
Abstract
Objective:
Amongst people with a mental illness, modifiable health risk behaviours contribute substantially to increased chronic disease morbidity and mortality. This study examined the prevalence of and interest in changing such behaviours amongst community mental health service clients in Australia.
Method:
A telephone interview was undertaken with Australian community mental health service clients. Participants reported engagement in four health risk behaviours: tobacco smoking, fruit and vegetable consumption, alcohol consumption, and physical activity. Participants were classified as at risk based upon Australian national guidelines. At-risk participants were asked whether they were considering improving their health risk behaviour within the next month. The association between psychiatric diagnosis and risk, and interest in improving health risk behaviours was examined.
Results:
Risk prevalence was highest for inadequate vegetable consumption (78.3%), followed by inadequate fruit consumption (60%), smoking (50.7%), physical inactivity (46.8%), short-term alcohol risk (40.3%) and chronic alcohol risk (35.3%). A majority of at-risk participants were considering improving their health risk behaviour for smoking, physical inactivity and inadequate fruit and vegetable consumption (65.1%, 71.1%, and 53.3%, respectively). After adjusting for demographic factors, no diagnostic categories were associated with risk for any behaviour. Those with a diagnosis of depression were more likely to be interested in quitting smoking and increasing physical activity.
Conclusions:
Regardless of diagnosis, a high prevalence of chronic disease health risk behaviours was identified, with many participants expressing an interest in improving these behaviours. Such findings reinforce recommendations that preventive care addressing the chronic disease risks of clients be provided routinely by mental health clinicians.
Trial Registration:
Australian New Zealand Clinical Trials Registry (ANZCTR) ACTRN12613000693729. URL: www.anzctr.org.au/
Keywords
Background
People with a mental illness experience higher rates of morbidity and mortality associated with chronic diseases than the general population, and a substantially lower life expectancy accordingly (Kilbourne et al., 2009; Lawrence et al., 2013). For example, review evidence indicates an increased likelihood of obesity, metabolic syndrome, diabetes, cardiovascular diseases, and respiratory diseases amongst people with a mental illness (de Hert et al., 2011). In the United Kingdom, the standardised mortality rates for circulatory and respiratory disease amongst people with a diagnosis of schizophrenia have been estimated at 2.6 and 4.9 times that of the general population, respectively (Brown et al., 2010). In Australia, the life-expectancy gap between those with a mental illness and the general population is estimated at 15.9 years for males and 12.0 years for females, with 77.7% of excess deaths attributed to physical health conditions (Lawrence et al., 2013). Four modifiable health risk behaviours are considered to contribute substantively to the greater chronic disease burden for people with a mental illness: tobacco smoking, inadequate nutrition, harmful alcohol consumption and physical inactivity (Kilbourne et al., 2009; Lawrence et al., 2013). Improvements in such health risk behaviours have been found to result in substantial health benefits and reductions in mortality (King et al., 2007). In Australia, the prevention of chronic disease has become a priority with efforts focusing on reducing tobacco use, addressing the health and social harms caused by risky consumption of alcohol, and reducing overweight and obesity through strategies addressing nutrition and physical activity, with specific acknowledgement of the need to address such behaviours within disadvantaged populations such as those with a mental illness (National Preventive Health Taskforce, 2008). Strategies have included various population health approaches including taxation, legislative, and marketing strategies.
Research examining the prevalence of chronic disease health risk behaviours among people with a mental illness has primarily focused on smoking (Lawrence et al., 2009; Reichler et al., 2001; Stockings et al., 2013; Ussher et al., 2011), with smoking rates consistently reported to be at least double that of the general population (Lawrence et al., 2009) and in certain sub-groups as high as 80–90% (Reichler et al., 2001; Ussher et al., 2011). Relatively fewer studies have examined the prevalence of other health risk behaviours among people with a mental illness, with such studies reporting that people with a mental illness are more likely to have unhealthy diets (Kilian et al., 2006; McCreadie, 2003). Variable findings have been reported with respect to the prevalence of other risk behaviours, with separate studies reporting either higher or lower rates of alcohol consumption or misuse (Davidson et al., 2001; Kilbourne et al., 2009; Kilian et al., 2006; Reichler et al., 2001), and either higher or lower levels of physical activity relative to the general population (Davidson et al., 2001; Kilbourne et al., 2009; Kilian et al., 2006).
The research that has examined the prevalence of multiple chronic disease health risk behaviours among people with a mental illness has primarily focused on patients with a specific diagnostic category (Filia et al., 2011; Hahn et al., 2014; McCreadie, 2003; Reichler et al., 2001; Ussher et al., 2011), most often schizophrenia (Filia et al., 2011; Hahn et al., 2014; McCreadie, 2003; Ussher et al., 2011), or those in inpatient settings (Kilian et al., 2006; Reichler et al., 2001; Ussher et al., 2011). Limited research has reported the prevalence of such health risk behaviours among people with other psychiatric illnesses, particularly among people with anxiety or depression, the most prevalent forms of mental illness (Kessler et al., 2009). In one such study, conducted in the United Kingdom (UK) of 956 community-dwelling people with a range of mental illness diagnoses, 50% of participants were smokers, with 37% undertaking no regular physical activity and 32% reporting poor nutrition (Smith et al., 2007). The generalisability of such findings is, however, limited by the inclusion of only those clients who their clinicians believed would benefit from a physical health program. No data were reported in the study regarding the prevalence of health risk behaviours by different diagnostic categories.
Contact with a mental health clinician is suggested to represent a key opportunity for addressing the chronic disease health risk behaviours of people with a mental illness (Lawrence et al., 2013). Despite such care being supported by clinical guidelines (NICE, 2010; NSW Health, 2009), its provision by mental health clinicians has been reported to be sub-optimal (Bartlem et al., 2014; Johnson et al., 2009), due in part to the perception by mental health professionals that clients are unwilling to improve their risk behaviours (Happell et al., 2012; Price et al., 2007; Wye et al., 2010). For example, in a survey of United States (US) community mental health psychiatrists, approximately one-quarter (23%) reported their clients do not want to quit smoking (Price et al., 2007), whilst in an Australian survey of psychiatric inpatient nurse unit managers, most participants (69%) believed that their clients were not interested in quitting (Wye et al., 2010).
In contrast to such perceptions by clinicians, research has suggested that a large proportion of people with a mental illness express a clear interest in changing their health risk behaviours, though most research has focused upon interest in quitting smoking (Ashton et al., 2013; Siru et al., 2009; Stockings et al., 2013). For example, in a recent Australian study of 1043 smokers with a mental illness, 88% reported wanting to quit smoking (Ashton et al., 2013), whilst a systematic review of motivation to quit smoking amongst people with a mental illness indicated that those with a mental illness are as motivated to quit smoking as the general population, with similar proportions of smokers classified within the contemplation (38% vs 33%) and preparation (19% vs 10%) stages of change (Siru et al., 2009).
Only four studies could be identified that examined the level of interest among people with a mental illness in changing other health risk behaviours (Buhagiar et al., 2011; Filia et al., 2011; Prochaska et al., 2014; Ussher et al., 2007). One study of physical activity beliefs and preferences amongst people with a variety of mental illnesses in the UK identified that half of the participants reported a strong interest in increasing their physical activity (Ussher et al., 2007). A higher level of interest was reported in an Australian study of people with a psychotic illness, with most contemplating quitting smoking (93%), improving their nutrition (84%), or increasing their physical activity (79%) (Filia et al., 2011). Similarly, in a UK study of outpatient mental health clients, including those with or without a psychotic illness, a large majority indicated a desire to improve their exercise (85–97%), diet (75–90%), and stop smoking (69–86%) (Buhagiar et al., 2011). Lastly, in the US, substantial proportions of psychiatric inpatient smokers participating in a tobacco treatment trial reported being in the preparation stage of change for binge alcohol consumption (57%), physical inactivity (51%), fruit and vegetable under-consumption (46%) and tobacco smoking (23%) (Prochaska et al., 2014). Further research is required to confirm the level of interest in changing health risk behaviours among people with a variety of types of mental illness to support the development of appropriate preventive care interventions to be delivered by mental health care professionals.
Given the limitations of the available evidence, a study was undertaken to investigate the prevalence of chronic disease health risk behaviours in people with a mental illness, and the interest of people with such an illness in changing these risks.
Methods
Design and setting
A cross-sectional survey was undertaken of community mental health clients in New South Wales, Australia (December 2011 to November 2012, inclusive). Ethical approval was obtained from the Hunter New England Human Research Ethics Committee (approval no. 09/06/17/4.03) and the University of Newcastle Human Research Ethics Committee (approval no. H-2010-1116).
Participants and recruitment
Community mental health services
All 12 community mental health services in a primarily metropolitan area were eligible for the study and invited to participate. The services provided a variety of forms of care that included general community mental health care and care to more specialised mental health populations, including older persons, psychiatric rehabilitation, early diagnosis, comorbid substance use, eating disorders and borderline personality disorder. Such services were staffed by multidisciplinary teams including nurses, psychologists, social workers, dieticians, occupational therapists, and psychiatrists. Clients were referred to the services through a variety of routes, including a general practitioner or other health provider, following discharge from a psychiatric hospital, or self-referral. Services providing inpatient care or care solely to clients under the age of 18 years were not eligible for inclusion.
Clients
Community mental health clients attending all 12 mental health services were eligible to participate if, based on electronic medical record data, they: were at least 18 years of age, had attended at least one face-to-face appointment with a clinical member of staff at any of the eligible services during the previous 2 weeks, had not previously been selected to participate (based on client identification number), and were not identified by their clinician as inappropriate to contact.
Over a period of 12 months, a weekly random sample of approximately 22 eligible clients (approximately 5% of total weekly eligible clients) was selected from the electronic medical records system using the survey select procedure in SAS v9.3. Selected clients were posted an information letter outlining the study. Clients were contacted by phone approximately 2 weeks later to further determine their eligibility, specifically that they: were English-speaking; not residing in an aged care facility; and were physically and mentally capable of responding to the survey items. Eligible consenting participants were administered a computer-assisted telephone interview at that time, or a more suitable time for completion of the survey was arranged.
Measures
Demographics and clinical descriptors
Items and response options were sourced from previously reported surveys of community health clients (McElwaine et al., 2013). Participants were asked to report their: Aboriginality, highest education level attained, current employment status, current marital status, and any psychiatric diagnoses for which they had received medical attention or taken medication within the last 2 months (depression, bi-polar disorder, schizophrenia or other psychotic disorders, anxiety disorders, other). Age, sex, postcode, service attended, and number of community mental health appointments within the previous 12 months were attained from the electronic medical records system for consenters and non-consenters.
Risk status
Participants were asked to report their health risk behaviours during the month prior to seeing the community mental health service. Survey items and response options are based on validated items from recommended assessment tools (Australian Bureau of Statistics, 1997; Babor et al., 2001; Heatherton et al., 1991; Marshall et al., 2008) and have been used previously in community surveys (McElwaine et al., 2013). Questions included: whether they had smoked any tobacco products; how many serves of fruit, and of vegetables they consumed on average per day; how many days per week they engaged in at least 30 minutes of physical activity; and how often they had a drink containing alcohol. Those who had consumed alcohol were further asked: how many standard drinks they consumed on a typical drinking day and how often they consumed more than four standard drinks on one occasion. As per the Australian national guidelines, risk was defined as: any reported smoking (Ministerial Council on Drug Strategy, 2004); consuming less than two serves of fruit, or five serves of vegetables per day (National Health & Medical Research Council (NHMRC), 2003); consuming more than two standard alcoholic drinks on a regular drinking day (chronic alcohol risk) or more than four standard drinks on any one occasion (short-term alcohol risk) (NHMRC, 2009); or engaging in less than 30 minutes of physical activity on at least 5 days a week (Department of Health and Aged Care, 1999).
Interest in modifying health risk behaviours
With respect to each health risk behaviour that participants were classified as being at risk for at the time of interview, participants were asked whether, over the next month, they were seriously considering: quitting smoking, eating more vegetables and/or fruit, reducing their alcohol intake, and doing more physical activity (yes, no, don’t know). Single-item measures of interest in change have been demonstrated to predict previous smoking quit attempts (Stockings et al., 2013) and to predict smoking cessation as accurately as measures containing multiple items (Sciamanna et al., 2000).
Statistical analysis
The SAS analysis package (SAS, v9.3) was used to analyse the data. Condensed response categories were created for the following variables, as shown in Table 1: age, Aboriginality, highest education level attained, employment status, marital status, geographic location, index of disadvantage, and number of community mental health appointments in the past 12 months. Residential postcode was used to calculate each clients’ geographic remoteness (Department of Health and Aged Care, 2001) and socio-economic index of disadvantage (Australian Bureau of Statistics, 2008). Participants who did not know to what extent they engaged in a health behaviour, were considered, on a conservative basis, to be at risk. Participants who did not know if they were seriously considering improving their health behaviour, were considered, on a conservative basis, that they were not considering such a change. Variables were created to reflect overall nutrition risk (at risk for inadequate fruit and/or vegetable consumption) and overall alcohol risk (chronic alcohol risk and/or short-term alcohol risk).
Demographic description of sample (n=558).
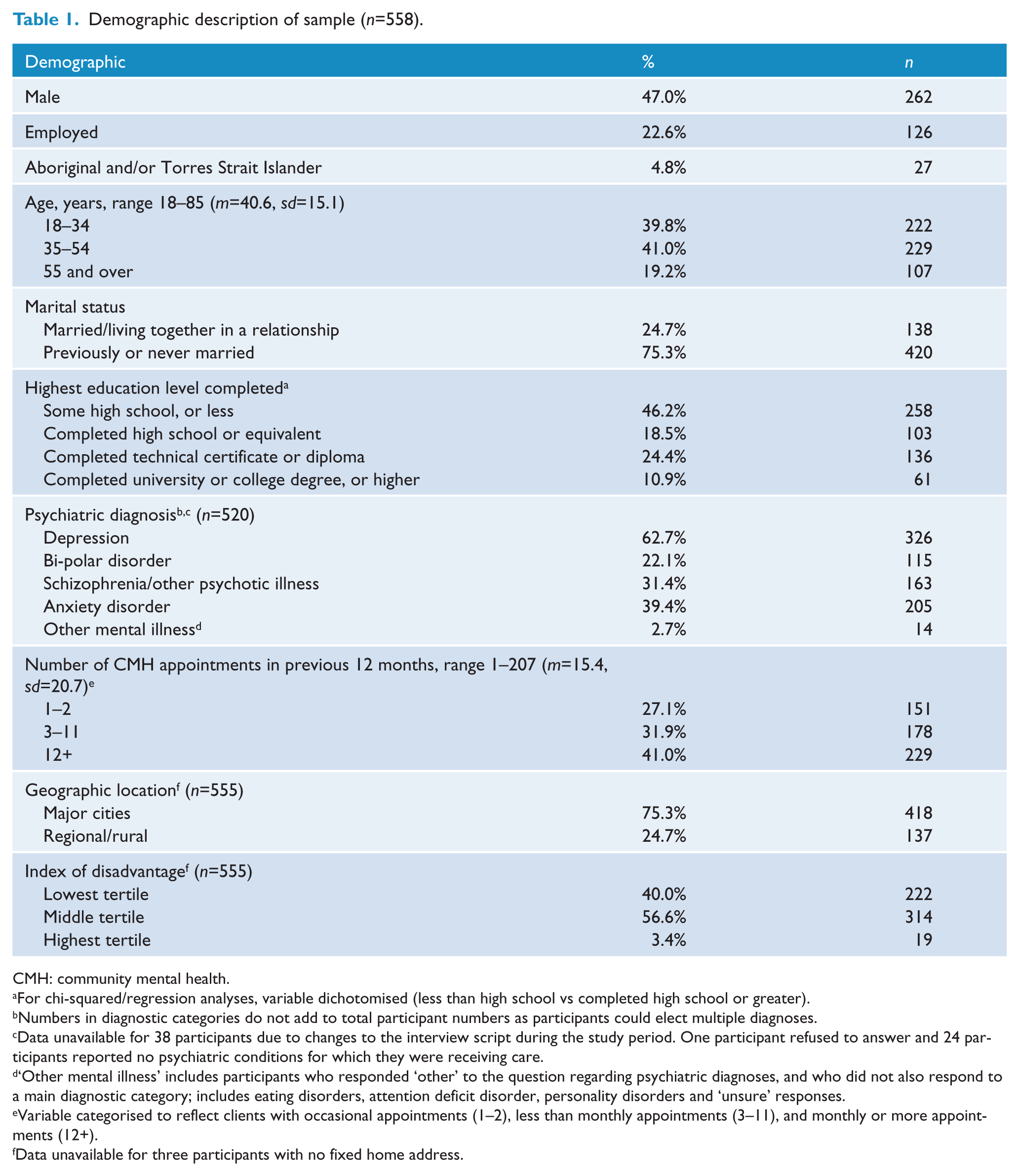
CMH: community mental health.
For chi-squared/regression analyses, variable dichotomised (less than high school vs completed high school or greater).
Numbers in diagnostic categories do not add to total participant numbers as participants could elect multiple diagnoses.
Data unavailable for 38 participants due to changes to the interview script during the study period. One participant refused to answer and 24 participants reported no psychiatric conditions for which they were receiving care.
‘Other mental illness’ includes participants who responded ‘other’ to the question regarding psychiatric diagnoses, and who did not also respond to a main diagnostic category; includes eating disorders, attention deficit disorder, personality disorders and ‘unsure’ responses.
Variable categorised to reflect clients with occasional appointments (1–2), less than monthly appointments (3–11), and monthly or more appointments (12+).
Data unavailable for three participants with no fixed home address.
Descriptive statistics were used to examine the demographic and clinical characteristics, the prevalence of each health risk behaviour and risk for multiple behaviours by diagnostic category, and interest in reducing risk by diagnostic category. Chi-squared analyses were used to obtain unadjusted odds ratios for the association between each main diagnostic category and participant risk status for each health risk behaviour (smoking, overall nutrition risk, overall alcohol risk, and physical inactivity) and between each main diagnostic category and participant interest in reducing behavioural health risks. Logistic regression models were used to examine those same associations to obtain odds ratios adjusting for age, sex, employment status, marital status, education, and Aboriginality.
Results
Participants
All 12 facilities agreed to participate in the study. Of the 1106 eligible participants selected, 903 (82%) were able to be contacted. Of those contactable, 129 (14%) were excluded due to ineligibility upon contact (primarily being mentally or physically incapable of responding to survey items, n=69). Of the remaining 774, 558 (72%) consented and completed the interview, with females being more likely to do so than males (76.2% vs 67.9%, p=0.009).
The mean age of participants was 40.6 years (range 18–85 years), with the greatest proportion of participants in the 35–54 age category (41%). The majority of participants (95.2%) were not of Aboriginal or Torres Strait Islander origin. The most common psychiatric disorder for which participants were receiving care or taking medication was depression (62.7%) (Table 1).
Prevalence of behavioural health risks
Across the risk behaviours, participants were most likely to be at risk for inadequate vegetable consumption (78.3%) and inadequate fruit consumption (60%); they were least likely to be at risk for harmful alcohol consumption (35.3% for chronic alcohol risk, 40.3% for short-term alcohol risk). Approximately half of the sample was smokers (50.7%), and a similar proportion reported being physically inactive (46.8%). Ninety-six percent of participants were at risk for at least one health risk behaviour, 78.4% were at risk for two or more behaviours, and 10.2% were at risk for all four risk behaviours (Table 2).
Participants at risk for health risk behaviours and multiple risks by diagnosis a .
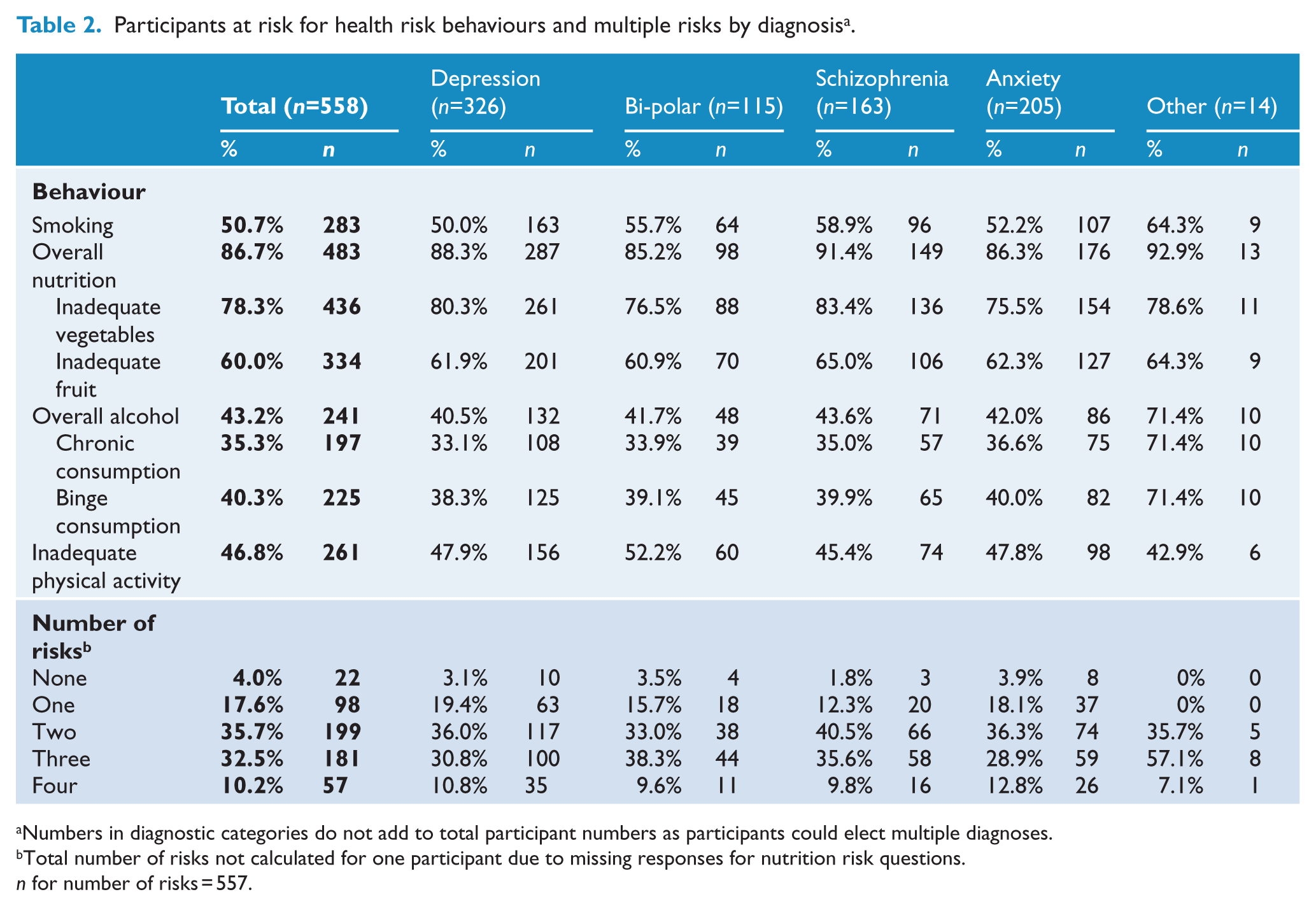
Numbers in diagnostic categories do not add to total participant numbers as participants could elect multiple diagnoses.
Total number of risks not calculated for one participant due to missing responses for nutrition risk questions. n for number of risks = 557.
Interest in modifying health risk behaviour
With the exception of harmful alcohol consumption, approximately one half or more of participants, regardless of diagnosis, expressed an interest in modifying their health risk behaviours. The majority of participants at risk due to smoking, physical inactivity or inadequate fruit and/or vegetable consumption were considering modifying their health risk behaviour (65.1%, 71.1% and 53.3%, respectively). Approximately one-quarter of participants at risk due to chronic and/or short-term alcohol consumption expressed an interest in decreasing their alcohol consumption (27.9%) (Table 3).
At-risk participants interested in modifying their health risk behaviours, by diagnosis a .
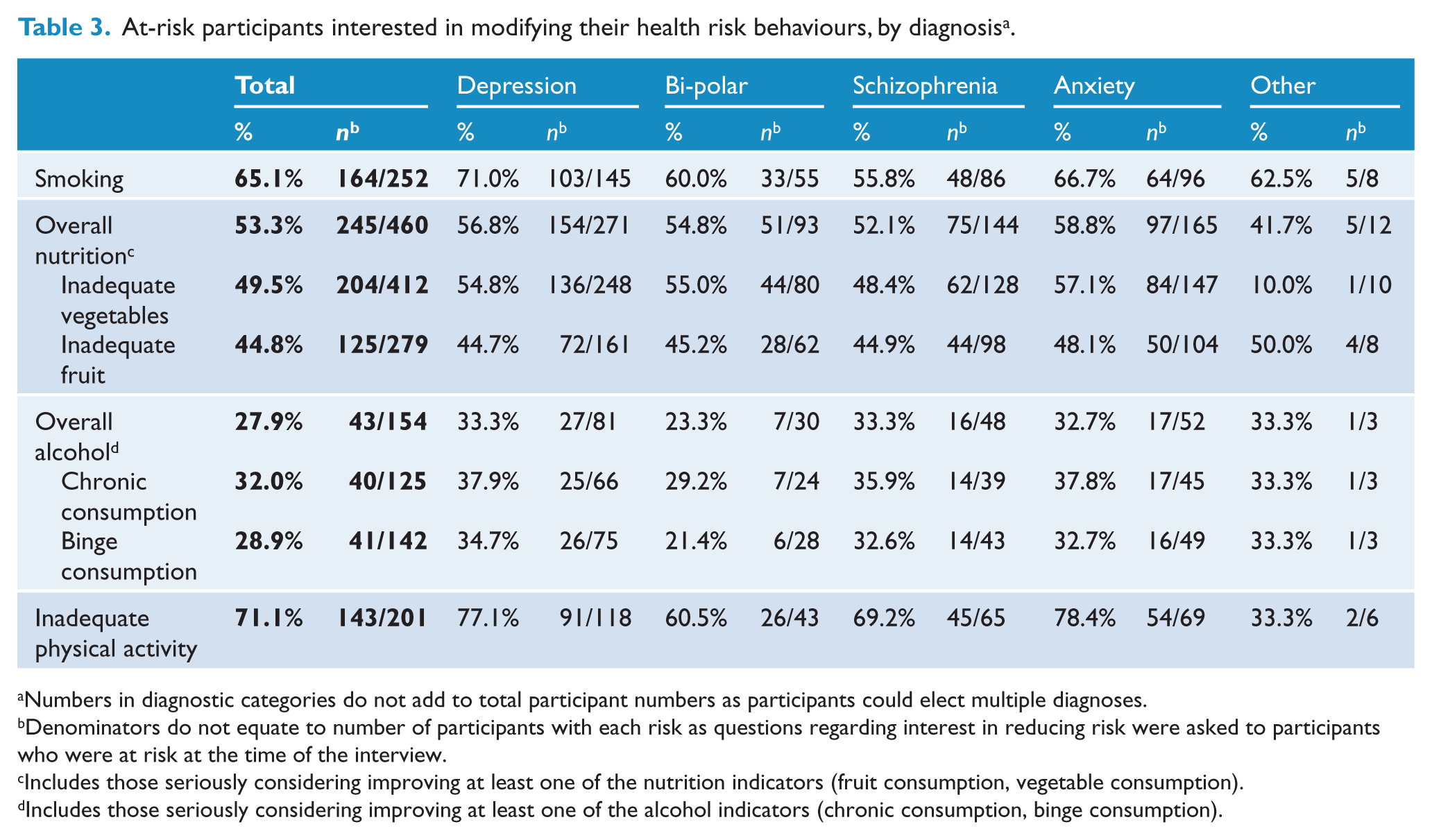
Numbers in diagnostic categories do not add to total participant numbers as participants could elect multiple diagnoses.
Denominators do not equate to number of participants with each risk as questions regarding interest in reducing risk were asked to participants who were at risk at the time of the interview.
Includes those seriously considering improving at least one of the nutrition indicators (fruit consumption, vegetable consumption).
Includes those seriously considering improving at least one of the alcohol indicators (chronic consumption, binge consumption).
Association between participant diagnosis, health risk behaviours, and interest in modifying health risk behaviours
After adjusting for demographic factors, no diagnostic categories were associated with risk status for any of the health risk behaviours (Table 4). Those with a diagnosis of depression were more likely than those with other diagnoses to be interested in quitting smoking (OR 1.96, p=0.02) and increasing their physical activity (OR 2.24, p=0.02) (Table 5).
Diagnostic associations with risk status.
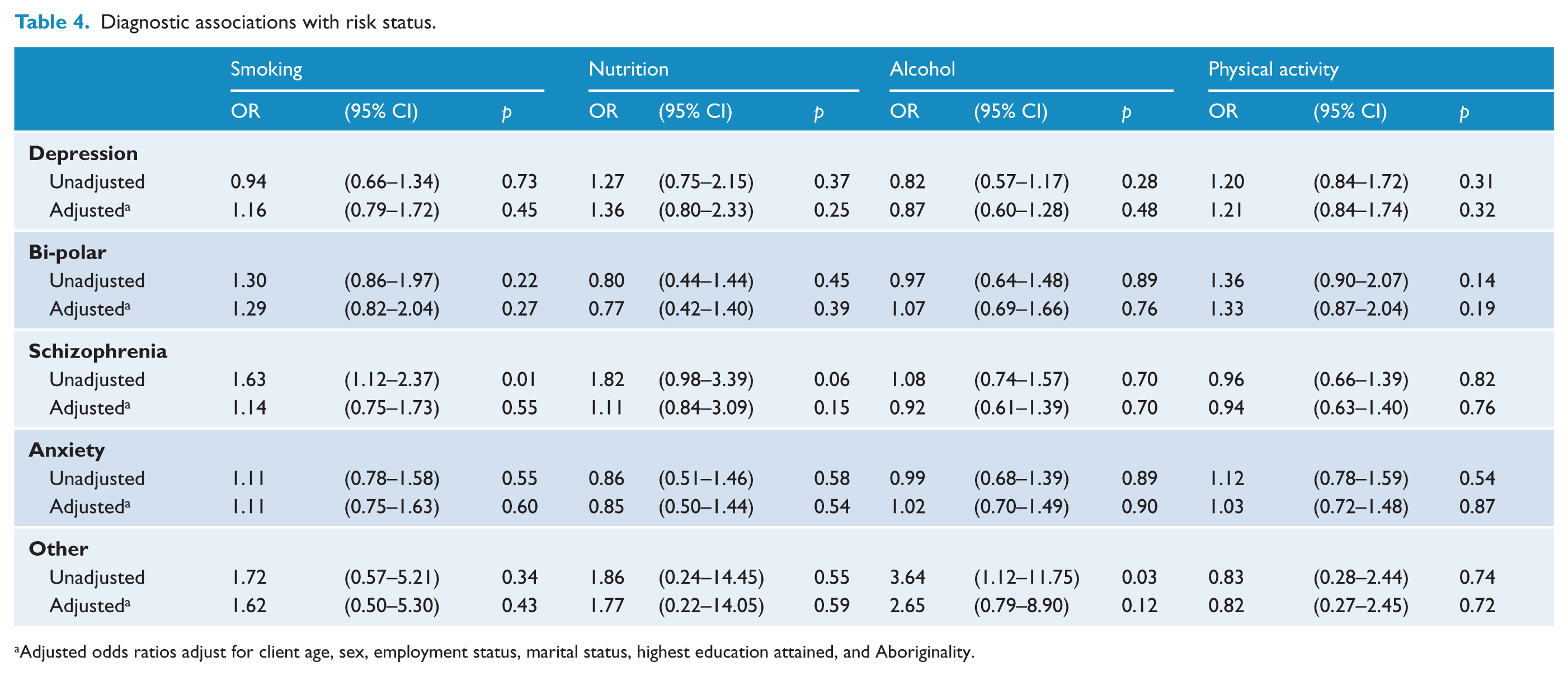
Adjusted odds ratios adjust for client age, sex, employment status, marital status, highest education attained, and Aboriginality.
Diagnostic associations with interest in improving health risks, for those at risk for each behaviour.
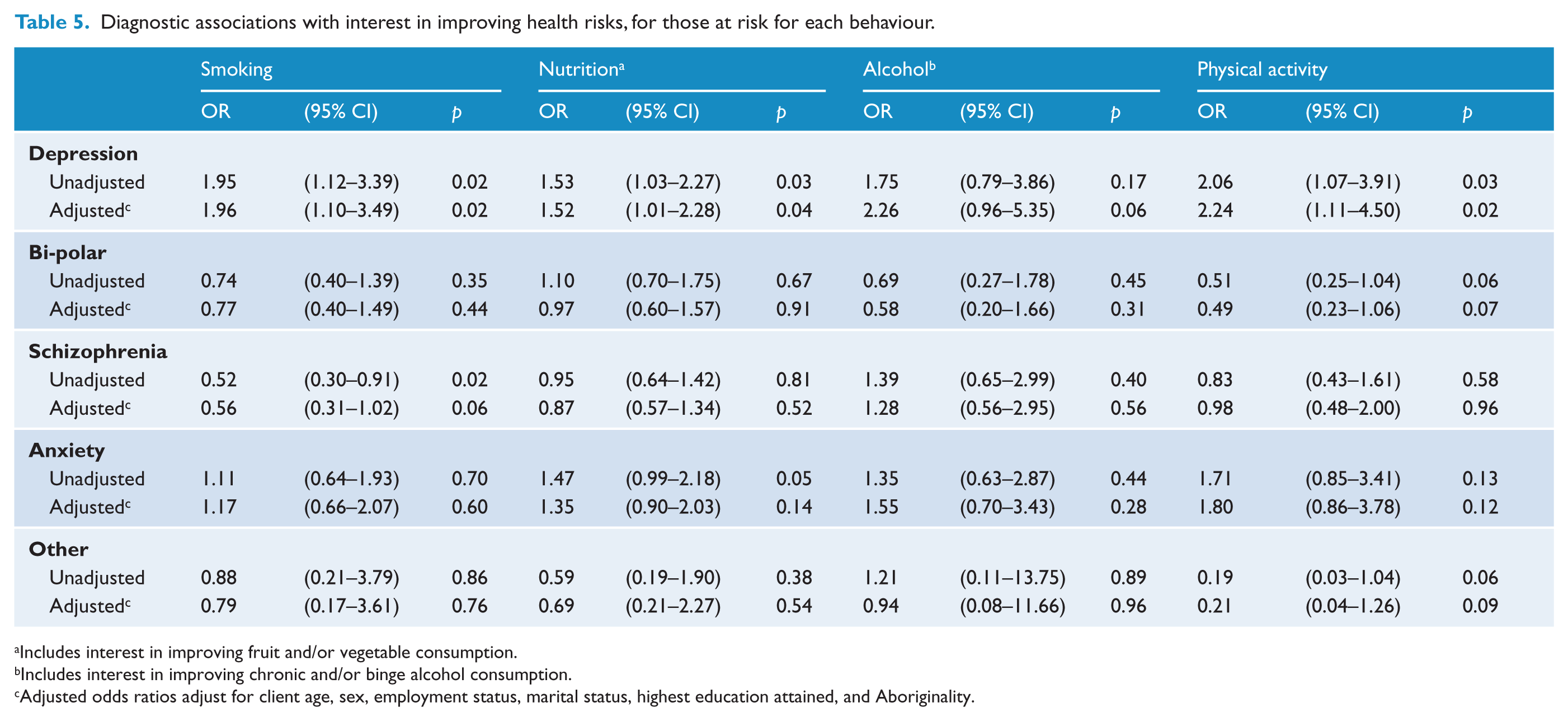
Includes interest in improving fruit and/or vegetable consumption.
Includes interest in improving chronic and/or binge alcohol consumption.
Adjusted odds ratios adjust for client age, sex, employment status, marital status, highest education attained, and Aboriginality.
Discussion
The study findings indicate a high prevalence of chronic disease health risk behaviours amongst community mental health clients, with a significant proportion of clients having multiple risks. Type of psychiatric diagnosis was not found to be associated with the likelihood of being at risk for any of the four health risk behaviours assessed. Between a half and three-quarters of at-risk participants expressed an interest in modifying their smoking, physical inactivity and inadequate fruit and vegetable consumption, and one-quarter expressed an interest in modifying their at-risk alcohol consumption. Participants with depression were more likely to express an interest in changing their smoking and physical inactivity than were those with other diagnoses. Such findings demonstrate a need and an opportunity for the development of interventions to support mental health clinicians to routinely provide care to all clients to reduce such health risk behaviours.
Despite an inability to make direct comparisons due to methodological differences between studies, the high prevalence of health risk behaviours is consistent with previous research with mental health clients (Davidson et al., 2001; Hahn et al., 2014; Kilbourne et al., 2009; Kilian et al., 2006; McCreadie, 2003; Smith et al., 2007). When compared to recent Australian data from generalist community health services using the same survey methodology and measures (McElwaine et al., 2013), the prevalence of health behaviour risks was higher in the current study, with the prevalence for smoking, at-risk alcohol consumption and physical inactivity being approximately twice as high. Although in some previous research the prevalence of health risk behaviours has been found to vary by psychiatric diagnosis (Kilbourne et al., 2009; Kilian et al., 2006), the number of such studies is small, limiting the ability to generalise from these findings. It is possible that absence of differences in the prevalence of risk across psychiatric diagnoses may be attributable to the accuracy limitations of self-reported diagnosis. Regardless, the finding in the present study of similarly high levels of risk across all categories of psychiatric diagnosis emphasises the importance of all mental health services addressing the health risk behaviours for all clients.
The high prevalence of multiple risks in the present study supports limited previous research suggesting a high prevalence of multiple health risk behaviours among people with a mental illness (Australian Bureau of Statistics, 2003). When compared to a methodologically comparable study of clients attending generalist community health services (43% with two or more risks) (McElwaine et al., 2013), the participants in this study had a higher prevalence of multiple health risk behaviours (78% with two or more risks). Given growing evidence of the effectiveness of multiple behavioural change interventions in general populations (Prochaska et al., 2006), and the markedly high prevalence of multiple health risk behaviours found in this study, research examining intervention strategies for addressing multiple risk behaviours for people with a mental illness is required (Prochaska et al., 2014).
The finding that, apart from at-risk alcohol consumption, a significant proportion of participants across all diagnostic categories expressed an interest in improving their health risk behaviours, contrasts with the previously reported perceptions of mental health clinicians that clients are unwilling to address their health risk behaviours (Happell et al., 2012; Price et al., 2007; Wye et al., 2010). Such findings may be conservative, however, as being interested in improving a behaviour implies that one is aware of the problematic nature of that behaviour (Prochaska and Velicer, 1997), and awareness was not examined in the current study. Further, although expressing an interest in change may not directly lead to a sustained change in behaviour, health behaviour theory supports the importance of intentions in predicting behaviour change (Cooke et al., 2014; Godin and Kok, 1996). Such findings reinforce the recommendations of clinical guidelines and policies that preventive care addressing the chronic disease risks of clients should be routinely provided by mental health clinicians to all clients (NICE, 2010; NSW Health, 2009). Further research is required to examine client acceptability of receiving preventive care that addresses these health risk behaviours during interactions with their mental health providers.
The markedly lower level of interest in modifying at-risk alcohol consumption is consistent with previously reported lower levels of interest in reducing alcohol consumption in the general population (Chan et al., 2012). An Australian study of generalist community nursing clients identified that fewer clients expressed an interest in reducing their alcohol consumption (48%) compared to quitting smoking (74%), increasing their fruit and vegetable intake (59%) and increasing their physical activity levels (84%) (Chan et al., 2012). In the general Australian population, awareness of the current alcohol consumption guidelines is low (Cotter et al., 2013), particularly amongst those who consume alcohol (Cotter et al., 2013). Among people with a mental illness it is possible that the observed lower level of interest is influenced by the consumption of alcohol as a form of self-medication or a coping mechanism (Bell and Britton, 2014) . Further research is required to identify the reasons for few clients expressing an interest in modifying their at-risk alcohol consumption.
People with a diagnosis of depression were more interested than those with other psychiatric diagnoses in quitting smoking and increasing their physical activity. Such a finding is supported by a review of studies regarding motivation to quit smoking amongst people with a mental illness that also identified a greater motivation to quit amongst those with depression (Siru et al., 2009). For all at-risk participants, regardless of diagnoses, interest in modifying at-risk alcohol consumption was markedly lower than for all other health risk behaviours.
A number of the study characteristics need to be considered when interpreting the findings. First, the observed estimates of risk prevalence may be conservative due to limitations in the accuracy of client report of health behaviours (de Beaurepaire et al., 2007). Second, as mental health diagnosis was based on client self-report, the diagnostic characteristics of the participants may be inaccurate, reflecting self-diagnosis rather than diagnosis by a health professional. However, the distribution of psychiatric diagnoses is consistent with those from larger investigations of the prevalence of mental illness in the community (Kessler et al., 2009). Third, as the study was undertaken within one area in Australia, the generalisability of findings to other health services within Australia and internationally is unknown.
The present study extends the limited data documenting the prevalence of health risk behaviours amongst people with a mental illness within community mental health services. The findings reinforce the need for further research to explore current levels of preventive care provision for this sub-group, and the particular need for interventions to support the provision of such care to people with a mental illness.
Footnotes
Acknowledgements
The authors would like to thank all members of the Preventive Care team, the electronic medical records team, the CATI interviewers, the Aboriginal Advisory group, the community mental health services, and the community mental health service clients for their contribution to the project. Authors KB and CL had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Author KB is responsible for the data analysis.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.