
Abstract
Keywords
Depression during the postnatal period has been reported to affect 10–20% of women [1]. A meta-analysis of 59 studies involving nearly 13 000 subjects [1] and reporting depression prevalence based on Edinburgh Postnatal Depression Scale (EPDS) [2] scores >12 or on diagnostic caseness, concluded that the mean prevalence of postnatal depression (PND) was 13%. Similar figures have been reported from Australian studies using EPDS > 12 [3], [4]. Australian studies have largely been restricted to English-speaking women in public hospitals in major cities or centres [5–8], with only a few including or reporting prevalence in regional centres [9–12] or in non-English-speaking women [7]. Gavin et al. in a more rigorous meta-analysis examining 30 studies reported a major depression point prevalence of 7.1% [13]. This is a much lower rate than that cited by O'Hara and Swain [1]. Estimates vary according to methodology, including characteristics of the sample (e.g. only primaparous, minority groups) and definition and measurement of depression (e.g. whether a screening tool or diagnostic interview used; what cut-off score is used on the screening tool; whether point or period prevalence is reported; and whether one is reporting major depression alone vs combined major and minor depression).
Two important and related factors that may influence prevalence are socioeconomic status (SES) and cultural background. These have been shown in numerous studies to have an impact on health, including mental health. While there have been a number of meta-analyses, including large follow-up studies (24 000 women) used to ascertain risk factors for PND [1], [13], [14], there remains a knowledge gap, with respect to SES and women from a variety of different cultures and cultural issues. These are of particular relevance to a number of major maternity services across Australia that cater for women with low SES and may explain some of the variation in depression prevalence across studies.
The beyondblue National Postnatal Depression Program introduced routine perinatal (antenatal and postnatal) depression screening protocols into 43 health services across Australia; in some instances this was through the introduction of new screening programmes, in others through partnerships with established programmes. This was in part an attempt to gain an understanding of the prevalence of PND in Australia, using a range of public and private services, metropolitan, rural and regional locations and incorporating culturally and linguistically diverse women (CALD), all of which are not commonly included in studies in this area of research. In addition, we evaluated routine screening and inform provision as the first step in improving health outcomes for women [15–17]. While current strategies for prevention do not appear to be effective [18], evidence suggests that detection and intervention can significantly improve outcomes for these women [19], [20] and it makes logical sense to do so as early as possible. In the beyondblue study, screening was combined with provision of emotional health information to women and families, as well as training for health professionals in psychosocial assessment (including use of the EPDS), specific treatment options and development of pathways to care. This article reports on the sample of women recruited into the beyondblue Program who were followed up at 6–8 weeks after childbirth.
Methods
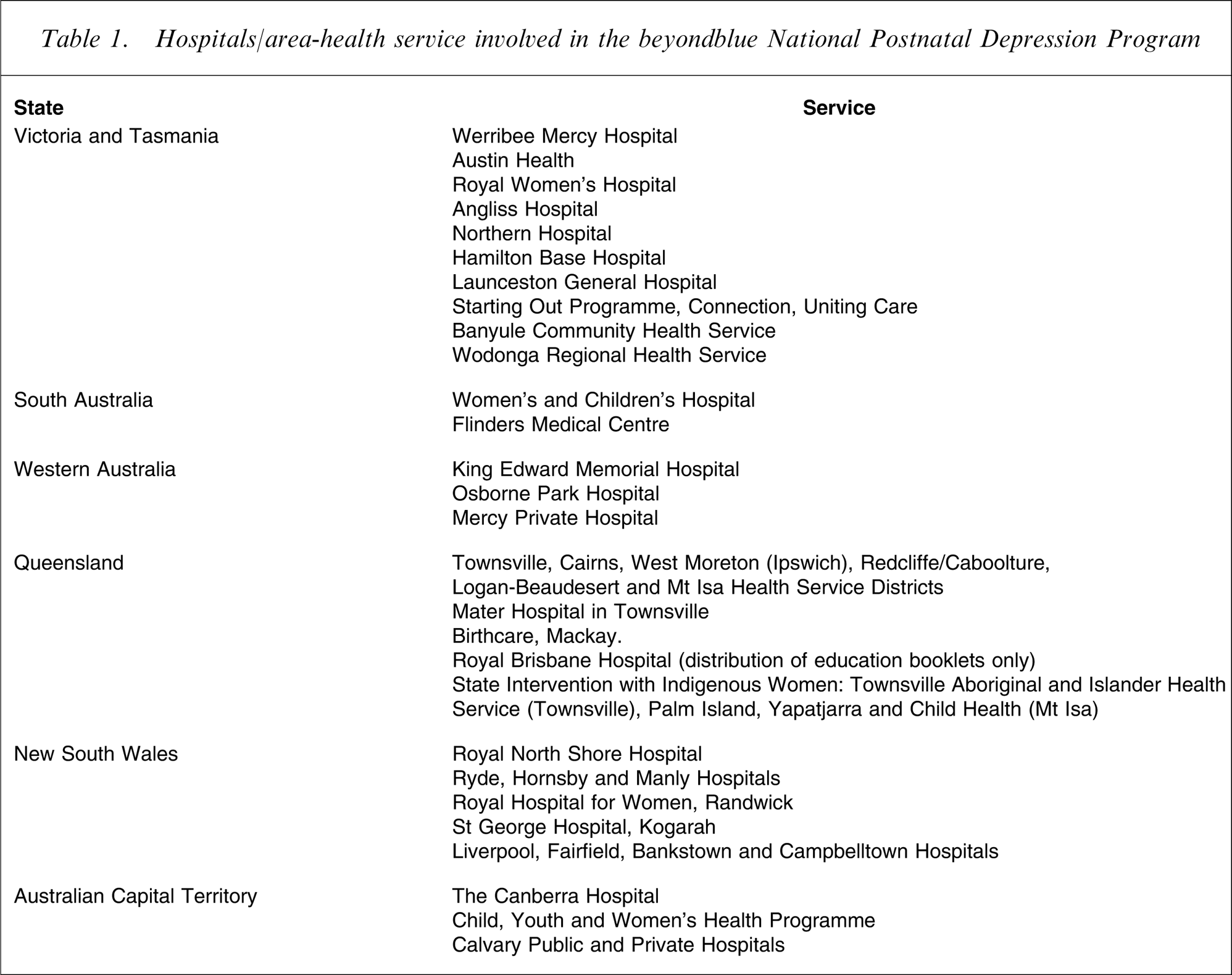
At the commencement of the project in 2002, health services from every State and Territory (excluding the Northern Territory) were invited to join the beyondblue program. Forty-three health services accepted. These were predominantly from city and/or suburban areas but included a representation of rural, remote and private-sector services. Included were major teaching hospitals in Adelaide, Perth, Launceston, Townsville, Canberra and Sydney; suburban teaching hospitals in Melbourne and Sydney; private hospitals in Sydney, Perth, Canberra, Townsville and Mackay; and rural and remote health services in Queensland and Victoria (Table 1). Eight services declined the invitation to participate, citing the following reasons: philosophical objection to perinatal depression screening; presence of other research projects within the service; or lack of staff time, training and knowledge.
Hospitals/area-health service involved in the beyondblue National Postnatal Depression Program
Ethics approval was obtained from all services prior to commencement and included permission for: baseline evaluation of postnatal women and health professionals’ knowledge and attitudes regarding perinatal depression; introduction of perinatal depression screening protocols; routine provision of information on perinatal emotional health; health professional training; specific intervention programmes; and an end evaluation.
In those regions that elected to participate, a baseline evaluation of women and health professionals assessing knowledge of perinatal depression, prevalence of depression and service and support use was conducted [21] and was repeated at completion in 2005 [22].
At all sites robust referral pathways for women with elevated EPDS screening scores were established, refreshed or piloted.
Population and sample
As described previously the present study was part of a larger public health initiative introducing screening as routine [15], [16]. Women recruited to the programme from the aforementioned health services were given questionnaires at two time points: the antenatal booking-in visit and 6–8 weeks postnatally.
Antenatal screening protocol
Women were first approached at their antenatal booking-in visit, where the purpose of the study was explained to them verbally and they were supplied with a plain language statement and a consent form. Women who agreed to participate completed the consent form, after which they were given a 34-item, self-report psychosocial risk factor questionnaire (PSRFQ). As well as collecting each participant's name, contact details and general practitioner details, the PSRFQ also included questions on the following variables: country of birth, language spoken at home, SES, occupation, highest level of education completed, past history of mental illness, current mental illnesses, major life events in the past 12 months, availability of emotional/practical supports, level of daily hassles, relationship with mother and partner, baby gender desired and past history of abuse (sexual, physical and emotional). Women also completed an EPDS at the time of recruitment; the results of the antenatal EPDS are not discussed in the present paper. In services where existing depression screening/assessment protocols were already established (e.g. in New South Wales as part of the Integrated Perinatal Care (IPC) programme [23]), the format of the PSRFQ was modified to meet local requirements. This resulted in responses to certain items in the PSRFQ (e.g. education and income) not being collected.
Postnatal screening protocol
At 6–8 weeks after childbirth, women completed a second EPDS. Where possible, links between antenatal and postnatal health services were utilized via the local maternal–child health service, which serviced the region where antenatal screening had been introduced. Where these links did not exist, the EPDS was administered through a direct mail-out from the State beyondblue Program office to the woman's home address. Results were entered in a central database and any women who did not return the EPDS were contacted by telephone or received a reminder letter on at least one occasion. All women who received the EPDS via mail, and scored >12 were contacted by telephone and offered contact details of postnatal support services in their area and advised to visit their GP. Courtesy letters were also sent to GPs informing them of their patient's participation in the beyondblue Program and of the elevated EPDS score.
Statistical analysis
Demographic and EPDS data were summarized with frequencies and percentages for each State.
An overall χ2 test was performed to test whether there was an association between State and the proportion of women with EPDS > 12. Because this forms a large contingency table a significant result from the χ2 test would not be particularly informative. Therefore, a logistic regression model was fitted, with State as a term to further explore State differences. Victoria was used as the reference State because (i) there was a large sample in Victoria, which stabilizes a model; and (ii) the prevalence in Victoria was the same as the overall National average. To take into account imbalances between demographic variables between the states, which may bias the data, a second logistic regression model was fitted in which key demographic variables (age, born in Australia, married/defacto vs not, private vs public) were included. The adjusted odds ratio for State provides an indication of differences between States, again using Victoria as the reference State.
Results
A total of 22 968 women were approached with a follow-up postnatal EPDS. Of those, 12 361 women, of whom 12 266 women had completed the antenatal EPDS, completed the postnatal EDPS, giving an overall response rate of 53.8%. Demographic data on the women who responded postnatally are cross-tabulated by State in Table 2. The mean age was 30.3 years compared to the 2002 national average of women giving birth of 29.4 years [24]. Individual states varied, with mean ages ranging from of 29.4 to 33.9 years. A total of 78.8% of women were born in Australia, compared to the 2002 national maternal average of 77.9% [25]. This ranged from 57.9% in New South Wales, where there was a strong ethnic representation from participating hospitals such as Liverpool and surrounding suburbs, to 95.2% Australian-born in Tasmania, which reflects a less ethnically diverse State.
Characteristics of women by State
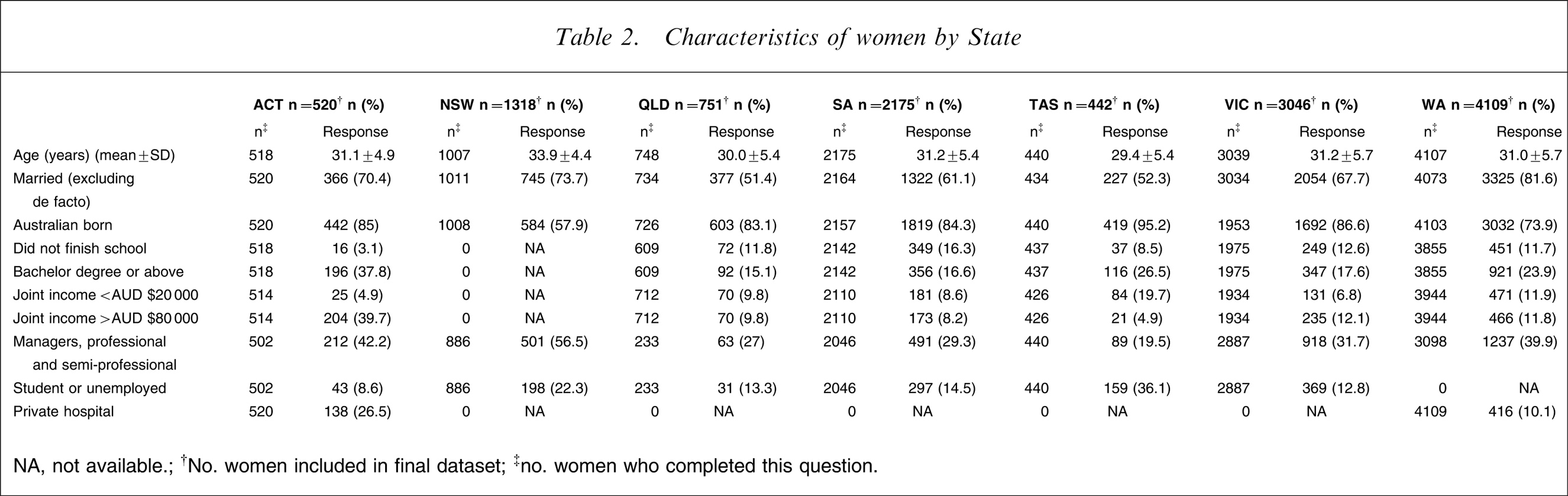
NA, not available; †No. women included in final dataset; ‡no. women who completed this question
Table 3 reports the EPDS scores > 9 (moderate likelihood of depression) and >12 (high likelihood of depression) on a State-by-State basis.
Postnatal EPDS scores by State

EPDS, Edinburgh Postnatal Depression Scale.
Differences in the prevalence rates were examined further in Table 4, using Victoria as the reference state because of its large sample size, which stabilizes the model. Using this model, Queensland and South Australia had significantly higher rates of EPDS >12 than Victoria, while that in Western Australia is lower. Although Tasmania appears to have a higher depression prevalence rate than Victoria, this difference was not statistically significant, probably due to the small sample size of the Tasmanian population. When the odds ratios were adjusted for differences in demographic variables, differences in Queensland rates are explained, but South Australia continues to have a significantly higher rate and Western Australia a lower rate of EPDS scores >12. In considering these variations between States, different questionnaire response rate could be an important factor; response rates were high from Western Australia (79.4%) and Australian Capital Territory (71.5%), low for Queensland (46%) and similar for other States (54.2-56.6%).
Odds ratios EPDS > 12 by State (n = 10 820†)
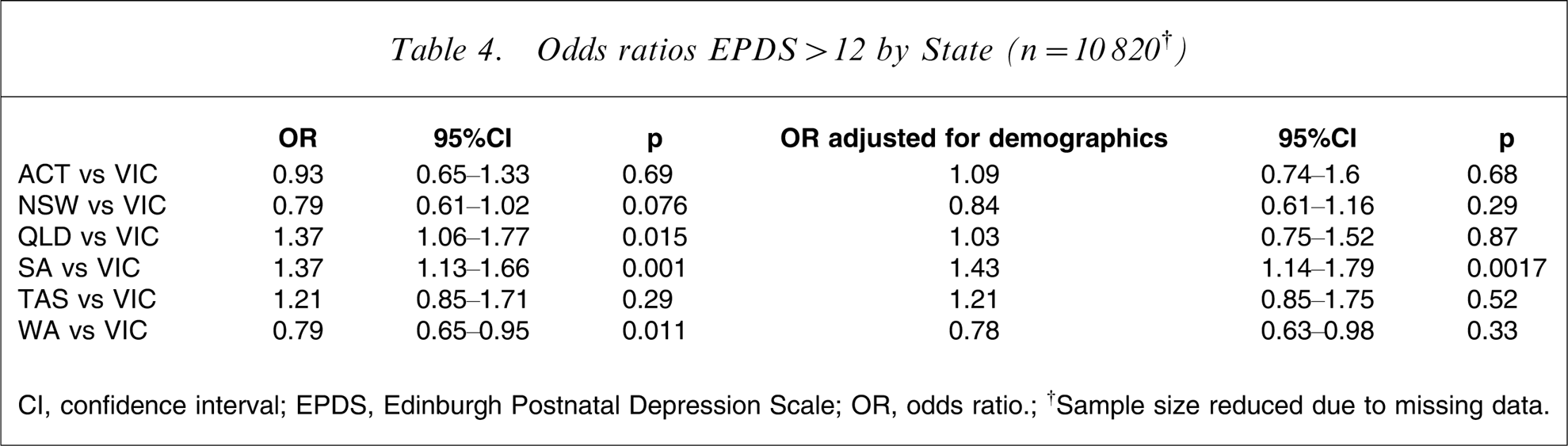
CI, confidence interval; EPDS, Edinburgh Postnatal Depression Scale; OR, odds ratio; †Sample size reduced due to missing data.
Table 5 compares public and private patients in the Australian Capital Territory, where income and education was high in both groups, and Western Australia. There was no difference in rates of EPDS >9 (16.5% vs 14.5%, p = 0.583) or >12 (7.6% vs 5.8%, p = 0.482) in the Australian Capital Territory. However, in Western Australia, public patients were more likely than private patients to have EPDS scores >9 (13.5% vs 8.7%, p = 0.005) and >12 (6.4% vs 3.6%, p = 0.026).
Postnatal EPDS scores: public vs private
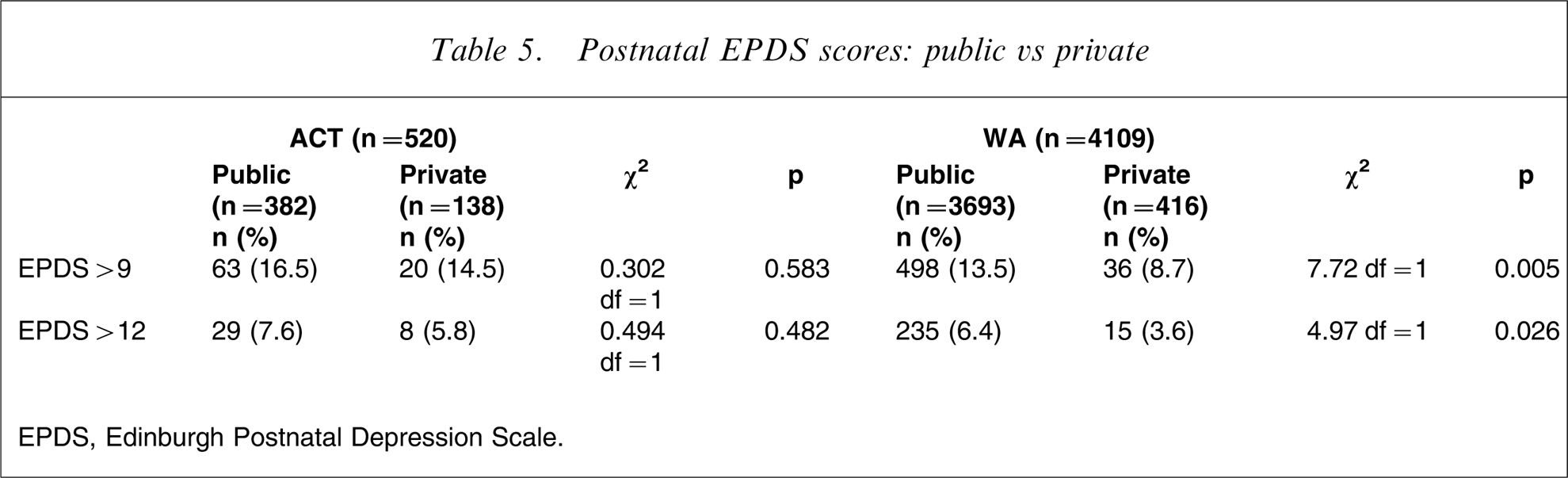
EPDS, Edinburgh Postnatal Depression Scale.
Discussion
This study examines for the first time, the point prevalence of probable postnatal depression in a large sample of women across Australia using the EPDS as a screening instrument. The present findings are somewhat restricted because of the study's link to a larger public health initiative, principally involving public hospitals, which were not randomly selected. However, because of representation from hospitals in regional, rural and remote areas as well as public and private, and women from culturally and linguistically diverse backgrounds, it provides the best and most complete overview yet available of the mental health status of women giving birth in Australia in the period 2002–2004.
The overall prevalence of probable major depression, using EPDS > 12, was found to be 7.5%, which is lower than that reported by O'Hara and Swain, who found 13% when combining self-report point and period prevalence [1]. It is also lower than other screening studies in Victoria that reported a point prevalence rate of 12.8% (n = 4148) using EPDS ≥12 at 4 months following childbirth [26] and 16.9% (n = 1336) at 6–7 months following childbirth [12]. However, results are almost identical to those reported by Austin et al. using a very similar screening methodology and with similar dropout rates [27].
The prevalence of probable postnatal depression reported here is close to that reported by Gavin et al. using diagnostically ascertained caseness [13]. Although the present study's bias towards public hospitals meant a higher proportion of low income and low education level families, which may have led us to expect a higher point prevalence rate, this was not the case. Given that studies using self-report screening tools tend to over-report rates of depression compared to those using diagnostic tools [13], the lower point prevalence in this and others studies [27] may partially be explained by the significant non-responder rates.
The timing of the assessment is likely to be relevant. Brown and Lumley have demonstrated that rates of depression are much higher when women are sampled later in the postnatal year [12]. This suggests that timing of screening is an important consideration. The current study used a screening time of 6–8 weeks after childbirth, compared to that used in the Brown and Lumley study of 6–7 months, as a matter of convenience to determine if linking screening with routine postnatal care was feasible. Given that presentation of depressive symptoms lies along a continuum of both prevalence and severity, we recommend that there is ongoing evaluation of mental health in the postnatal period, with up to three points in time for it to be highlighted: 6–8 weeks; 3–4 months and 6–8 months. This approach will ensure that the greatest number of distressed women is identified, particularly given women are often missed at one or more times [28].
The low rate of elevated EPDS scores in the private sector may be due to the better socioeconomic and educational status of these women. It could also reflect the ability of these women to access appropriate support services earlier in their distress or that educated women are more concerned about stigma [29] (i.e. not completing the EPDS accurately). This fact did not seem to be an issue for the privately insured women in Australian Capital Territory, where the response rate was also high (71.5%), although numbers were lower in Australian Capital Territory than Western Australia.
With respect to individual State differences, there were significantly lower rates of depression in Western Australia and New South Wales, compared to the other States. This may be explained by the presence of established antenatal and/or postnatal depression screening/assessment protocols in these states. The longstanding nature of these programmes compared to their recent introduction in other States may itself have produced an effect of lowering depression rates by increasing overall awareness of perinatal mental health issues in participants. This idea is supported by our evaluation of the positive impact on being involved in a screening programme through an improved ability to recognize depressive symptoms in the postnatal period and higher rates of satisfaction with service and support options [15], [17].
The most obvious limitation of the present study was the response rate, with only 58.2% of women returning their EPDS. Although this is comparable with other Australian studies (75%, 71.4%, 62.5%, 50.1% [4], [11], [12], [30]), the results presented should be considered with caution because the women sampled may not be truly representative of the Australian population. It is also important to consider the mental health status of women who did not respond, because previous studies have suggested that depressed women are less likely to complete questionnaires relating to their mood than their non-depressed counterparts [27]. However, Queensland, with a low response rate but high prevalence, goes somewhat against this argument. Although it was not possible to determine why women refused to complete the EPDS, we suggest that this may be due to the high levels of stigma, fear and shame associated with acknowledging a postnatal mood disorder.
Conclusions
Depression during the postnatal period has been demonstrated to have significant long-term impacts on the woman [31], [32], her partner [33], [34] and her children [35–37]. Postnatal psychiatric illness is now reported as a leading cause of maternal death in Australia [38]. Hence, postnatal depression, and perinatal mental health in general, represents a serious public health issue that demands attention.
This study confirms that postnatal depressive symptoms, as assessed using the EPDS, affect a significant number of women giving birth in Australia, the point prevalence of which appears higher for women in the public sector, with lower socioeconomic and educational levels. Conversely, the point prevalence rate of elevated EPDS scores is lower in States where screening protocols have been established.
The present study spanning 43 centres, while having methodological limitations, has allowed us to identify the minimum number of women affected by probable postnatal depression. Given the limited response rate, it is likely the true point prevalence has been underestimated. Intriguingly, reduced prevalence rates in the two States with long-standing perinatal screening and early intervention programmes, suggests that such a process reduces morbidity for this population. This strengthens the case for the need to urgently consider how to identify and manage the emotional health needs of women antenatally in obstetric services, as we have advocated previously [16]. Specific State-related issues, such as availability of specialist perinatal mental health services and liaison between treating health professionals, also need to be considered.
Footnotes
Acknowledgements
This study was funded by beyondblue. Thanks to all the women participating in this study and the many agencies that supported this project.