
Abstract
Suicide is a global public health problem. An estimated 877000 people committed suicide in 2002 [1]. The annual suicide rate during the 1995–1999 period was approximately 23/100000 in China, with >287000 suicide-related deaths, making suicide the fifth most frequent cause of death [2]. Due to the lack of historical data and a comprehensive registration system, the clear trend of suicide in China is uncertain. Preliminary evidence, however, suggests that the pattern of suicide in China is unique in that it is characterized by a large discrepancy between rural and urban suicide rates (rural vs urban suicide rate: 3:1; [2, 3]), a high female: male ratio [2–6], and the frequent use of pesticides [6].
In Western settings suicide-related behaviours including suicidal ideations, plans and attempts have been found to be an important predictor of completed suicide [7–10]. Understanding the patterns and correlates of suicidal behaviour is essential for planning health-care policy to reduce suicide and suicide-related problems [9]. To date, however, only two studies on suicide-related behaviour have been conducted in China using epidemiological approaches. As part of a multicentre international survey on suicidal behaviour, Bertolote et al. investigated 503 rural dwellers in Yuncheng using the Chinese Version of the European Parasuicide Study Interview Schedule (EPSIS) [11]. Lifetime suicidal ideation, plans, and attempts were 18.5%, 7.4%, and 2.4%, respectively. The major limitations of that study included its small sample size, failure to examine the sociodemographic and psychiatric correlates of suicidal behaviour, and lack of involvement of urban residents. Lee et al. interviewed 5201 people in urban regions of Beijing and Shanghai using the Chinese version of the Composite International Diagnostic Interview (CIDI) and reported that lifetime suicidal ideation, plans, and attempts were 3.1%, 0.9%, and 1.0%, respectively [12]. But rural people, who accounted for around 75% of the Chinese population, were not targeted in that study, thereby limiting the generalizability of its findings.
In Beijing the average suicide rate for the 1987–1996 period was 9.8/100000 (6.0 and 17.3 for urban and rural areas of the capital, respectively [13]), which is significantly lower than the corresponding figure (23/100000) for the whole country [2]. This discrepancy indicates that there could be considerable differences in the rates of suicide across China.
The study reported herein set out to investigate the following: (i) lifetime prevalence of suicide-related behaviour in a population of subjects aged ≥15 years living in both the urban and rural areas of Beijing, China (Beijing municipality consists of 18 districts; the eight central districts constitute urban Beijing (Beijing city) and the remaining 10 peripheral districts form the rural part of Beijing; in China, including Beijing, residents are categorized as either urban or rural dwellers; this is recorded on their household cards kept by the local Public Security Bureau); (ii) sociodemographic correlates of suicide-related behaviour; and (iii) treatment preference of subjects with suicide-related behaviour.
Methods
Subjects and sampling
The study was undertaken in Beijing between 1 and 24 April 2003, as part of a large-scale epidemiological survey of the prevalence of psychiatric disorders. Details of the methods have been reported elsewhere [14]. Briefly, the study adopted a stratified, multistage systematic selection design based on Beijing's 2002 population census data. Participants who fulfilled the following criteria were recruited: (i) age ≥15 years; (ii) cohabitating with at least one other family member; (iii) permanent residency in Beijing; (iv) fluency in Mandarin and ability to comprehend the contents of the interview; and (v) willingness to participate in the study. The study protocol was approved by the Human Research and Ethics Committee of Beijing Anding Hospital. Written consent was obtained from participants or their family members for those who could not sign for themselves due to being illiterate or who were younger than 18 years of age as long as they verbally agreed to participate.
In China, neighbourhood and village communities in urban and rural regions, (NCs and VCs, respectively) are basic community organizations each with several hundred households. In the present study 6267 households were selected from the household registry from the 126 NCs/VCs of Beijing. Selection using a random number table took into account the population and the ratio of urban to rural residents in each of the 18 districts and counties in the municipality of Beijing. The person in each selected household aged >15 years whose date of birth was closest to 1 April was invited to participate in the study.
Assessment tools and procedures
Interviews were conducted at the participants’ homes. Sociodemographic and clinical data were collected using a questionnaire designed for the study. The scope of suicidal behaviour was defined according to the following questions: (i) suicidal ideation: have you ever felt so low that you thought of committing suicide; (ii) suicide plans: have you ever made a plan for committing suicide; (iii) suicide attempts: have you ever attempted suicide. An essentially identical definition of suicide-related behaviours has also been used in other recent studies [9, 12].
The Chinese version of the CIDI version 1.0 (CIDI 1.0) generates psychiatric diagnoses according to both the DSM-III-R and ICD-10. In the present study only DSM-III-R diagnoses were used to establish lifetime psychiatric disorders. Both the original CIDI and its validated Chinese version have satisfactory psychometric properties [15, 16].
The interviews were conducted face to face by 102 qualified psychiatrists who were selected from 18 mental health services in Beijing. The interviewers received training in epidemiological fieldwork in a 10 day workshop run by a trainer (Dr S.R. Li, Institute of Mental Health, Peking University) who had received training in using CIDI 1.0 in a course organized by the World Health Organization. The workshop included an overview of the project and covered the sampling and assessment procedures, techniques and potential difficulties of field interviews, mock interviews, and quality assessment.
Statistical analysis
Data were analysed using SPSS 13.0 for Windows (SPSS, Chicago, IL, USA). The sample was weighted according to the age and sex distribution of Beijing's population in 2002. First, stepwise logistic regression was used to calculate the crude and adjusted odds ratios (ORs) for sociodemographic and clinical factors including age, sex, marital and employment status, education level, monthly income, place of residence (urban vs rural), family history of suicide and major medical conditions as potential correlates of suicide-related behaviours as appropriate. Crude ORs examined the association between suicide-related behaviours and each of the sociodemographic and clinical factors separately on single logistic regression, while adjusted ORs were used to measure the relationship between suicide-related behaviours and each variable after controlling for the effects of other variables on multiple logistic regression. Second, the crude ORs examined the association between any type of suicide-related behaviours and major DSM-III-R psychiatric disorders using single and multiple logistic regression. The level of significance was set at 0.05 (two-tailed).
Results
A total of 6251 subjects were approached, of whom 5926 (94.8%) who met the study criteria agreed to participate. The sociodemographic data of participants are shown in Table 1. Table 2 presents the estimated lifetime prevalence rates of suicidal ideation, plans and attempts according to sex and age for the rural and urban regions. The overall lifetime prevalence of suicidal ideation, plans, and attempts was 2.3%, 1.4%, and 1.0%, respectively. As expected, suicide attempts occurred less often compared to suicidal ideation and plans in all age groups. Women consistently reported higher lifetime prevalence than men in all three aspects of suicide-related behaviour in both the rural and urban samples. Figure 1 presents the lifetime prevalence of suicidal ideation, suicide plans and attempts for the whole sample and separately for the rural and urban samples.
Percentage of subjects who had (––) suicidal ideation; (– – –) suicide plan; and (······) suicide attempt for (a) the total sample; (b) the rural sample; and (c) the urban sample.
Sociodemographic data of the participants (n=5926)
RMB, Renminbi; $US1=approx. RMB6.80.
Lifetime prevalence of suicide-related behaviours
CI, confidence interval.
Subjects who reported one or more forms of suicidal behaviour were asked whether they sought help from health service providers for their mental health problems. In the whole sample, only 36.2% of the subjects with a history of any suicide-related behaviour sought help from medical practitioners; the figures were 44.8% and 26.1% in the rural and urban samples, respectively. A mere 20.7% of the subjects in the whole sample with suicidal behaviour had visited mental health professionals, with the breakdown of prevalence rates being 30.5% and 9.1% in the rural and urban samples, respectively.
Table 3 summarizes the crude and adjusted ORs for the relationship between sociodemographic variables and suicide-related behaviour. Age ≥25 years, female sex, unmarried status, illiteracy, lower (<RMB500 month−1) or higher (>RMB2000 month−1) income and having a major medical condition were all associated with one or more types of suicide-related behaviour.
Sociodemographic correlates for suicide-related behaviours (logistic regression analysis)
CI, confidence interval; OR, odds ratio; RMB, Renminbi; $US1=approx. RMB6.80.
Only significant OR(s) and 95% CI(s), and variables entered in the final model are reported.
∗Significant at the 0.05 level, two-sided test.
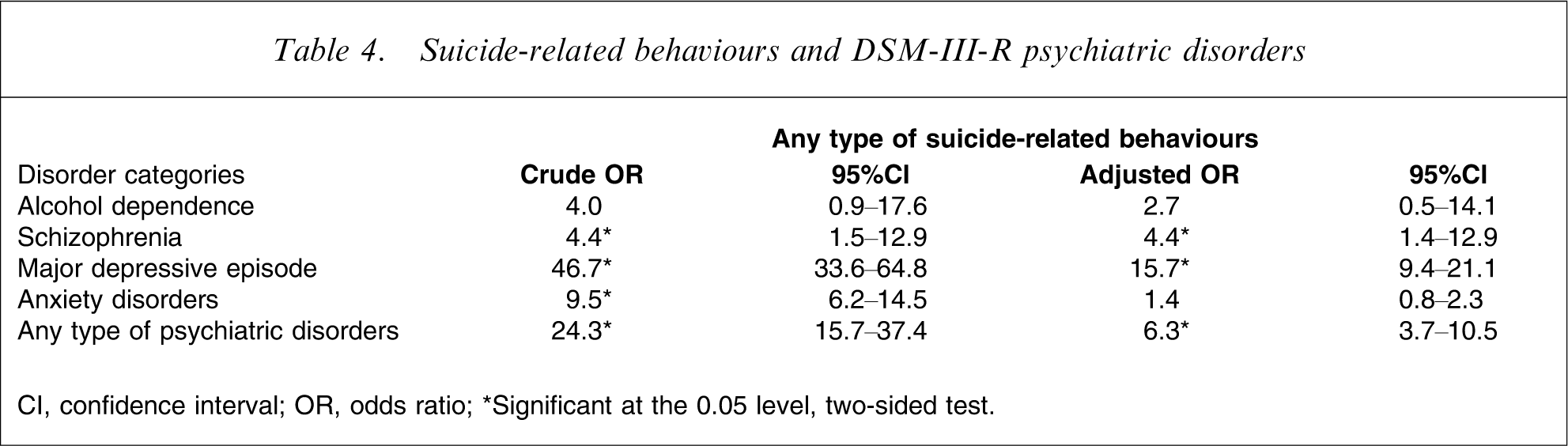
Table 4 presents the relationship of DSM-III-R mental disorder with suicide-related behaviours. On multivariate analysis, major depressive episode (MDE) was significantly associated with more frequent suicide-related behaviours (OR=15.7), followed by schizophrenia (OR=4.4).
Suicide-related behaviours and DSM-III-R psychiatric disorders
CI, confidence interval; OR, odds ratio
∗Significant at the 0.05 level, two-sided test.
Discussion
To the best of our knowledge this is the first epidemiological survey on suicide-related behaviour using standardized assessment in a large, random sample including both rural and urban regions in China.
Prevalence of suicidal behaviour
The prevalence estimates of suicide-related behaviour in the urban sample in the present study are compatible with the figures reported from China [12], while the prevalence rates in the rural sample were considerably lower than those found in the Bertolote et al. study [11]. The discrepancy between the two studies might be accounted for by the difference in the social and economic conditions of the two populations [17]. Due to rapid urbanization during the past decade, the rural region of Beijing is more affluent than the majority of rural areas in China, such as Yuncheng, the site of the Bertolote et al. [11] survey. Urbanization has been shown to decrease the risk of suicide in Chinese populations [5]. The lack of previous epidemiological surveys concurrently involving rural and urban samples in China hinders direct comparison.
The prevalence of suicide-related behaviour found in the present study is at the low end of the range reported from other cultures. In a large-scale epidemiological survey using the Diagnostic Interview Schedule that involved >40000 people across nine countries and regions, the lifetime prevalence of suicidal ideation ranged from 2.09% (Beirut) to 18.51% (Christchurch, New Zealand) and that of suicide attempts from 0.72% (Beirut) to 5.93% (Puerto Rico) [18]. In another multicentre study in eight countries using the EPSIS, the lifetime suicidal ideation ranged from 2.6% to 25.4%; the figures for suicidal plan and attempt ranged from 1.1% to 15.6% and 0.4% to 4.2%, respectively [11]. Beautrais et al. carried out a survey involving 12992 participants aged ≥16 years using face-to-face CIDI interviews in New Zealand and found that the lifetime prevalence of suicidal ideation, plan, and attempts was 15.7%, 5.5%, and 4.5%, respectively [19]. De Leo et al. conducted random telephone interviews of 11572 persons from the general public and estimated the lifetime prevalence of suicide plan and attempts to be 4.4% and 4.2%, respectively [10]. The considerable discrepancy between the low prevalence found in the study and earlier reports could be due to several reasons. The first involves the application of different methodology and criteria for suicide-related behaviour. Second, it is assumed that Chinese people are less willing than others to report suicide-related behaviour due to shame and fear of discrimination and stigmatization [12]. Third, there may be significant differences in the prevalence of suicide-related behaviour under different sociocultural circumstances. Fourth, prevalence rates may change over time [11].
Sociodemographic correlates of suicide-related behaviour
Unlike studies in Western settings [9, 19] and the urban regions of Beijing and Shanghai [12], the present survey found that young participants (aged 15–24 years) had a lower risk of suicide-related behaviour than other age groups. This is compatible with an earlier finding that the percentage of young people (aged 10–19 years) among all suicide completers in China was low (4%) [2]. We cannot offer an explanation for the low rate of suicide-related behaviour in young people, particularly the virtual absence of suicidal ideation in 15–24-year-old men. We hypothesize that the one-child policy in China, coupled with the preference for male offspring due to the perception that they are potential breadwinners and carers, may result in better upbringing and social support in this age group. It has been reported that the frequency of suicides among students has risen during the last years in Beijing [20, 21], casting doubt on the validity of this hypothesis. The relationship between age and suicide-related behaviour in Chinese populations needs to be further explored.
In line with a number of studies, the present study found that suicide-related behaviour was associated with female sex, unmarried status, low monthly income and low educational level [11, 12, 18, 19, 22–24].
A U-shaped relationship between monthly income and suicidal ideation and plans was observed in the present study: that is, participants both in the lowest (<RMB500 month−1) and highest (>RMB2000 month−1) income brackets had higher rates of suicidal ideation and plans. The increased risk of suicide-related behaviour for the high-income earners may be explained by the creation of permanent tension in the daily lives of these people due to excessive workloads and higher levels of responsibility [25].
Similar to the discrepancy between rates of completed suicide in rural and urban in China, we found that rural dwellers in the present study were more likely to have suicide-related behaviours, although the difference did not reach significance. A lack, however, of surveys of suicide-related behaviour concurrently involving rural and urban samples in both China and in Western settings makes any comparison between the present results and the literature difficult. The relatively poor living standards, educational opportunities, and access to health care, and the limited number of social support agencies operating in rural regions [2, 26] may all contribute to the higher likelihood of rural suicide-related behaviour.
It is of note that the ratio of estimated suicide rates in rural and urban regions reached 3.3 in China between 1995 and 1999 [2], and 2.9 in Beijing between 1987 and 1996 [13]. In the present study, however, the corresponding ratios of suicidal ideation, plans and attempts between rural and urban samples were only 1.6, 1.2, and 1.4, respectively. These figures are not as striking as the ratio of completed suicide. We speculate that the major reason for the relatively low rate of suicide-related behaviour in the present rural sample was selection bias; the rural area of Beijing is probably far more affluent than most of the rural regions in China [27]. Also, people living alone and migrants working in Beijing were excluded from the study. These two groups have probably more social and psychological hardship than the study participants, making them more prone to suicide-related behaviour [28]. The high suicide rate in rural China found in earlier studies [2] could be attributable to the high mortality rate of suicide attempts using lethal methods, such as the ingestion of pesticides or rat poison [2, 22, 26], compounded by the lack of well-trained local health professionals [2, 26].
Having a serious medical condition was significantly associated with suicide-related behaviour in China. The cost of medical care in China has been rising steeply over the past decades, and nowadays only a small proportion of people can afford optimal health care. We hypothesize that under these circumstances the fear of causing financial difficulty for the family or living with ill-health may lead to higher rates of suicide-related behaviour.
On multivariate analyses the significant association between suicide-related behaviour and educational level was eliminated after other sociodemographic and clinical variables were controlled. This result, however, should be treated with caution because the potential confounding influence of collinearity that exists between any two variables or between a variable and a combination of other variables cannot be ruled out. The role of education in suicide-related behaviour needs to be determined in future studies.
Seeking help from health professionals for suicide-related behaviour
In the present study only one-third of subjects acknowledging suicide-related behaviours sought help from medical practitioners following suicide-related behaviours during that period. The situation in the urban sample was even worse. These figures are considerably lower than results from New Zealand, where 55% of those with suicidal ideation and 55.3% with an attempt turned to a health professional for help [19]. The present result lends further support to the finding that a considerable proportion of people with suicide-related behaviour and related psychiatric disorders do not receive treatment or are poorly treated [19]. The low rate of help-seeking behaviour could be the consequence of several factors. First, many Chinese people consider suicide-related behaviour as a response to social stress rather than the result of a psychiatric illness. Therefore, they do not believe suicide-related behaviour is treatable primarily by mental health professionals [25]. Second, the still strong stigmatization and discrimination of psychiatric patients in China prevent those with suicide-related behaviour from visiting mental health clinics [29]. Third, there is still inadequate access to psychiatric services and a lack of available, effective treatment for suicide-related behaviour except for a few telephone hotlines in Beijing and some other parts of China. We have no explanation for the unexpected finding that more rural subjects with a history of suicide-related behaviour sought help from medical practitioners than did their urban counterparts. We can only speculate that rural people living with their families might have better social-support networks, which would have contributed to the relatively high rate of treatment seeking.
Psychiatric disorders and suicide-related behaviour
In the present study 8.9% of people with any psychiatric disorder reported suicidal ideation, 5.6% had a plan, and 4.7% made an attempt. The corresponding figures for those without a psychiatric disorder were 0.4%, 0.3%, and 0.1%, suggesting that a psychiatric disorder dramatically elevated the rates of suicide-related behaviour. MDE was the strongest correlate for suicide-related behaviour, followed by schizophrenia. These findings confirm the associations between psychiatric disorders, particularly depression, and suicide-related behaviours in the Chinese sociocultural context [12, 30].
Strengths and limitations of the study
The major strengths of the present study are its careful planning, sound methods, large sample and the involvement of clinicians as highly skilled interviewers. The findings should be interpreted, however, in the context of the following shortcomings. First, the study targeted only residents of Beijing, one of the most developed and affluent cities of the country. In Beijing, urban dwellers account for approximately 73.5% of the population, whereas the corresponding proportion is 36% in China. Thus, the results may not apply to other regions of China. Second, in the present study 126 NCs/VCs were randomly selected according to the size of the population and the ratio of urban to rural residents in each of the 18 districts and counties in Beijing. Due to rapid urbanization during recent years, however, the sharp distinction between rural and urban residency is often blurred: that is, officially designated rural residents move to urban areas while urban residents choose to live in rural areas. As a result, rural residents were overrepresented in the present study compared to Beijing's 2002 population census data (41.9% vs 26.5%). Third, people living alone were not included in the study. Involving a family member helped ensure easier access to the participants. This practice has often been used in mental health surveys in China [12]. It may have led to selection bias because people living alone might be more likely to be at higher risk of suicidal behaviour. Fourth, as a spin-off of a large epidemiological survey on psychiatric disorders, only three simple questions on suicide-related behaviour were asked. More severity quantification measures should be used in future studies. In addition, exploring the correlates of suicide-related behaviour was not a primary objective of the survey, and the correlates of suicide-related behaviours might thus be inadequate. Fifth, age was divided into too many categories, which might have influenced the power to reach the level of significance in multivariate analyses. This potential bias was unavoidable because the population was characterized according to these age categories in the Beijing population census, so the same age groups had to be used in the study. Finally, the study was cross-sectional and the causality of the relationship between suicide-related behaviour and sociodemographic variables could not be explored.
Conclusions
The present findings suggest that policymakers and health professionals in China should pay more attention to public education in order to improve the recognition and currently low treatment rate of suicide-related behaviour, allocate sufficient resources to implement strategies that identify high-risk populations, introduce effective interventions that target suicide-related behaviour and impulsive acts, and find more efficient ways of treating intoxication due to pesticides and other substances.
Footnotes
Acknowledgements
This study was supported by a grant from the Beijing Municipal Science and Technology Commission (No. H010910130112-200100528). The use of the Chinese version of CIDI 1.0, which was validated at the Institute of Mental Health, Beijing University, was authorized by the World Health Organization. The authors would like to thank all of the mental health professionals and participants involved in the project.