
Abstract
In a cyclical and recurring illness such as bipolar disorder, prodrome detection is of vital importance. This paper describes manic and depressive prodromal symptoms to relapse, methods used in their detection, problems inherent in their assessment, and patients’ coping strategies. A review of the literature on the issue was performed using MEDLINE and EMBASE databases (1965–May 2006). ‘Bipolar disorder’, ‘prodromes’, ‘early symptoms’, ‘coping’, ‘manic’ and ‘depression’ were entered as key words. A hand search was conducted simultaneously and the references of the articles found were used to locate additional articles. The most common depressive prodromes are mood changes, psychomotor symptoms and increased anxiety; the most frequent manic prodromes are sleep disturbances, psychotic symptoms and mood changes. The manic prodromes also last longer. Certain psychological interventions, both at the individual and psychoeducational group level, have proven effective, especially in preventing manic episodes. Bipolar patients are highly capable of detecting prodromal symptoms to relapse, although they do find the depressive ones harder to identify. Learning detection, coping strategies and idiosyncratic prodromes are elements that should be incorporated into daily clinical practice with bipolar patients.
Because of its cyclical and recurring nature, bipolar disorder is a serious illness that causes differing levels of hardship to an important number of patients. Since the introduction of lithium, which has proven effective beyond any doubt in the prevention of manic and to a lesser degree depressive episodes, in the last few years new mood stabilizers have appeared to prevent relapse and recurrence in bipolar disorder. The ideal mood stabilizer, however, has still to be found. Work should, therefore, continue on other methods of relapse control.
Early detection by patients of the first symptoms or signs of relapse, called prodromes, is one very important such method. The duration of a prodrome is defined as the time interval between the recognition of the first symptom and the moment when the symptoms of an episode are at their most intense [1, 2]. There are different ways of categorizing them, for example as behavioural, psychological, cognitive, affective or idiosyncratic [3–6]. The ability to detect prodromes is part of the concept of insight. Insight is not an all-or-nothing construct but consists of three components: recognition that one has a mental illness; compliance with treatment; and the ability to relabel unusual mental events as pathological [7]. Adequate insight may allow a patient to better handle their illness and can influence their functioning [8].
In psychiatry, research on prodromes was initially directed to the field of schizophrenia, with the objective of making possible early therapeutic intervention and preventing the first stages from becoming full-blown episodes. In 1980, Herz and Melville did retrospective interviews with 145 schizophrenia patients and 80 family members about the period preceding a relapse event, finding that most were able to describe a prodromal period [9]. To this end, they developed and validated an early symptom questionnaire, a structured interview with some open questions, which proved useful for prevention [10]. In the case of bipolar disorder, the first studies focused strongly on mania [1]. As early as the 1960s, Jacobson described a program for the early detection and control of hypomanic episodes based on individual-prodrome assessment and the intermittent use of lithium [11].
Over the last few years, this topic has received more and more attention due to the increased use of psychoeducation groups in bipolar disorder and the publication of several articles, reporting significant benefits obtained when patients are taught techniques for the early detection of relapse signs [12–15]. Some findings provide a rationale for the study of relapse prodrome. To know if certain variables concerning patients’ behaviour toward their illness were predictive of admission, 50 patients were interviewed upon admission and over the following 12 months. The characteristics that distinguished the 36 patients who were again admitted later on were: more past hospital admissions; higher scores indicating difficulties recognizing and responding to early symptoms of relapse; and less accepting of medication [16].
This article presents a review of the literature about the prodromes preceding both manic and depressive phases, their duration, and patient coping strategies.
Methods
A literature review was conducted. Databases searched were: MEDLINE and EMBASE (1965–May 2006). The search used the words ‘bipolar disorder’, ‘prodromes’, ‘early symptoms’, ‘manic’ and ‘depression’. A hand search was conducted simultaneously and the references of the articles found were used to locate additional articles.
Retrospective methods
One of the most often quoted studies on bipolar prodromes is Smith and Tarrier [3]. They used a semi-structured interview and a 40-item questionnaire consisting of 15 depressive and 15 manic symptoms and 10 cross-episode symptoms. These 40 symptoms included eight that indicated the emergence of psychotic symptoms, such as ‘feeling very religious’ or ‘feeling in another world’, while others assessed neurotic symptoms, such as ‘lots of aches and pains’ or ‘worrying a lot’. Subjects were also asked about other symptoms not included in the list, especially any idiosyncratic experiences. Symptoms were rated on a severity scale from 0 = absent, 1 = mild, to 2 = strong. The questionnaire was retrospective but did have adequate predictive validity [17].
Another retrospective study looked at patients’ ability to describe in detail the development of their own symptoms. It used a semi-structured interview that rated on a 6-point scale from bad to very good patients’ ability to recognize and respond appropriately to initial symptoms of relapse [16]. Other studies used open self-administered questionnaires, in which patients spontaneously listed and described in detail specific prodromal symptoms of previous episodes [1, 4, 6].
Advantages
This approach lets subjects provide the symptoms they best remember and, by allowing each case to be personalized, makes it possible to point out more individual differences. Furthermore, when scoring scales are used, finding can be compared.
Some questionnaires include a section where patients can describe their own specific symptoms. For example, in one of the major studies, some patients identified specific symptoms such as getting very angry with one's ex-wife, feeling increased sensitivity to racism, or cutting one's own face [3]. Other studies using descriptive methods yielded symptoms such as getting involved in other people's problems or getting irritated specifically with one's husband [4], feeling the need to bathe more often every day or craving certain foods [18].
Disadvantages
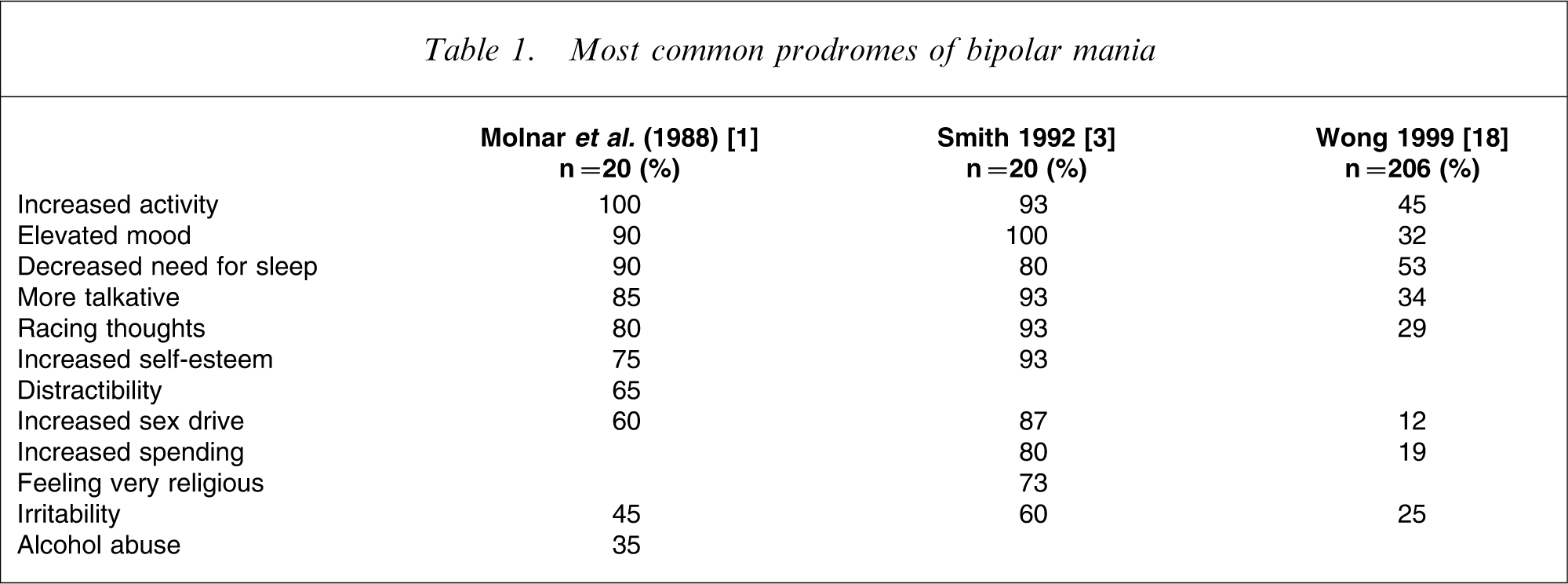
One of the disadvantages of this type of study is that when lists of possible symptoms are used, patients tend to report more prodromes than when interviews are used (Table 1). These studies are also affected by the inescapable bias of memory; it is well known that the further a memory is removed in time, the more imprecise it is [19]. The use of predetermined lists also entails the risk of patients reporting symptoms similar to their own but less intense, thereby losing the opportunity to report idiosyncratic symptoms.
Most common prodromes of bipolar mania
Prospective methods
Prospective studies include some noteworthy methods such as that of Altman et al., a naturalistic study that gathered data from 19 recently hospitalized bipolar patients who were followed for 9 months after their release [5]. Information was collected on the 4 months preceding manic and depressive episodes, and compared with the same period in patients who had suffered no relapse, using the Brief Psychiatric Rating Scale. Significantly higher levels were found of a factor called ‘unusual thought content’, which refers to ideas of reference and delusions before manic relapses, while depressive relapses were preceded by higher levels of conceptual disorganization, referring to confused, disconnected or disorganized speech. These data indicate that, although mood changes are typical symptoms of bipolar relapse, small but significant alterations in thought processes are detected before a relapse that may precede mood changes and, thus, serve as ‘leading indicators’. Another prospective study also showed consistent prodromal symptoms of manic or depressive relapse between 2 and 4 weeks before a full episode in the majority of patients [20].
Advantages
One of the advantages of prospective studies is that they make it possible to determine if some of the common prodromal symptoms are reported reliably across time. In fact, one study was conducted with this objective in mind. Forty bipolar patients were interviewed about their prodromes and coping strategies in a basal assessment and another one 18 months later. With the exception of one cognitive item (increased self-esteem), bipolar patients were able to report mania prodromal symptoms reliably with a period of 18 months apart. The studies’ findings highlight the importance of prodrome detection, because two of the most frequent items – no need to sleep, and more goal-directed behaviour – are easily detectable by patients or family members [15].
Prospective studies can be further enhanced by the use of both self-applied and non-self-applied instruments, thereby increasing sensitivity [21].
Results
Prodromes and bipolar depression
All studies conducted on this topic point out that most bipolar patients can identify the early symptoms of bipolar depression, with an average of 82% [1, 3, 22], although they find it harder to detect the prodromes of depression than those of mania [4]. According to the review by Jackson et al., after analyzing three studies that record the percentages reported by patients [1, 3, 4], the average prevalence of these symptoms would be: mood changes (48%), psychomotor symptoms (41%), increased anxiety (36%), appetite changes (36%), suicidal ideas (29%), sleep disturbances (24%) and other symptoms in 22% [22].
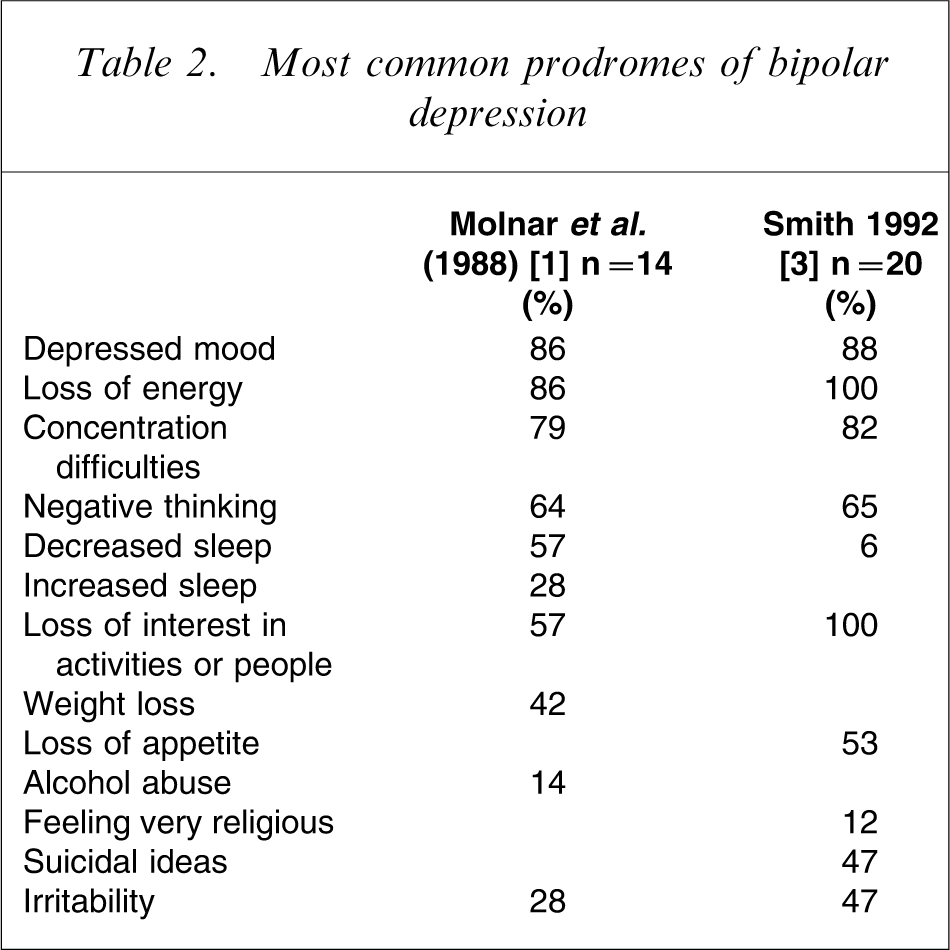
Two of the pioneering studies list as the most frequent depressive prodromes, appearing in 100% of patients [3], anergia, low self-esteem and social isolation, or depressive mood, anergia and loss of concentration [1]. Other studies found cognitive symptoms to be the most frequent [6]. Table 2 presents the most relevant data.
Most common prodromes of bipolar depression
Bipolar patients tend to report a pattern of depressive prodromes very individualized and diverse. This may be due to a lack of qualitative differences between depressive prodromes and the residual symptoms of depression, making it more difficult for patients to distinguish one from the other. Furthermore, the high numbers of patients incapable of detecting are probably attributable to the presence of residual depressive symptoms, characterized by a gradual impairment of functioning and a slow and stealthy emergence of bipolar depression [23]. Other authors point out that, while manic prodromes are very conspicuous, early depression symptoms (such as loss of interest in work or social relations) can be subtle and develop gradually over weeks or months, making their detection more complicated. Also, cognitive and somatic depressive symptoms are more difficult to identify [15].
The duration of depressive prodromes varies enormously depending on the type of study. Data range from 2 to 365 days, with great individual variability [1, 3, 5, 24]. As for the difference between unipolar and bipolar depressions, some studies have found bipolar depressive episodes to appear faster than their unipolar counterparts [24, 25].
Prodromes and mania
In the case of mania, all studies tackling this subject find that most bipolar patients are able to point out manic prodromes. Although the samples used tend to be small, this finding is solid [1, 3, 5].
The previously quoted review by Jackson et al. [22] of several studies shows that between 75 and 100% of patients were able to identify one or more prodromal symptoms of mania. The majority identified sleep disturbances as a prodromal indicator of mania. The symptoms were, by order of frequency: sleep disturbances (77%), psychotic symptoms (47%), mood changes (43%), psychomotor symptoms (34%), others (30%), appetite changes (20%), and increased anxiety (16%). In Molnar's article [1], the most often cited manic prodrome was increased activity, followed by elevated mood. In general, the majority of studies name sleep disturbances as the most prominent. It is, therefore, important to monitor this factor that Wehr et al. considered a vital pathway in the genesis of mania (Table 1) [26].
Another study conducted for the validation of a coping inventory identified the following most frequent symptoms: reduced sleep, increased activity, over talkative, euphoria, racing thoughts/ideas going too fast, and irritability, which are very similar to those found in previous articles [18].
The majority of studies indicate that patients have less difficulty pointing out manic prodromal symptoms than prodromes of depression [15]. This may be due to the fact that most are behavioural and, as such, more easy detectable by patients than cognitive or affective symptoms. Correspondingly, studies have found that teaching bipolar patients to detect early warning signs and to seek help is more helpful in preventing manic than depressive episodes [14].
Duration ranges from 1 to 120 days [1, 3, 27–29]. Traditionally, mania is considered to appear suddenly, usually in 1–7 days [27, 30, 31]. However, results vary. Thus, authors such as Molnar et al. find that manic prodromes are significantly longer than depressive prodromes (20.5±21.29 days, range = 1–84 days, n = 20, compared with 10.96±8.57 days, range = 2–31 days, n = 14) [1]. Other studies come to the same conclusion and report longer manic prodromes than depressive (28.9 and 18.8 days, respectively) [3]. The same result is obtained by studies comparing the appearance of mania with that of unipolar or bipolar depression [32].
Relapse prodrome common to both phases
There are prodromal symptoms to relapse common to both phases, such as sleep disturbances. Several epidemiological studies have provided data suggesting that insomnia is a clear risk factor for depression. A study of patients with major depression without psychotic symptoms found first, that patients suffering from relapses experience higher levels of sleep disturbances several weeks before a relapse and second, that sleep complaints can precede the series of symptoms that make up the syndrome of major depression [33]. Also a recent prospective study using self-reports of mood, sleep and bedrest conducted with 59 bipolar patients using ChronoRecord [34] found a clear temporal relation between sleep and mood, so that a decrease in sleep or bedrest was followed by clinical hypomania or mania the next day, while an increase was followed by depression [34].
Role of family members in the detection of prodromes
Although family members play a crucial role in detecting prodromal symptoms to relapse, few studies have included samples of family members. One study that assessed 74 patients diagnosed with bipolar disorder I and 45 family members using an open questionnaire in which they listed specific prodromes of manic or depressive episodes that were later classified into six categories (behavioural, cognitive, mood, neurovegetative, social or other) found that almost 90% of patients and family members gave at least one manic prodromal symptom, and approximately 80% at least one prodrome of depression. Many were idiosyncratic. Agreement between patient and family members on reported symptoms was strong for the prodromal phase of both polarities [6].
Coping with prodromes
Some studies on psychosocial interventions have included a section dedicated to teaching coping strategies in order to prevent full episodes [14, 15, 35]. One study on this subject interviewed 40 bipolar patients about depressive and manic prodromes and their coping strategies, as well as their levels of insight and social functioning. The results indicated that subjects tended to use both behavioural and cognitive techniques to counter depressive prodromes, and predominantly behavioural strategies against manic prodromes. Insight is definitely correlated with how subjects cope with manic prodromes, and it also affects their social functioning. One possible hypothesis would be that the initial stages of mania manifest themselves more in public contexts, while depression is a more private matter; leading those subjects less capable of coping with manic prodromes to suffer more serious consequences in their social functioning. In this study, the strategies most often used with manic prodromes by the group with good coping abilities were: trying to reduce their activities and restrain themselves; initiating relaxing activities; increasing resting or sleeping time; and visiting their doctor. The group with bad coping abilities tackled manic prodromes by continuing with their tasks or taking on more, enjoying the feeling of being high, going out more and spending money, finding more things to fill their days with, or not doing anything in particular. As for depressive prodromes, the good coping group listed getting organized and staying busy; getting social support and meeting with people; avoiding negative thoughts and distracting themselves; and recognizing realistic thoughts and evaluating whether they are worth worrying about. The bad coping group reported staying in bed and trusting it would all just pass; not doing anything; and taking extra medication such as lithium or hypnotics [4].
The prospective analysis of coping strategies shows that patients using behavioural strategies (e.g. prioritizing and reducing their tasks to a more realistic level) had fewer manic relapses over the course of 18 months. As for depressive prodromes, fewer relapses were suffered by patients using techniques such as staying busy and using distractions to avoid worrying, as opposed to those who used passive techniques or drinking [15].
A specific instrument exists for assessing coping strategies used by bipolar patients during the prodromal phase of their manic episodes. It is a 40-item questionnaire with four subscales (stimulus reduction, problem-directed coping, seeking professional help, and denial or blame) [18].
Psychological interventions
There are two studies of special note that investigated the effectiveness of psychological interventions in prodrome detection. The first study used individual interventions and the second one, a more extensive psychoeducational program.
The study by Perry et al. consisted of 69 patients who had suffered a relapse in the previous 12 months [14]. They were randomly assigned to a control group or to an experimental group that received 7–12 individual psychoeducationally oriented sessions. The researchers then measured the time until the next manic or depressive relapse, the number of relapses, and social functioning. The treatment given to the experimental group proved effective in reducing manic relapses. No effect was observed on the prevention of depressive episodes. The explanation offered was that manic prodromes are more distinct and protracted than depressive prodromes, and that acute mania can be treated more rapidly and effectively than acute depression. Also, improving the detection of depressive symptoms without the appropriate strategies for dealing with them may be useless, because the experimental group showed no improvement in the number of relapses and received significantly higher doses of antidepressants. Social functioning improved, probably because intervention increased patients’ confidence that they would be able to deal with relapses.
The second one was a 2 year study with a treatment group of 60 patients and a control group, also of 60 patients, who received non-structured treatment. The results showed a significantly lower number of manic or hypomanic, mixed and depressive phases, and longer euthymic periods before the first relapse after the psychological intervention. However, that study also covered other important aspects such as following one's habits and doing so regularly; the results could, therefore, not be attributed solely to the detection of prodromes [12]. To solve this problem, another, similar study was conducted with a sample of bipolar patients who adhered closely to the treatment. The results showed a significant improvement in the 25 patients of the experimental group when compared with the control group that received non-structured treatment. Therefore, an increase in these patients’ ability to detect prodromes improves the course of their illness [13].
Discussion
A fundamental objective in the treatment of bipolar patients is the development of therapeutic strategies for relapse prevention. The first studies on the prodromes of affective disorders were conducted in the 1960s and were characterized by methodological problems and very heterogeneous samples, resulting in very disparate and difficult-to-generalize results.
However, the analysis of the progressive studies on this matter shows that there is sufficient evidence of the benefits of patients acquiring both detection skills and coping strategies. Furthermore, many studies point out that bipolar patients, in spite of their characteristic lack of insight, are normally quite capable of recognizing prodromal symptoms [36]. But there are some differences between manic and depressive relapse prodromes that have to be taken into account. It is generally thought that patients have more difficulties pointing out depressive prodromes [4], and these are also more diverse than manic prodromes [4, 37]. The most prevalent manic symptom is sleep disturbances, and the most prevalent depressive symptom is mood changes [22].
The different duration of both types of prodromes has led to various hypotheses. It may be due to different biological processes, or perhaps it is an artefact because the prodromal symptoms of mania are more rapidly identified. This is why it is easier for mental health services to treat mania than depression. It has been pointed out that recognizing early symptoms and initiating treatment reduces significantly manic, but not depressive relapses [14], and that once the warning signs have been identified, effective pharmacological treatment can more effectively be administered in acute mania than in depression [38]. The greatest challenge, therefore, is the early detection of bipolar depression.
Another of the aspects analysed was the implication for treatment of detecting relapse prodromes. The optimal duration of lithium maintenance treatment in bipolar patients is still a matter of controversy among experts. In one pilot study, the authors used the reappearance of prodromes as a signal to restart lithium treatment in patients who had stopped taking this mood stabilizer. The study closely followed a sample of clinically stable patients who were highly conscious of their illness and had very cooperative families [39]. Another option that has been proposed is to eliminate maintenance medication and replace it with prodrome monitoring [2]. This approach has yielded good results in some cases [40], but in other studies five patients were similarly followed during 2 years [39], three of them relapsing and one experiencing significant symptoms. The fifth patient was followed with good results. In any case, such measures must be taken with caution [41].
Studies that evaluate prodromes face a series of common limitations. One of them is overlap with other psychiatric variables, given the possible confusion between premorbid features and prodromal or residual symptoms. For example, certain personality traits may in the long run form characteristic ways of feeling, thinking and acting in the course of a depression. To partly avoid this, subclinical symptoms include only those that appear very clearly, as described in some studies about affective prodromes [42–44].
In addition, it should be borne in mind that an important number of bipolar patients fail to completely recover from an acute episode. The patients in the Judd et al. study, which had a 12.8 year follow up, continued to experience subsyndromic symptoms, especially of the depressive type [45]. Prodromes could play a pathophysiological role in affective disorders, and some residual symptoms could progress and turn into prodromal symptoms of relapse [46]. A model has been described to study prodromal and residual symptoms in psychiatric illnesses. The phenomenon called ‘rollback’ refers to an illness that remits but progressively recapitulates, albeit in the opposite order, many of the states and symptoms that were observed when it was developing. There exists, therefore, a relationship between prodromal and residual symptoms, and certain prodromes can be overshadowed by the acute manifestations of the disorder and continue as residual symptoms until they finally turn into relapse prodromes [47]. Another problem inherent in prodrome assessment is how to identify exactly when a prodrome ceases to be and a full episode starts, especially when there are quantitative but not qualitative differences between the prodromes and the symptoms experienced during an episode.
Furthermore as psychoeducation, relapse prevention may have side-effects. Patients with an obsessive–compulsive personality may become exceedingly concerned about detecting relapse prodromes, increasing the number of visits to their psychiatrist. Others may become too rigid about sleeping habits, missing social events or travels [48]. Teaching early awareness of depressive symptoms has been associated with an increase in the use of antidepressants, without decreasing the number of depressive episodes [14]. Another risk of this procedure is an unnecessary hypervigilance with an increased level of anxiety in patients and families [49].
A very important matter for daily clinical practice is that of the prodromal symptoms characteristic of each individual patient. General symptoms such as sleep disturbance are present in most patients for example, but are not very sensitive. In some patients the onset of affective episodes tends to follow a sequence that repeats itself, something that can be confirmed by family members, and facilitates early therapeutic intervention. The most relevant prodromal warning signs are often very individual. To analyse this matter, in some studies subjects are asked about symptoms not included in the checklist and the majority of patients identified idiosyncratic symptoms as part of their relapse prodrome [3]. These idiosyncratic symptoms are probably the result of a combination of biological and psychological factors and past experiences [23], and support the idea of an individual ‘relapse signature’ for the majority of patients.
Getting patients to learn to regularly monitor early symptoms of relapse or to know their idiosyncratic symptoms in cooperation with their physician are key aspects of daily practice in the treatment of bipolar disorder. Not only can relapses and hospital admissions be reduced but monitoring, detecting and coping with prodromes can have other significant effects, for example on patients’ professional functioning, interpersonal relationships, and family and social life. Prospective studies should be conducted that include the monitoring of prodromes in order to provide more detailed information about the duration and specific symptoms associated with the prodromes of mania, and its duration.