
Abstract
Background:
Research suggests that people suffering from chronic pain have elevated rates of suicidality. With an ageing population, more research is essential to gain a better understanding of this association.
Aims:
To document the prevalence and correlates of chronic pain and suicide, and estimate the contribution of chronic pain to suicidality.
Method:
Data from the 2007 Australian National Survey of Mental Health and Wellbeing, a nationally representative household survey on 8841 people, aged 16–85 years, was analysed.
Results:
The odds of lifetime and past 12-month suicidality were two to three times greater in people with chronic pain. Sixty-five percent of people who attempted suicide in the past 12 months had a history of chronic pain. Chronic pain was independently associated with lifetime suicidality after controlling for demographic, mental health and substance use disorders.
Conclusions:
Health care professionals need to be aware of the risk of suicidality in patients with chronic pain, even in the absence of mental health problems.
Introduction
Chronic pain, defined as pain that persists for greater than three months (Merskey and Bogduk, 1994), is a common worldwide complaint, with rates in the general population estimated from 17% (Blyth et al., 2001) to 41% (Tsang et al., 2008). Chronic pain is associated with poorer physical health (Eriksen et al., 2006), poorer quality of life (Hagg et al., 2003; Ojala et al., 2014) and a greater risk of developing depression (Currie and Wang, 2004) and other mental health problems (Dersh et al., 2002; McWilliams et al., 2003). Although there are behavioural, physical and medication interventions for chronic pain, it is often the case that many patients have to accept a lifetime treatment plan for the management of their pain, which may not alleviate the pain completely (Breivik et al., 2006).
It is not unexpected then, that rates of suicidality (defined as ideation, plans and attempts) are elevated amongst this group (Meilman, 1984). Emerging research suggests that people suffering from chronic pain have almost double the risk of death by suicide (Tang and Crane, 2006). Amongst people with chronic pain, rates of lifetime ideation range from 21% to 50%, current ideation from 0% to 24%, and rates of lifetime suicidal attempts from 5% to 14% (Tang and Crane, 2006). These studies, however, have generally been based on small, clinical samples, so it is unknown if the same pattern exists in the general pain population. Further, recent epidemiological research suggests chronic pain is independently associated with suicidality after controlling for demographic and mental health factors (Braden and Sullivan, 2008; Ilgen et al., 2013; Ratcliffe et al., 2008).
With an ageing population, and the likely increase in chronic pain, the issue of chronic pain and its relationship to suicidality is of timely importance. To our knowledge, there has been no study that has estimated the contribution that chronic pain may make to suicidality in the general population, and there are few existing data on the relationship between chronic pain and suicide in the Australian population. The aims of the current study were to:
document the prevalence of chronic pain in Australia;
examine lifetime and past 12-month suicidal behaviours in people with chronic pain, and estimate the contribution that a history of chronic pain may make to suicidality in the general population;
determine whether chronic pain is associated with suicide when controlling for socio-demographic variables and mental health diagnoses;
determine the risk factors for the past 12-month suicidal behaviours amongst people with chronic pain.
Method
Sample
Data from the Confidentialised Unit Record File (CURF) for the Australian 2007 National Survey of Mental Health and Wellbeing (NSMHWB) (Slade, et al., 2009) were obtained from the Australian Bureau of Statistics (ABS). The 2007 NSMHWB was conducted by trained interviewers from the ABS between August and December of 2007. The aim of the survey was to provide representative estimates on a national level. The 2007 NSMHWB sample was based on a stratified, multistage area probability sample of people aged 16–85 years in rural and urban private dwellings across all Australian States and Territories. The area-based selection ensured that all sections of the population living in private dwelling within the geographical scope of the survey were represented, representing a total of 17,352 dwellings. Special dwellings (hospitals, nursing homes, gaols, hotels) and dwellings in remote and sparsely settled regions of the country were not sampled, which reduced the effective sample size to 14,805 dwellings. All interviews were conducted in English, meaning that non-English speakers were excluded from the sample. Each interview was conducted in person and took approximately 90 minutes to complete.
There were 8841 fully responding participants, which represented a rate of 60%. Owing to the lower than expected response rate (it was expected that a 75% response rate would be achieved), extensive non-response analyses were undertaken to assess the reliability of the survey estimates. A purposive sample of fully non-responding households in two metropolitan areas, Sydney and Perth, was followed up with a short-form interview, to gain a qualitative assessment of non-response bias. The study indicated the impact of non-response to be small at the aggregate level, but possible underestimation of the prevalence of mental disorders may exist for men, young persons and the Perth population. The final sample represented an estimated population count (EPC) of 16,015,000 Australian adults. For further information about the procedure and instrument see Slade et al., (2009).
Survey
The 2007 NSMHWB was based on the World Mental Health Survey Initiative version of the Composite International Diagnostic Interview (WMH-CIDI) (Kessler and Ustun, 2004). This interview has undergone extensive methodological development and testing and has been used in household surveys in at least 28 countries around the world. This version of the instrument collects both diagnostic information on a broad range of mental disorders and information on risk factors, impacts, patterns and treatment of mental disorders. There were some modifications made to the WMH-CIDI to tailor the survey to the Australian context. The following questions and measures from the 2007 NSMHWB were used in the current study.
Chronic pain
The chronic conditions section was based on the WMH-CIDI chronic conditions module. The information provided is self-reported by the respondent and is not verified by a medical practitioner. The current study used questions that related to the presence of arthritis, migraines and back/neck pain that had persisted for a period of 6 months. A combined category of ‘any pain’ was created on the basis of endorsement of any one chronic pain condition (arthritis/migraines, back/neck problems).
Socio-demographics
Consistent with Ratcliffe et al., (2008), age was split into categories of <25 years, 25–44 years, 45–64 years and ⩾65 years, and was dichotomised into above and below 60 years of age when examining bivariate and multivariate relationships. Marital status was dichotomised to married/de facto, with widowed/separated/single/divorced as the reference category. A dichotomous variable was created whereby those who had completed high school were deemed to have completed school. Not completing school was the reference category. Employment was dichotomised: not employed or not in the labour force was the reference category.
Mental health and substance use
The WMH-CIDI produces diagnostic information according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and the International Classification of Diseases, 10th Revision (ICD-10). Only DSM-IV diagnoses were reported here. The WMH-CIDI uses a lifetime time frame, with questions on experiences of symptoms in the previous 12 months in combination with lifetime diagnoses used to establish 12-month diagnoses. Diagnoses were derived using standard WMH-CIDI diagnostic algorithms. DSM-IV lifetime and past 12-month diagnoses were assessed. The following diagnoses were used in the current study based on previous studies (Braden and Sullivan, 2008): major depression (MD), general anxiety disorder (GAD), post-traumatic stress disorder (PTSD), alcohol use disorders (AUD), drug use disorders (DUD). AUD and DUD were those that met criteria for abuse and/or dependence.
Suicidal behaviour
The 2007 NSMHWB suicide questions were adopted from the WMH-CIDI without modification. Participants were asked about suicidal behaviour in their lifetime and in the 12 months prior to interview. Suicidal behaviour includes: ideation (serious thoughts about committing suicide), plans and attempts. Lifetime and past 12-month suicidality were dichotomously coded with a code of ‘1’ representing a positive response to the relevant experience.
For the past 12-month risk factors, due to small numbers, correlates of past 12-month suicidal behaviours in people with chronic pain were again dichotomously coded, so that endorsement of one suicidal behaviour in the past 12 months was coded as ‘1’, representing at least one suicidal behaviour (thought, plan, or attempt) in the preceding 12 months. Whilst there may be concerns grouping these behaviours together, due to small numbers of the past 12-month suicide attempt, and that 60% of suicide attempts occur within a year of the onset of suicidal ideation (Nock et al., 2010), we believe that for the purposes of this exploratory study the grouping is deemed sufficient.
Physical health
A dichotomous variable was created from the global question ‘In general, would you say your health is excellent, very good, good, fair or poor?’, as those who endorsed poor or fair health, with excellent/very good/good as the reference category.
Data
Weights
Person weights and replicate weights were generated by the ABS and obtained from the CURF (Australian Bureau of Statistics, 2009b). Person weights were generated to reflect the characteristics of the total population in 2007 NSMHWB. Person weights were based on the following: first, to reflect the inverse probability of being selected for survey participation. Second, weights were calibrated to benchmarks for state, part of state, age and sex. In this case, benchmarks were based on the ABS Estimated Resident Population (ERP) for June 2007, which were projected from the 2006 Census of Population and Housing (Australian Bureau of Statistics, 2008). Third, calibration for household composition, educational attainment and labour force status was performed (Australian Bureau of Statistics, 2009a).
Replicate weights were produced using the delete-a-group jack-knife method (Australian Bureau of Statistics, 2009a; Rust and Rao, 1996). This involved division of the sample into 60 non-overlapping subsamples. Each was produced following the selection procedures used to create the full sample. One at a time each subsample is dropped and the procedures applied to produce the person weights are applied to the remaining sample. When applied in statistical analysis procedures, the replication approach produces estimates for the parameter of interest using each replicate weight. The variability among these estimates is used to estimate the sampling error for the whole sample estimate.
Data analysis
All analyses were based on weighted data, controlling for stratification and clustering, and were conducted using STATA, version 12.0 (StataCorp. 2011; College Station, TX: StataCorp LP). The application of the weights ensured the data were representative of the national population. In the descriptive analyses, statistical differences were assessed using odds ratios (ORs) and 95% confidence intervals (CIs). Owing to the overlap of pain conditions, a general ‘any pain’ category was used in some of the analyses. Logistic regressions were used to estimate the ORs for suicidal behaviours (i.e. thoughts, plan, attempt) while controlling sequentially for socio-demographic, mental health and chronic pain covariates. Covariates in the first set of regressions were: age, sex, married/de facto, completed school and employed (demographics). Covariates in the second model were: demographics and major depression, GAD, PTSD, AUD and DUD (mental health). Covariates in the third model were: demographics, mental health and the presence of one or more of the other pain conditions. Although the survey data have been weighted by age and sex, they have been included in the regressions due to their documented association with suicidality. The covariates and order in which they were added were determined by previous research on known factors for suicide. It was expected that mental health would account for the biggest risk.
A logistic regression was conducted to determine protective and risk factors of past 12-month suicidal behaviour in people with any chronic pain. Factors, such as social connectedness, have been found to be protective suicide risk factors and have been less focused on than suicide risk factors (Donald et al., 2006). All suicidal behaviour was grouped together due to the sequencing of the questions (i.e. had to experience thoughts to be asked about plans and attempts) and small numbers.
Results
Prevalence of chronic pain in the Australian population
Lifetime chronic (greater than 6 months) arthritis/rheumatism was reported by 15.6% of the sample, equating to 2.5 million people aged 16–85 years (Table 1). Lifetime chronic migraines were reported by 8.3%, which amounted to 1.3 million people in Australia. Lifetime chronic back/neck problems were reported by 28.0% of the sample, which equates to around 4.5 million people. Overall, more than 6 million people in Australia reported suffering from any of these chronic pain conditions, almost one-third of the Australian population.
Prevalence of chronic pain among Australian adults, 2007.
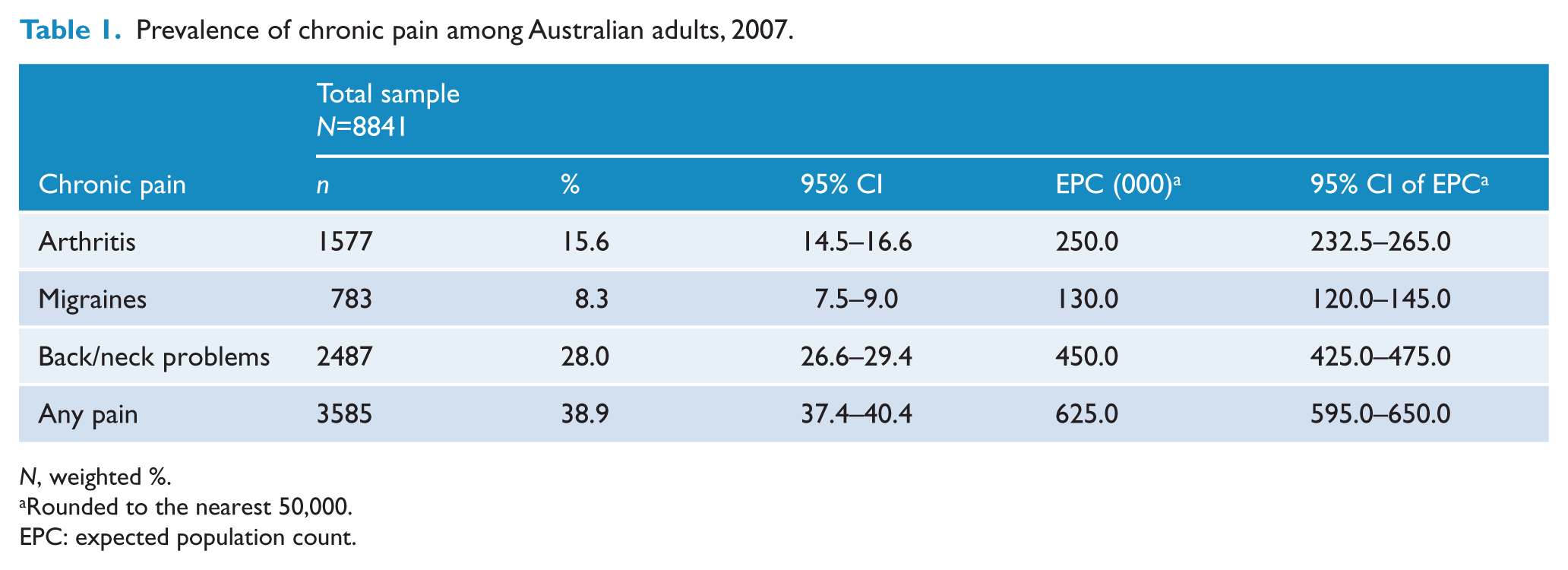
N, weighted %.
Rounded to the nearest 50,000.
EPC: expected population count.
There were high rates of comorbidity of chronic pain conditions. Just under two-fifths of those with back pain reported another chronic pain condition (arthritis and/or migraines). Approximately 50% of those with arthritis and three-fifths of those with migraines also reported suffering from another chronic pain condition.
Across the age groups, the 65 years and over age group had the highest levels of chronic pain (59%) – the most common pain condition being arthritis (see Appendix A). Half the 45–64-year-old age group reported experiencing pain, with the most common reported problem being back/neck problems. Just under one-third of the 25–44-year-old age group and one-sixth of the under 25 years age group reported the experience of ‘any pain’.
Socio-demographic and clinical characteristics of the sample
Owing to the comorbidity of pain conditions, the following bivariate analyses were conducted on the ‘any pain’ category (Table 2). People with chronic pain were more likely to be female and over 60 years of age, and less likely to have completed school, be employed or be married or in a de facto relationship. People with pain were also more likely to suffer from any lifetime or past 12-month mental health disorders (major depression, GAD and PTSD). Whilst those with chronic pain were more likely to meet criteria for a lifetime AUD compared with people without chronic pain, there were no differences for past 12-month AUDs. Conversely, people with chronic pain were more likely to have 12-month diagnoses of substance use disorder, but not lifetime, compared to those without chronic pain (Table 2).
Socio-demographic and clinical characteristics of people with and without chronic pain, NSMHWB, 2007.
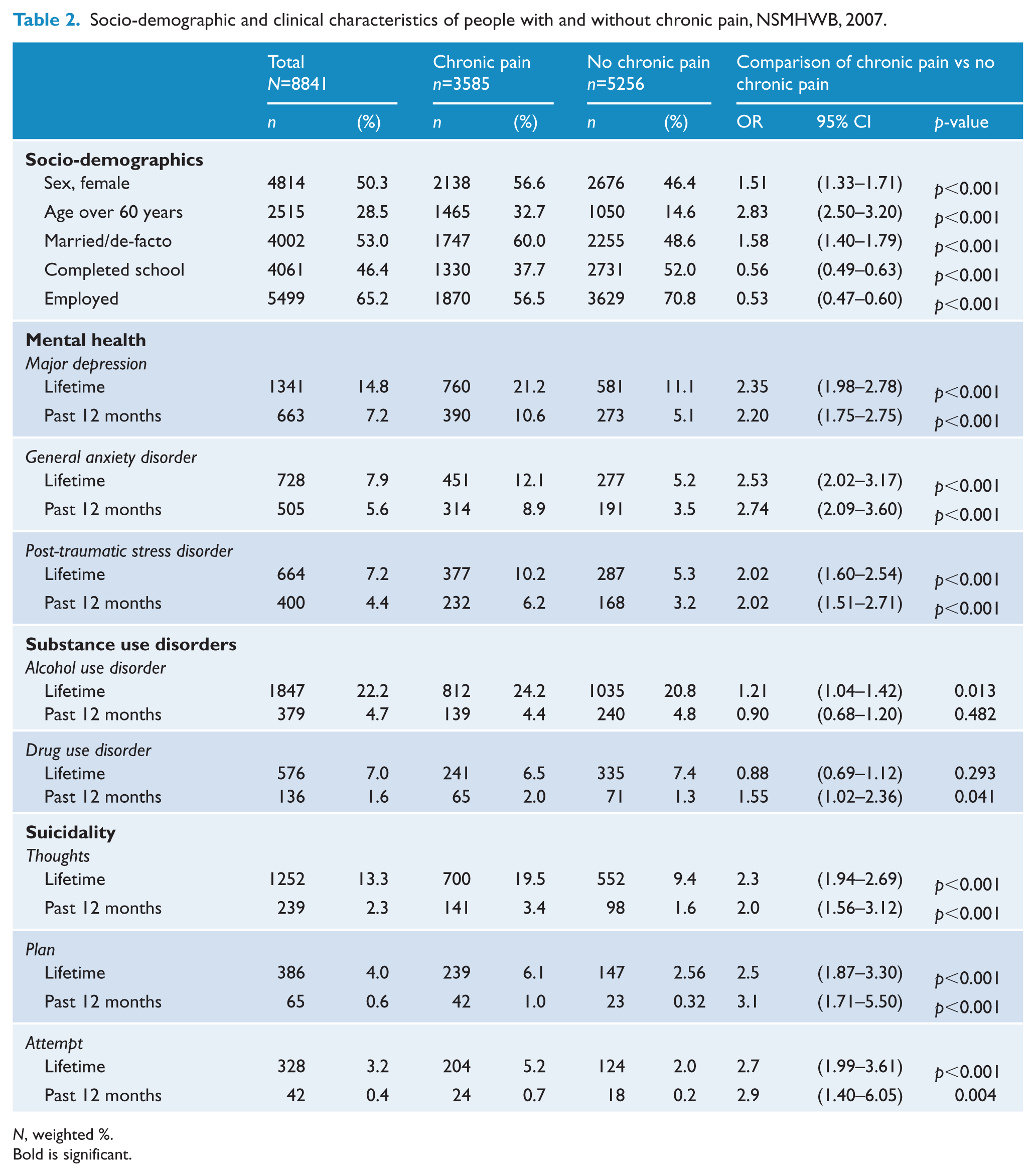
N, weighted %.
Bold is significant.
Chronic pain and suicidality in the Australian population
People with chronic pain had 2.3 times the odds of lifetime suicidal thoughts (Table 2), and 2.0 times the odds of reporting past 12-month suicidal thoughts, compared to people without chronic pain. People with chronic pain had 2.5 greater odds of having made a suicide plan at some point, and 3.1 greater odds of a past 12-month suicide plan, compared to those without pain. People with chronic pain had 2.7 times greater odds of making a lifetime suicide attempt, and a 2.9 greater odds of having made a suicide attempt in the past year, compared to people without pain.
Among those who engaged in suicidal thoughts or behaviours, people with a history of chronic pain made up the majority of the total (Table 3). Just over 50% of people with lifetime suicidal thoughts had a history of chronic pain; two-thirds (65%) of those who had attempted suicide in the previous 12 months had chronic pain, equating to approximately 42,000 people out of the estimated 64,000 who had attempted suicide nationally. The contribution of pain to overall suicidality by age groups can be seen in Appendix B.
Prevalence of chronic pain amongst people who had experienced lifetime and past 12-month suicidality.
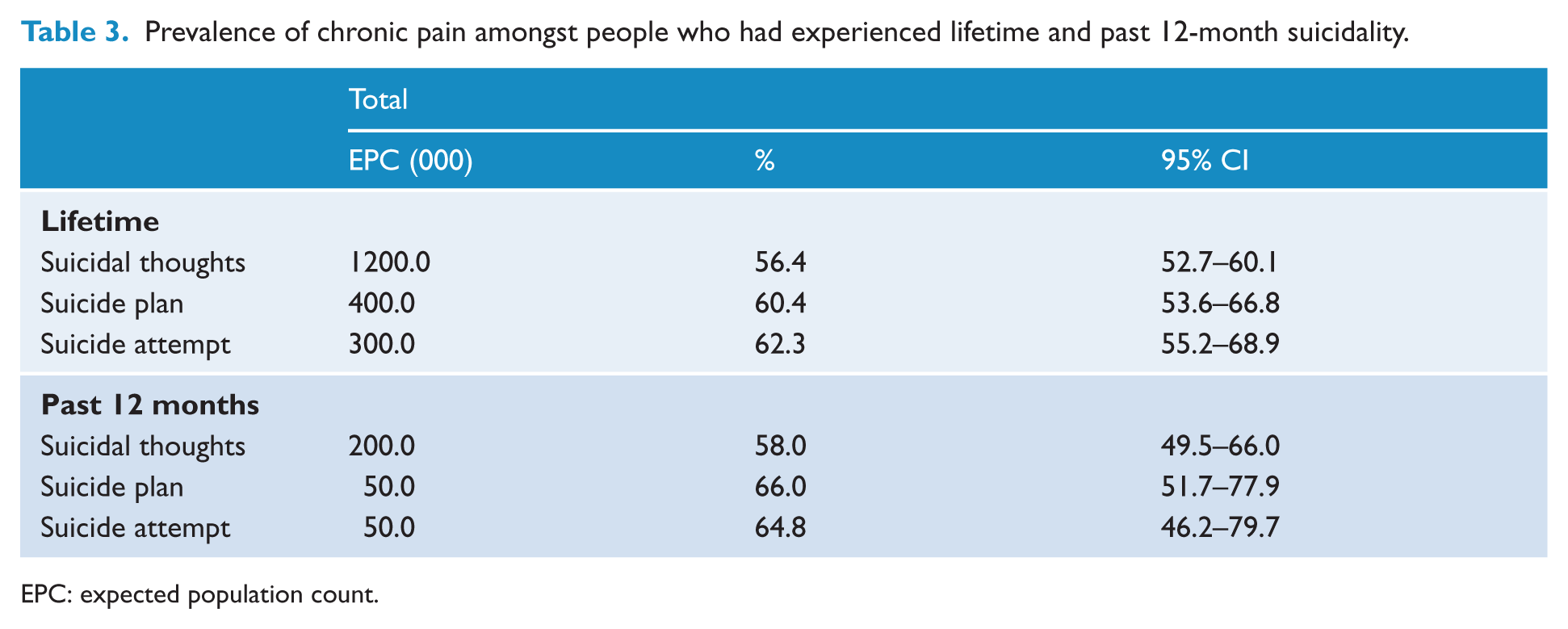
EPC: expected population count.
There was a difference between pain conditions and their contribution to suicidal thoughts or behaviours. Between 15.2% and 20.6% of people who had experienced lifetime and/or past 12-month suicidality had a history of migraines (Appendix C). Between 13.1% and 23.2% of people who had experienced lifetime and/or past 12-month suicidality had a history of arthritis. Between 45.3% and 54.3% of people who had experienced lifetime and/or past 12-month suicidality had a history of chronic back pain.
Chronic pain as an independent predictor of suicidality
In the unadjusted models and after adjusting for socio-demographic characteristics, all pain conditions and the ‘any pain’ condition were significantly associated with lifetime suicidality (Table 4).
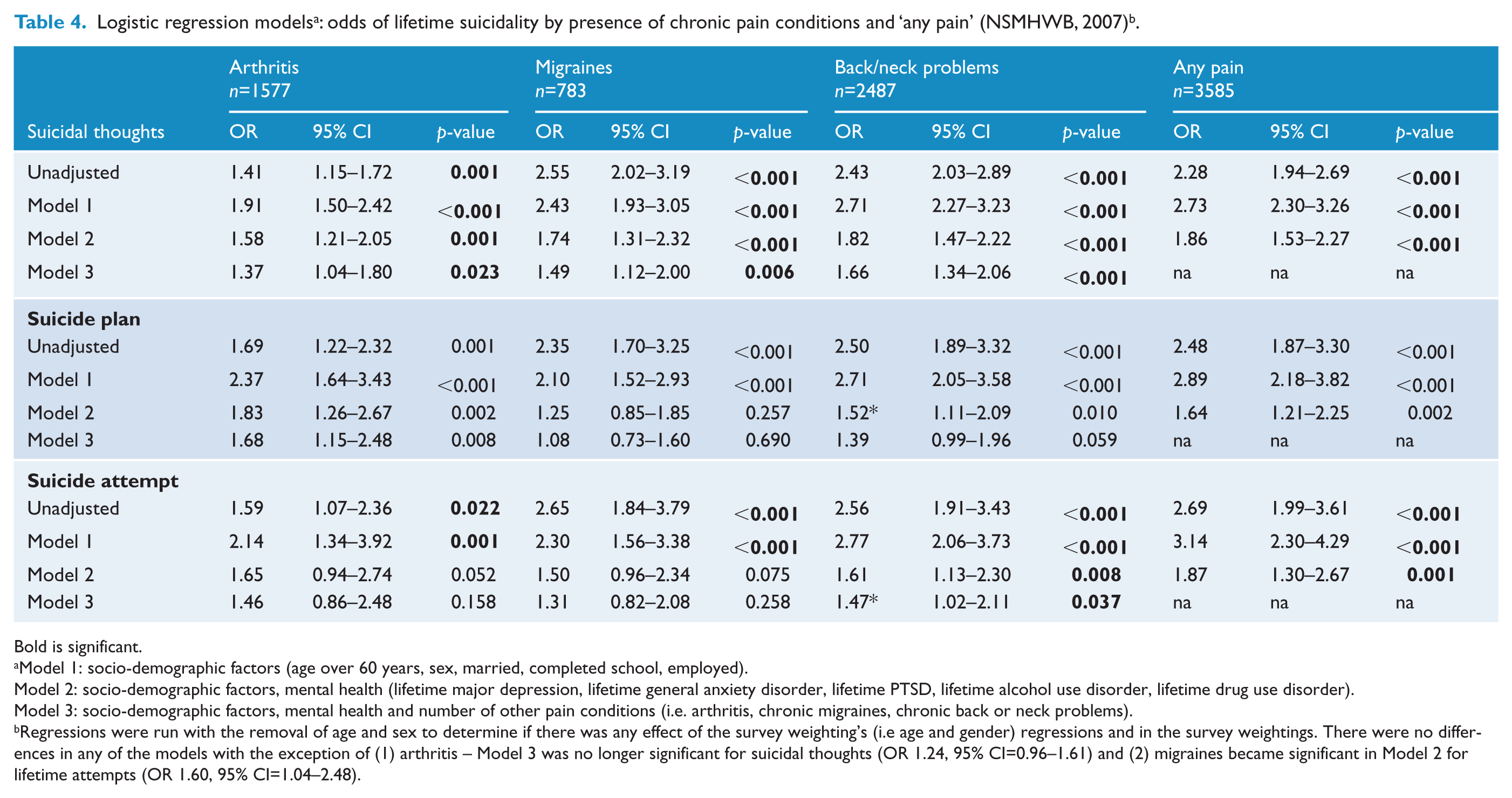
Bold is significant.
Model 1: socio-demographic factors (age over 60 years, sex, married, completed school, employed).
Model 2: socio-demographic factors, mental health (lifetime major depression, lifetime general anxiety disorder, lifetime PTSD, lifetime alcohol use disorder, lifetime drug use disorder).
Model 3: socio-demographic factors, mental health and number of other pain conditions (i.e. arthritis, chronic migraines, chronic back or neck problems).
Regressions were run with the removal of age and sex to determine if there was any effect of the survey weighting’s (i.e age and gender) regressions and in the survey weightings. There were no differences in any of the models with the exception of (1) arthritis – Model 3 was no longer significant for suicidal thoughts (OR 1.24, 95% CI=0.96–1.61) and (2) migraines became significant in Model 2 for lifetime attempts (OR 1.60, 95% CI=1.04–2.48).
After adjusting further for mental health disorders, the model, although reduced, remained significant for: suicidal thoughts for all the pain conditions and the ‘any pain’ category, suicide plan for arthritis, back/neck problems, and the ‘any pain’ category. After adjusting for socio-demographic and mental health, only back/neck problems and ‘any pain’ remained significant for lifetime suicide attempts.
After further adjusting for the number of other pain conditions, arthritis remained significantly associated with lifetime suicidal thoughts and plans. Migraines remained significantly associated with lifetime thoughts, but not lifetime suicidal plans or attempts. Back/neck problems remained significant after further adjusting for the other pain conditions for lifetime suicidal thoughts and attempts, but not lifetime suicidal plans.
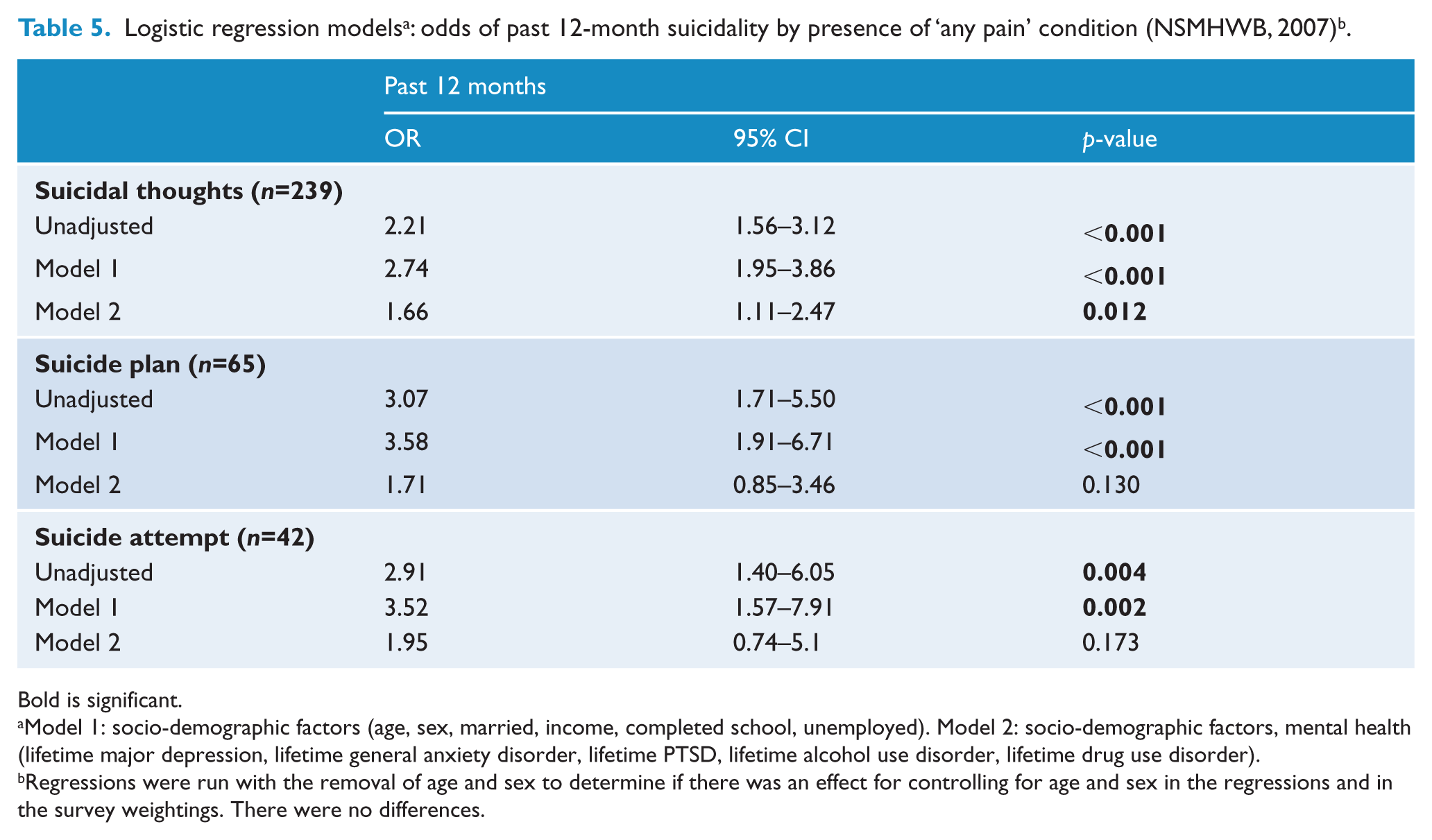
Owing to the small numbers, only the ‘any pain’ category was used in analyses of past 12-month suicidality (Table 5). In the unadjusted model and after controlling for socio-demographic factors, ‘any pain’ was significantly associated with past 12-month suicidal thoughts, plans and attempts. After further adjusting for mental health disorders, chronic pain remained significantly associated with suicidal thoughts (adjusted OR 1.66, 95% CI=1.11–2.47), although it was no longer associated with suicide plans or attempts.
Bold is significant.
Model 1: socio-demographic factors (age, sex, married, income, completed school, unemployed). Model 2: socio-demographic factors, mental health (lifetime major depression, lifetime general anxiety disorder, lifetime PTSD, lifetime alcohol use disorder, lifetime drug use disorder).
Regressions were run with the removal of age and sex to determine if there was an effect for controlling for age and sex in the regressions and in the survey weightings. There were no differences.
Risk factors associated with past 12-month suicidal behaviours in people with chronic pain
Figure 1 presents a logistic regression of the odds of suicidal behaviours amongst people with pain (data from the regression can be found in Appendix D). People who had chronic pain were more likely to experience past 12-month suicidal behaviours if they suffered from past 12-month major depression (OR 3.51, 95% CI=1.91–6.45), past 12-month GAD (OR 2.11, 95% CI=1.07–4.17), past 12-month PTSD (OR 2.52, 95% CI=1.36–4.67), past 12-month AUD (OR 2.53, 95% CI=1.13–5.63), or reported their physical health to be fair-to-poor (as opposed to good or very good; OR 2.57, 95% CI=1.54–4.20).
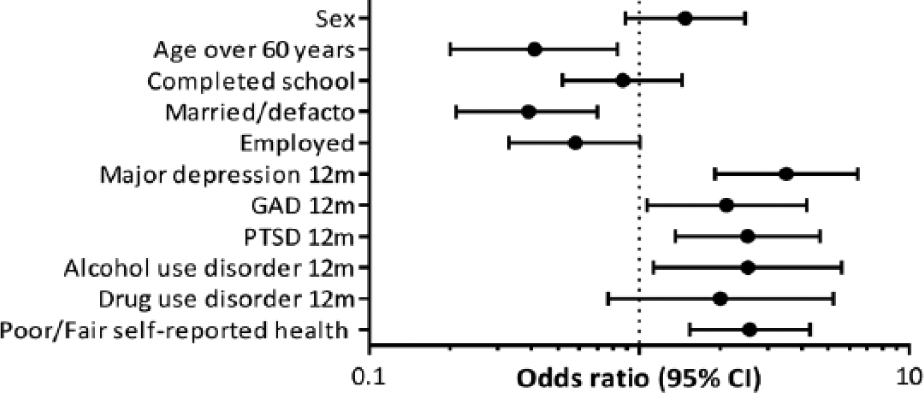
Odds of past 12-month suicidal behaviours amongst those with chronic pain.
People with pain were less likely to experience past 12-month suicidal behaviours if they were over 60 years old (OR 0.14, 95% CI=0.20–0.83) or they were married/de-facto (OR 0.39, 95% CI=0.12–0.70).
Discussion
Key findings
To our knowledge, this is the first population-based study that has estimated the proportion of people with suicide attempts who had chronic pain specifically: we estimate two out of three people who attempt suicide in Australia in a given year (65%) have a co-occurring chronic pain condition. People with a history of chronic pain contributed a substantial proportion of the total number of people who had engaged in lifetime and past 12-month suicidality. Approximately 58% of the people with suicidal thoughts in the previous 12 months had a history of chronic pain. While high-risk groups such as younger people, males, people with mental disorders, and gay, lesbian, bisexual and transgender people have generally been recognised as at-risk groups, there has been little discussion of the contribution that people with chronic pain may make to the population of those who experience suicidality (Senate Community Affairs References Committee, 2010; Suicide Prevention Australia, 2012). Our finding suggests that those with chronic pain are at high risk for suicide and a substantial proportion of people who engage in suicidal behaviours have a history of chronic pain.
To our knowledge, this is also the first Australian study that has compared the socio-demographics and clinical characteristics of those with chronic pain in a nationally representative survey. Consistent with previous literature (Blyth et al., 2001; Braden and Sullivan, 2008; Tang and Crane, 2006), chronic pain was found to be associated with a number of socio-demographics and clinical characteristics. People with chronic pain have a number of complex issues surrounding employment, physical health and mental health (Rogers et al., 2013), and with a heightened risk of suicide it is clear that a number of these issues need to be addressed when receiving treatment for their chronic pain. These results provide support to the complexity of chronic pain patients and the need for a multi-disciplinary approach to their care and treatment.
Consistent with the literature (Tang and Crane, 2006), lifetime and past 12-month suicidality were more common in those with chronic pain, with substantial variations across different pain conditions, whereby those with neck or back problems had by far the highest levels of suicidality. The current results, however, differed from the other epidemiological studies from Braden and Sullivan (2008), Ratcliffe et al., (2008) and Ilgen et al., (2008) with regards to specific pain conditions. Specifically, migraines in the current study were not associated with lifetime suicidality, after controlling for mental health and substance use. Pain conditions are highly comorbid, and it may be a limiting factor of general national surveys to determine the effect that specific pain conditions have on suicidality. More focused research in this area is essential to understand the relationship between specific pain conditions and suicidality.
The finding that chronic pain was independently associated with lifetime suicidality and past 12-month suicidal ideation, after controlling for mental health, raises important clinical implications. Whilst previous suicide research has identified the importance of mental health factors and their contribution to suicide, the finding of chronic pain as independently associated with suicide suggests the need for clinicians to be aware of this heightened risk in people presenting with chronic pain, irrespective of their mental health status (Cheatle, 2011). Further, patients that present with pain and mental health issues may be at a much heightened risk for active (plans and attempts) suicidality and should be assessed with appropriate referrals to mental health professionals made if necessary. Future research will be important in examining what specific pain-related factors, such as pain severity, pain coping, length of time in pain and pain conditions, are associated with suicide.
The prevalence of chronic pain in the current study was higher than previous estimates by Blyth et al., (2001) in the Australian population. Over one-third of the sample (38%) reported the experience of chronic pain compared to the previous estimates of 17% of males and 20% of females. An ageing population may explain some of this difference (the first estimates were made on data from 1997, compared to 2007 in the current study), though it is difficult to determine if this is an increase or differences in methodology. Despite these concerns, it is clear that chronic pain is common in Australia and is an area that requires future research and consideration.
Strengths and limitations
The strengths of this study are that it is population-based and provides detailed information on DSM-IV mental health problems and chronic conditions, but there are a number of limitations that need to be considered. First, it is not possible to determine whether the chronic pain and suicidality were directly related to each other. Whilst we are able to examine associations, the cross-sectional design of the survey does not allow us to determine causality. Furthermore, pain factors, such as length and severity, have been found to be factors associated with suicidality in chronic pain patients (Hassett et al., 2014; Tang and Crane, 2006); the current survey did not examine these factors. The numbers for past 12-month suicidal plans and attempts amongst people with chronic pain were relatively low (n=65 and n=42, respectively) and the current findings were not consistent with previous research that suggests an association between chronic pain and past 12-month plans and attempts after controlling for mental health (Ratcliffe et al., 2008). This finding needs to be interpreted with caution: it may be the lack of statistical power that led to a non-significant result. Despite these limitations, the findings of this study are important and suggest that more focused research on chronic pain patients may aid in the understanding of this relationship. Prospective longitudinal studies of pain, suicide and mental health will help our understanding of these associations and will be important clinically.
Conclusions
The current study found that chronic pain was a common complaint in the Australian population and a substantial proportion of people who engaged in suicidal behaviours had a history of chronic pain. Whilst previous research and treatments have focused on mental health and suicide, with an ageing population and the finding of chronic pain being independently associated with suicidality, it suggests clinicians need to be aware of this heightened risk in patients with chronic pain and, if necessary, provide referrals to appropriate mental health professionals.
Footnotes
Funding
This study received funding from the Australian National Health and Medical Research Council (NHMRC, #1022522). LD is supported by NHMRC research fellowships (#1045318). The National Drug and Alcohol Research Centre at the University of NSW is supported by funding from the Australian Government under the Substance Misuse Prevention and Service Improvements Grant Fund. The funder had no role in the design, conduct, analysis, interpretation or write-up of this manuscript.
Declaration of interest
LD has received untied educational grants from Reckitt Benckiser for the post-marketing surveillance of opioid substitution therapy medications in Australia, and the development of an opioid-related behaviour scale. LD, GC and RB have received untied educational grants from Mundi Pharma to conduct surveillance of the use of pharmaceutical opioids in Australia. All such studies’ design, conduct and interpretation of findings are the work of the investigators; the funders had no role in those studies.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.