
Abstract
Objective:
The assessment of the depressive component during mania has become critical for the accurate diagnosis of mixed states, which were defined very narrowly in the past classification systems before Diagnostic and Statistical Manual of Mental Disorders (5th ed.). The aim of this study was to compare socio-demographic, clinical and therapeutic characteristics, as well as clinical and functional outcomes, between manic patients with and without mixed features to validate the relevance of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.) mixed specifier.
Methods:
This is a subanalysis of a multicentre naturalistic study MANía Aguda y COnsumo de Recursos (acute mania and health resource consumption [MANACOR]) on the burden of mania in bipolar patients from four hospitals in Catalonia (Spain). The sample consisted of 169 adult patients presenting a manic episode and systematically assessed during a 6-month period.
Results:
A total of 27% (n = 46/169) of manic patients showed mixed features. Total number of episodes (p = 0.027), particularly depressive and mixed, was greater in manic patients with mixed features, as well as depressive onset (p = 0.018), suicide ideation (p = 0.036), rapid cycling (p = 0.035) and personality disorders (p = 0.071). In contrast, a higher percentage of pure manic subjects were inpatients (p = 0.035), started the illness with mania (p = 0.018) and showed family history of bipolar disorder (p = 0.037), congruent psychotic symptoms (p = 0.001) and cannabis use (p = 0.006). At baseline, pure manic patients received more risperidone (p = 0.028), while mixed patients received more valproate (p = 0.049) and antidepressants (p = 0.005). No differences were found in syndromic recovery at the end of the study. However, depressive change was higher in the mixed group (p = 0.010), while manic change was higher in the pure manic group (p = 0.029). At the end of follow-up, the group with mixed features showed a significant trend towards higher psychosocial dysfunction.
Conclusion:
A total of 27% of manic patients showed mixed features. Groups differed regarding clinical characteristics, course of illness, psychosocial functioning, prescribed treatment and symptom progress. Depressive symptoms in mania should be routinely assessed and considered to guide treatment.
Introduction
Bipolar disorder is a highly heterogeneous illness, with differences not only in the frequency and intensity of mood episodes but also in the symptomatic presentation and illness prognosis. In a longitudinal 2-year study, Baldessarini et al. (2010) reported that unstable, polymorphous states in bipolar disorder predicted an excess of future depression-related morbidity, particularly including mixed states. The coexistence of manic and depressive symptoms is not new in the phenomenology of bipolar disorder. Despite mixed symptoms having been reported since the first descriptions of the disease, they have not always received enough attention. This is very serious if we consider that mixed symptoms seem to influence illness presentation (Swann et al., 2013), outcomes (Baldessarini et al., 2010; Martin-Carrasco et al., 2012) and treatment response (Ouanes et al., 2014; Yildiz et al., 2011). When compared with patients with pure mania, those with mixed mania appear to show a more severe form of bipolar disorder with a worse course of illness: earlier age of onset and more unfavourable outcomes regarding frequency and duration of relapses, time of recovery periods, anxiety and substance use comorbidities, suicide risk and response to treatment (Azorin et al., 2009; Goldberg and McElroy, 2007; Pacchiarotti et al., 2013; Swann et al., 2013; Vieta and Valenti, 2013).
It seems clear, therefore, that the assessment of the possible depressive component during mania will improve accuracy of diagnosis and classification, hopefully leading to a better tailored treatment, better prognosis and improved functioning (Vieta et al., 2014) and contributing to clarifying questions about potential underlying mechanisms (Swann et al., 2013). The identification of symptoms of the opposite sign may reduce underdiagnosis and misdiagnosis of bipolar disorder, often influenced by the complexity and varied manifestation of mixed symptoms as well as by different definitions and terminology used over time according to changes in diagnostic criteria. Compared with the restrictive Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) definition, which required the overlap of symptoms from a full manic and depressive episode, Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) has introduced a broader definition, which seems to better represent the nature of this condition. With the adoption of a mixed categorical–dimensional model, mixed features have become a specifier that can be applied to a current manic, hypomanic or depressive episode in bipolar I or bipolar II disorder when at least three symptoms of the opposite polarity are present.
Identifying subgroups of patients based on phenomenological subtypes could potentially guide the most effective therapeutic interventions in the context of a personalized approach and could help improve outcomes. The aim of this subanalysis, based on a 6-month naturalistic study, was to consider the depressive dimension in a sample of manic patients in order to compare socio-demographic, clinical, illness-course characteristics, psychosocial functioning, prescribed treatment and outcomes between bipolar patients in mania with and without mixed features following DSM-5 criteria.
Methods
This study represents a subanalysis of a naturalistic trial (MANACOR) aimed at describing the general burden (clinical, functional, health resource consumption and costs) associated with manic episodes in bipolar patients from four University Hospitals in Catalonia (Spain) which have a specific catchment area for public health care. The original study combined prospective and retrospective data collection. Details about the methodology are given elsewhere (Hidalgo-Mazzei et al., 2015). This study was started in January 2011 and was completed in December 2013. The protocol was reviewed and approved by the respective hospital ethics committees.
Subjects
The sample involved 169 adult patients from four different psychiatric hospitals and outpatient clinics in Catalonia, Spain. The selected patients were 18 years or older with a type I bipolar disorder, according to Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) criteria, and already included in a systematic follow-up bipolar disorder programme at their respective hospitals. The main inclusion criterion was a present manic episode, defined as having a Young Mania Rating Scale (YMRS) score of ⩾15, which could have been handled in an inpatient or outpatient setting.
Procedure and assessment
Attending psychiatrists of inpatient and outpatient clinics were asked to identify potential patients who met the mentioned inclusion criteria. Individual treatments were determined clinically by each patient’s treating psychiatrist. Information regarding emergency room and outpatient visits, hospital admissions, suicide attempts, sick-leave days and pharmacological treatment prescribed was collected. Socio-demographic data, along with personal and family, medical and psychiatric history, and relevant information about the course of bipolar disorder, were extracted from medical records. Clinical data and employment-functional status were assessed during the manic episode and over the 6-month follow-up. Health resource utilization was afterwards calculated as described in detail elsewhere (Hidalgo-Mazzei et al., 2015).
At baseline and follow-up, the patients were evaluated through standardized clinical instruments, included in the bipolar disorder programme protocols of each hospital involved. The systematic follow-up consisted of periodic appointments with the psychiatrist. This study included a baseline, 1-month (or after discharge in case the patients were hospitalized) and 6-month clinical interviews and assessments through the following instruments: the Spanish version of the YMRS (Colom et al., 2002) to measure the intensity of manic symptoms, the 17-item Hamilton Depression Rating Scale (HDRS-17; Bobes et al., 2003) to measure the intensity of depressive symptoms, the Spanish version of the Clinical Global Impression Scale for Bipolar Disorder (CGI-BP; Vieta et al., 2002) to assess the patient’s global clinical state, the Functioning Assessment Short Test (FAST; Rosa et al., 2007) to evaluate psychosocial functionality and the 4-item Morisky–Green test (Val et al., 1992) to assess treatment adherence. In this subanalysis, we focused on the comparison between manic patients with and without mixed features in the current episode based on DSM-5 criteria.
Data analysis
Statistical analyses were performed with the Statistical Package for Social Sciences (SPSS) version 18.0. In order to make a comparison between manic patients with and without mixed features, descriptive statistics were used to determine means and frequencies for continuous and discrete variables, respectively. Group differences were analysed using independent samples t-test or chi-square, depending on the nature of the variables. All the analyses were two-tailed with alpha set at p < 0.05.
Results
The total sample was composed of 169 subjects in a manic episode, of which 46 (27%) patients had mixed features. Table 1 shows the baseline differences between manic patients with and without mixed features. No differences were found in socio-demographic characteristics such as age, gender and marital status. Except for family history of bipolar disorder, which was higher in the group of manic patients without mixed features, no differences were found when family history of psychiatric illnesses or affective disorders in general were analysed, nor in family history of suicide.
Socio-demographic and clinical data of the sample at baseline.
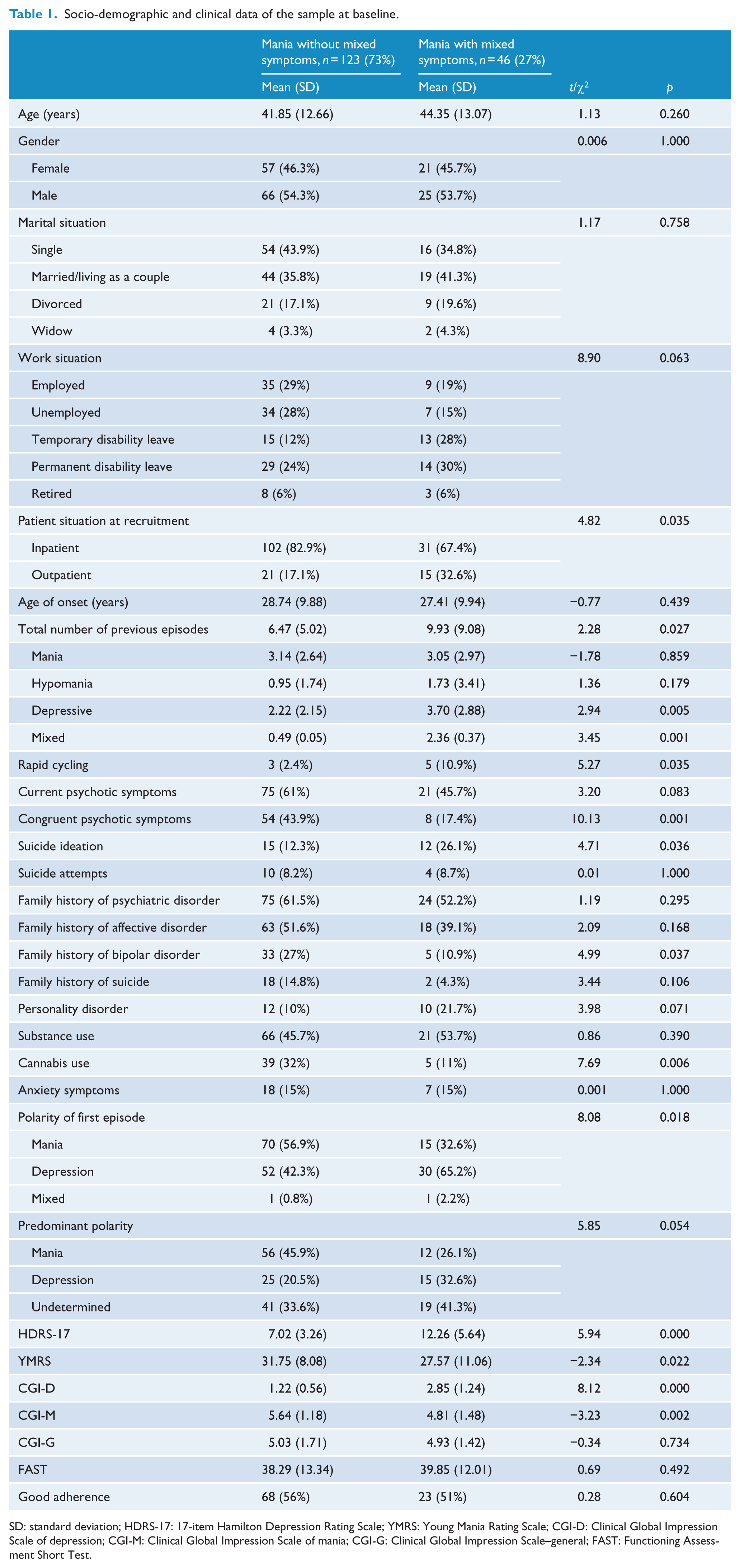
SD: standard deviation; HDRS-17: 17-item Hamilton Depression Rating Scale; YMRS: Young Mania Rating Scale; CGI-D: Clinical Global Impression Scale of depression; CGI-M: Clinical Global Impression Scale of mania; CGI-G: Clinical Global Impression Scale–general; FAST: Functioning Assessment Short Test.
Overall, there were more inpatients in the group with pure mania (83%). Among subjects with mixed features, 67% were inpatients. Although both groups started the illness at a similar age, the total number of previous episodes was significantly greater in the manic patients with mixed features, who also had a higher incidence of past rapid cycling. When the type of episodes was analysed, significant differences were found particularly for previous depressive and mixed episodes. Significant differences were observed in the polarity of first episode, a higher percentage of pure manic patients showing a first manic episode (57%), while a higher percentage of patients with mixed features had had a first depressive episode (65%). Considering the previous course of the illness, a significant trend was found (p = 0.053), with 45% of the pure manic patients having manic predominant polarity compared with 26% of the patients with mixed features; depressive predominant polarity was present in 20% of the patients with pure mania compared with 33% of the patients with mixed features. The rest of the total sample (around 36%) did not have predominant polarity, 41% of the patients with mixed features being in the undetermined category.
History of psychosis tended to be higher in manic patients without mixed features; a significant difference was obtained when mood congruence of psychotic symptoms was evaluated, congruent symptoms being more prominent in patients with pure mania. Although groups did not differ in the number of suicide attempts, there was a higher incidence of suicide ideation in manic patients with mixed features. No differences were found regarding substance abuse, although the subgroup with pure mania showed a higher use of cannabis when different substances were analysed separately. Groups were comparable in terms of anxiety symptoms. A significant trend was observed in personality disorders, patients with mixed features showing higher axis II comorbidity.
During the manic episode, 98% of the total sample was taking antipsychotics, 84% mood-stabilizers, 44% lithium, 6% antidepressants and 63% benzodiazepines. Concerning specific pharmacological treatments, pure manic patients received more risperidone (30% vs 13%; p = 0.028), while manic patients with mixed features received more valproate (48% vs 31%; p = 0.049), olanzapine (46% vs 30%; p = 0.076) and antidepressants (17% vs 1.6%; p = 0.005). No differences between groups were found regarding lithium, carbamazepine, asenapine, quetiapine and benzodiazepines.
In terms of symptom outcomes (Figure 1), depressive scores assessed by the HDRS were higher for the mixed group at each assessment point, although significance disappeared at the end of the follow-up (t = 1.93; p = 0.062). Regarding manic symptoms, only at baseline scores in the YMRS were significantly higher for the group without mixed features (t = −2.34; p = 0.022). When changes from baseline to the end of follow-up were compared, significant differences were obtained in both depressive (t = −2.65; p = 0.010) and manic symptoms (t = 2.23; p = 0.029), depressive change being higher for the mixed group while manic change being higher for the pure manic group. Similarly, groups differed in the changes from baseline to the end of the follow-up assessed through the CGI of mania (t = 2.89; p = 0.005) and depression (t = −3.64; p = 0.001) but not in the CGI general (t = 1.05; p = 0.293).
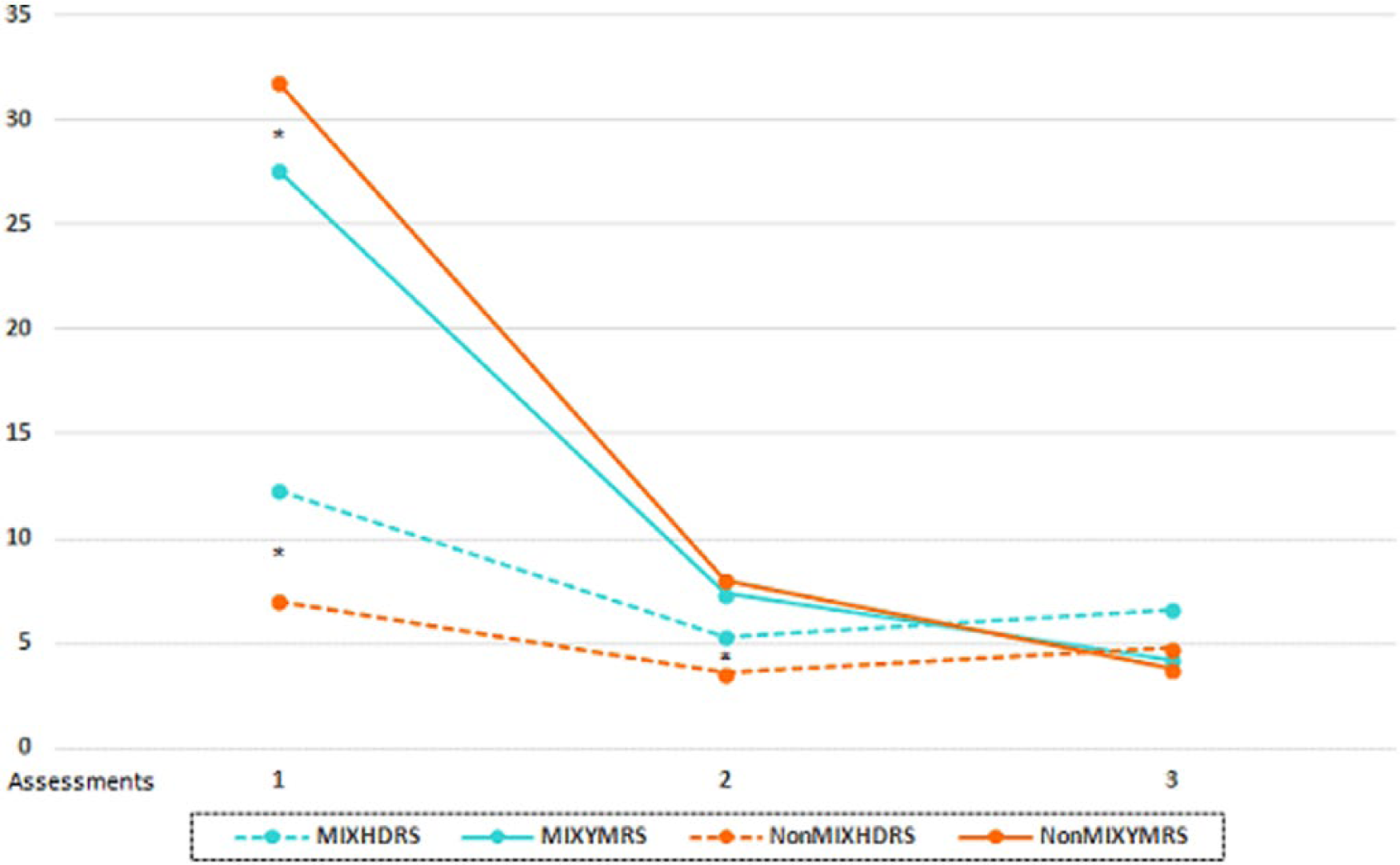
Symptom severity over 6 months.
With respect to psychosocial functioning, no differences were found between groups in the total FAST scores during the study except for a trend at the end of the follow-up that indicated poorer scores for the group with mixed features (28.56 vs 24.23; t = 1.73; p = 0.085). The number of days off work between the first and the second visit also tended to be higher (t = 1.97; p = 0.059) for the group who showed mixed features (mean: 24, standard deviation [SD]: 11.01) compared with the patients with pure mania (mean: 18.50, SD: 7.85).
Around 50% of the sample showed good adherence at baseline, with no significant differences between manic patients with or without mixed features (Table 1). Groups did not differ in treatment adherence at any assessment point and both showed a better adherence during the follow-up. The percentage of good adherence was greater in the second visit (79% of the patients with pure mania and 73% of the patients with mixed features) than in the last assessment (61% of the patients with pure mania vs 56% of the patients with mixed features).
At the end of the study, both groups were compared in terms of clinical and functional outcomes divided as follows: syndromic (i.e. full clinical syndrome, with HDRS scores greater than 17 or YMRS greater than 11); subsyndromic (HDRS scores between 9 and 16 or YMRS between 7 and 11); euthymic (HDRS scores lower than 9 and YMRS lower than 7); and functional recovery (FAST scores lower than 12). At 6-month follow-up, both groups had exactly the same proportion of syndromic patients, while patients with mixed features showed more subsyndromal symptoms, lower achievement of euthymia and lower functional recovery; however, these differences did not reach statistical significance (Figure 2). Non-significant differences were found between both groups when health resource consumption, pharmacological treatment costs and total direct costs were calculated by the procedure described in further detail elsewhere (Hidalgo-Mazzei et al., 2015).
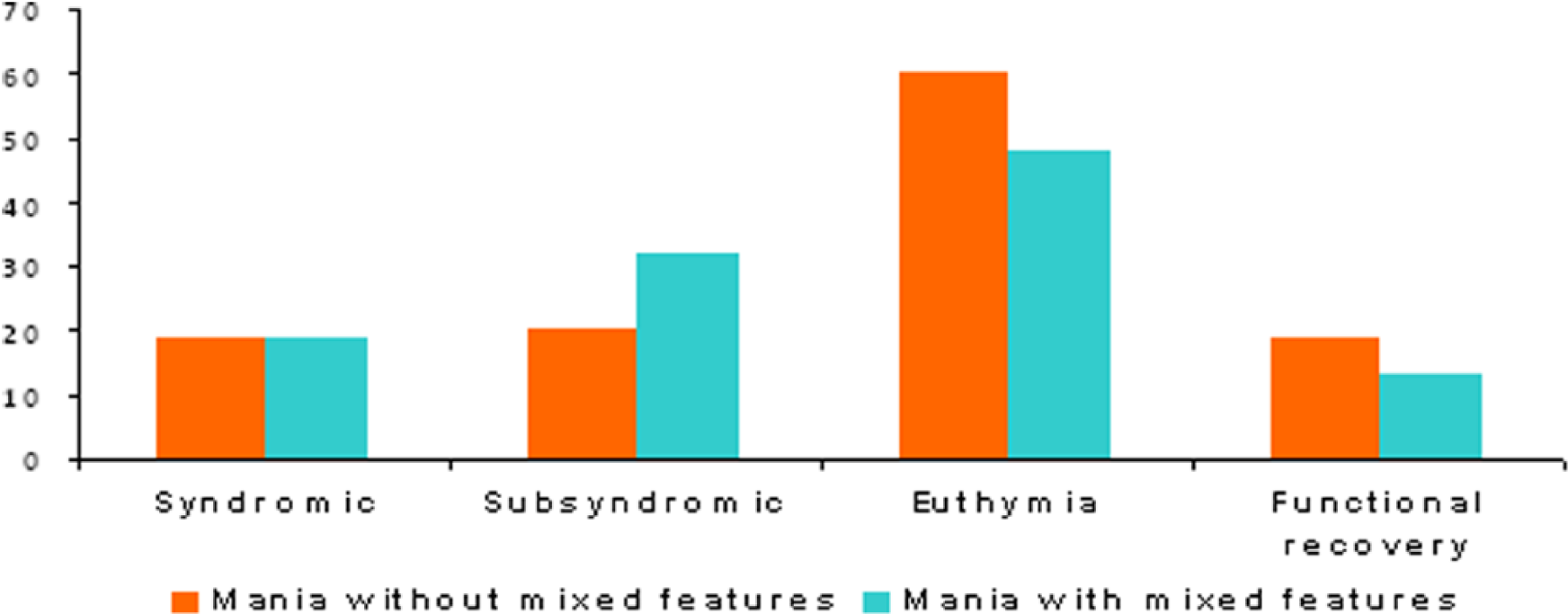
Percentage of patients syndromic, subsyndromic, euthymic and functionally recovered at the end of the follow-up.
Discussion
This study showed that in a sample of patients with acute mania, 27% of the subjects had mixed features according to DSM-5 criteria. Although at the end of the study both groups had an identical proportion of patients in a syndromic phase, the groups with and without mixed features differed in clinical characteristics, course of illness, psychosocial functioning and prescribed treatment, as well as in the progress of symptoms during the follow-up.
Despite the fact that the majority of studies indicate that the illness prognosis is worse in patients with mixed symptoms, data are still scarce and highly variable depending on the diagnostic criteria used (DSM-IV-TR, International Classification of Diseases, 10th revision (ICD-10), McElroy criteria; Vieta and Morralla, 2010). This study indicates that between a quarter and a third of patients assessed during a manic episode have mixed features. Previously, a similar percentage was described by Azorin et al. (2009), who found that 34% of the bipolar subjects had mixed symptoms, defined as a score of over 3 on the CGI-BP-mania and CGI-BP-depression scales. With a sample of bipolar inpatients, Pacchiarotti et al. (2011) observed that 34.3% of the patients had a history of pure manic episodes, 39.5% had both manic and mixed episodes and 26.1% had a history of pure mixed episodes according to DSM-IV criteria. Similarly, 37% of the patients fulfilled DSM-IV criteria of mixed episode in a Spanish sample (González-Pinto et al., 2011). In all, 30% of mixed mania, defined as at least two depressive symptoms, had been described in a study carried out by Hantouche et al. (2006).
No differences were found in demographic characteristics such as age and gender. Although some studies have reported that women are overrepresented in mixed mania (Hantouche et al., 2006; McElroy et al., 1995), other authors did not support this finding (Valenti et al., 2011) and suggest that gender ratios may be different due to variations in study population, setting and diagnostic criteria used (González-Pinto et al., 2011). Despite both groups having a similar age of onset, in this study, the total number of previous episodes was higher in manic patients with mixed features. This is one of the most consistent findings in the literature (Azorin et al., 2009; González-Pinto et al., 2011; Hantouche et al., 2006; Pacchiarotti et al., 2011). As expected, when specific types of episodes were compared, a greater number of previous depressive and mixed episodes were found in this group. Similarly, and according to Azorin et al. (2009), the history of rapid cycling was more common in patients with mixed features. Significant differences were observed in the polarity of the first episode, a higher percentage of pure manic patients showing a first manic episode, while a higher percentage of patients with mixed features had had a first depressive episode. Defining predominant polarity as at least twice as many episodes of one pole over the other (Colom et al., 2006), 41% of the mixed patients were in the undetermined category. In contrast, Perugi et al. (2014) reported that 61.9% of the mixed bipolar patients were neither predominately manic nor predominately depressive, although they used factor analysis to define phenomenological subtypes. In our study, a significant trend was found between groups, manic patients without mixed symptoms more often having manic predominant polarity than manic patients with mixed features. Previously, Baldessarini et al. (2010) had described a poor prognosis for patients presenting mixed states, their morbidity during follow-up being far more depression or dysthymia than mania or hypomania. They found evidence that both initial depression-related and mania-related presentations were strongly predictive of later, similar morbidity types and by strong excesses of similar morbidity during follow-up. Polarity of the first episode (Calabrese et al., 2004; Daban et al., 2006) and predominant polarity of subsequent episodes over the course of bipolar disorder (Baldessarini et al., 2012; Colom et al., 2006) seem to be related to clinical factors and act as a predictor of long-term morbidity, therefore having therapeutic implications (Nivoli et al., 2013).
Regarding affective symptoms, there were differences between groups at baseline, with depressive scores being higher in the mixed group and manic scores being higher in the group without mixed features. As expected, both manic and depressive symptoms were reduced at the end of the follow-up, and significant differences between groups disappeared. This could be explained because both groups had a similar and adequate response to treatment. Similarly, groups differed in the changes from baseline to the end of the follow-up assessed through the CGI of mania and depression but not in the CGI general. Although at the end of the study manic patients with mixed features showed poorer clinical outcomes, the differences did not reach statistical significance, and the percentage of patients in a syndromal state was identical. These results contrast with other studies which found that mixed states had a significantly lower recovery rate than pure mania (Azorin et al., 2009), although our definition of syndromic state goes beyond the recovery of the manic phase and referred to the absence of any kind of acute episode, including both (hypo)mania and depression, at the end of the follow-up.
Regarding functional outcomes, a trend to significance (p = 0.085) was observed at the end of follow-up, with the mixed features group showing poorer scores (28.56 vs 24.23) in the total FAST. There was also a tendency to higher number of days off work in this subgroup of patients, which confirms the greater functional impairment in patients with mixed features. The association between mixed episodes and poor psychosocial functioning had been previously described (Rosa et al., 2009). Although differences between groups are not remarkably high, it seems that patients with mixed features require a longer time to achieve good psychosocial functioning. This is not surprising if we consider that both syndromal and residual depressive symptoms appear as one of the factors most robustly associated with poor functional outcome (Bonnin et al., 2010; Gitlin et al., 2011; Judd et al., 2005; Martino et al., 2009; Reinares et al., 2013a; Simon et al., 2007). This study points out that although clinical recovery is similar between patients with and without mixed features, functional recovery seems to be slightly worse or perhaps slower to achieve in the subgroup of manic patients with mixed symptoms. Considering that the cut-off point of the overall FAST indicative of significant disability has been established above 11, it is clear that the sample of this study showed a very poor psychosocial functioning at 6-month follow-up. Only 18% of the whole sample completely recovered their psychosocial functioning. These results are similar to those described by Rosa et al. (2011), where 26% of the patients achieved functional recovery despite most of them having achieved clinical remission of acute symptoms. Furthermore, findings also highlight the previously reported gap between syndromal and functional recovery (Rosa et al., 2011; Tohen et al., 2000), the latter being much more difficult to obtain, for the whole sample. Finally, the results indicate the negative impact of manic episodes on functional outcomes as other articles had previously remarked (Bonnin et al., 2014) and the need for relapse prevention.
With respect to history of psychosis, and according to Hantouche et al. (2006), congruent symptoms were more prominent in manic patients without mixed symptoms. No significant differences were observed with regard to the presence of anxiety, in contrast with previous findings (Cassidy, 2010). We cannot rule out that an accurate assessment of anxiety through the use of specific measures could have led to differences. Recently, Malhi et al. (2014) recommended the inclusion of standardized measures of distractibility and psychomotor agitation for the study of mixed states. It was interesting to observe that although groups did not differ in the number of previous suicide attempts, there was a higher incidence of suicide ideation in manic patients with mixed features. Other studies, however, have found that patients with mixed symptoms show not only higher suicide ideation but also a higher number of suicide attempts (Azorin et al., 2009; Baldessarini et al., 2012; Hantouche et al., 2006; Pacchiarotti et al., 2011; Undurraga et al., 2012). We could hypothesize that in a sample of depressive mixed states instead of manic mixed states results might be different. No differences were found in substance abuse between both groups although when different substances were analysed separately, the subgroup without mixed features showed a higher use of cannabis. The selective association of cannabis with manic or hypomanic morbidity but not depressive symptoms had been previously reported (Baethge et al., 2008), as well as the role of cannabis to increase the risk of subsequent manic symptoms (Henquet et al., 2006). It is worth mentioning that in the study by González-Pinto et al. (2011), age of onset seemed to mediate some of the factors related to outcome in mixed episodes, and they found that the differences between groups for substance abuse and suicide attempts disappeared after adjusting for age of onset. In this study, age of onset was very similar for both groups although current age was slightly but not significantly younger in those with pure mania. A significant trend was observed in personality disorders, patients with mixed features showing a higher comorbidity. Other authors have found a significantly greater comorbidity with axis II disorders in patients with mixed episodes (Valenti et al., 2011). Hantouche et al. (2006) stated that mixed mania was characterized by high frequency of past diagnostic errors, particularly those of anxiety and personality disorders. Although it may not be the case in our sample, as it was taken from systematic follow-up programmes, this potential error should always be taken into account. Except for family history of bipolar disorder, which was higher in the group of patients with pure mania, no differences were found when family history of psychiatric illnesses, affective disorders or family history of suicide was analysed.
In terms of treatment, 98% of the patients were taking antipsychotics, 84% mood-stabilizers, 44% lithium, 6% antidepressants and 63% benzodiazepines, which is consistent with international studies on current prescription trends (Vieta et al., 2013). No differences between groups were found regarding specific agents such as lithium, carbamazepine, asenapine, quetiapine and benzodiazepines. However, a higher percentage of manic patients without mixed features received risperidone, while the percentage was higher for manic patients with mixed features to receive valproate, olanzapine and antidepressants. The figures about the latter are worth mentioning as in bipolar disorder the efficacy and safety of antidepressants are still controversial (Reinares et al., 2013b; Vazquez et al., 2013). In this study, although the number of patients with antidepressants was higher in those with mixed features (17.4% vs 1.6%), its use was relatively low compared with previous studies (Rosa et al., 2010). For example, in the European Mania in Bipolar Longitudinal Evaluation of Medication (EMBLEM) study, 36% of the total sample received antidepressants at baseline, and at 24 months, 55% of the patients with mixed states and 27% of those with pure mania were receiving antidepressants (Azorin et al., 2009). The results of the current naturalistic study are more in accordance with clinical guidelines and expert consensus which recommend avoiding the use of antidepressants in manic patients with mixed features (Pacchiarotti et al., 2013).
The data obtained in this study showed that treatment adherence was very poor at baseline, only around 50% of the patients had good adherence and no differences between groups were found. This figure is similar to those from other studies indicating that between 30% and 50% of the individuals do not fully adhere to prescribed prophylactic treatments (Murru et al., 2013). It is not surprising that the percentage is in the high range as patients were in an acute episode at baseline. Although in the second visit around 75% of the sample showed good adherence, the rate decreased again at the end of follow-up, with 61% of good adherence in patients with pure mania and 56% in patients with mixed features. Improving adherence still represents a challenge in bipolar disorder (Berk et al., 2010), highlighting the need for an integrative approach in which pharmacological treatment was complemented with psychological interventions in order to obtain a better prognosis of the illness (Reinares et al., 2014).
In bipolar disorder, outcomes are highly variable depending on which endpoints are determined. One of the strengths of this study was that all syndromic, symptomatic and functional variables were included in order to obtain a global picture of the illness prognosis. In addition to this, this study also assessed the economical burden, non-significant differences being found between both groups in terms of costs, although this issue has been explored in further detail elsewhere (Hidalgo-Mazzei et al., 2015). However, some limitations should be considered such as the fact that only patients with bipolar I disorder were included, the lack of a long-term follow-up as the duration of the study was 6 months only, the absence of a systematic use of standardized instruments to assess specific symptoms such as anxiety and the fact that pharmacological treatment was introduced in a naturalistic way which makes it difficult to control for its potential impact on different outcomes. Nevertheless, naturalistic cohorts may serve as useful representations of current clinical practices and results. Finally, due to the exploratory nature of the study, multiple comparisons were analysed without multiplicity adjustment, and therefore, the chances of detecting a non-existent effect cannot be ruled out.
Despite the previous limitations and the fact that the percentage of syndromic recovery at the end of the study was the same for both groups, the findings suggest that even when only a few symptoms (at least three) of the opposite sign were used to define mania with mixed features, this subpopulation seems to represent a group with a differential clinical history, course, psychosocial and symptom progress compared with patients with pure mania, supporting the current approach of the DSM. Due to the high severity of this condition, the depressive dimension should be assessed and taken into consideration from the very beginning as well as its potential implications for therapeutic decision-making which requires further research. Similarly, future studies should be carried out in order to assess depression with or without concurrent manic symptoms.
Footnotes
Declaration of interest
Professor Eduard Vieta is a consultant or grant recipient with Almirall, Astra-Zeneca, Bristol-Myers-Squibb, Elan, Eli Lilly, Ferrer, Forest Research Institute, Gedeon Richter, Glaxo-Smith-Kline, Janssen-Cilag, Jazz, Lundbeck, Merck, Novartis, Otsuka, Pfizer, Roche, Sanofi, Servier, Schering-Plough, Shire, Sunovion, Takeda, Teva and United Biosource Corporations. Dr Juan Undurraga has been a speaker for Janssen-Cilag. Other authors have no conflicts of interest to declare. All the authors are responsible for the content and writing of this article.
Funding
This study was partially supported by the postdoctoral fellowship Beatriu de Pinós granted by the Agency for Management of University and Research Grants (AGAUR), agency of the Secretariat of Universities and Research under the Department of Economy and Knowledge of the Catalan Government (Generalitat de Catalunya) and the Marie Curie-COFUND actions of the Seventh Framework Programme of Research and Technological Development of the European Union; as well as the Biomedical Research Networking Centres (CIBER) and the Consolidated research groups 2014 SGR 398; and the Spanish Ministry of Economy and Competitiveness (PI12/0091) PN 2008–2011, Instituto de Salud Carlos III, Subdirección General de Evaluación y fomento de la Investigación; Fondo Europeo de Desarrollo Regional. Unión Europea, Una manera de hacer Europa. Dr Mur would like to thank the Instituto de Salud Carlos III, Spanish Ministry of Economy and Competitiveness for her research grant FIS-MSC Grant (PI11/01956). This research has been funded by Lundbeck.