
Abstract
Objective:
Stigma and discrimination are central concerns for people with mental health problems. The aim of the study was to carry out a national survey in order to assess experiences of avoidance, discrimination and positive treatment in people with mental health problems.
Methods:
In 2014, telephone interviews were carried out with 5220 Australians aged 18+, 1381 of whom reported a mental health problem or scored highly on a symptom screening questionnaire. Questions covered experiences of avoidance, discrimination and positive treatment by friends, spouse, other family, workplace, educational institution and others in the community.
Results:
In most domains, respondents reported more positive treatment experiences than avoidance or discrimination. Friends and family were more likely to avoid the person than to discriminate.
Conclusion:
The results can provide input into the design of anti-discrimination interventions and further empower people with mental health problems as they advocate for change in the area of discrimination.
Background
Stigma and discrimination are often nominated as central concerns for people with mental health problems (Corrigan et al., 2003; McNair et al., 2002). Stigma and discrimination adversely impact wellbeing in a number of ways, including worsening of psychological distress, inhibition of help-seeking and treatment adherence, limiting of personal relationships and reductions in the ability to achieve educational and vocational goals (Corrigan, 2004; Link et al., 1997; Wells et al., 1994).
Until relatively recently, most stigma-related research involved surveys comprising questions about attitudes towards people with mental health problems, rather than the experiences of people with these problems (Reavley and Jorm, 2011a, 2011b). A limited number of studies have attempted to assess experiences of discrimination in people with mental health problems, but these have typically assessed experiences in clinical populations or people with one specific disorder (most commonly schizophrenia) (Angermeyer et al., 2004; Lasalvia et al., 2013; Thornicroft et al., 2009; Wahl, 1999). There is relatively little published data on the prevalence rates of mental disorder–related discrimination in the general population. The population-based World Mental Health Surveys included a question about discrimination or unfair treatment experienced in the last 30 days, reporting mean prevalence rates of 26.2% in developing countries and 16.3% in developed countries (Alonso et al., 2008). However, no further information on the range of life domains affected by discrimination was collected. A US study used data from the 1994–1995 National Health Interview Survey–Disability Supplement to ask about experiences of discrimination in the workplace, finding that 20% of workers with serious mental illness reported some type of job-related discrimination (Baldwin and Marcus, 2006). A 2010 Canadian population survey explored stigma and discrimination experiences in the life domains of family relationships, romantic life, school or work life, financial situation and housing situation in 752 people who had received treatment for a mental health problem in the year prior to the survey (Stuart et al., 2014). This was defined as someone having ‘held negative opinions about you or treated you unfairly’ and the results showed that 37.4% of respondents had these experiences in at least one life domain. However, there was no further exploration of the nature of these experiences and importantly, no population-based studies have systematically assessed experiences of positive treatment.
Therefore, the aim of the current study was to carry out a national population-based survey in order to assess experiences of avoidance, discrimination and positive treatment in people with mental health problems.
Methods
The survey involved computer-assisted telephone interviews (CATI) with a national sample of 5220 members of the general community aged 18 and over. The survey was carried out by the survey company Social Research Centre. A ‘dual frame’ approach was used, with the sample contacted by random-digit dialling of both landlines and mobile phones. This approach was taken in order to minimise the potential bias of collecting data solely from households with a landline telephone connection. The landline-only approach may under-sample young people, particularly young men (Hu et al., 2011). Call procedures for the survey featured: (1) call attempts placed over different days of the week and times of day, (2) placing up to four calls for mobiles and six calls for landlines to establish contact (with additional calls for hard appointments as necessary), (3) limited call initiation during business hours except by appointment and (4) late shifts dialling to landline numbers identified as Western Australia. Interviews were conducted between October and December 2014. Ethics approval was obtained from the University of Melbourne Human Research Ethics Committee.
Survey interview
After initial questions covering sociodemographic information (age, gender, marital status, postcode, country of birth, language spoken at home, level of education and Aboriginal and Torres Strait Islander status), respondents were taken through the 12-month version of the Kessler 6 (K6) mental health symptom screening questionnaire (Kessler et al., 2010). This questionnaire asks participants to think about 1 month in the last 12 months when they were most depressed, anxious, or emotionally stressed. Respondents were also asked whether, over the last 12 months, they had experienced any sort of mental health problem (defined in the preamble to the question in the following way): a period of weeks or more when you are feeling depressed, anxious, or emotionally stressed, and these problems are interfering with your life. Mental health problems could include, for example, depression, anxiety disorders, eating disorders, schizophrenia, bipolar disorder, or personality disorders.
Those respondents who answered yes to this question were then asked what they thought the problem was. Respondents who specified any of the following mental health problems were considered in scope: depression/major depression, attempted suicide or self-harm, anxiety/anxiety disorder, post-traumatic stress disorder/PTSD, agoraphobia, panic disorder, obsessive–compulsive disorder/OCD, social phobia, generalised anxiety disorder/GAD, eating disorder/anorexia/bulimia, schizophrenia/paranoid schizophrenia, schizoaffective disorder, psychosis/psychotic, bipolar/bipolar disorder/manic-depressive disorder, mental illness, personality disorder/borderline personality disorder, attention deficit-hyperactivity disorder/ADHD, Autism/Asperger’s and nervous breakdown. At this point, survey respondents were divided into two groups: (1) those who scored in the ‘high’ range on the K6 (equal to or above 19) or who reported having had an in-scope mental health problem and (2) those who did not meet these criteria.
Those in the first group were then asked the following questions about their experiences of avoidance, discrimination and positive treatment (with a past 12-month timeframe specified in the introduction to this section of the questionnaire): ‘Have any of your friends avoided you because of the emotional or mental health problems you have told me about?’, ‘Have any of your friends discriminated against you in other ways because of these problems?’, ‘Can you please describe what happened?’, ‘Have any of your friends treated you more positively because of these problems?’ and ‘Can you please describe what happened?’. The same questions were asked for the following people or situations: spouse or intimate partner, other members of the family, people in the workplace, looking for work, people in the place of education, health professionals (with an additional question on type of professional), other people in the community or neighbourhood, other people and other situations. For people or situations in the ‘looking for work’, ‘health professionals’, ‘other people’ and ‘other situations’ categories, the question relating to avoidance was omitted.
In a subsequent section of the questionnaire, all respondents were asked whether they knew any adult with a mental health problem (see definition above). Those who reported definitely knowing someone in this category were asked if there was more than one person. In such cases, they were asked to think about the person they knew best. They were asked about the mental health problem the person had, how they knew the person had the problem, as well as the person’s age, gender and relationship to the respondent. Those that knew someone with an in-scope mental health problem (see definition above) were asked the following questions (with a past 12-month timeframe specified in the introduction to this section of the questionnaire): ‘Did any of this person’s friends avoid them because of their mental health problems?’, ‘Did any of this person’s friends discriminate against them in other ways because of their problems?’, ‘Did any of this person’s friends treat them more positively because of their problems?’. If the respondent answered any of these questions in the affirmative, they were then asked: ‘How did you find out about this happening – Did you observe this happening yourself or did the person or someone else tell you about it?’. The same questions were asked for the following people or situations: spouse or intimate partner, other members of the family, people in the workplace, looking for work, people in the place of education, health professionals (with an additional question on the type of professional), other people in the community or neighbourhood, other people and other situations.
Respondents were also asked if, in the last 12 months, they themselves had avoided the person or anyone else with a mental health problem, treated the person or anyone else unfairly, or treated the person or anyone else more positively because of their mental health problems. Those who answered in the affirmative were asked to describe what happened.
Further questions were asked about respondents’ disclosure of their mental health problems and views on the dangerousness of people with mental health problems, their exposure to people with mental health problems and their exposure to media reports of violence by people with mental health problems. Data relating to this section of the survey will be reported elsewhere. The average interview length was 19.4 minutes.
Statistical analysis
The data were analysed using percent frequencies and 95% confidence intervals. A pre-weight was applied to adjust for the dual frame design and the respondent chance of selection. The achieved sample was close to the Australian national population in terms of geographic distribution; however, there was an under-representation of males and of younger adults, and an over-representation of university-educated individuals and people with an English-speaking background. These biases were adjusted for by ‘raking’ (also known as rim weighting or iterative proportional fitting) to account for known population proportions of gender, age, education level, region and telephone status (with age and gender based on Australian Bureau of Statistics [ABS] data of March 2014 [Australian Bureau of Statistics, 2014b], level of education and region based on ABS 2011 census data [Australian Bureau of Statistics, 2014a] and telephone status based on 2011 Australian Communication and Media Authority data [Australian Communication and Media Authority, 2014]). All analyses were performed using Intercooled Stata 13 (StataCorp LP, Texas, USA).
Results
Overall, 5220 interviews were completed, with 2589 on landlines and 2631 on mobiles. The standard response rate for the survey was 37.5% and the American Association of Public Opinion Research (AAPOR) response rate (which enables a more accurate assessment of the response rate, as some households that refuse the screening process would in fact be in scope) was 18.5%. A total of 732 (16.5%) respondents were found to have K6 scores of 19 or above and 1159 (23.9%) respondents had a mental health problem considered to be in scope. Among these respondents, 840 (63.6%) had received a diagnosis and 842 (64.0%) had received treatment. When asked about their mental health problems, 769 (58.8%) respondents named the problem as depression, 555 (48.4%) as an anxiety disorder and 60 (4.8%) as bipolar disorder. Thus, 1381 (28.8%) respondents were asked the questions about personal experiences of avoidance, discrimination and positive treatment.
Additionally, 2703 (51.0%) respondents knew someone with an in-scope mental health problem in the previous 12 months, with 1568 (49.8%) naming the problem as depression, 726 (23.8%) as an anxiety disorder and 500 (15.5%) as bipolar disorder. When asked to describe their relationship with the person, 1271 (46.3%) respondents described them as a family member, 907 (34.3%) as a friend, 202 (8.1%) as a spouse and 158 (5.7%) as a work colleague. When asked how they knew the person had a mental health problem, 1626 (61.6%) respondents reported that the person had told them, 1363 (50.1%) reported that they recognised it and 644 (23.8%) reported that someone else told them.
Tables 1–4 show the percentages of respondents with personal experiences of avoidance, discrimination and positive treatment by people and in situations described above, as well as avoidance, discrimination and positive treatment experienced by a known adult with a mental health problem. For personal experiences, in all domains other than looking for work, treatment by nurses, mental health nurses, dentists, paediatricians, surgeons, community nurses, landlords, Centrelink (government welfare agency) workers, other government officials, real estate agents and insurance-related situations, respondents reported a greater frequency of positive treatment experiences than avoidance or discrimination. In the domains of friends and spouse or partner, respondents reported a greater frequency of personal experiences of avoidance than discrimination.
Experiences of discrimination and positive treatment by friends and family.
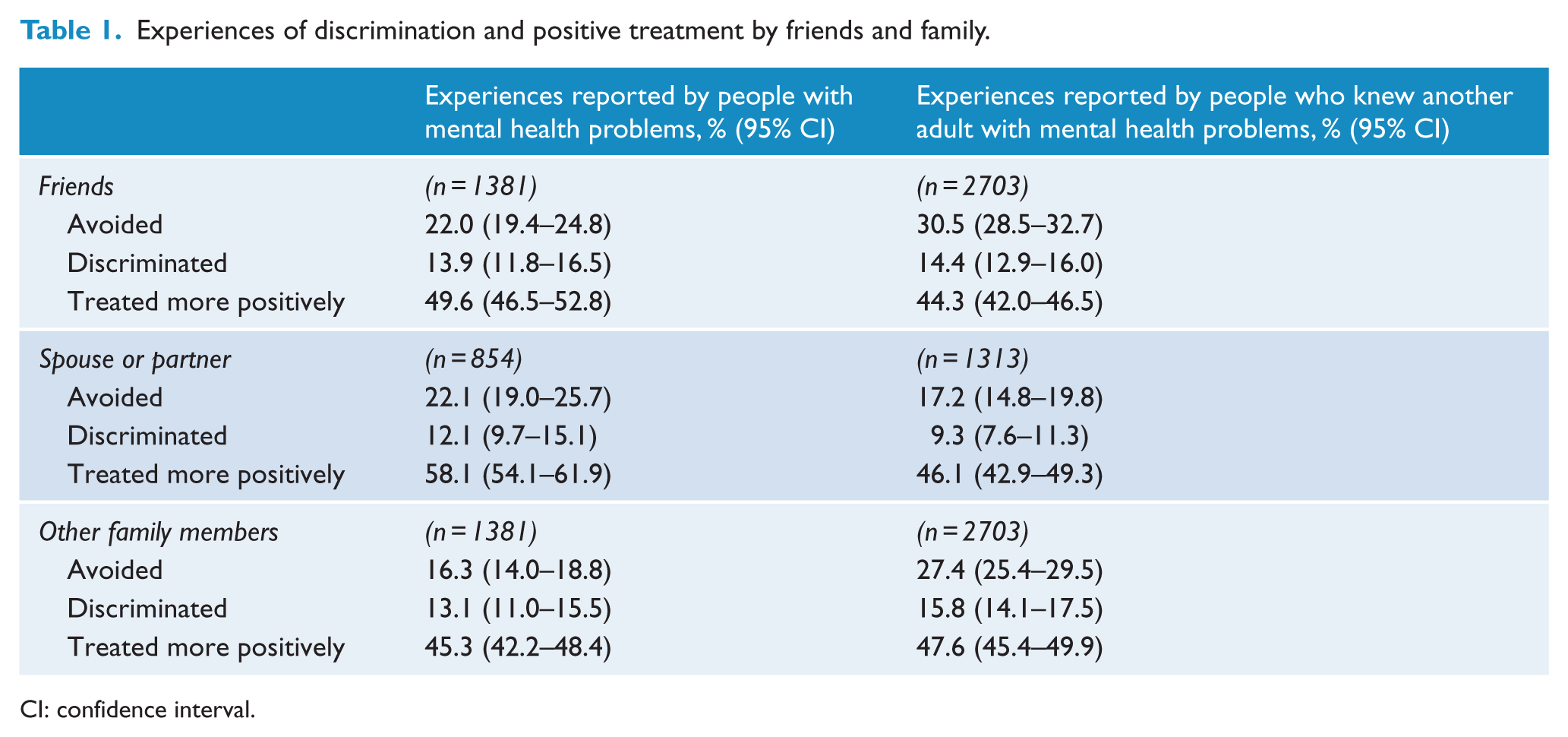
CI: confidence interval.
Experiences of discrimination and positive treatment by people in the workplace or place of education.
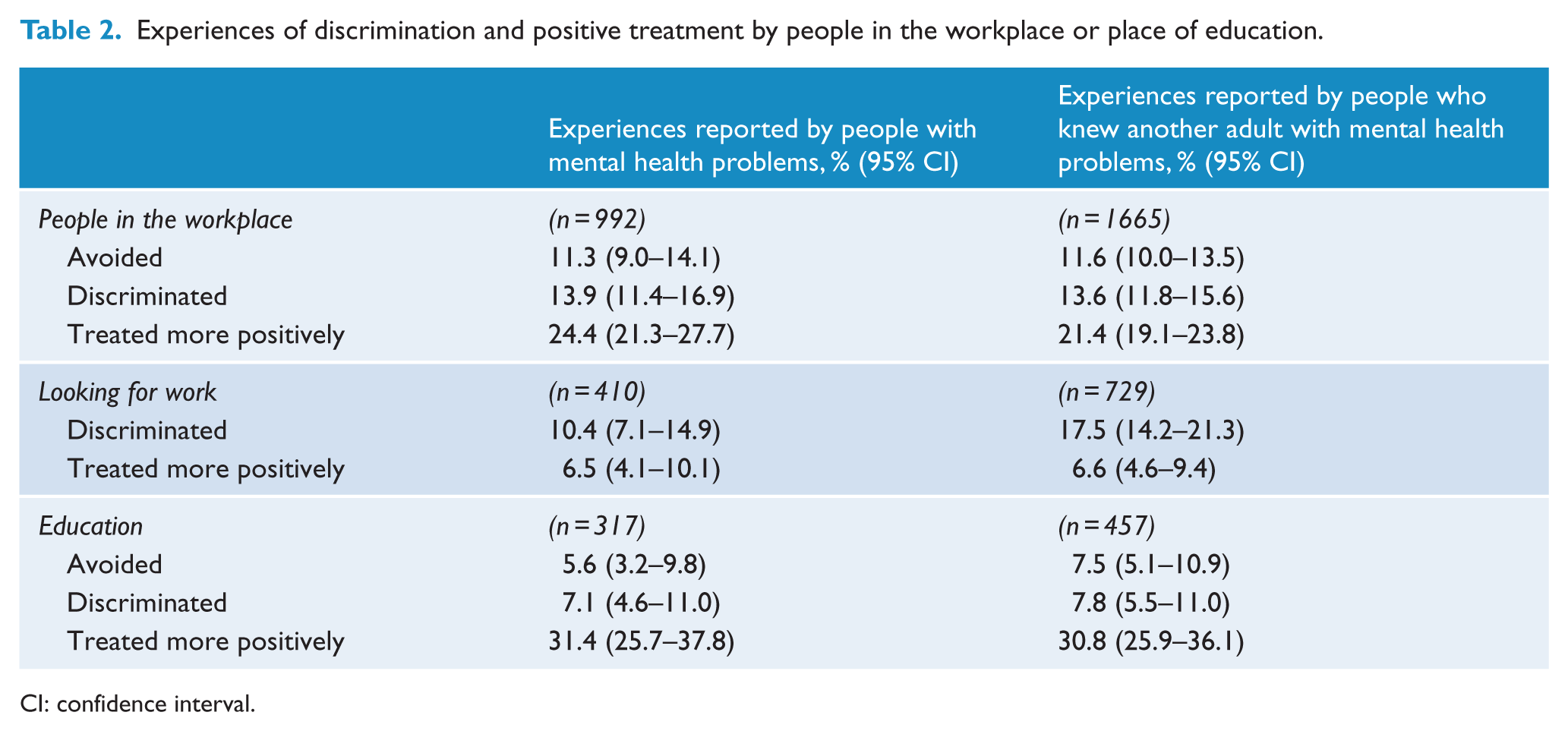
CI: confidence interval.
Experiences of discrimination and positive treatment by health professionals.
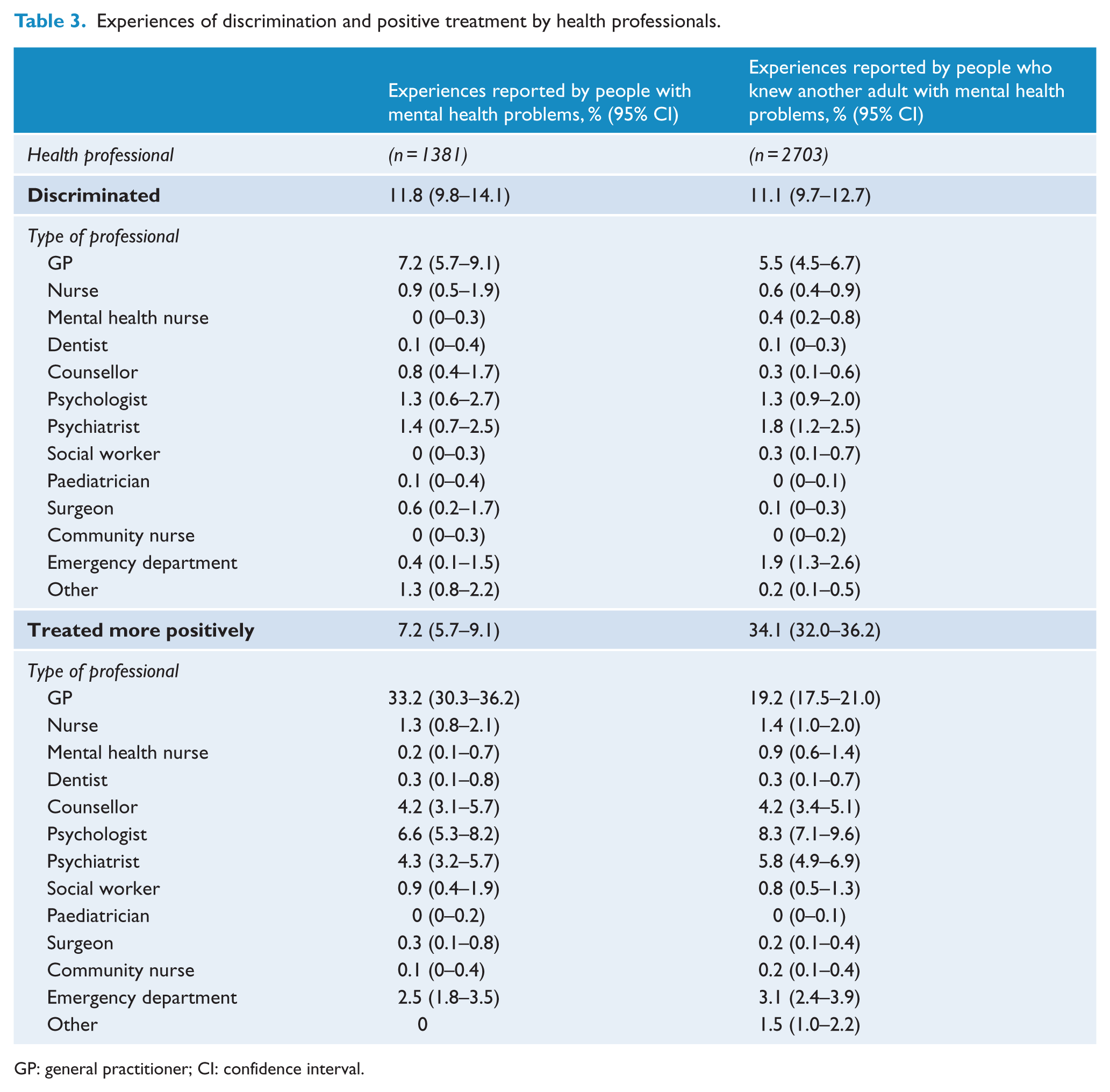
GP: general practitioner; CI: confidence interval.
Experiences of discrimination and positive treatment by people in the community or neighbourhood.
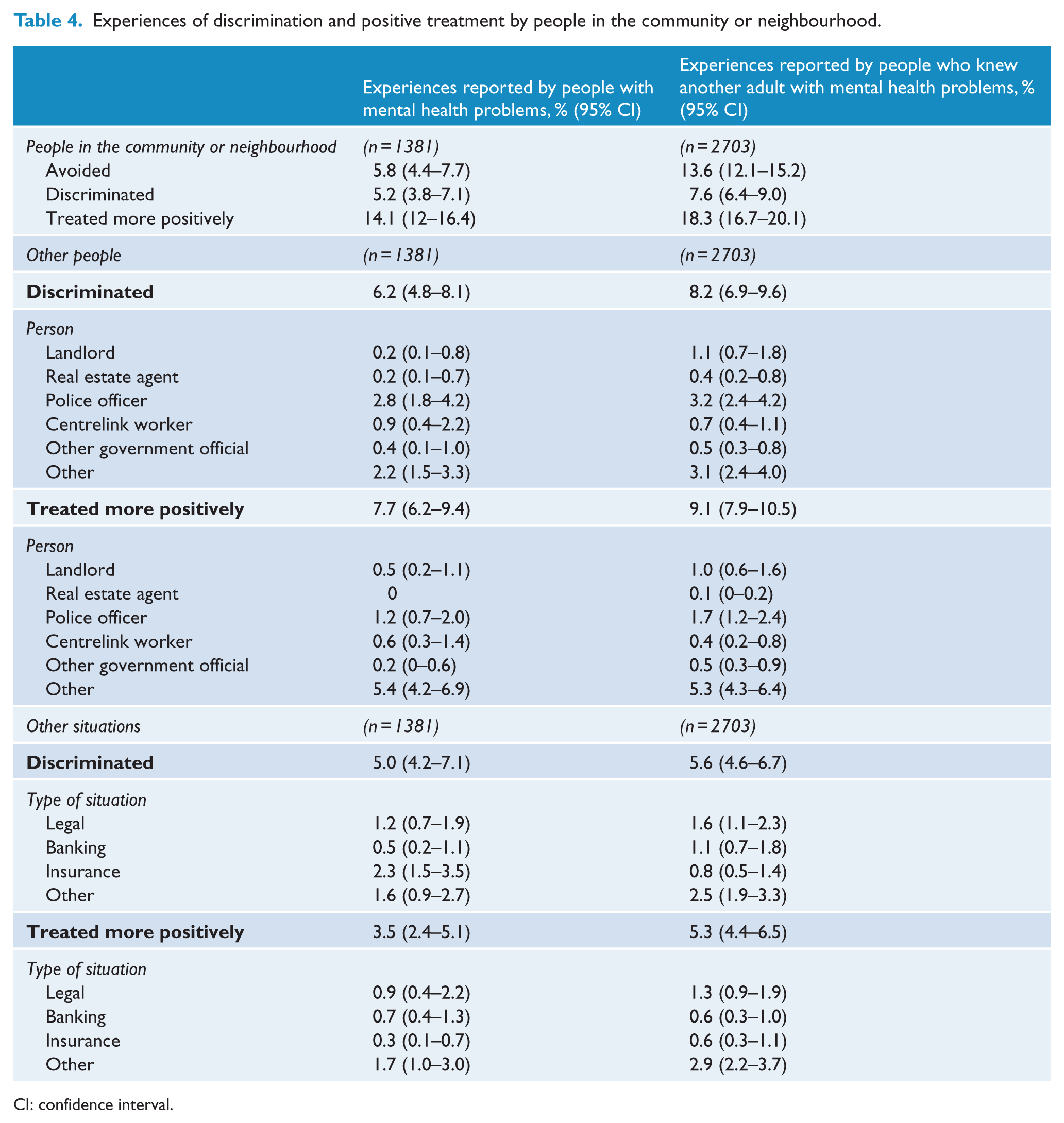
CI: confidence interval.
For experiences in other adults, respondents also reported a greater frequency of positive treatment than avoidance or discrimination in all domains other than looking for work, treatment by mental health nurses, social workers, paediatricians, surgeons and community nurses. In addition, a greater frequency of avoidance than discrimination was seen in the domains of friends, spouse or partner, other family members and other people in the community or neighbourhood.
When compared with personal experiences of avoidance, experiences in other adults were reported in higher frequencies in the domains of friends, other family members and people in the community or neighbourhood. Personal experiences of discrimination were reported in higher frequencies than experiences in other adults in the domain of insurance.
Table 5 shows respondents’ treatment of other people with mental health problems. Respondents reported that their positive treatment of other people with mental health problems was more frequent than avoidance which was more frequent than discriminatory treatment.
Respondent treatment of other people with mental health problems.
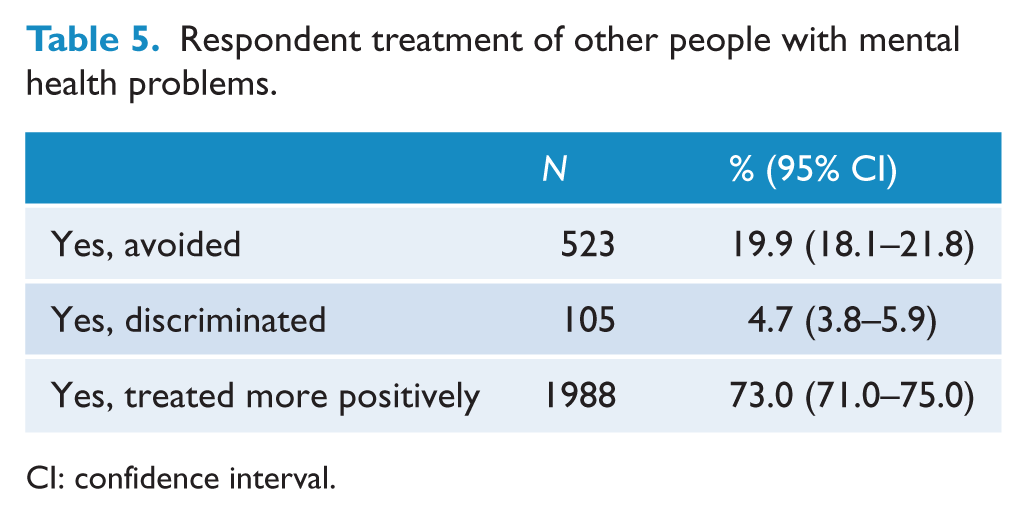
CI: confidence interval.
Discussion
This paper reports results of the first national population-based survey to assess experiences of avoidance, discrimination and positive treatment in a wide range of life domains in people with mental health problems. Results showed that, in most domains, respondents reported a greater frequency of positive treatment experiences than avoidance or discrimination. The highest rates of all types of experiences were found in the domains of friends, spouse or partner and other family members, a finding that is likely to be explained by the greater number of opportunities for contact between the person with mental health problems and friends and family. These findings are in line with the results of the Canadian survey that asked respondents who had been treated for a mental illness in the past year about unfair treatment (Stuart et al., 2014). The results showed that this was most common in relation to intimate personal relationships, such as family (32%) or romantic relationships (30%).
Thus, the social environments of friends, families, workplaces and educational institutions in particular are sources of both discrimination and support, depending on the circumstances of the individual. Further work is needed to explore the factors predicting both discrimination and positive treatment in order to best promote the latter.
The study also showed that friends and family were more likely to avoid the person than to discriminate, a finding in line with those from studies of service users conducted in other countries. In a US study of 1301 service users with various diagnoses, Wahl (1999) found that being shunned or avoided were the most common experiences, with few reports of actual discrimination. A German study of 209 patients with either schizophrenia or depression found that 60% of people with schizophrenia experienced rejection by others and 51.5% experienced avoidance of contact, while for depression, 45.3% experienced rejection by others and 26.4% avoidance of contact (Angermeyer et al., 2004). In a 35-country survey of people with major depressive disorder attending specialist mental health services, Lasalvia et al. (2013) found that 40% reported being avoided or shunned by other people, 33% reported discrimination in the area of making or keeping friends, 21% reported discrimination in the area of keeping a job, 21% in dating or intimate relationships, 17% in the neighbourhood, 13% in finding a job, 12% in education and 6% by police. In a similar study with people with schizophrenia, similar patterns were seen, although rates of discrimination were generally higher (Thornicroft et al., 2009). The rates of avoidance and discrimination reported in these studies of service users are higher than in the current study involving a community sample. Another contrast with the current study is that positive treatment was reported to be rare in service users with schizophrenia or depression (Angermeyer et al., 2004; Lasalvia et al., 2013), although this may be due to differences in the way the questions were phrased.
The domains for which discrimination were not outweighed by positive treatment included looking for work. This finding suggests the need to better support people with mental health problems who are looking for work, whether this is in supporting them to overcome anticipated discrimination or in other ways that support vocational rehabilitation, including education of employers to support stigma reduction (Henderson et al., 2013).
When reports of personal experiences of avoidance, discrimination and support were compared with reports of these experiences in other adults with mental health problems, similar patterns were seen. In some domains, notably those of friends, other family members and people in the community or neighbourhood, reports of avoidance experiences in other adults were of higher frequencies than personal experiences of avoidance. This is of interest in the context of the potential difficulties in interpreting another person’s actions as ‘discrimination’. Other studies have found relatively high levels of anticipated discrimination in people with mental health problems, and it is possible that a person with a mental health problem may interpret another person’s actions as discrimination when someone who does not have a mental health problem would not (Lasalvia et al., 2013; Thornicroft et al., 2009). The results of this study suggest that this is unlikely. When experiences of discrimination were compared with the results of the questions asking respondents how they treated other people with mental health problems, discrimination and avoidance were notably less common and positive treatment notably more common. While social desirability may have influenced responses to these questions, it is also possible that people act in ways that are discriminatory without necessarily realising or intending to, perhaps due to underlying assumptions about the capacities of people with mental health problems. Anti-stigma campaigns that directly focus on such behaviours may be important in overcoming discrimination (Henderson and Thornicroft, 2013; Thornicroft et al., 2014).
The study has several strengths. It is the first study to assess, at a population level, mental health problem–related experiences of avoidance, discrimination and positive treatment in a wide range of domains. Interviews were used to gather reports of actual experiences of people with a wide range of mental health problems rather than responses to hypothetical scenarios. As the survey collected data from people who are not in contact with mental health services, the results are less likely to be biased towards under-reporting due to people who have experienced very high levels discrimination avoiding service contact (Lasalvia et al., 2013). It is also less likely to be biased towards over-reporting due to people who have experienced discrimination being more likely to volunteer to take part in a survey on the topic. Limitations of the study include the relatively low response rate of 37% which, while in line with other similar Australian surveys, may limit the generalisability of the results (Curtin et al., 2005).
It is hoped that the results of the current study can provide much-needed input into the design of anti-discrimination interventions, for example, public education about human rights and the impact of discrimination on mental wellbeing; action from health services to help overcome anticipated discrimination as a barrier to help-seeking and the incorporation into treatments such as Cognitive Behavioural Therapy of techniques to address discrimination as well as symptoms. Compared to other studies, more detailed information on positive treatment was also collected, allowing for incorporation of these findings into the design of anti-stigma interventions, e.g. key messages to workplaces or families about the kinds of actions that reduce the impact of mental health problems. As data on experiences in those with and without diagnoses were also collected, further analyses will also shed light on the impact of diagnosis and treatment on discrimination and positive treatment. It may also empower people with mental health problems to further advocate for change in the area of discrimination by providing further evidence of the validity of their experiences.
Footnotes
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The study was funded by the National Health and Medical Research Council.