
Abstract
Objective:
To evaluate the impact of the National Perinatal Depression Initiative on access to Medicare services for women at risk of perinatal mental illness.
Method:
Retrospective cohort study using difference-in-difference analytical methods to quantify the impact of the National Perinatal Depression Initiative policies on Medicare Benefits Schedule mental health usage by Australian women giving birth between 2006 and 2010. A random sample of women of reproductive age enrolled in Medicare who had not given birth where used as controls. The main outcome measures were the proportions of women giving birth each month who accessed a Medicare Benefits Schedule mental health items during the perinatal period (pregnancy through to the end of the first postnatal year) before and after the introduction of the National Perinatal Depression Initiative.
Results:
The proportion of women giving birth who accessed at least one mental health item during the perinatal period increased from 88 to 141 per 1000 between 2007 and 2010. The difference-in-difference analysis showed that while there was an overall increase in Medicare Benefits Schedule mental health item access as a result of the National Perinatal Depression Initiative, this did not reach statistical significance. However, the National Perinatal Depression Initiative was found to significantly increase access in subpopulations of women, particularly those aged under 25 and over 34 years living in major cities.
Conclusion:
In the 2 years following its introduction, the National Perinatal Depression Initiative was found to have increased access to Medicare funded mental health services in particular groups of women. However, an overall increase across all groups did not reach statistical significance. Further studies are needed to assess the impact of the National Perinatal Depression Initiative on women during childbearing years, including access to tertiary care, the cost-effectiveness of the initiative, and mental health outcomes. It is recommended that new mental health policy initiatives incorporate a planned strategic approach to evaluation, which includes sufficient follow-up to assess the impact of public health strategies.
Introduction
Mental health problems in the perinatal period (pregnancy to first postnatal year) are a major public health issue with significant morbidity and costs for mother, infant and society (Bauer et al., 2014; Burke, 2003; Kingston et al., 2012; Murray and Cooper, 1996). Postnatal depression and anxiety disorders affect around 15% of women, with up to 45% of cases beginning in pregnancy (Austin et al., 2010; Gavin et al., 2005). Recent estimates indicate that postnatal depression costs the Australian economy AUD433 million a year, along with a loss of 20,732 disability adjusted life years (Deloitte, 2012). Furthermore, the economic cost in one year of not treating perinatal mental health conditions was estimated to be in excess of AUD560 million for births in 2013 (PwC and COPE, 2014). While there are acceptable and effective treatments for perinatal depression (Dennis, 2004; Dennis and Stewart, 2004), perinatal screening guidelines differ worldwide, and more evidence-based research on the utility of perinatal depression screening is needed (Chaudron and Wisner, 2014; Thombs et al., 2014).
In 2008, the beyondblue National Action Plan for Perinatal Health recommended universal psychosocial assessment of women during the perinatal period (beyondblue, 2008). This was followed by the Australian Commonwealth Government Department of Health’s National Perinatal Depression Initiative (NPDI) (2008–2013). The NPDI included the development of clinical practice guidelines recommending routine antenatal and postnatal screening for depression using the Edinburgh Postnatal Depression Scale plus some form of psychosocial assessment (Austin et al., 2011a), new perinatal mental health services under the Access to Allied Psychological Services (ATAPS) initiative, training of primary health care professionals and community awareness and education (Australian Government Department of Health, 2009). Overall, AUD85 million was invested in the NPDI, made up of AUD30 million contributions from both Commonwealth and state and territory governments, AUD20 million from the Commonwealth to ATAPS specifically for perinatal mental health items and AUD5 million to beyondblue. ATAPS items are part of the Better Outcomes in Mental Health Care programme introduced in 2001 (Australian Government Department of Health, 2010), which allow general practitioners (GPs) to refer patients to allied health professionals, including psychologists, for subsidised mental health treatment funded through local primary care organisations (Medicare Locals) via state and territory governments.
Australia’s universal health insurance scheme, Medicare, provides access to primary care services, public hospitals and subsidised pharmaceuticals to all Australians through a levy on tax payers. Medicare pays benefits or rebates for professional health services listed on the Medicare Benefits Schedule (MBS) including mental health services provided by psychiatrists and, in more recent years, by GPs and allied health professionals.
Alongside the introduction of the NPDI, there have been numerous other mental health policy initiatives introduced over the last decade. The Council of Australian Governments (COAG) committed AUD4.1 billion to mental health over 2006–2011 as part of the National Action Plan for Mental Health (COAG, 2013), funding 145 separate initiatives including ‘Better Access to Mental Health Care’ (frequently referred to as the ‘Better Access’ initiative) in November 2006. This scheme introduced a number of MBS items for selected mental health services, including items for psychological treatment with registered psychologists and other mental health professionals (Australian Government Department of Health, 2014).
The 2006 Better Access initiative has led to a significant increase in access to, and utilisation of, Medicare funded mental health care. The number of patients accessing the newly introduced MBS items increased from 34 to 53 per 1000 between 2007 and 2009, with the number of services claimed through Medicare increasing from 2.7 million to 4.6 million over the same period. Individuals from ‘at-risk’ populations, such as the young, those from lower socioeconomic backgrounds and those in remote areas, have experienced lower rates of uptake, but have also experienced the greatest percentage increases in uptake over time (Pirkis et al., 2010, 2011).
While the impact of the Better Access initiatives is relatively clear in terms of access to Medicare funded services at a population level, there has been no evaluation of how access to Medicare funded services for women giving birth has been affected by the introduction of NPDI (Austin et al., 2012), nor evaluation of the NPDI more broadly.An important point of contact with the health care system for women with perinatal mental illness or morbidity is through Medicare funded services, provided by a GP, psychologist or psychiatrist. Therefore, an evaluation of Medicare service utilisation is critical to understanding whether the NPDI has been effective in providing access to mental health care for women at this vulnerable time in their lives. This study aims to address this question by quantifying the uptake of MBS mental health items for women during the perinatal period before and after the introduction of the NPDI compared to a control group of women of similar age; the hypothesis being that the NPDI resulted in increased access to primary and secondary mental health care during the perinatal period.
Methods
Data sources
The Australian Government’s Department of Human Services, Medicare Information Service Branch provided an extract of monthly aggregate claims data for mental health MBS services undertaken during the perinatal period for women giving birth (perinatal women) between August 2006 and December 2010 (the birth observation period). To capture the perinatal period for all women in the cohort, the extract included claims for services between 1 November 2005 and 31 December 2011 (the study period).
The mental health MBS items included were as follows: psychiatric services – 291, 293, 296, 297, 299, 300, 302, 304, 306, 308, 310, 312, 314, 316, 318, 319, 320, 322, 324, 326, 328, 330, 332, 334, 3.36, 338, 342, 344, 346, 348, 350, 352, 353, 355, 356, 357, 358, 359, 361, 364, 366, 367, 369, 370, 855, 857, 858, 861, 864, 866, 14,224; GP services – 2702, 2710, 2712, 2713, 2721, 2723, 2725, 2727, 170, 171, 172, 2574, 2575, 2577, 2578, 2704, 2705, 2707, 2708, 4001; allied health (including psychologists) services – 109,68; 80,100; 80,105; 80,110; 80,115; 80,120; 80,000; 80,005; 80,010; 80,015; 80,020; 81,355; 10,956; 80,125; 80,130; 80,135; 80,140; 80,145; 80,150; 80,155; 80,160; 80,165; 80,170; 81,325; 81,000; 81,005; 81,010. This list is slightly different from the MBS-subsidised list of items specified by the Australian Institute of Health and Welfare (AIHW) (https://mhsa.aihw.gov.au/services/medicare/data-source/), because the AIHW list excluded important pregnancy counselling items, and included items not considered relevant for this population (e.g. electroconvulsive therapy).
To identify women who had given birth and thus been exposed to the NPDI (perinatal women), the oldest woman of reproductive age (18–44 years) on a Medicare Card for which a baby had been added was identified as the mother of the child. The MBS mental health items claimed by that woman in the 9 months leading up to the birth and the 12 months following the birth (the perinatal period) were extracted and stratified by temporal period to birth (9 months leading to the birth, 1–6 months following the birth, 7–12 months following the birth), and provider type (GPs, allied health professionals and psychiatrists). Women were grouped by month of birth (August 2006 to December 2010), age at time of birth (<25, 25–34 and ⩾35 years) and level of remoteness as defined by Australian Bureau of Statistics Accessibility/Remoteness Index of Australia (ARIA) categories (major city, regional, remote) (ABS, 2006). A woman was only selected once in the study period, and the baby could have been the woman’s first or subsequent child. Confinement data were used to provide national estimates of the number of women giving birth during the birth observation period (ABS, 2010).
To identify a group of women who had not been exposedto the NPDI but who had been exposed to other mental health initiatives (controls), the same data extraction was performed for a random sample of 60,000 women of reproductive age per month (approximately 3 controls to each woman giving birth) enrolled with Medicare who did not give birth between November 2004 and December 2011. The MBS mental health items claimed by these women in the 9 months before and 12 months after the middle of each month were extracted. This control group was particularly important because of the introduction of Better Access MBS items and numerous other mental health initiatives during the study period.
Statistical analysis
Descriptive statistics included the annual proportion of women accessing MBS mental health items, and the average number of services claimed per woman by age,remoteness, temporal period and provider type. A difference-in-difference econometric method was used to examine the effect of the NPDI on access to MBS mental health items by perinatal women. This approach allowed us to control for (1) time invariant differences between the perinatal group (women of reproductive age who gave birth in a birth observation period) and the control group (women of reproductive age who did not give birth in an observation period) (first difference), and (2) time-varying factors due to environmental impacts, such as the introducton Better Access items and the de-stigmatising of mental illness during the study period (second difference). The model structure is set out as follows

Yi,t is the number of women accessing at least one MBS mental health item per 1000 women of group i at time t. Ti is a binary variable to indicate the perinatal group or control group. Pt is a dummy variable indicating pre- and post-policy periods. Ti * Pt is an interaction term indicating the effect of the NPDI on the perinatal group while taking into account other background policies and environmental factors common to both groups. Given a lack of publicly available data relating to rates of uptake of the NPDI at national or state levels (Austin et al., 2012), we proposed that the NPDI started to take effect from January 2009. This cut-off date was based on expert advice from the study investigators and an 2012 survey (unpublished) undertaken of state and territory representatives under the NPDI (Highet and Purtell, 2012) .
The estimates of the policy impact are presented in two forms: a linear model to quantify the NPDI impact on the number of women accessing at least one MBS mental health item during the perinatal period per 1000 perinatal women (absolute change), and a natural log transformation of the dependent variable to quantify the proportion of perinatal women accessing at least one MBS mental health item during the perinatal period (relative change).
The standard difference-in-difference model described above relies on the parallel paths assumption such that no time-varying differences exist between the cases and control groups. That is, without the introduction of the NPDI, utilisation of MBS items would increase at approximately the same rate for both cases and controls. Given that our birth observation period is relatively short (August 2006 to December 2010), we would not anticipate time-varying behaviours among cases and controls in terms of access to MBS mental health items. The main exception to this would be exposure to the NPDI by the case group.
Results
Descriptive statistics
Access to mental health MBS items
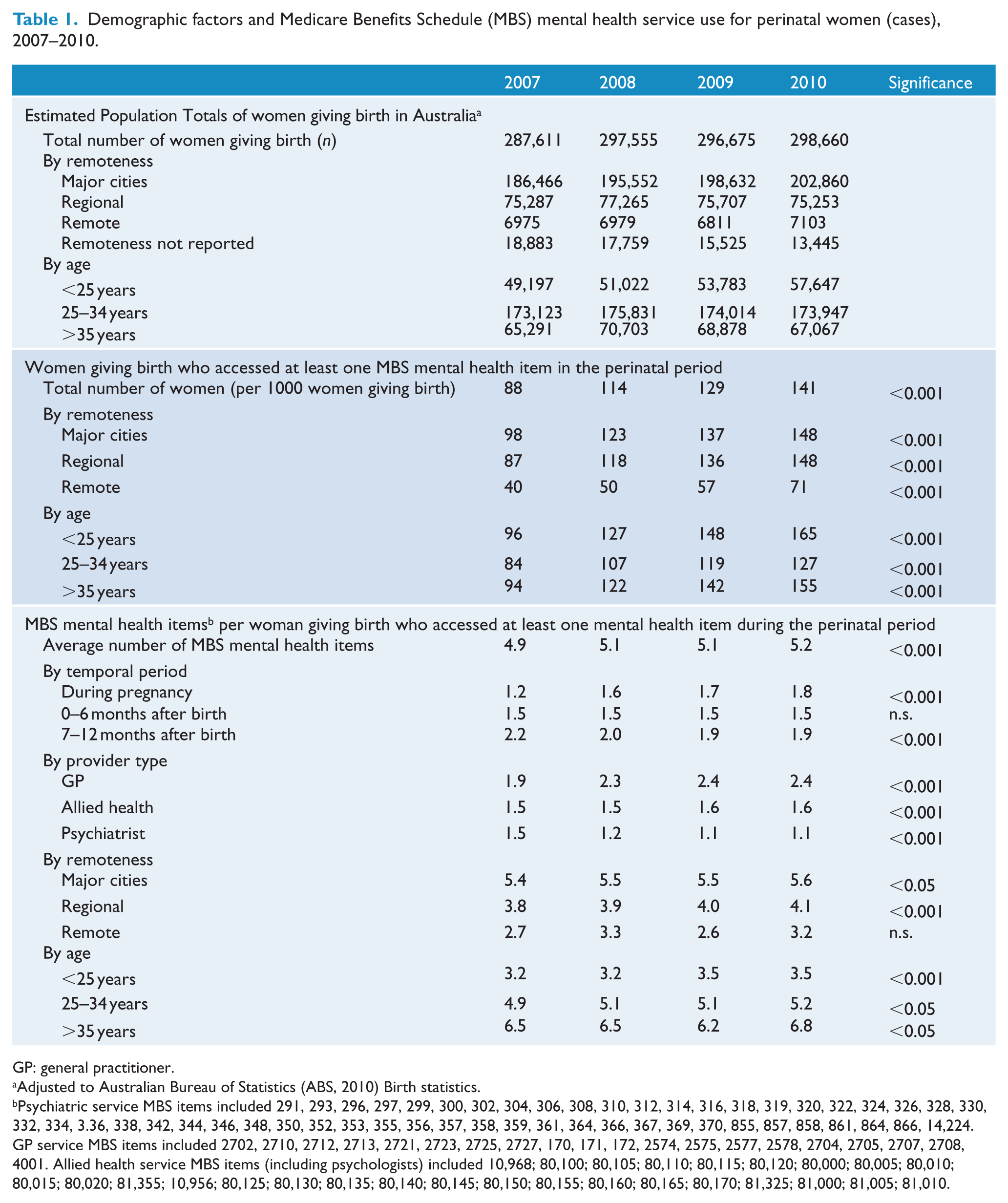
Table 1 presents the annual descriptive statistics for women who gave birth during the study period and claimed MBS mental health items during the perinatal period. During the birth observation period two thirds of births were to women residing in major cities, 27% in regional areas and 2% in a remote area. Approximately 18% of women giving birth were aged less than 25 years, 59% were aged 25–34 years and 23% were aged 35 years or older.
Demographic factors and Medicare Benefits Schedule (MBS) mental health service use for perinatal women (cases), 2007–2010.
GP: general practitioner.
Adjusted to Australian Bureau of Statistics (ABS, 2010) Birth statistics.
Psychiatric service MBS items included 291, 293, 296, 297, 299, 300, 302, 304, 306, 308, 310, 312, 314, 316, 318, 319, 320, 322, 324, 326, 328, 330, 332, 334, 3.36, 338, 342, 344, 346, 348, 350, 352, 353, 355, 356, 357, 358, 359, 361, 364, 366, 367, 369, 370, 855, 857, 858, 861, 864, 866, 14,224. GP service MBS items included 2702, 2710, 2712, 2713, 2721, 2723, 2725, 2727, 170, 171, 172, 2574, 2575, 2577, 2578, 2704, 2705, 2707, 2708, 4001. Allied health service MBS items (including psychologists) included 10,968; 80,100; 80,105; 80,110; 80,115; 80,120; 80,000; 80,005; 80,010; 80,015; 80,020; 81,355; 10,956; 80,125; 80,130; 80,135; 80,140; 80,145; 80,150; 80,155; 80,160; 80,165; 80,170; 81,325; 81,000; 81,005; 81,010.
The proportion of women giving birth who accessed at least one MBS mental health item during the perinatal period increased from 88 to 141 per 1000 women giving birth between 2007 and 2010. While all age groups exhibited increased access, those aged less than 25 years and over 35 years showed the most pronounced increase in access (Table 1 and Figure 1). While access rates for those in regional areas matched those in major cities by 2010 (148 per 1000), the percentage of perinatal mothers in remote areas who accessed a mental health MBS item continued to lag behind at 71 per 1000 (Table 1).
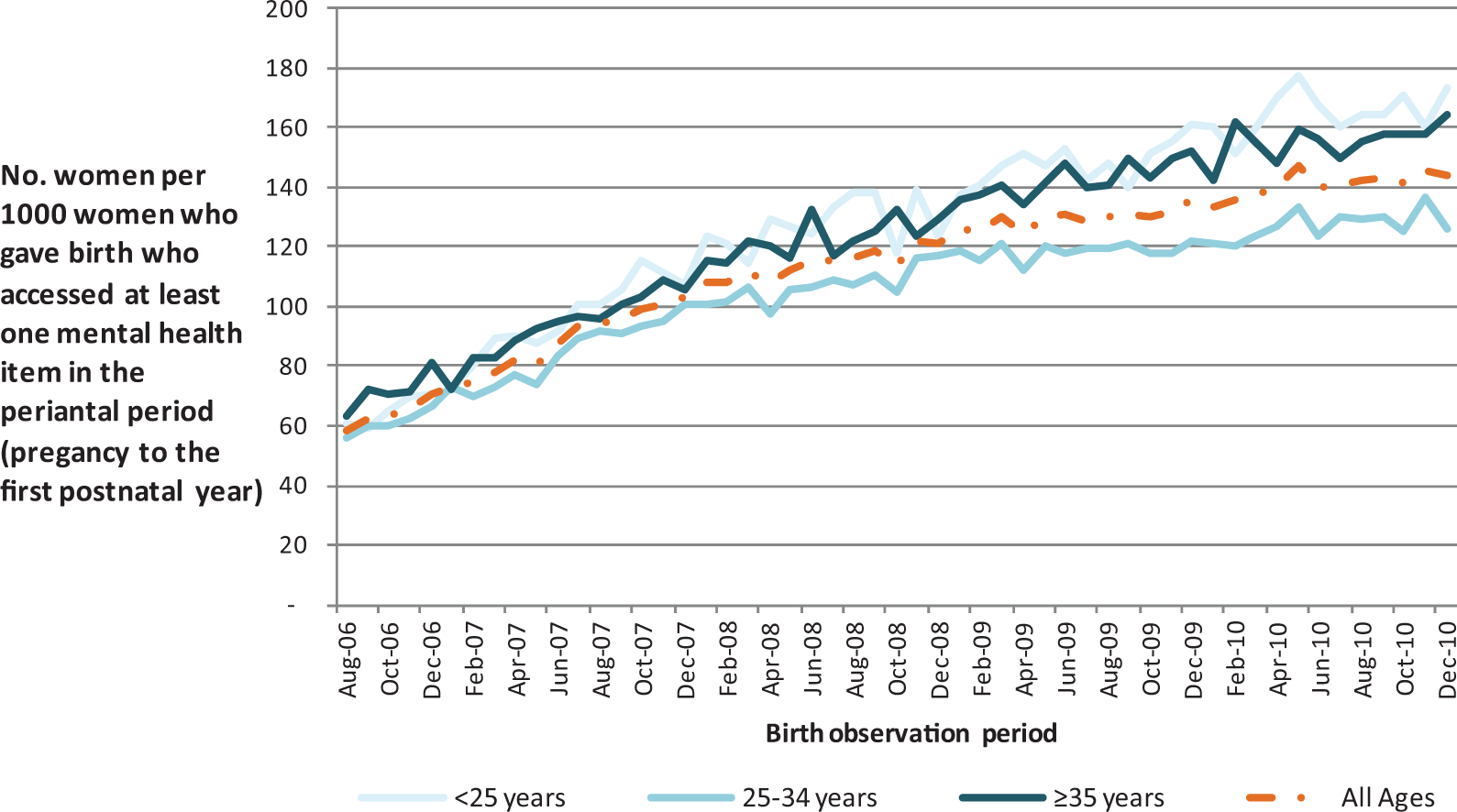
Rate of access of Medicare Benefits Schedule (MBS) mental health items by women who have given birth by month of birth and age.
Women who accessed at least one mental health item during the perinatal period also exhibited increasing number of items claimed over the study period with an average of 4.9 MBS mental health items claimed per woman in 2007, rising to 5.2 MBS items claimed per woman in 2010.
Temporal changes in access by type of provider
In addition to increased access to MBS funded services, there were also changes in the timing of access within the perinatal period for different types of providers (Figure 2). Of women giving birth between August 2006 and December 2010 who had accessed at least one MBS mental health item, the percentage who had accessed a GP or allied health service during pregnancy increased from 3% to 36% for GP services and from 1% to 20% for allied health services, while the percentage accessing a psychiatrist during pregnancy fell from 17% to 8% (Figure 2). The average number of services accessed during pregnancy increased from 1.2 services per woman in 2007 to 1.8 services per woman in 2010 (Table 1).
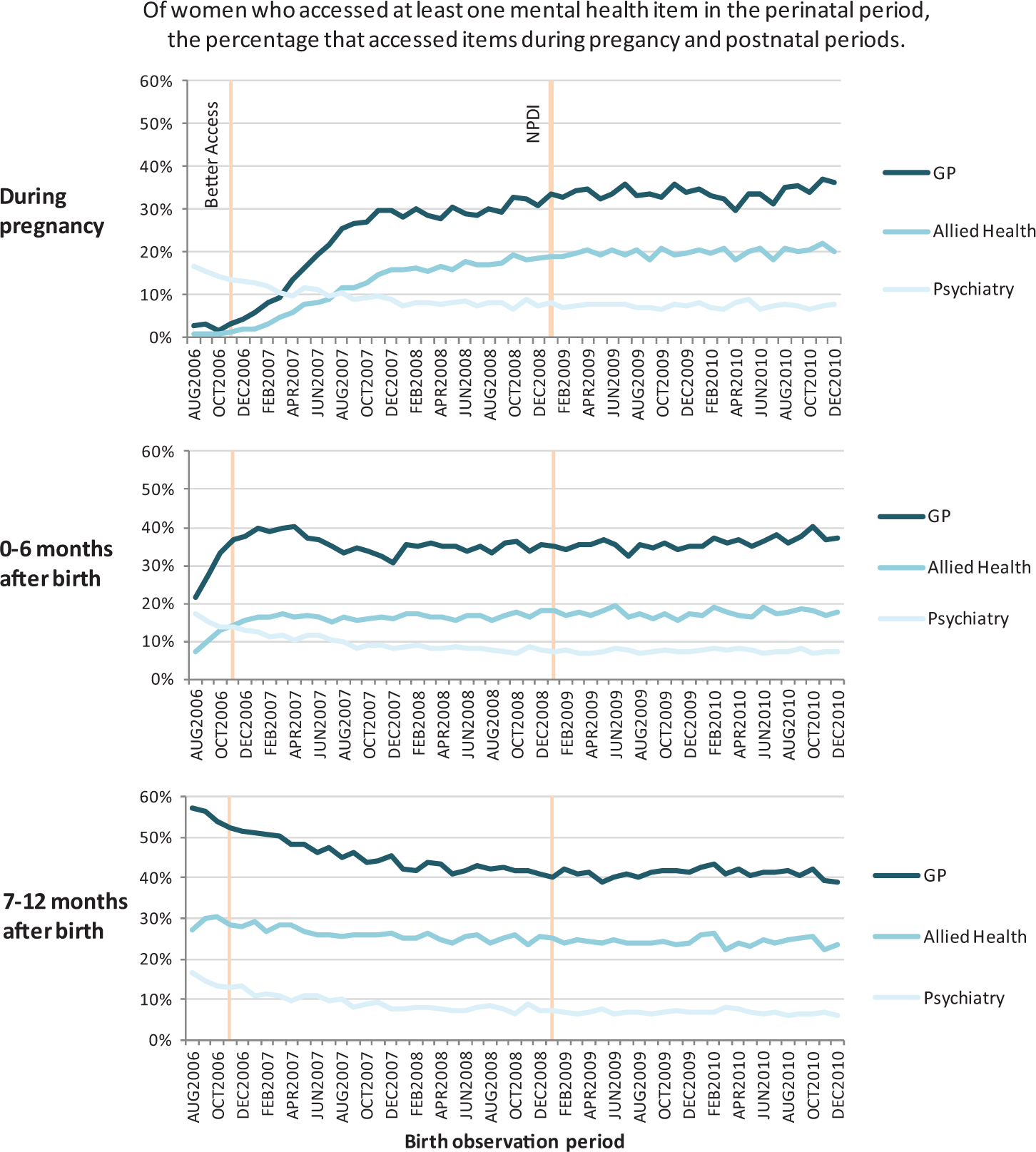
Medicare Benefits Schedule (MBS) mental health item temporal analysis by month of birth and provider type.
Conversely, the percentage of perinatal women who accessed at least one MBS mental health item during their perinatal period and who claimed a GP mental health item in the 7–12 months following birth fell from 57% to 39% (Figure 2). The proportion of services undertaken during the 7–12 months following the birth also decreased from 2.2 services per woman in 2007 to 1.9 services per woman in 2010 (Table 1). Most of the temporal changes in access coincided with the introduction of the Better Access items in November 2006 and may be due, in part at least, to generic MBS items being replaced by Better Access mental health items (Charles et al., 2006).
Econometric results to examine the NPDI policy impact on access to Medicare treatment
The econometric estimates of the effect of the NPDI on MBS mental health access are summarised in Table 2. Overall, while there was an increase in MBS mental health access for perinatal women in Australia after the introduction of the NPDI compared to the control women, this did not reach statistical significance (Figure 3(A)). However, significant differences were observed in some sub-groups of perinatal women. Namely, those aged less than 25 years and those over 34 years both showed significant increases in access after the introduction of the NPDI compared to control women (Figure 3(B) and (D)). For perinatal women under 25 years, the NPDI resulted in an average increase of 19 women per 1000 women giving birth per month accessing MBS mental health items after the policy compared to before (after controlling for background effects). This equates to a 10% average increase in the number of mothers accessing mental health items after the policy compared to before. For perinatal women aged over 34 years, the NPDI resulted in an average increase of 13 women per 1000 (7%) per month accessing MBS mental health items after the policy compared to before. There wasn’t a significant impact of the NPDI on perinatal women aged between 25 and 34 years who represented the largest age group of women giving birth during the study period (Figure 3(C)).
Summary of difference-in-difference regressions to estimate the impact of National Perinatal Depression Initiative (NPDI) policy on number of perinatal women accessing Medicare Benefits Schedule (MBS) mental health items per 1000 women who gave birth.
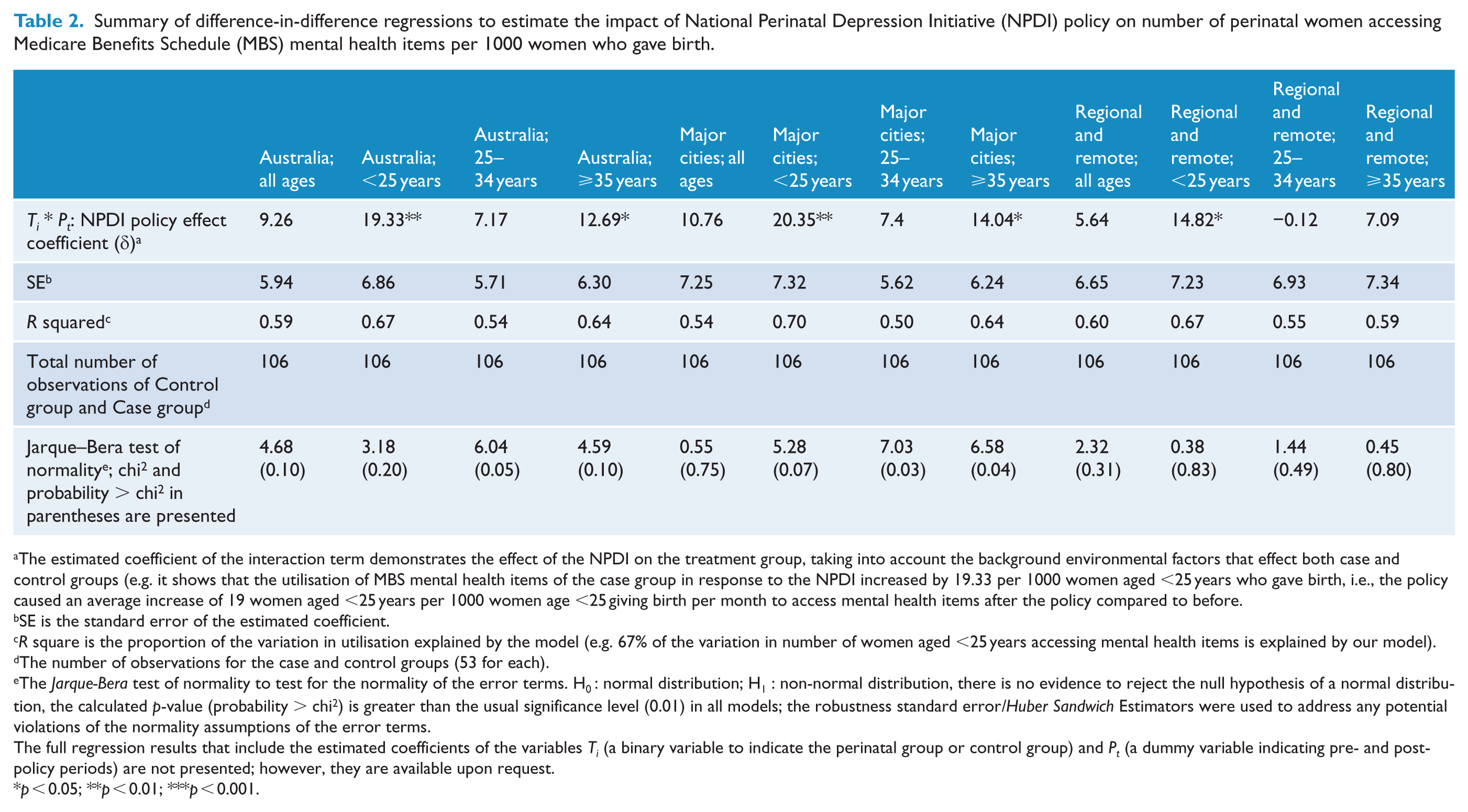
The estimated coefficient of the interaction term demonstrates the effect of the NPDI on the treatment group, taking into account the background environmental factors that effect both case and control groups (e.g. it shows that the utilisation of MBS mental health items of the case group in response to the NPDI increased by 19.33 per 1000 women aged <25 years who gave birth, i.e., the policy caused an average increase of 19 women aged <25 years per 1000 women age <25 giving birth per month to access mental health items after the policy compared to before.
SE is the standard error of the estimated coefficient.
R square is the proportion of the variation in utilisation explained by the model (e.g. 67% of the variation in number of women aged <25 years accessing mental health items is explained by our model).
The number of observations for the case and control groups (53 for each).
The Jarque-Bera test of normality to test for the normality of the error terms. H0 : normal distribution; H1 : non-normal distribution, there is no evidence to reject the null hypothesis of a normal distribution, the calculated p-value (probability > chi2) is greater than the usual significance level (0.01) in all models; the robustness standard error/Huber Sandwich Estimators were used to address any potential violations of the normality assumptions of the error terms.
The full regression results that include the estimated coefficients of the variables Ti (a binary variable to indicate the perinatal group or control group) and Pt (a dummy variable indicating pre- and post- policy periods) are not presented; however, they are available upon request.
p < 0.05; **p < 0.01; ***p < 0.001.
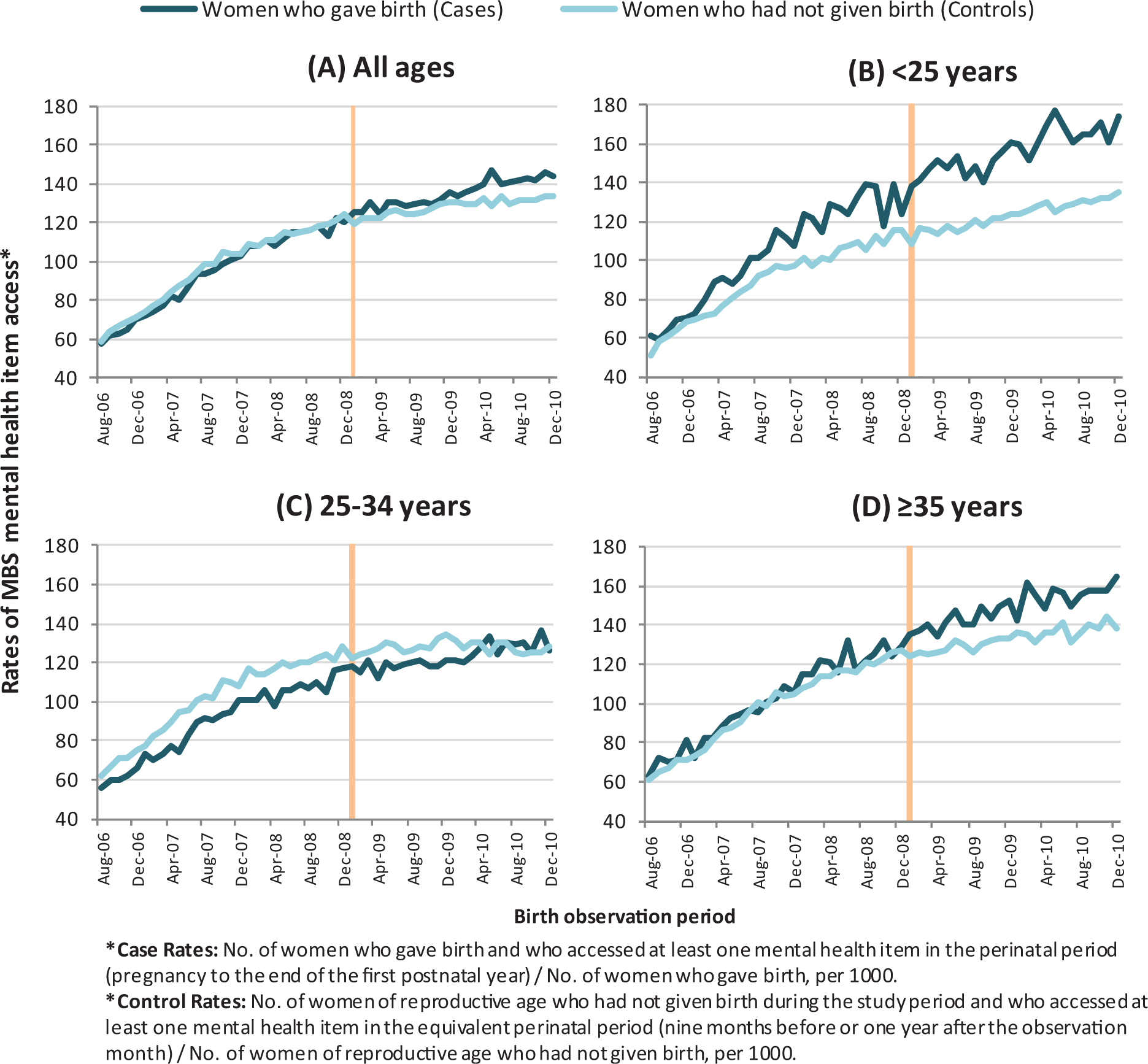
Rates of access to Medicare Benefit Schedule (MBS) mental health items by Case and Control women by age group.
There were also some regional differences in access. In major cities, perinatal women under 25 years and over 34 years showed increased uptake of mental health services after the introduction of the NPDI (an additional 20 [7%] and 14 [7%] women per 1000 women giving birth per month, respectively). However, in regional and remote areas, only women under 25 years showed increased uptake (an additional 15 women per 1000 per month (6%)) (Table 2).
A number of robustness techniques were used to ascertain the precision of the estimated results. First, the Jarque–Bera test of normality was conducted to test whether the normality assumptions of the error terms were met. The test results showed that there was no serious departure from normality assumptions of the error terms. Second, the robustness standard error/Huber Sandwich Estimator was used to address any potential violations of the normality assumptions of the error terms.
Discussion
This is the first study to evaluate the impact of the NPDI in terms of access to mental health treatment. It demonstrates that during the 2 years after its introduction, the NPDI appears to have been effective in increasing mental health access by both younger and older mothers, particularly those in major cities, but has not been as effective in women who gave birth aged between 25 and 34 years. Our findings are consistent with the fact that the NPDI was likely to have had greater impact initially in the metropolitan areas, as screening and training were often centralised in urban areas and in the major maternity settings. Furthermore, clinical practice guidelines recommend that screening should only be performed if adequate access to referral services exists. Although we are unable to comment definitely on the socioeconomic status of women included in this study, previous research has shown that young parents are more likely to be living in disadvantaged circumstances and experiencing financial difficulties (Schmied et al., 2013). Therefore, access to subsidised Medicare treatment may be more pronounced in younger mothers in response to the NPDI and other mental health initiative. The reason for increased uptake in older mothers is less clear but is in keeping with previous findings that rates of service use for mental health issues is highest for women aged 35–44 years (Burgess et al., 2009).
This study also provides some evidence that there has been a shift to accessing mental health care earlier in the perinatal period, particularly during pregnancy compared to later in the postnatal period. This shift occurred around the time of the introduction of the Better Access items in 2006 and not necessarily in relation to the NPDI. However, some states introduced perinatal mental health initiatives around this time, including the New South Wales (NSW) Integrated Perinatal and Infant Care Strategic Framework (NSW Department of Health, 2009), which may have also contributed to the increase in access to Medicare funded services. A shift to earlier access is an important finding since there is a growing body of literature that suggests that antenatal depression is at least as common as postnatal depression (Lancaster et al., 2010). Access earlier in the perinatal period is likely to be due to a number of factors, including increasing recognition in the literature that women suffer with depressive and anxiety disorders as commonly in pregnancy as in the postnatal period (Gaynes et al., 2005), which is reflected in the Australian policy (Austin et al., 2011b) and clinical practice guidelines (Austin et al., 2011a). This conceptual shift has been accompanied by a change in terminology over the last 10 years from ‘postnatal’ to ‘perinatal’ (designating pregnancy and the postnatal period) when referring to mental health issues in women at this time in their childbearing years (Austin, 2004). Taken together, these factors have shifted depression screening and psychosocial assessment practices and may have contributed to women accessing psychological services earlier in the perinatal period.
One of the challenges of this policy analysis has been that a number of other mental health initiatives and policies were introduced over the study period, making it difficult to isolate the impact of the NPDI per se. To overcome this challenge, we utilised a control group of women who were not exposed to the NPDI – that is, women of reproductive age who had not given birth during the study period. This allowed us to account for comparisons before and after NPDI policy, and comparisons between perinatal and control women. We also used a novel method of identifying women in the Medicare claims database who had recently given birth by linking the enrolment of a baby on a Medicare card to its mother and then tracking the mother’s MBS services usage.
Our method has limitations. Parity could not be controlled for because Medicare data do not include this information, and Medicare’s advice to select a woman only once in the dataset to remove the likelihood of double counting could have increased the representation of first time mothers in the later observation periods in our study. However, previous investigations have shown no effect of parity on perinatal depression (National Health and Medical Research Council [NHMRC], 2000). In addition, 7% of children recorded on a Medicare card could not be assigned to a mother (e.g. no women of reproductive age on the Medicare Card, mother not registered with Medicare for 12 months post delivery). Also, while not a limitation of the method, it should be noted that ATAPS sessions are not paid for by Medicare. However, referral to an allied health professional under ATAPS requires a GP to complete a mental health plan using an appropriate MBS mental health item. Therefore, the impact of the NPDI on uptake of these items to treat perinatal mental health conditions is only partially measured by this study. A recent analysis of ATAPS items shows that between April 2008 and December 2010, 6591 ATAPS sessions of care were delivered to women for perinatal depression (Ftanou et al., 2011). The use of non-mental health specific MBS items by GPs to manage mental health issues is likely to result an underestimate of access by women in the perinatal period. This was demonstrated by a survey of GP encounters for postnatal depression in 2005 (Charles et al., 2006). Quantifying the relative impact of this practice by GPs before and after the NPDI was not possible in this study. However, the temporal analysis does point to a decisive shift from non-mental health MBS items to mental health MBS items around the time of Better Access in 2006, indicating that such a shift would not introduce a bias for this NPDI analysis. A final limitation is that jurisdictions implemented the NPDI variably around 2009 so a definitive cut-off for the policy analysis was not possible.
A prospective evaluation of the NPDI was not built into the policy implementation, nor were data collection processes included to capture the degree of screening uptake. Therefore, the type of retrospective analysis employed in this study is the only option for evaluating Medicare service uptake as a result of the NPDI. Evaluation is a key component of policy development and implementation. It is therefore strongly recommended that new mental health policy initiatives incorporate a planned strategic approach to evaluation, allowing for better identification of counterfactuals and more complex modelling that would allow the difference-in-difference model assumptions to be relaxed. A planned approach to evaluation should also include sufficient follow-up to assess the impact of public health strategies on health services, and on the short and longer term mental health outcomes for mothers and their families.
This study only evaluated the NPDI impact on access to Medicare funded services. While a particularly important sector for this group of women and their families, future studies should examine how integrated screening and enhanced care in the perinatal period – as recommended in the clinical practice guidelines developed and implemented under the NPDI – impact access to tertiary care for women with more severe conditions. Furthermore, given the controversy surrounding the cost-effectiveness of routine depression screening in the perinatal period (Chaudron and Wisner, 2014; Paulden et al., 2009; Thombs et al., 2014), future studies should also report economic costs of mothers, families and the Australian taxpaying community.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The current study was funded by a National Health and Medical Research Council (NHMRC) partnership grant APP1028554: ‘The Australian Perinatal Mental Health Reforms: Using Population Data to Evaluate their Impact on Service Utilisation and Related Cost-Effectiveness’. Beyondblue is a funding partner on this grant. Dr Georgina Chambers, Professor Elizabeth Sullivan, Dr Nicole Highet, Associate Professor Maxine Croft, Associate Professor Cathrine Mihalopoulos, Professor Vera Morgan and Professor Marie-Paule Austin are Chief Investigators on the above Grant. Associate Professor Cathrine Mihalopoulos is funded by a NHMRC Early Career Research Grant 1035887. Dr Nicole Highet was the former Deputy CEO and National Perinatal Advisor of beyondblue between 2001 and 2013.