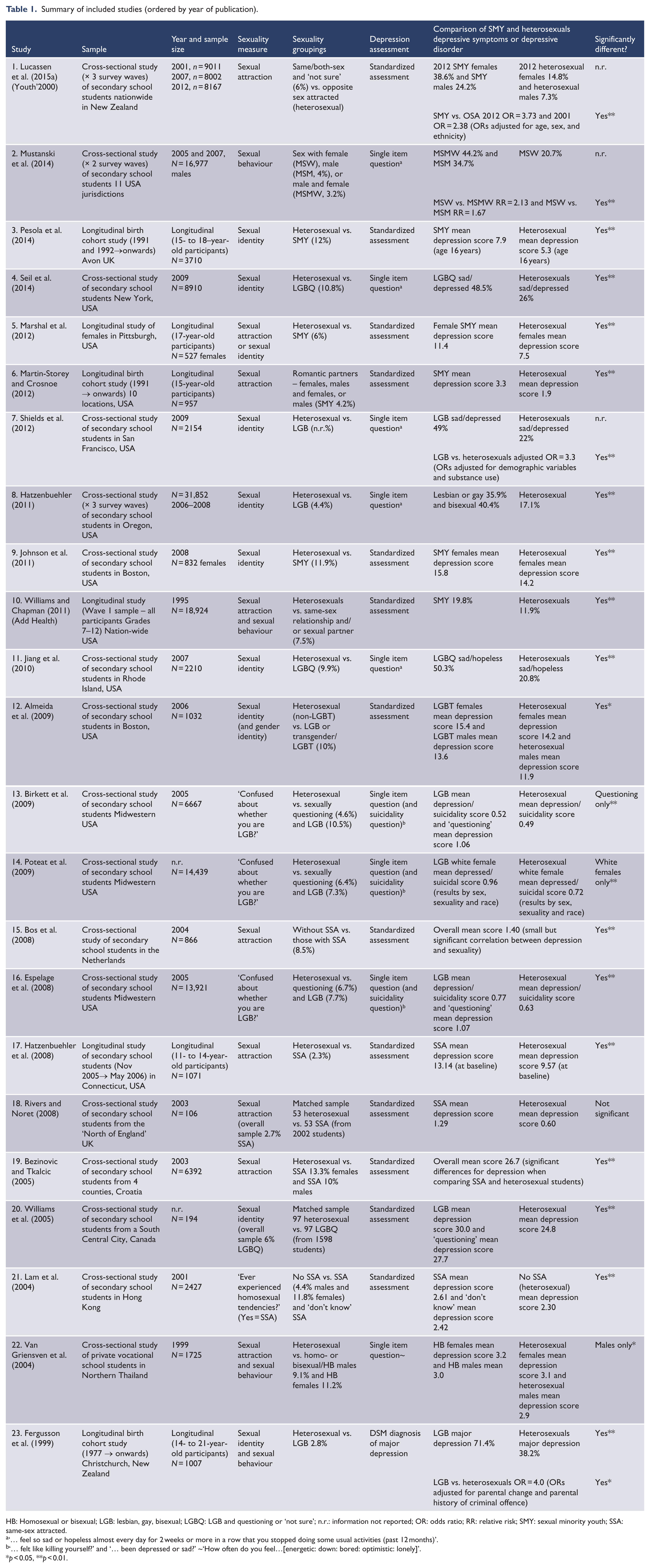
HB: Homosexual or bisexual; LGB: lesbian, gay, bisexual; LGBQ: LGB and questioning or ‘not sure’; n.r.: information not reported; OR: odds ratio; RR: relative risk; SMY: sexual minority youth; SSA: same-sex attracted.
‘… feel so sad or hopeless almost every day for 2 weeks or more in a row that you stopped doing some usual activities (past 12 months)’.
‘… felt like killing yourself?’ and ‘… been depressed or sad?’ ~‘How often do you feel…[energetic: down: bored: optimistic: lonely]’.
p < 0.05, **p < 0.01.
Date and location of studies
All 23 studies have been published since 1999 and almost half of the papers were published after 2010. The studies were from eight countries, with 14 studies from the United States, and 2 studies each from the United Kingdom and New Zealand. The remaining studies were from Europe, Asia and Canada.
Study design and sizes
The reviewed studies were predominantly cross-sectional and carried out in school settings; however, six studies were longitudinal, with three of these being studies of cohorts recruited from birth. Most of the studies were large with over 1000 participants (Tables 1 and 2), with the largest study having 31,852 participants. The smallest studies consisted of two papers with matched samples of sexual minority youth and heterosexual young people (n = 106 and n = 194). In total, the studies in the review included 165,380 individuals, of which an estimated 14,352 were sexual minority youth.
Assessment of the evidence using the Joanna Briggs Institute Prevalence Critical Appraisal Tool (Munn et al., 2014), systematic review of depression prevalence among sexual minority youth.
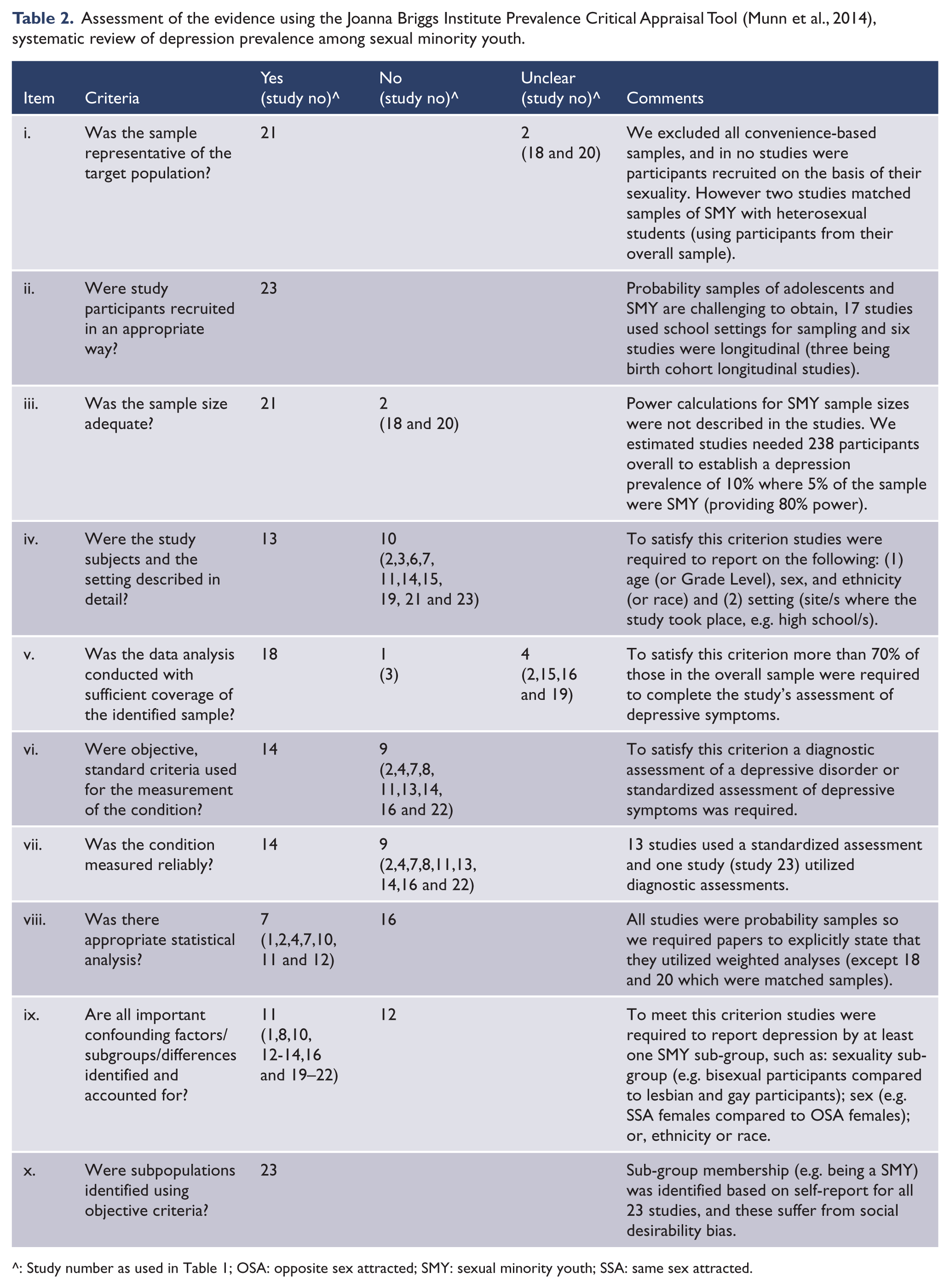
^: Study number as used in Table 1; OSA: opposite sex attracted; SMY: sexual minority youth; SSA: same sex attracted.
Measuring sexuality
There were reliability issues in determining participants’ sexuality, specifically there was no consistent method for determining sexuality for participants in the studies, and many measured more than one dimension of sexuality. Nine studies based their definitions on participants’ sexual attractions (with three of these including another dimension of sexual orientation) and 10 primarily used sexual identity labels like heterosexual, lesbian and gay (with two of these studies including another dimension of sexual orientation). Four used sexual behaviour to determine sexuality and four used a single-item question. Specifically, in three studies ‘Do you ever feel confused about whether you are lesbian, gay, or bisexual (LGB)?’ and in one study ‘Have you ever experienced homosexual tendencies?’ The proportion of sexual minority youth in the studies ranged from 2.3% to 12% (with this being 13.3% for same-sex attracted females in one study) and between 2.8% and 10.5% identifying as lesbian, gay or bisexual.
Assessing depressive symptoms or depressive disorder
There were issues in terms of reliability, as there was no consistent method for establishing depressive symptomatology (Table 2) and only one study included a diagnostic interview (i.e. Fergusson et al., 1999). This study used a diagnosis of major depression based on the Diagnostic and Statistical Manual of Mental Disorders (DSM) with participants between the ages of 14 and 21 years. Nine studies used a single-item question while 13 studies used a standardized assessment or a shortened version of an assessment (for the adapted questionnaires, cut-offs for the clinical severity of depressive symptoms were not reported). The assessments included the following:
The Child Depression Inventory (CDI; i.e. Hatzenbuehler et al., 2008), where possible scores range from 0 to 54, and with a mean cut-off of 14.5 for discriminative validity for detecting major depressive disorder (based on a systematic review and meta-analysis of diagnostic utility of various assessments) (Stockings et al., 2015). A shortened form of the CDI was also used in one study (i.e. Martin-Storey and Crosnoe, 2012).
The Reynolds Adolescent Depression Scale – Short Form (RADS-SF; i.e. Lucassen et al., 2015a) where scores ⩾28 were used as a cut-off for clinically significant depressive symptoms, because an analysis of earlier results from the Youth’2000 project showed that this cut-off best matched that of the full RADS (Milfont et al., 2008).
The Short Mood and Feelings Questionnaire (i.e. Pesola et al., 2014) where possible scores range from 0 to 26, and where scores ⩾12 are indicative of clinically significant depressive symptoms (Angold et al., 1995).
The Beck Depression Inventory (BDI; i.e. Williams et al., 2005) where possible scores range from 0 to 63, and where scores ⩾29 are indicative of severe depressive symptoms (Beck et al., 1996).
Adapted versions of the Modified Depression Scale (i.e. Almeida et al., 2009; Johnson et al., 2011), the Center for Epidemiological Studies-Depression Scale (CES-D; i.e. Lam et al., 2004; Williams and Chapman, 2011), the Child Symptom Inventories (i.e. Marshal et al., 2012), the General Health Questionnaire (i.e. Bos et al., 2008), Brief Symptom Inventory (i.e. Rivers and Noret, 2008) and Depressiveness and Existential Crisis assessment (i.e. Bezinovic and Tkalcic, 2005).
Quality of the evidence base
Most studies were representative of the target population, had appropriate recruitment strategies, adequate sample sizes and measured depressive symptoms in at least 70% of the sample. Slightly over half of the papers provided detailed descriptions of their study, and used standardized, reliable and objective measures of depressive symptoms or depressive disorder. Twenty-one studies were probability samples, but only seven explicitly stated that their analyses were weighted. Fewer than half of the studies examined within-group differences in their sample (Table 2).
Depressive symptoms or depressive disorder
In 22 out of the 23 studies, sexual minority youth were significantly more likely to experience depressive symptoms or depressive disorder. In one study (Birkett et al., 2009), only those questioning their sexuality reported higher levels of depressive symptoms, but this study relied only on a single-item question to determine depressive symptoms. Poteat et al. (2009) found that only white LGB females reported higher levels of depressive symptoms, and Van Griensven et al. (2004) found that only sexual minority males were more likely to have depressive symptoms; however, both studies assessed depressive symptoms using a single-item. One other study (Rivers and Noret, 2008) found no significant differences between sexual minority youth and heterosexual young people; however, this was based on a small sample of 106 participants.
Meta-analysis
Where studies reported categorical data on depressive symptoms or depressive disorder for results comparing sexual minority youth with heterosexual young people, the estimate for the relationship was OR 2.94 (95% confidence interval [CI] = [2.27, 3.80], p < 0.001). The estimated study level ORs ranged from 1.78 to 4.04 (see Figure 2).
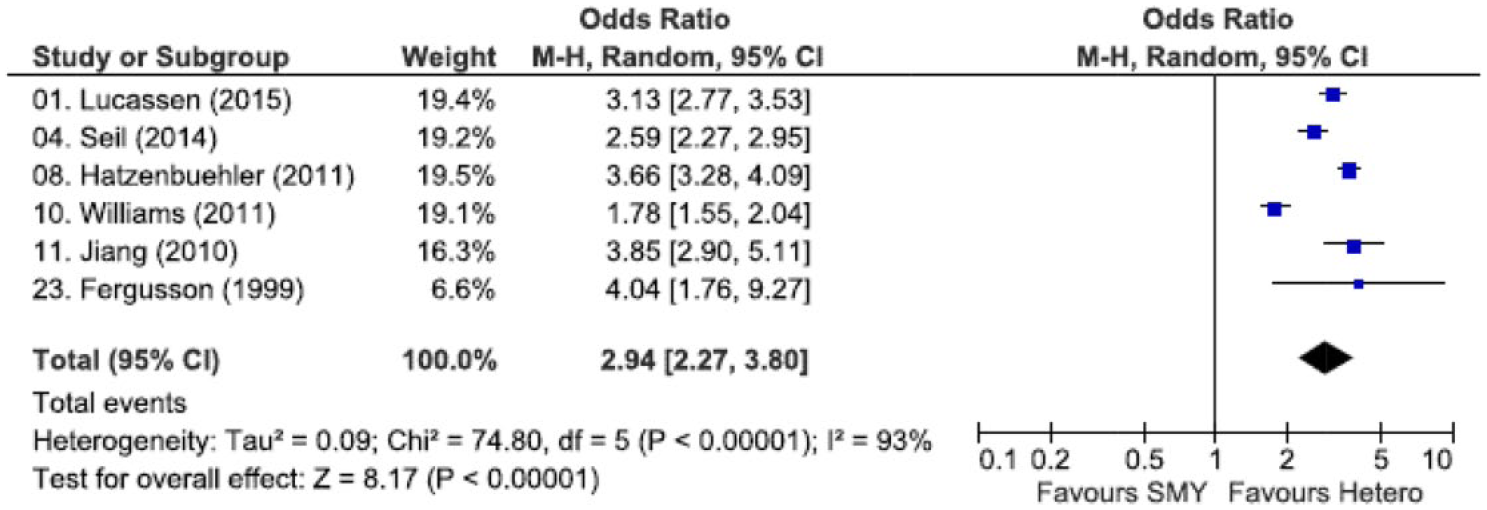
Odds ratios and 95% confidence intervals for studies testing the association between sexuality and depressive symptoms or depressive disorder.
Where studies reported continuous data on depressive symptoms comparing sexual minority youth with heterosexual young people, the overall standardized mean difference was d = 0.39 (95% CI = [0.33, 0.45], p < 0.001), with a range of 0.17–0.81 across studies (see Figure 3).
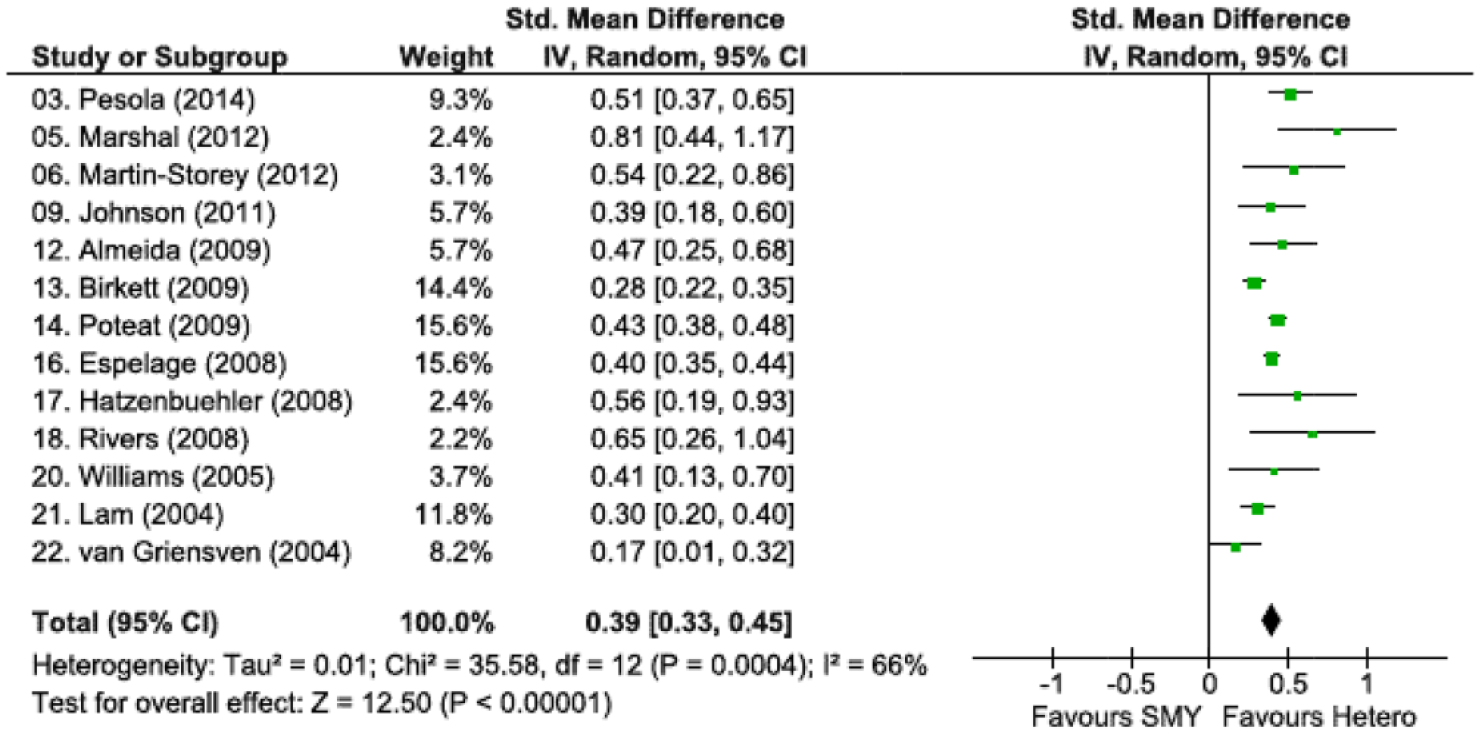
Standardized mean difference and 95% confidence intervals for studies testing the association between sexuality and depressive symptoms.
Five studies provided data comparing LGB (i.e. LGB young people or youth who were same-sex attracted) and questioning young people (i.e. youth questioning or unsure of their sexuality) and depressive symptoms. But the results for these comparisons did not reach statistical significance (standardized mean difference d = 0.21, 95% CI = [−0.04, 0.46], p = 0.1, I2 = 94%).
Only four studies reported data that allowed for comparisons to be made between male sexual minority and female sexual minority youth. The results indicated that sexual minority males are less likely to report depressive symptoms, relative to female sexuality minority youth (standardized mean difference d = 0.34, 95% CI = [0.16, 0.51], p < 0.001, see Figure 4).
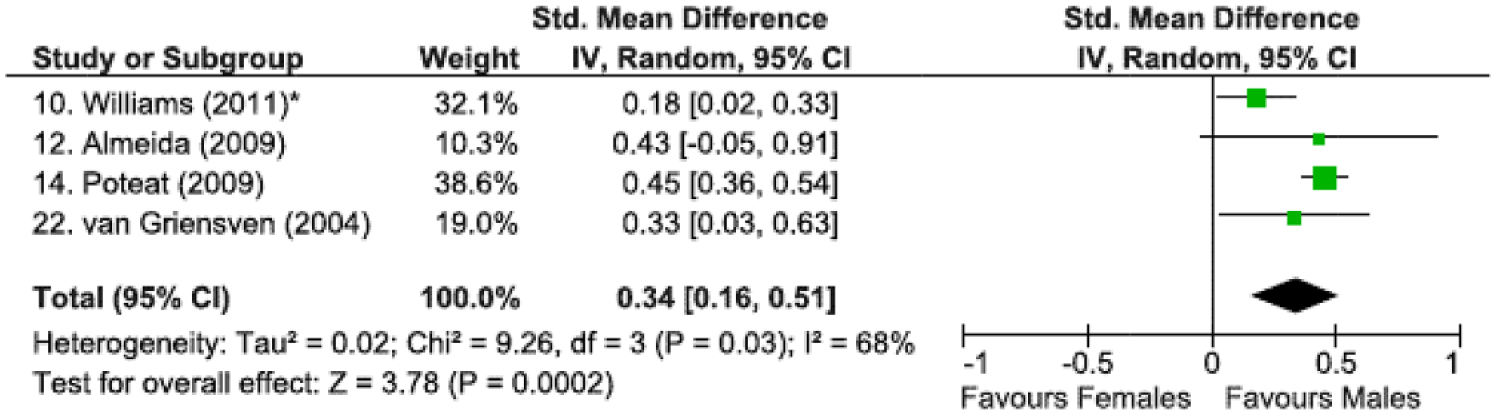
Standardized mean difference and 95% confidence intervals comparing male sexual minority and female sexual minority youth and depressive symptoms.
Discussion
In this review and meta-analysis, we have shown that sexual minority young people have approximately three times the odds of depressive symptoms or a depressive disorder compared with their heterosexual peers, and increased depressive symptoms of moderate effect size. Female sexual minority youth appear to be at particular risk, based on the results from four studies.
Strengths and limitations of the review
We included only population studies and excluded research that used non-random and potentially biased samples. We were careful to utilize search strategies that were inclusive and relevant, particularly in terms of the definition of sexual minority young people. Our findings are limited by the quality of evidence in some of the studies. Nonetheless, we have appraised the quality of the studies, and have summarized these in Table 2. Heterogeneity was high for the meta-analysis of dichotomous results (i.e. I2 93%), yet the same direction of effect was evident across these studies, and the findings were further supported by the results from studies reporting continuous data. However, the results based on secondary school samples are likely to under-estimate depression for both the sexual minority youth and heterosexual young people, as evidence suggests that adolescents excluded from mainstream education are likely to come from disadvantaged backgrounds and have high mental health needs (Denny et al., 2004). Our focus has been on sexual minority youth and not on adolescents who are diverse in terms of their gender identity (e.g. transgender youth) or sex (i.e. intersex young people). This is because there are insufficient probability studies conducted with these adolescents at present.
Comparisons to prior reviews
Three prior reviews have also concluded that sexual minority individuals are more likely to report mental ill-health, two primarily focused on adults (King et al., 2008; Plöderl and Tremblay, 2015) and the other on young people (Marshal et al., 2011). King et al.’s (2008) review included four studies (out of 25) that were conducted with adolescents. The inconsistent methods of assessing depressive symptoms or depressive disorder were critiqued in this review, and only one of the youth studies met all four of their quality criteria (King et al., 2008). Plöderl and Tremblay (2015) focused on adults as well as adolescents for a range of issues including depressive symptoms or depressive disorder, suicidality, anxiety disorders, alcohol use, drug use and other disorders. Based on their review of PubMed articles, they reported that in 97% of studies rates of depressive symptoms were elevated (Plöderl and Tremblay, 2015). Marshal et al. (2011) included 11 studies on depressive symptoms or depressive disorder in sexual minority youth in their analyses, but they included non-random samples, presumably because there were fewer population-based studies at the time. Our review not only reinforces previous findings but also strengthens the evidence on which they are based. Our analyses suggest that, similar to females compared to males in the overall population, female sexual minority youth are at greater risk of depressive symptoms when compared to male sexual minority youth. Our review has strengthened previous findings by comparing male and female sexual minority youth, including more recent studies, assessing the evidence more closely, and excluding convenience-based studies. By excluding convenience-based studies, we have been able to report the proportion of sexual minority young people more confidently at between 2.3% and 12%. It should be noted that questions on sexuality, by virtue of being ‘sensitive’ are affected by social desirability bias. Moreover, recent work has also indicated that ‘mischievous responders’ could artificially inflate sexual minority numbers (e.g. there may be heterosexual adolescents who think it is humorous to report that they are LGB, transgender and/or physically disabled in questionnaires; Robinson-Cimpian, 2014). Our estimate of the proportion of sexual minority youth is inclusive of adolescents who reported same-sex attractions, rather than the more limited constructs of sexual identity or same-sex sexual behaviour. Therefore, having up to 12% of adolescents reporting these attractions is not surprising, as a greater proportion of young people are likely to have these sexual attractions than those who identify as LGB, or report having had sex with a same-sex partner (Wichstrom and Hegna, 2003). We believe that this review is timely as there has been a recent call to action recommending that there should be more research into the mental health of lesbian, gay, bisexual, transgender and intersex (LGBTI) people, e.g., the recent position statement from the Royal Australian and New Zealand College of Psychiatrists highlighting the need to address the mental health needs of the LGBTI people (Royal Australian and New Zealand College of Psychiatrists, 2016). The findings from our review support this position statement, but also highlight particular needs for young people in the overall LGBTI population, particularly female sexual minority youth.
Much is still unknown about the optimal treatment of depressive symptoms in adolescents (Malhi et al., 2015), hence it is time to consider in what ways young people overall can be treated, alongside gaining an understanding of how sexual minority young people can receive more targeted support and assistance, to ensure that their mental health is enhanced. Work in this area has begun, for instance where an existing intervention has been assessed with young people more generally, such as attachment-based family therapy (Devenish et al., 2016), which has been modified specifically with suicidal sexual minority youth in mind (Diamond et al., 2013). This approach has also been employed in the treatment of depressive symptoms using a form of computerized cognitive behavioural therapy, called SPARX (Merry et al., 2012), which has been adapted and evaluated among sexual minority youth with depressive symptoms (Lucassen et al., 2015b, 2015c).
Future studies in this field would be improved by the inclusion of standardized symptom measures or diagnostic assessments that have established validity and reliability such as the CDI, BDI, CES-D and RADS (Stockings et al., 2015). Moreover, we would recommend the use of sexual attraction to assess adolescent sexuality. We consider this is an appropriate measure to use from a developmental perspective and is a view supported by others (Saewyc et al., 2004).
Conclusion
Depressive symptoms and depressive disorder in adolescents are associated with considerable morbidity and tend to persist into adulthood (Thapar et al., 2012). Sexual minority youth make up a relatively small but important sub-group of the overall population (i.e. 2.3–12% of adolescents) and there is now robust evidence to suggest that this group of young people are at elevated rate of depressive symptoms and depressive disorder (although there are ongoing reliability issues in terms of how sexuality is defined and depressive symptoms or depressive disorder are assessed in this area of research). Sexual minority youth face the double stigma of being in this marginalized group and having mental health problems. More needs to be done to enhance their mental health taking into account the challenges they are likely to face accessing appropriate help.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.