
Abstract
Objective:
To examine the associations between beliefs about the causes of depression, schizophrenia, social phobia and post-traumatic stress disorder (PTSD) and stigmatising attitudes towards people with these disorders.
Methods:
In 2011, telephone interviews were carried out with 6019 Australians aged 15 or over. Participants were presented with a case vignette describing either depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia or PTSD. Participants were asked about their beliefs about the causes of these disorders and about their personally held stigmatising attitudes, stigmatising attitudes perceived in others and the desire for social distance from the person described in the vignette.
Results:
Belief in a weak or nervous personality as the cause of mental disorders was most consistently associated with personal stigma, perceived stigma and desire for social distance across vignettes. Belief in biogenetic causes was associated with a decreased belief in mental disorders as due to weakness rather than sickness, but was not linked to either a decreased or increased belief in dangerousness and unpredictability or desire for social distance. Belief in physical causes was associated with an increased belief in mental disorders as due to weakness rather than sickness. Belief in psychosocial causes had no consistent associations with stigma.
Conclusions:
Explaining mental disorders as due to personality characteristics is a more important factor in stigma than either biogenetic or psychosocial explanations.
Introduction
Stigma may be defined as “a mark of shame, disgrace or disapproval which results in an individual being rejected, discriminated against, and excluded from participating in a number of different areas of society” (World Health Organization, 2001). People with mental disorders must cope with their symptoms and also with the stigma that arises from erroneous beliefs, stereotypes and prejudice about these disorders. These stigmatising attitudes are often nominated as a central concern for people with mental disorders and may compound psychological distress, impact on treatment seeking, social participation and the ability to achieve educational and vocational goals (Corrigan et al., 2003; Lasalvia et al., 2013; McNair et al., 2002).
Stigmatising attitudes towards people with mental disorders have been conceptualised and measured in different ways. In their stigmatisation model, Link and Phelan (2001) define stigma as the co-occurrence of its components: labelling, stereotyping, separation, status loss, and discrimination. They also note that for stigmatization to occur, power must be exercised. Corrigan and Watson (2002) have defined public stigma as the discrimination directed against people with mental illness by individuals from the general population who endorse related stereotypes, and distinguished this type of stigma from self-stigma, which is the harm to self-esteem that results from internalising stereotypes. Although stigma is often discussed as a single construct, cumulative evidence clearly indicates that it is complex and multidimensional (Griffiths et al., 2004; Stansfield et al., 2008; Watson et al., 2005). A number of components of stigma have been identified, including personal stigma, stigma perceived in others, internalised self-stigma, perception of mental disorders as due to weakness, reluctance to disclose to others, perceived dangerousness, desire for social control and desire for social distance (Jorm and Oh, 2009). Other components of stigma include emotional reactions to people with mental disorders and discrimination (Angermeyer et al., 2010; Lasalvia et al., 2013). The current study focuses on aspects of stigma related to labelling, stereotyping and separation aspects of stigma. Several scales to assess these aspects of stigma have been developed, with the Social Distance Scale (SDS: Link et al., 1999) (which assesses the desire to avoid contact with a particular group of people) and the Depression Stigma Scale (DSS; Griffiths et al., 2004), which assesses personal stigma and stigma perceived in others, commonly used in Australia. Previous analyses using data from two large surveys of the Australian population have shown that the latter scale has two components, relating to beliefs that a person with a mental disorder is ‘Weak not sick’ and ‘Dangerous or unpredictable’ (Yap et al., 2014).
The widely acknowledged need to improve rates of help seeking for mental disorders and reduce stigmatising attitudes to people with mental disorders have led to awareness campaigns and psycho-education interventions in a number of countries (Dumesnil and Verger, 2009). Such campaigns often emphasise the biological and genetic causes of mental disorders in order to discourage the view that people with mental disorders are to blame for their difficulties. There have even been calls for campaigns attempting to decrease stigma and normalise depression and other mental disorders by calling them ‘brain diseases’ (Corrigan and Watson, 2004). In recent years, the concept of a ‘chemical imbalance’ as a cause of depression has become widespread, partly due to the efforts of the pharmaceutical industry whose advertising campaigns emphasise the use of antidepressants to correct this imbalance (Deacon, 2009; France, 2007). Surveys of the general public that have included questions exploring beliefs about the causes of depression reveal a high level of agreement with the view that a ‘chemical imbalance’ is a likely cause of depression (Cook and Wang, 2011; Pilkington et al., 2013). Studies examining changes in public attitudes over time have shown rising public acceptance of biological and genetic (biogenetic) explanations for mental disorders (Schomerus et al., 2012).
However, some experts have criticised the emphasis on biological factors as being overly simplistic and argue that public health messages should acknowledge the complex interaction between biogenetic and psychosocial factors (Hinshaw and Cicchetti, 2000). Moreover, in recent years, concern has been raised that the emphasis on biogenetic causes may increase some aspects of stigma (Dietrich et al., 2004; Phelan, 2002; Read et al., 2006). A recent meta-analysis showed that, while biogenetic explanations of mental illness are linked to reduced blame, they are also associated with increased belief in dangerousness and a desire for social distance (Kvaale et al., 2013). These associations were stronger for schizophrenia than for other disorders. In order to inform anti-stigma campaigns, there is a need to further explore the links between causal beliefs about and stigmatising attitudes towards mental disorders, including how these links vary according to disorder.
The current study aimed to use data from the 2011 Australian National Survey of Mental Health Literacy and Stigma to examine the associations between beliefs about the causes of depression, schizophrenia, social phobia and post-traumatic stress disorder (PTSD) and stigmatising attitudes towards people with these disorders.
Methods
The survey involved computer-assisted telephone interviews (CATI) with a national sample of 6019 members of the general community aged 15+. The survey was carried out by survey company The Social Research Centre. The sample was contacted by random-digit dialling of both landlines and mobile phones covering the whole country from January to May 2011. Further details of the methods are given elsewhere (Reavley and Jorm, 2011).
Survey interview
The interview was based on a vignette of a person with a mental disorder. On a random basis, respondents were read one of six vignettes: depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and PTSD. Respondents were also randomly assigned to receive either male (‘John’) or female (‘Jenny’) versions of the vignette. All vignettes were written to satisfy the diagnostic criteria for either major depression or schizophrenia according to DSM-IV and ICD-10 and have been published previously (Jorm et al., 2005b; Reavley and Jorm, 2011).
After being presented with the vignette, respondents were asked what, if anything, they thought was wrong with the person described in the vignette and a series of questions about the likely helpfulness of a wide range of interventions, their health, knowledge of causes and risk factors, contact with people like those in the vignette and stigmatising attitudes. The focus of this paper is respondents’ beliefs about the causes of and stigmatising attitudes towards people with mental disorders.
Personal and perceived stigma
Stigmatising attitudes were assessed with two sets of statements, one assessing the respondent’s personal attitudes towards the person described in the vignette (personal stigma) and the other assessing the respondent’s beliefs about other people’s attitudes towards the person in the vignette (perceived stigma) (Griffiths et al., 2004). The personal stigma items were: (1) People with a problem like (John/Jenny)’s could snap out of it if they wanted. (2) A problem like (John/Jenny)’s is a sign of personal weakness. (3) (John/Jenny)’s problem is not a real medical illness. (4) People with a problem like (John/Jenny)’s are dangerous. (5) It is best to avoid people with a problem like (John/Jenny)’s so that you don’t develop this problem. (6) People with a problem like (John/Jenny)’s are unpredictable. (7) If I had a problem like (John/Jenny)’s I would not tell anyone. (8) I would not employ someone if I knew they had a problem like (John/Jenny)’s. (9) I would not vote for a politician if I knew they had suffered a problem like (John/Jenny)’s.
The perceived stigma items covered the same statements but started with “Most other people believe that…”. Ratings of each were made on a 5-point Likert scale ranging from ‘strongly agree’ to ‘strongly disagree’.
Previous factor analyses using data from the current survey and a similar survey involving young people aged 15 to 25 years have shown that the personal and perceived stigma scales each have two components, relating to beliefs that a person with a mental disorder is ‘Weak not sick’ (items (1), (2), (3) and (5) above) and ‘Dangerous or unpredictable’ (items (4), (5) and (6) above) (Yap et al., 2014). Scale scores were therefore calculated for each of these four scales. Pearson correlations between the scales were as follows: Personal weak not sick and Personal dangerous/unpredictable scales r = 0.40; Personal weak not sick and Perceived weak not sick scales r = 0.07; Personal weak not sick and Perceived dangerous/unpredictable scales r = −0.09; Personal dangerous/unpredictable and Perceived weak not sick scales r = 0.08; Personal dangerous/unpredictable and Perceived dangerous/unpredictable scales r = 0.33; and Perceived weak not sick and Perceived dangerous/unpredictable scales r = 0.62 (all correlations significant at p < 0.001).
Social distance
Self-reported willingness to have contact with the person described in the vignette was measured using the 5-item scale developed by Link et al. (1999). The items rated the person’s willingness to (1) move next door to (John/Jenny); (2) spend an evening socialising with (John/Jenny); (3) make friends with (John/Jenny); (4) work closely with (John/Jenny) on a job; (5) have (John/Jenny) marry into their family. Each item was rated on a 4-point scale ranging from definitely willing to definitely unwilling and a scale score was calculated. Pearson correlations between the Social distance scale and the personal and perceived stigma scales were as follows: Personal weak not sick r = 0.24 (p < 0.001); Personal dangerous/unpredictable r = 0.57 (p < 0.001); Perceived weak not sick r = 0.01 (p = 0.29); and Perceived dangerous/unpredictable r = 0.23 (p < 0.001).
Causal beliefs
The respondents were asked about the likelihood that the following were causes of the problem described in the vignette: ‘A virus or other infection’, ‘An allergy or reaction’, ‘Day to day problems, such as stress, family arguments, difficulties at work or financial difficulties’, ‘The recent death of a close friend or relative’, ‘A recent traumatic event, such as bushfires threatening your home, a severe traffic accident or being mugged’, ‘Problems from childhood, such as being badly treated or abused, losing one or both parents when young or coming from a broken home’, ‘That these sorts of problems are inherited or genetic’, ‘That these sorts of problems are caused by a chemical imbalance in the brain’, ‘Being a nervous person’, and ‘Having weakness of character’. Responses were dichotomised to contrast respondents who perceived the cause as ‘Very likely’ or ‘Likely’ (1), to other respondents (0).
Statistical analysis
Answers to the causal beliefs items were subjected to principal components factor analysis followed by Promax rotation. Inspection of eigenvalues and the scree plot were used to determine the number of components to retain.
Factor scores were subsequently created and used in linear regression analyses in order to examine the relationship between beliefs about the causes of the mental disorders described in the vignettes and the personal and perceived ‘Weak not sick’ and ‘Dangerous/unpredictable’ scales and the Social distance scale. All analyses controlled for age, gender, country of birth and level of education. A significance level of p < 0.01 level was used to avoid type 1 error resulting from multiple comparisons. All analyses were conducted using Intercooled STATA Version 12 for Windows (StataCorp 2011).
Results
Principal components factor analysis yielded four factors with an eigenvalue > 1. Items loading primarily on the first factor were: ‘A virus or other infection’ (0.85), ‘An allergy or reaction’ (0.85). This factor was termed ‘Physical causes’. Items loading primarily on the second factor were: ‘Day to day problems’ (0.74), ‘The recent death of a close friend or relative’ (0.79), ‘A recent traumatic event’ (0.75), ‘Problems from childhood’ (0.62). This factor was termed ‘Psychosocial causes’. Items loading primarily on the third factor were: ‘That these sorts of problems are inherited or genetic’ (0.82), ‘That these sorts of problems are caused by a chemical imbalance in the brain’ (0.77). This factor was termed ‘Biogenetic causes’. Items loading primarily on the fourth factor were: ‘Being a nervous person’ (0.80) and ‘Having weakness of character’ (0.81). This factor was termed ‘Weak or nervous personality causes’.
A summary of linear regressions exploring differences in stigma scale scores according to causal belief factor scores for the depression and depression with suicidal thoughts vignettes is given in Table 1. Results for early and chronic schizophrenia are given in Table 2 and those for social phobia and PTSD are given in Table 3.
Summary of linear regressions (β-coefficients) exploring differences in scale scores according to causal beliefs for the depression and depression with suicidal thoughts vignettes.
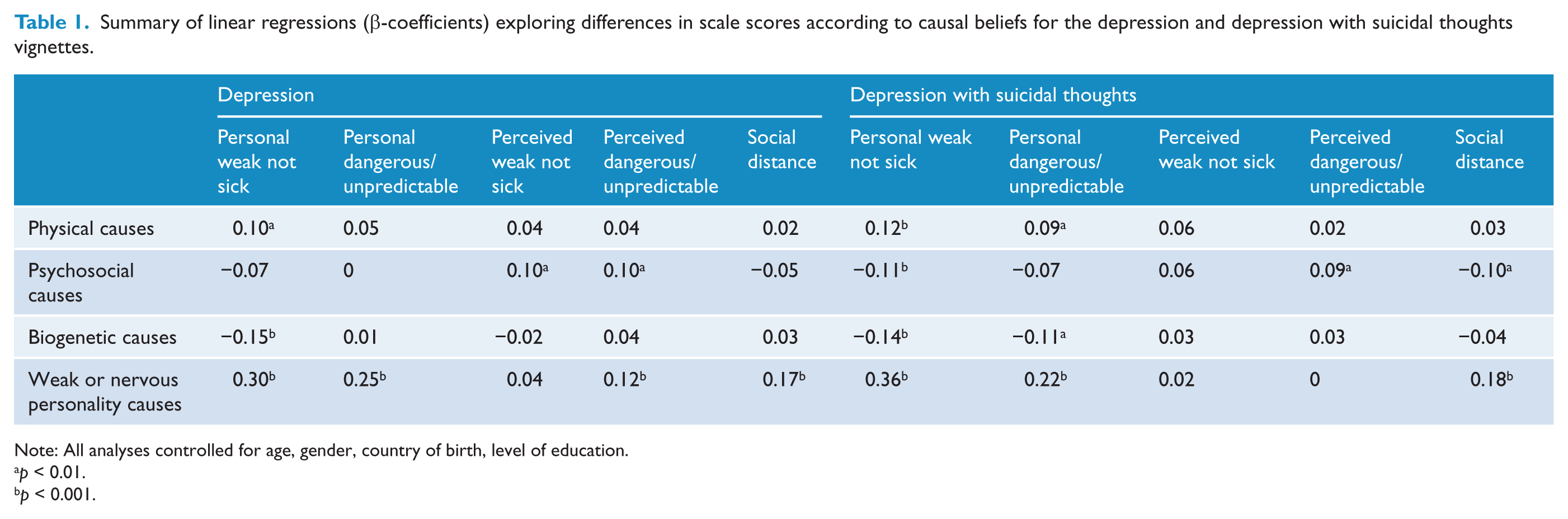
Note: All analyses controlled for age, gender, country of birth, level of education.
p < 0.01.
p < 0.001.
Summary of linear regressions (β-coefficients) exploring differences in scale scores according to causal beliefs for the early schizophrenia and chronic schizophrenia vignettes.
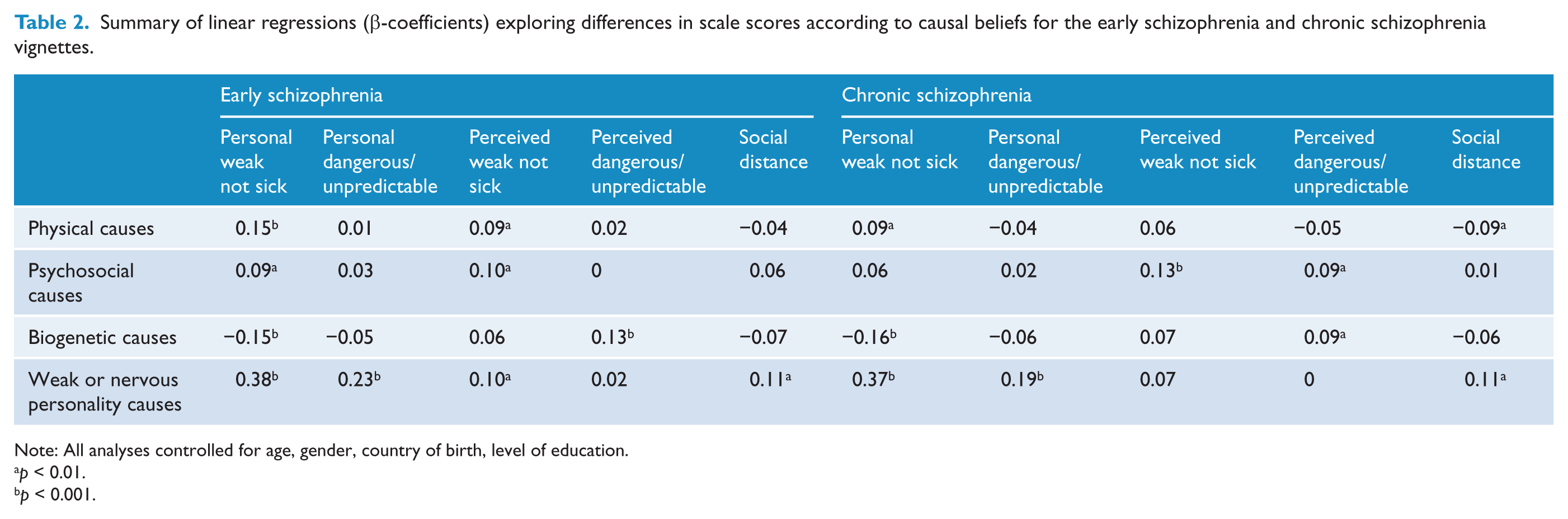
Note: All analyses controlled for age, gender, country of birth, level of education.
p < 0.01.
p < 0.001.
Summary of linear regressions (β-coefficients) exploring differences in scale scores according to causal beliefs for the social phobia and PTSD vignettes.
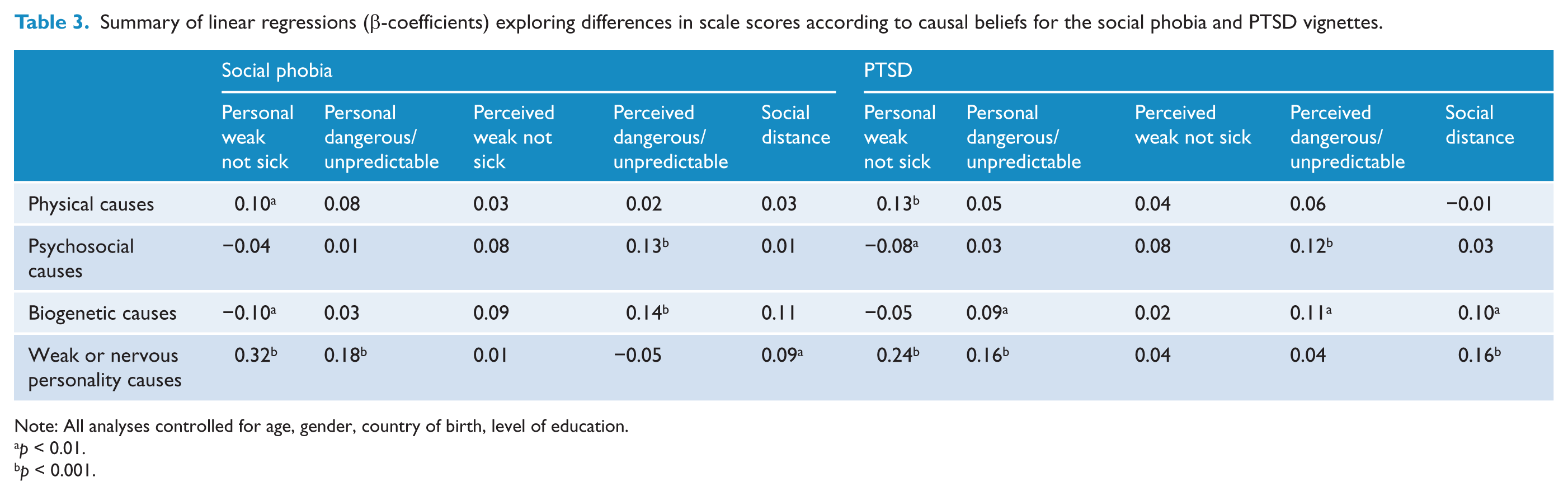
Note: All analyses controlled for age, gender, country of birth, level of education.
p < 0.01.
p < 0.001.
Physical causes
Belief in physical causes of the disorder described in the vignette was associated with higher scores on the Personal weak not sick scale for all vignettes; with higher scores on the Perceived weak not sick scale for the early schizophrenia vignette; with higher scores on the Personal dangerous/unpredictable scale for depression with suicidal thoughts vignettes; and with lower scores on the Social distance scale for the chronic schizophrenia vignette.
Psychosocial causes
Belief in psychosocial causes of the disorder described in the vignette was associated with higher scores on the Personal weak not sick scale for the early schizophrenia vignette and lower scores on the depression with suicidal thoughts and PTSD vignettes; higher scores on the Perceived weak not sick scale for the depression, early schizophrenia and chronic schizophrenia vignettes; higher scores on the Perceived dangerous/unpredictable scale for the depression, chronic schizophrenia, social phobia and PTSD vignettes; and lower scores on the Social distance scale for the depression with suicidal thoughts vignette.
Biogenetic causes
Belief in biogenetic causes of the disorder described in the vignette was associated with lower scores on the Personal weak not sick scale for all vignettes other than the social phobia vignette; lower scores on the Personal dangerous/unpredictable scale for the depression with suicidal thoughts vignette; higher scores on the Personal dangerous/unpredictable scale for the PTSD vignette; higher scores on the Perceived dangerous/unpredictable scale for the early schizophrenia, chronic schizophrenia, social phobia and PTSD vignettes; and higher scores on the Social distance scale for the PTSD vignette.
Weak or nervous personality causes
Belief in weak or nervous personality as a cause of the disorder described in the vignette was associated with higher scores on the Personal weak not sick and Personal dangerous/unpredictable scales for all vignettes; with higher scores on the Perceived weak not sick scale for the early schizophrenia vignette; with higher scores on the Perceived dangerous/unpredictable scale for the depression vignette; and with higher scores on the Social distance scale for all vignettes.
Discussion
This paper reports on a study that used data from a survey of the Australian public to examine the associations between beliefs about the causes of mental disorders and personally held stigmatising attitudes, stigmatising attitudes perceived in others and the desire for social distance from a person described in a vignette of one of the following mental disorders: depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and PTSD. The results showed that belief in a weak or nervous personality as a cause was associated with higher scores on the Personal weak not sick, Personal dangerous/unpredictable and Social distance scales for all vignettes. This is of significance as the previous literature has focused on biogenetic explanations but ignored personality explanations. These results suggest that directly addressing these misconceptions may be useful in reducing stigmatising attitudes towards people with mental disorders. Due to the conceptual overlap between the Personal weak not sick scale and the weak or nervous personality, a Pearson correlation coefficient was computed to assess the relationship between the scale and the weak or nervous personality factor score. This was found to be 0.36 (p < 0.001). In addition, the regression coefficients were recalculated after removing the only item from the Personal weak not sick and Perceived weak not sick scales that specifically mentioned weakness, i.e. ‘A problem like (John/Jenny)’s is a sign of personal weakness’. This only resulted in one difference: for the depression with suicidal thoughts vignette, the negative β-coefficient relating to the association between Personal weak not sick scale scores and belief in psychosocial causes reached significance at the p < 0.01 level. These data suggest that the associations are not simply due to similarities in item content and that the scale and the factor scores are not assessing identical constructs.
The results also showed that belief in biogenetic causes of all the disorders other than PTSD was associated with less stigmatising attitudes as measured by the Personal weak not sick scale. These results may be compared with those of the recent meta-analysis conducted by Kvaale et al. (2013), who examined the links between biogenetic explanations and blame, perceptions of dangerousness and desire for social distance. Their results showed a small to medium negative correlation between endorsing biogenetic explanations and blame and a small positive correlation between biogenetic explanations and desire for social distance. There was also a small to very small positive correlation between biogenetic explanations and perceptions of dangerousness and unpredictability, with subgroup analyses showing the association for schizophrenia and depression. These findings contrast with the current study which showed that biogenetic explanations were not generally associated with belief in dangerousness or desire for social distance (other than for PTSD). It is possible that these differences in findings are also due to variations in awareness-raising approaches taken in different countries. In Australia, beyondblue, a long and relatively successful mental health literacy campaign (Jorm et al., 2005a), emphasises multi-causal explanations for depression (http://beyondblue.org.au) and there were no Australian general population studies included in this section of the Kvaale et al. (2013) meta-analysis. Moreover, associations between causal beliefs are likely to be impacted by cultural factors, for example genetic causes may be associated with higher levels of shame and stigma in some populations (Yang et al., 2013). However, a recent study analysing changes over an 8-year period in stigmatising attitudes in Australia has shown an increase in perceptions of dangerousness and unpredictability (Reavley and Jorm, 2012). The results of the current study reinforce the importance of viewing and addressing stigma towards mental disorders as a multidimensional construct (Yap et al., 2014) and suggest that the increase in beliefs about dangerousness is likely to be due to factors other than an emphasis on biogenetic explanations for mental disorders, and that efforts to address this may need to focus on other areas, including media coverage of mental disorders and violence (Jorm and Oh, 2009; Jorm and Reavley, 2014).
Associations were different depending on the stigma scale used. A notable finding is that personal and perceived stigma are not strongly correlated and are associated differently with causal beliefs. If perceived stigma is conceived as a more socially desirable way of expressing personal stigma, then this is a surprising finding. However, another interpretation, put forward by Griffiths et al. (2006), is that perceived stigma reflects sensitisation to the issue of stigma in society. Griffiths et al. (2006) favoured this interpretation based on the findings comparing Australia with Japan, where the Japanese public had greater personal stigma, while the Australian public had greater perceived stigma. They argued that the greater perceived stigma in Australia was due to media exposure and awareness campaigns which created an exaggerated public perception of the level of stigma in the Australian community.
The results of the current study did not show consistent patterns of association between belief in psychosocial causes and stigmatising attitudes. For the depression with suicidal thoughts and PTSD vignettes, belief in psychosocial causes was linked to a lower likelihood of belief in personal weakness while, for the early schizophrenia vignette, it was linked to an increased belief in personal weakness. Psychosocial causes were also linked to increased scores on the Perceived weak not sick scales for the depression and both schizophrenia vignettes and increased scores on the Perceived dangerous/unpredictable scale for all vignettes other than early schizophrenia. These results suggest that a focus on psychosocial causes of mental disorders may not be a particularly useful strategy for reducing stigma.
Limitations of the study include its cross-sectional nature, which precludes conclusions about causality. A further limitation is the lack of detail on the meaning participants ascribe to the various causal beliefs, e.g. a belief in genetic causes may be interpreted as a single gene, as might occur in some physical diseases (e.g. Huntington’s disease), or may be seen as a more complex interplay between multiple genetic and environmental factors. In addition, stigmatising attitudes were assessed in relation to an unknown person described in a vignette. It is unclear how such beliefs might differ in cases where the person with the disorder is known to the respondent. There is a need for further research into the links between attitudes and behaviours towards people with mental disorders, as these were not assessed in the current study.
Conclusions
The results of the current study suggest that explaining mental disorders as due to personality characteristics is a more important factor in stigma than either biogenetic or psychosocial explanations.
Footnotes
Funding
The study was funded by the Commonwealth Government Department of Health and Ageing. The authors receive salary support from the National Health and Medical Research Council.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.