
Abstract
Objective:
Research has established the mental health sequelae following disaster, with studies now focused on understanding factors that mediate these outcomes. This study focused on anger, alcohol, subsequent life stressors and traumatic events as mediators in the development of mental health disorders following the 2009 Black Saturday Bushfires, Australia’s worst natural disaster in over 100 years.
Method:
This study examined data from 1017 (M = 404, F = 613) adult residents across 25 communities differentially affected by the fires and participating in the Beyond Bushfires research study. Data included measures of fire exposure, posttraumatic stress disorder, depression, alcohol abuse, anger and subsequent major life stressors and traumatic events. Structural equation modeling assessed the influence of factors mediating the effects of fire exposure on mental health outcomes.
Results:
Three mediation models were tested. The final model recorded excellent fit and observed a direct relationship between disaster exposure and mental health outcomes (b = .192, p < .001) and mediating relationships via Anger (b = .102, p < .001) and Major Life Stressors (b = .128, p < .001). Each gender was compared with multiple group analyses and while the mediation relationships were still significant for both genders, the direct relationship between exposure and outcome was no longer significant for men (p = .069), but remained significant (b = .234, p < .001) for women.
Conclusions:
Importantly, anger and major life stressors mediate the relationship between disaster exposure and development of mental health problems. The findings have significant implications for the assessment of anger post disaster, the provision of targeted anger-focused interventions and delivery of government and community assistance and support in addressing ongoing stressors in the post-disaster context to minimize subsequent mental health consequences.
Introduction
There is a large body of literature detailing the mental health sequelae of exposure to a natural disaster, with elevated rates of posttraumatic stress disorder (PTSD), depression, other anxiety disorders and substance use disorders most commonly reported (Acierno et al., 2007; Mason et al., 2010; Norris, 2006). Consistent with this literature, the mental health outcomes of Australia’s 2009 Black Saturday bushfires, the country’s worst natural disaster in over 100 years, have recently been published (Bryant et al., 2014). The Black Saturday bushfires affected over 100 communities and resulted in 173 fatalities, 3,500 buildings (including 2,133 houses) damaged or destroyed, and massive adverse impact on community infrastructures in regional and rural areas. In this study, Bryant et al. (2014) found significant elevations in rates of PTSD and Depression in the impacted communities, especially in the more heavily affected regions. However, while these elevated rates of mental disorder were reported, consistent with the extant literature (Bonanno, 2004) was that the majority of those who experienced the fires – more than 80% – recovered without developing significant mental health problems.
While a consistent picture is emerging of the mental health consequences of natural disaster, there is a growing body of research investigating factors that influence the development of mental disorders after these events (e.g. Acierno et al., 2007; Adams et al., 2006; Aksaray et al., 2006; Eksi et al., 2007; Papadatou et al., 2012; Van Loey et al., 2012). Along with characteristics of the traumatic event (such as threat to life, loss of a loved one), mental health outcomes are influenced by gender, subsequent negative life and traumatic life events, alcohol use, social support and the speed at which financial compensation was received. In the context of disaster, post-trauma stressors are particularly relevant because the post-disaster period can be fraught with further stressors, such as: rebuilding of family homes; adapting to changes in the community services and structures; displacement from communities, loss of personal items, loss of employment; the stress that often accompanies dealing with insurers and the recovery system; and these disaster-related stressors are associated with worse mental health outcomes (Galea et al., 2007).
There has been an emerging interest in the role of anger in trauma survivors. Anger has been found to feature prominently in military veterans, motor vehicle accident survivors, victims of crime, and relief workers after disaster and there are emerging indications that anger may be significantly implicated in the development and maintenance of PTSD in these populations (Evans et al., 2006; Foa et al., 1995; Jakupcak et al., 2007; Mayou et al., 2002; McFall et al., 1999; Novaco and Chemtob, 2002). While alcohol use disorders are also an outcome of trauma exposure in their own right, interactions between anger and alcohol abuse have been found to further negatively influence recovery and treatment responsivity for trauma affected military veterans (Forbes et al., 2008). Current hypotheses regarding the impact of anger on development and maintenance of PTSD include its function as a mobilizing emotion in impeding the processing of more vulnerable emotions such as fear, anxiety and loss (Foa et al., 1995; Forbes et al., 2005).
In the aftermath of a disaster, even natural disasters, anger features prominently at both the individual and community level (Evans et al., 2006; Jayasinghe et al., 2008; Rubin et al., 2012). There is commonly anger at the perceived deficiencies in the acts of the relevant authorities who are seen as having failed in their duty to provide sufficient protection, or indeed anger between community members on various dimensions such as levels of preparation and assistance (Solomon and Thompson, 1995). Commonly, anger increases over time with dissatisfaction at the authorities responsible for recovery programs and insurance claims processing, which leads to the experience of additional stressors post the natural disaster. Friction can arise within the community as to the best allocation of limited resources towards the tasks of recovery, which erodes the protectiveness afforded by strong social support networks (Honeycutt et al., 2008).
While anger, alcohol use, ongoing life stressors and subsequent trauma have been examined as potential factors influencing mental health outcomes, these factors as yet have not been examined simultaneously with emotional and behavioral response factors of anger and alcohol use. It is possible that one of these factors may act as a proxy for the other, for example, ongoing stressors confer a risk only to the extent that they generate anger, or alternatively, anger confers a risk as an indicator of ongoing life stressors and subsequent trauma. Therefore this study examined the influence of anger, alcohol, ongoing life stressors and subsequent trauma on mediating the relationship between exposure to the Black Saturday bushfires and the subsequent development of mental health disorder. Norris (2006) argued that to better understand these issues advanced forms of regression modeling, such as structural equation modeling, are best suited. In this study a mediation model path analysis was utilized as a specific form of a structural equation modeling to identify which, if any, additional factors mediate the relationship between the disaster exposure and mental health outcomes.
Method
Participants
This study involved 1017 (Male = 404, Female = 613) adult residents (mean age 53.1 years) sampled across 25 communities in 10 locations in rural and regional Victoria as part of the Beyond Bushfires: Community Resilience and Recovery study (Gibbs et al., 2013; www.beyondbushfires.org.au). Contact details of both current resident and relocated persons since the fires (N = 7,693 adults) were obtained from the Victorian Electoral Commission (VEC). Compared with available census data, the participants in this study were disproportionately older, female, and more educated than the general community. One personalized letter of invitation was approved by the VEC to be sent to the adults in this sample. Furthermore, community awareness activities, area-based phone calls, mailbox drops, news media and social media activities were also conducted to increase awareness of the study and methods for registration.
Measures
Region: this was defined as high-impact (operationalized as many houses lost plus fatalities; n = 630), medium-impact (operationalized as upper end of range, may include small number of fatalities through to communities with no fatalities but significant amount of property damage; n = 182), and low-impact (operationalized as no evidence of burning; n = 205).
Loss of property: this was measured in a self-report question ‘Extent to which respondent lost personal or business property/possessions’. Scored from ‘0’ (Nothing) to ‘10’ (Everything).
Loss of a loved one: this was measured in a self-report question ‘Whether someone close died as a result of the Feb 2009 fires’. Scored as ‘No’; ‘Yes’; ‘Don’t Know’, or ‘Prefer not to answer’.
Fear for life: this was measured in a self-report question ‘Did you fear for your life?’. Scored as ‘No’; ‘Yes’; ‘Don’t Know’, or ‘Prefer not to answer’.
Posttraumatic Stress Disorder Checklist – Screen (PCL): This 4-item version of the PCL (Bliese et al., 2008) comprises four items each scored on a 5-point Likert scale that indexes key symptoms of PTSD and refers to the previous four weeks. The PCL Screen was altered to ask whether the symptom being endorsed was in response to reminders of the Black Saturday fires (PCL Fire-related), or in response to reminders of traumatic events generally (PCL General).
Depression symptoms were assessed using the Patient Health Questionnaire (PHQ-9: Kroenke et al., 2001), which comprises nine items that are scored on a 4-point Likert scale.
Alcohol Use was measured with the 3-item self-report Consumption Scale of the Alcohol Use Disorder Identification Test (AUDIT-C: Bush et al., 1998). This scale is an abbreviated version of the AUDIT, the most commonly used measure of alcohol abuse. The AUDIT-C employs the initial three questions of the AUDIT, which measures the amount of alcohol consumption but not adverse effects of alcohol use.
Major Life Stressors: participants were questioned as to whether they had experienced a major life stressor since the fires in the form of disruptions to their (a) occupation, (b) accommodation, or (c) personal relationships.
Post-Fire Traumatic Events: participants were asked to indicate whether subsequent to the fires they had been exposed to any of the following potentially traumatic events: (a) natural disaster, (b) serious accident, and (c) assault or violence.
Anger: participants answered the two screening questions from the Anger Attacks Questionnaire (AAQ: Arciniegas et al., 2005).
Procedure
The study was approved by the University of Melbourne Human Research Ethics Committee. Baseline data collection was piloted in late 2011 then conducted between April 2012 and January 2013. Relevant to the current analyses, the interview administered the AAQ, AUDIT-C, PS-PTSD, PHQ, and questions about aspects of the fire, major life stressors and post-fire traumatic events.
Statistical analyses
In the analyses we sought to define the best model that could explain the direct relationship between exposure to bushfires and mental health outcomes, while accounting for any indirect relationship through an additional mediating variable. To complete this analysis we identified two latent variables and four observed variables that were of interest. Observed variables are directly measured, while latent variables are calculated from multiple observed variables. The observed variables were Anger, Major Life Stressors, Post-Fire Traumatic Events and Alcohol Use. Exposure to bushfires and mental health outcomes were constructed as latent variables. ‘Exposure to Bushfires’ was calculated using four measures: i) extent of property loss, ii) geographical region, iii) fear for life, and iv) loss of loved one. ‘Mental Health Outcomes’ was calculated using three measures: PCL (Fire-related), PCL (Non fire-related) and Depression. Each latent variable will be initially tested with a confirmatory factor analysis.
Structural equation modeling (SEM) with Mplus version 7.01 (Muthén and Muthén, 1998–2011) was employed to examine the strength of the relationships between the variables of interest. Mplus permits simultaneous calculations of multiple direct and indirect relationships. In the model an arrow between variables denotes the relationship examined, with the head of the arrow representing the variable that is regressed on the variable located at the tail of an arrow (see Figure 1). When the path between two variables includes more than one arrow this represents an indirect relationship, with the middle variable being a mediator between the two variables located at either end of the path. The regression coefficient (β) measures the strength of a relationship between variables, with a higher standardized value signifying a stronger relationship.
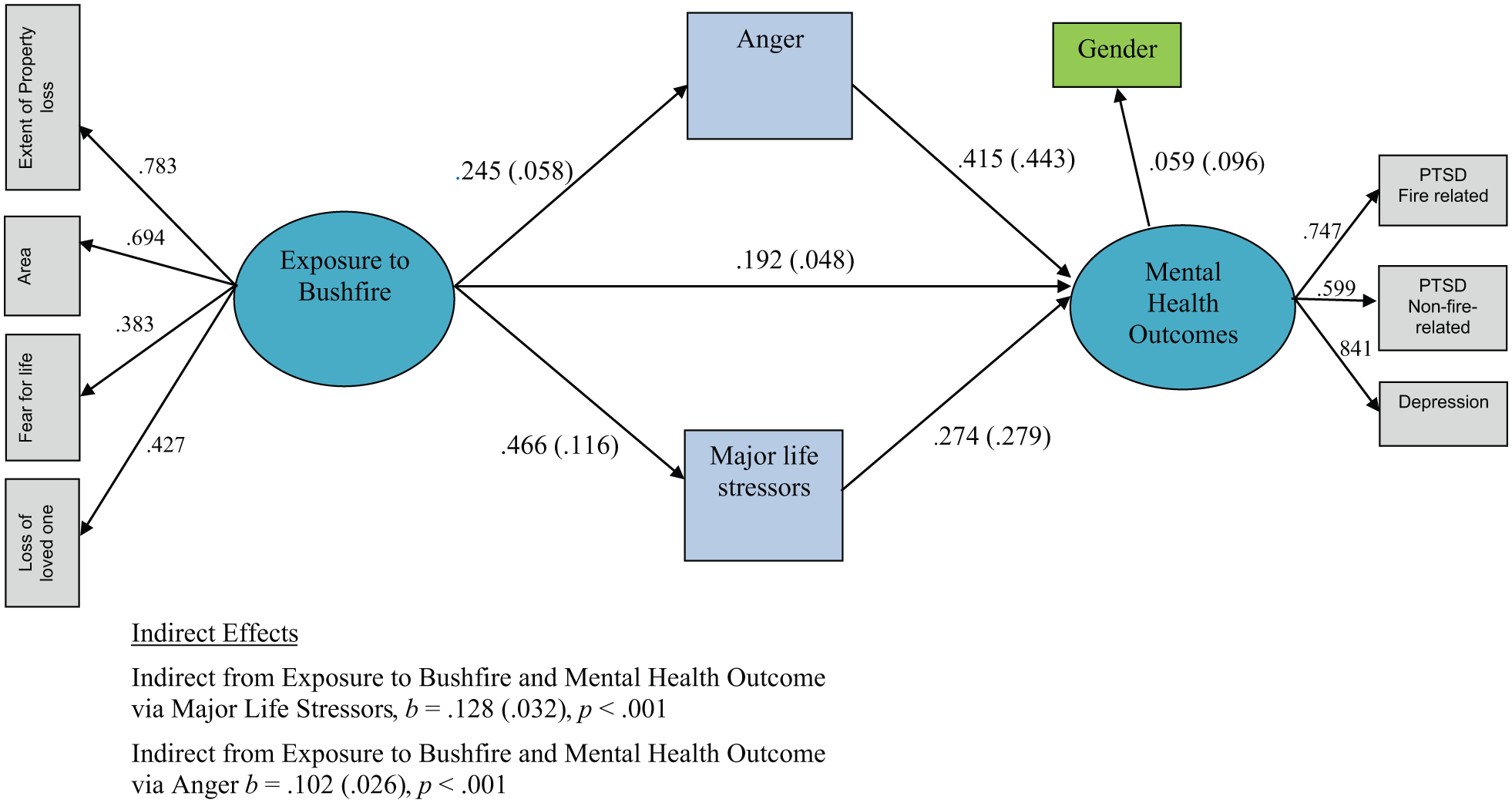
Mediation model for risk factors Anger and Major Life Stressors occurring between Exposure to Bushfires and Mental Health Outcomes.
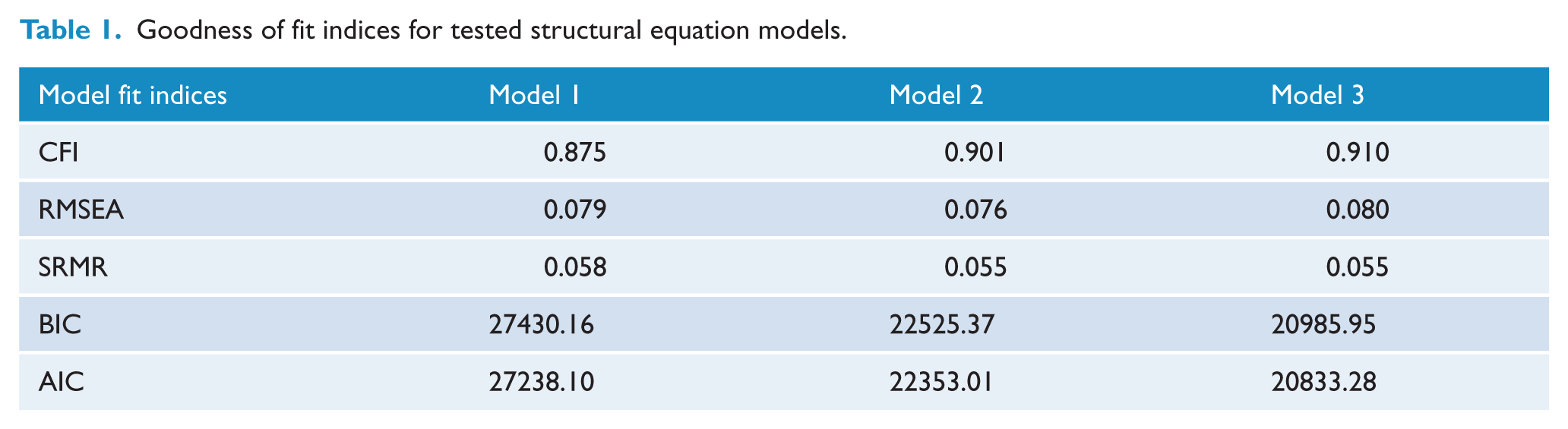
Before interpreting direct and indirect relationships in a SEM it is sensible to determine that the model defined adequately represents the data by appraising multiple fit indices (Brown, 2006; Vandenberg and Lance, 2000). To assess model fit, we reviewed the Comparative Fit Index (CFI: Bentler, 1990); the Root-Mean-Square-Error-Approximation (RMSEA: Steiger, 1989); and the Standardized Root Mean Square Residual (SRMR: Joreskog and Sorbom, 1981). If the CFI levels fall below .90 then the model will be rejected (Hu and Bentler, 1999). A RMSEA value near .06 and a SRMR near .08 supports the model as fitting the data well (Hu and Bentler, 1998).
Initially a model will be defined with Anger, Major Life Stressors, Post-Fire Traumatic Events and Alcohol use as mediator between ‘Exposure to Bushfires’ and ‘Mental Health Outcomes’. Gender was included as a controlling variable on ‘Mental Health Outcomes’ to allow for the accepted gender differences in prevalence rates for psychiatric disorders. A decision about whether to amend the model will be made based on the overall model fit, and the significance of individual regression coefficients of the specified model. Models will be compared against the same fit indices described earlier along with the Bayesian Information Criterion (BIC), and the Akaike’s Information Criterion (AIC).
Results
Participant characteristics
Almost one-third of the sample suffered the loss of another person from the bushfires and 49% feared for their life. More than two thirds of the sample suffered loss of property from the bushfires. Subsequent to the bushfires one-quarter of the sample have endured another traumatic event and over 50% of the sample reported experiencing one or more major life stressful event (for detailed information about the development of psychiatric disorders, see Bryant et al., 2014).
Model definition
Confirmatory factor analyses indicated that the ‘Exposure to Bushfires’ and ‘Mental Health Outcomes’ both were clearly represented as a single factor (both observed CFI = 1.00 and TLI = 1.00). Similarly the mental health outcomes loaded as a single factor supporting their representations as single latent factors of ‘Exposure to Bushfires’ and ‘Mental Health Outcomes’ in the model.
Table 1 shows the fit indices for three models tested. Model one was rejected because the CFI was below the threshold defined for a well-fitting model (.900). A review of the output found that Alcohol Use was a non-significant predictor (p = .811) of mental health outcomes. Model two removed this relationship and met the criteria of a well-fitting model. However, the low β (= .002) and borderline significant (p = .05) indirect relationship via the Post-Fire traumatic events as a mediator was of concern. To test whether this variable should be retained we retested the SEM under model three with Post-Fire traumatic events removed. The substantial decrease in the AIC and BIC values under the more parsimonious model three strongly supported the selection of this as the preferred SEM (see Figure 1). This procedure was repeated with the outcome variables defined as observed variables separately (fire PTSD, non-fire PTSD and depression) rather than a latent variable and the results were unchanged, including a still marginal contribution of Post-Fire traumatic events on non-fire PTSD (β = .001, p = .07). Further information is available from the authors upon request.
Goodness of fit indices for tested structural equation models.
As shown in Figure 1, ‘Exposure to Bushfire’ had a significant direct relationship with ‘Mental Health Outcomes’, and importantly there were significant indirect effects via Anger and Major Life Stressors. These indirect effects suggest that both the levels of anger and experience of highly stressful life events contributed independently to the mental health difficulties above and beyond the factors associated with the Bushfire event. The inclusion of gender as a controlling variable on the mental health outcomes in the model strengthens the results by removing any potential confound from a gender imbalanced sample. An interaction variable combining anger and major life stressors was computed and tested, however it did not significantly contribute to outcomes beyond the independent contributions of the two predictor variables separately (β = .000, p = .29).
Gender effects
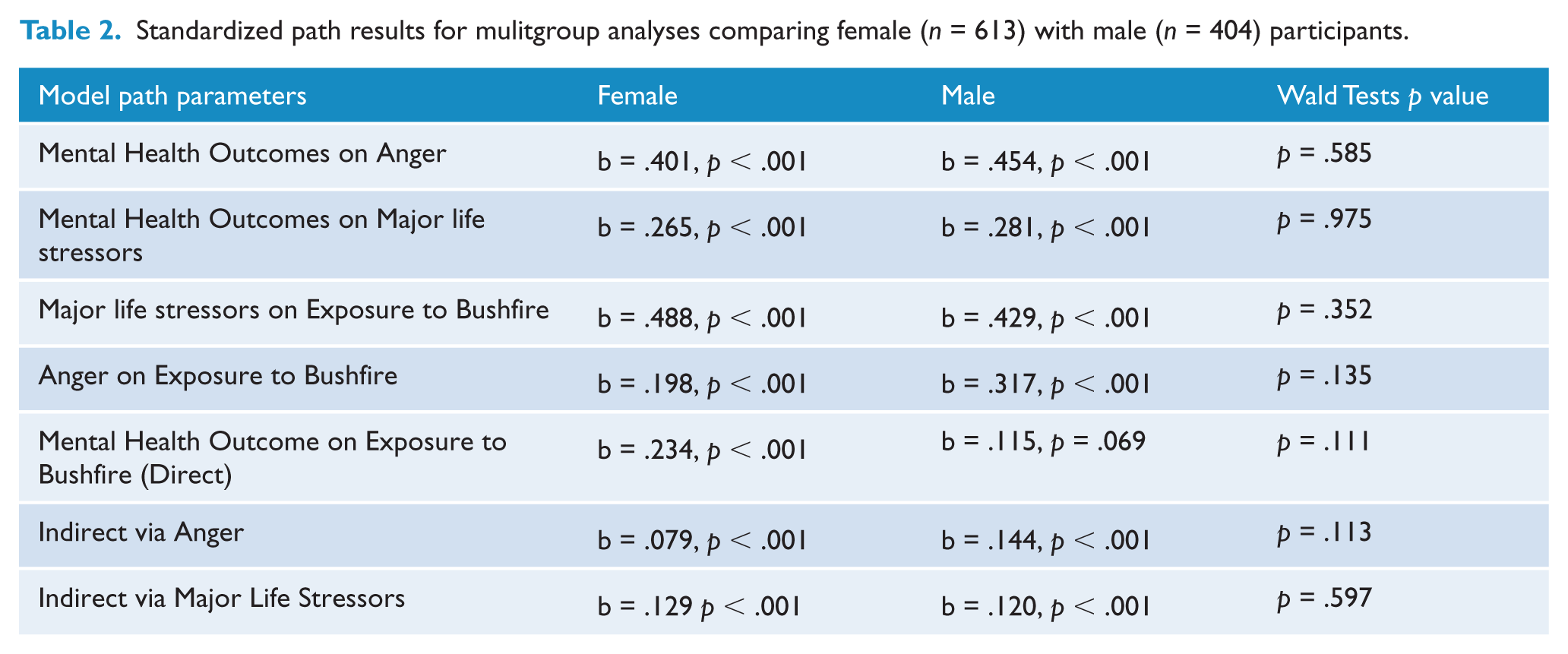
Given the literature on the influence of gender, it was included in the model as a control variable and consistent with the literature was significantly associated with outcomes (see Figure 1). To further assess any difference across gender on the model defined, we ran a multigroup analyses using gender as a grouping variable (females n = 613 and males n = 404). Table 2 shows the results were similar in the analyses with females and males with one notable exception. In the male group the direct relationship between ‘Exposure to Bushfire’ and ‘Mental Health Outcomes’ was non-significant, whereas the same path between ‘Exposure to Bushfire’ and ‘Mental Health Outcomes’ was significant for females. Interestingly the indirect paths via Anger and Major Life Stressors remained significant in both the male and female groups. Wald chi-square tests were run to compare the beta coefficients for equality between the male and female groups. Table 2 shows that none of the parameters were significantly different between male and females.
Standardized path results for mulitgroup analyses comparing female (n = 613) with male (n = 404) participants.
Discussion
This study examined the roles of anger, alcohol use, subsequent major life stressors and traumatic events in mediating the relationship between exposure to a major natural disaster and mental health outcomes. Of these factors, anger and major life stressors were confirmed as the most substantial mediators, each contributing independently in the final structural model. A combined variable consisting of an interaction between major life stressors and anger, reflecting anger in the context of stressors, did not offer a significant further contribution to the model. The contribution of the subsequent trauma variable to the model did reach marginal statistical significance, relating to the manifest outcome variable of non fire-related PTSD, however even this contribution was relatively weak compared with anger and major life stressors and the model improved significantly upon its removal. It is important to note that subsequent trauma was significantly related to mental health outcome as would be expected, but this relationship alone was insufficient to produce a mediation relationship between the exposure variable and mental health outcomes.
The post-disaster context is frequently characterized by significant stressors such as relocation, rebuilding, loss of community structures and functions and often loss of income (Kessler et al., 2008). Prior research has attested to the impact of ongoing stressors on posttraumatic mental health across a range of traumatic situations (King et al., 1998). The major novel finding of this study was that anger contributed significantly to mental health outcomes. The experience of anger is commonly reported at the individual and community level in relation to managing posttraumatic stressors, including confronting the losses sustained in the trauma, perceptions of responsibility for inadequate protection from or assistance following the traumatic event, and perceived unfairness of the impacts of the event (Kessler et al., 2008).
The finding that anger and ongoing stressors did not interactively contribute to mental health outcomes beyond their independent effects is interesting. It is common for anger to be observed following disasters as a result of ongoing stressors, including rebuilding delays, problems with insurance claims, community priorities, and other persistent difficulties, for example, the recovery process (Kessler et al., 2008; Norris et al., 2002). Accordingly, it would be reasonable to expect that anger and ongoing stressors may together contribute to the level of distress one is experiencing after disaster. The absence of this pattern possibly suggests that the effect of anger on mental health outcome may emanate more from characterological factors, including personality and appraisal style, rather than uniformly resulting from the effects of stressors after the disaster. Further research which defines the characterological factors that increase the risk for developing mental health problems would be valuable.
Interestingly, this study found that while anger and ongoing stressors were significant mediators for males and females, in males these factors fully mediated the relationship between exposure to the fires and outcomes. That is, in males, anger and the experience of ongoing stressors fully accounted for the relationship between the exposure and losses associated with the fires and subsequent mental health, whereas in females, while both these factors influenced mental health, the impact of the fires themselves still considerably influenced outcomes. Despite these findings, the gender differences did not reach significance when compared directly. These findings however do raise some questions about possible gender differences in emotional processing following trauma and require further investigation. It is consistent with findings of treatment studies for PTSD where baseline anger appears to significantly impede treatment outcomes in studies of male trauma survivors, but not in studies examining outcomes of treatment in women (Lloyd et al., 2014). Anger is a mobilizing emotion and can impede activation or facilitate avoidance of emotions associated with fear, vulnerability and loss (McHugh et al., 2012). This may account for its negative influence on mental health outcomes for men and women. That anger and major life stressors fully accounted for the relationship between exposure and outcome in men may indicate that for men anger has a primary role in the emotional experience of the traumatic event itself rather than a secondary emotion. The failure of alcohol to influence mental health outcomes is interesting. One reason for the failure to find an effect may relate to the elevated rates of alcohol use across the fire and non-fire affected communities, thereby resulting in a ceiling effect (Bryant et al., 2014).
The findings of this study have implications for post-disaster support. First, it is important that measurement of anger is routinely included in screening and assessment methods for high-risk survivors of trauma, along with measures of common mental disorders. Second, practitioners delivering care for disaster survivors need to be skilled in the delivery of evidence-based interventions targeted on anger (Deffenbacher, 2011; Novaco et al., 2012) and consider the application of these for trauma survivors (Forbes et al., 2013). Finally, government and community investment in support and assistance to prevent or minimize the subsequent post-disaster stressors has the potential to significantly reduce the subsequent psychiatric burden following the disaster and facilitate recovery. It is important that communities are provided support to develop ongoing capabilities to manage the mental health difficulties that can develop, rather than short-term external assistance designed primarily to meet an immediate need (Greenhill et al., 2009).
This study also includes a number of limitations. In the context of a large broad-based community survey it is inevitable that in order to minimize response burden that brief measures of constructs be used where possible. In this case it needs to be acknowledged that brief although well-validated screen versions of measures of PTSD, depression, anger and alcohol were used, rather than the full versions of these measures that may have added measurement strength. In addition, self-report measures rather than structured clinical interviews were used to measure response. These limitations notwithstanding, these findings have significant implications for the assessment of anger post disaster and the provision of targeted anger-focused interventions and delivery of government and community support and assistance to address ongoing stressors in the post-disaster context to minimize subsequent mental health consequences.
Footnotes
Funding
This project was supported by an ARC Linkage Grant (LP100200164).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.