
Abstract
Objective:
The aim of this study is to evaluate the impact of the Canterbury earthquakes on the mental health of the local population by examining prescribing patterns of psychotropic medication.
Method:
Dispensing data from community pharmacies for antidepressants, antipsychotics, anxiolytics and sedatives/hypnotics are routinely recorded in a national database. The close relationship between prescribing and dispensing provides the opportunity to assess prescribing trends for Canterbury compared to national data and therefore examines the longitudinal impact of the earthquakes on prescribing patterns.
Results:
Short-term increases in the use of anxiolytics and sedatives/hypnotics were observed after the most devastating February 2011 earthquake, but this effect was not sustained. There were no observable effects of the earthquakes on antidepressant or antipsychotic dispensing.
Conclusion:
Short-term increases in dispensing were only observed for the classes of anxiolytics and sedatives/hypnotics. No sustained changes in dispensing occurred. These findings suggest that long-term detrimental effects on the mental health of the Canterbury population were either not present or have not resulted in increased prescribing of psychotropic medication.
Introduction
This paper examines the impact of the series of Canterbury earthquakes on local psychotropic medicine prescribing. The earthquakes started with a 7.1 magnitude earthquake on 4 September 2010 and continued for more than 2 years with further major earthquakes in February, June and December 2011 and over 10,000 aftershocks. The February 2011 earthquake was the most devastating. It resulted in significant loss of life and multiple injuries (182 people died and 6659 were injured in the initial 24 hours) and widespread damage to property and infrastructure (Ardagh et al., 2012). In addition to the acute trauma, there have also been persistent effects on the population over a lengthy period because of repeated aftershocks, infrastructure damage, insurance disputes and delays in rebuilding. In this context, there were widespread concerns and expectations among the public and health professionals that mental health and primary care providers would face significant increases in demand as a result of worsening mental health in the Canterbury population. This prompted our evaluation of the literature and prescribing data to examine whether or not these concerns were matched by actual changes in prescribing for Canterbury.
A considerable literature reports that earthquakes and other disasters have both short- and long-term mental health effects (Norris et al., 2002a, 2002b). In the immediate aftermath of disasters, there are often high levels of anxiety, stress and sleep disturbance which are widespread but usually self-limiting (Galea et al., 2003; Van Griensven et al., 2006). In the longer term, the overwhelming finding from most studies is that the majority of people are resilient and continue to function without significant impairment (Bonanno, 2004; Fergusson and Boden, 2014). However, studies also report increased rates of depression, post-traumatic stress disorder and other psychiatric disorders in a minority which often persist (Bryant et al., 2014). The extent to which mental disorders are reported to increase following disasters varies. Some studies find little measurable impact from disasters (Canino et al., 1990), whereas others report significantly increased rates of mental disorder following disasters (North et al., 1999).
It is likely that methodological differences and factors such as the severity of the disaster and the unique effects of disasters on communities are important in explaining some of the variations in these findings. For example, many studies do not have a pre-disaster baseline with which to compare prevalence, and a number of studies rely on cross-sectional methodology with wide variations in timing of sampling and degree of exposure to the disaster. In general, studies with pre-disaster rates of measures to compare tend to find lesser or non-significant changes as a result of disasters (Canino et al., 1990; Fergusson et al., 2014; Knudsen et al., 2005; Spittlehouse et al., 2014), whereas studies that examine sub-populations with greater degrees of exposure and the use of cross-sectional methodology tend to find greater effects (see, for example, Galea et al., 2007; North et al., 1999; Salcioglu et al., 2003). Despite rates of mental disorder following disasters varying considerably (and resilience being the norm for most), the most consistent findings appear to be an exposure hierarchy with increased rates of mental disorder being found in those with a higher exposure to the disaster and a temporal gradient with rates of mental disorder generally reducing as time passes.
In considering the impact of a disaster on prescribing, it is noteworthy that significant proportions of affected individuals do not seek or receive professional help for their difficulties. Again, rates of help-seeking vary significantly between studies. The factors most commonly associated with treatment-seeking are level of psychopathology, level of exposure to the disaster and being of Caucasian background (Boscarino et al., 2005).
Previous studies have reported patterns of psychotropic medication use after disasters. In the presence of a functioning healthcare system, psychotropic use in this context can be regarded as an indirect measure of community psychiatric morbidity (Usher et al., 2012). Study designs include phone surveys of affected individuals addressing medication use (Boscarino et al., 2003) and pharmaco-epidemiological studies extracting prescribing medication rates for populations (Rossi et al., 2011) or sub-populations such as insurance holders (DiMaggio et al., 2007). The most consistent findings are short-term increases in prescribing of sedating medication (benzodiazepines and antipsychotics). However, there are a range of limitations to these studies, including the degree to which the study population is representative of the affected population, whether or not the datasets allow examination of local and national trends and whether or not all relevant medications are considered.
We have previously reported on the impact of the Canterbury earthquakes on inpatient psychiatric admissions and found reductions in bed occupancy in the immediate aftermath of the February earthquake with no rebound to increased occupancy over the study period (Beaglehole et al., 2015). This paper extends the examination of the impact of the Canterbury earthquakes on mental health by reporting psychotropic prescribing patterns. Our study adds to the existing literature by reporting all relevant psychotropic classes (antidepressants, anxiolytics, antipsychotics and sedatives/hypnotics) compared with national trends over a prolonged period to examine both acute and long-term effects of the earthquakes.
Method
The amount of medication dispensed, in units, by all pharmacies is routinely recorded nationally for District Health Boards (a regional organisation that provide health and disability services to populations within a defined geographical area). A unit of medication is defined as a tablet of any strength. In general, units of medication dispensed will correlate with the total amount of medication used by the population. In addition, units dispensed by pharmacies will closely correlate with prescribing by medical practitioners, although a small minority of scripts (7% in a large study in the New Zealand setting) will not be presented at pharmacies to be dispensed (Mabotuwana et al., 2009). As a consequence, dispensing data can be regarded as a proxy representing the underlying prescribing behaviours of medical practitioners in Canterbury. For the purposes of this study, we examined the units dispensed of the pharmaceutical classes of antidepressants, antipsychotics, anxiolytics (encompassing alprazolam, clonazepam, diazepam, lorazepam, oxazepam and buspirone) and sedatives/hypnotics (encompassing lormetazepam, midazolam, nitrazepam, temazepam, triazolam and zopiclone) (as defined by the Pharmaceutical Management Agency [PHARMAC], a New Zealand Crown agency that decides, on behalf of District Health Boards, which medicines and related products are subsidised for use in the community and public hospitals.)
The antipsychotic data were further broken down to include an examination of quetiapine prescribing according to high (100 and 200 mg) and low strength tablets (25 mg). We did this because there is a controversy about off-label prescribing of quetiapine (Monasterio and McKean, 2011) for anxiety and insomnia which commonly occurs with low strength tablets, and we wanted to see whether the earthquakes resulted in a change of prescribing for this indication.
We examined pharmacy dispensing over an extended time period from July 2007 to January 2014. This provided the opportunity to examine pre-existing local and national trends prior to the onset of the earthquake series in September 2010 and to clarify the short- and long-term impacts of the earthquakes on medication dispensing.
We compared dispensing data for the population serviced by the Canterbury District Health Board (Canterbury DHB) with national figures, excluding the Canterbury DHB. The Canterbury DHB provides health services to slightly over 500,000 people in the city of Christchurch, outlying towns and rural areas, and prescribing data capture all scripts dispensed in this region (approximately 11.5% of the national population). Greater Christchurch (defined as the city of Christchurch and immediate outlying towns within a commuter belt) comprises 85% of the population serviced by the Canterbury DHB and was the area most affected by the series of earthquakes. Over the approximate study period, Statistics New Zealand reported a 2.6% increase in the greater Christchurch population, whereas nationally, the population increased by 5.3% over the same period. As a consequence, data were corrected for the changes in population to derive population-adjusted figures reporting on Canterbury DHB dispensing as a percentage of national figures.
The study was approved by the University of Otago Ethics Committee (approval HD14/22). No specific funding or grant was required for this research.
Results
The dataset allowed a comparison of Canterbury DHB and national dispensing trends over an extended time period (July 2007–January 2014) in order to assess the impact of the earthquakes on prescribing.
For the class of antidepressants, there was a national trend for increased dispensing of antidepressants over the study period. This was present to a lesser degree in the Canterbury DHB data (Figure 1). When the population-adjusted Canterbury DHB data were compared to national figures as a percentage of total dispensing, there was an immediate fall in dispensing for the month of February 2011 followed by a gradual decline for the 3 years following the February earthquake (Figure 2). However, the relative decline in dispensing was largely due to increased dispensing nationally with no significant change in Canterbury DHB dispensing of antidepressants occurring following the earthquakes.
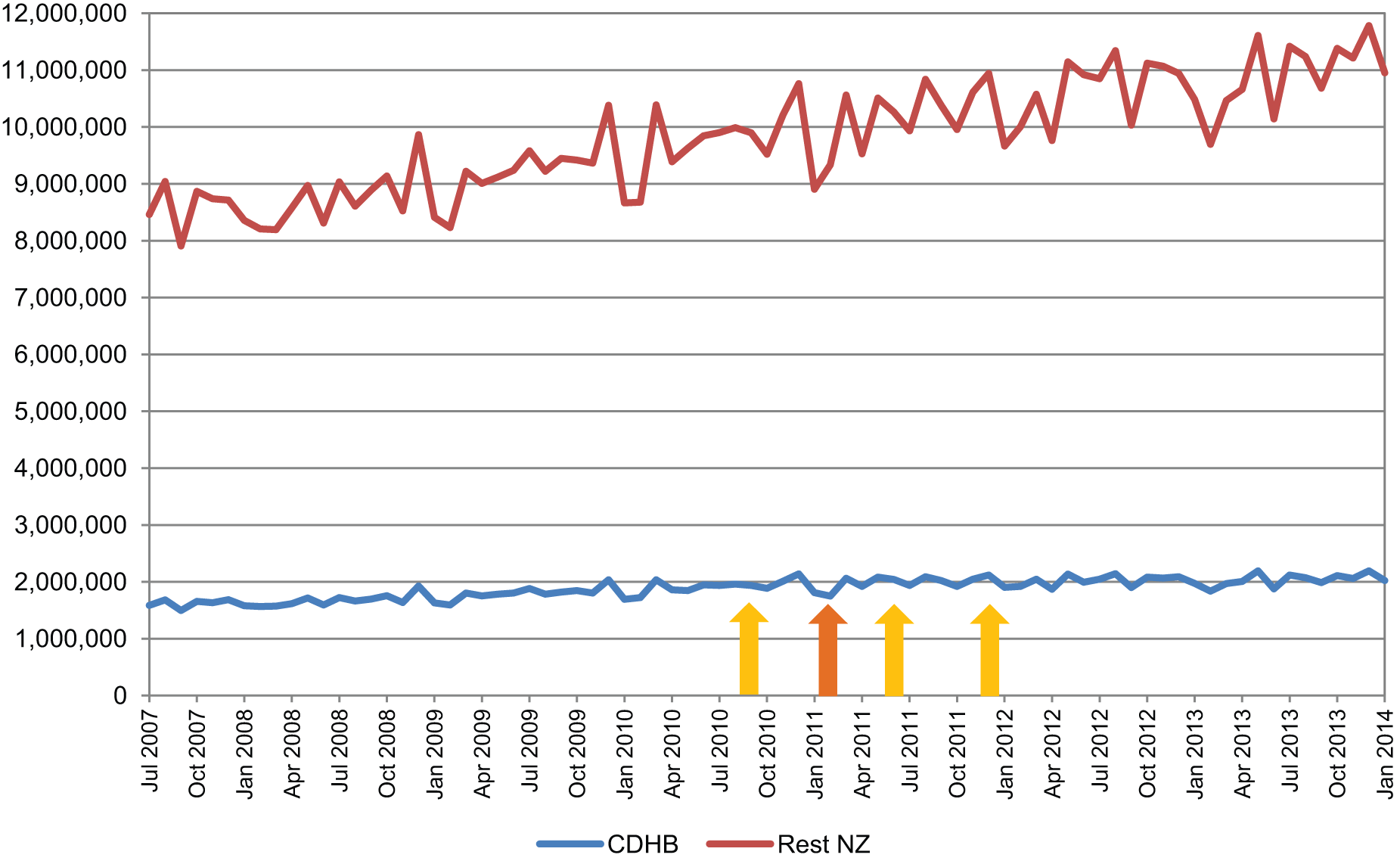
Units of antidepressants dispensed.
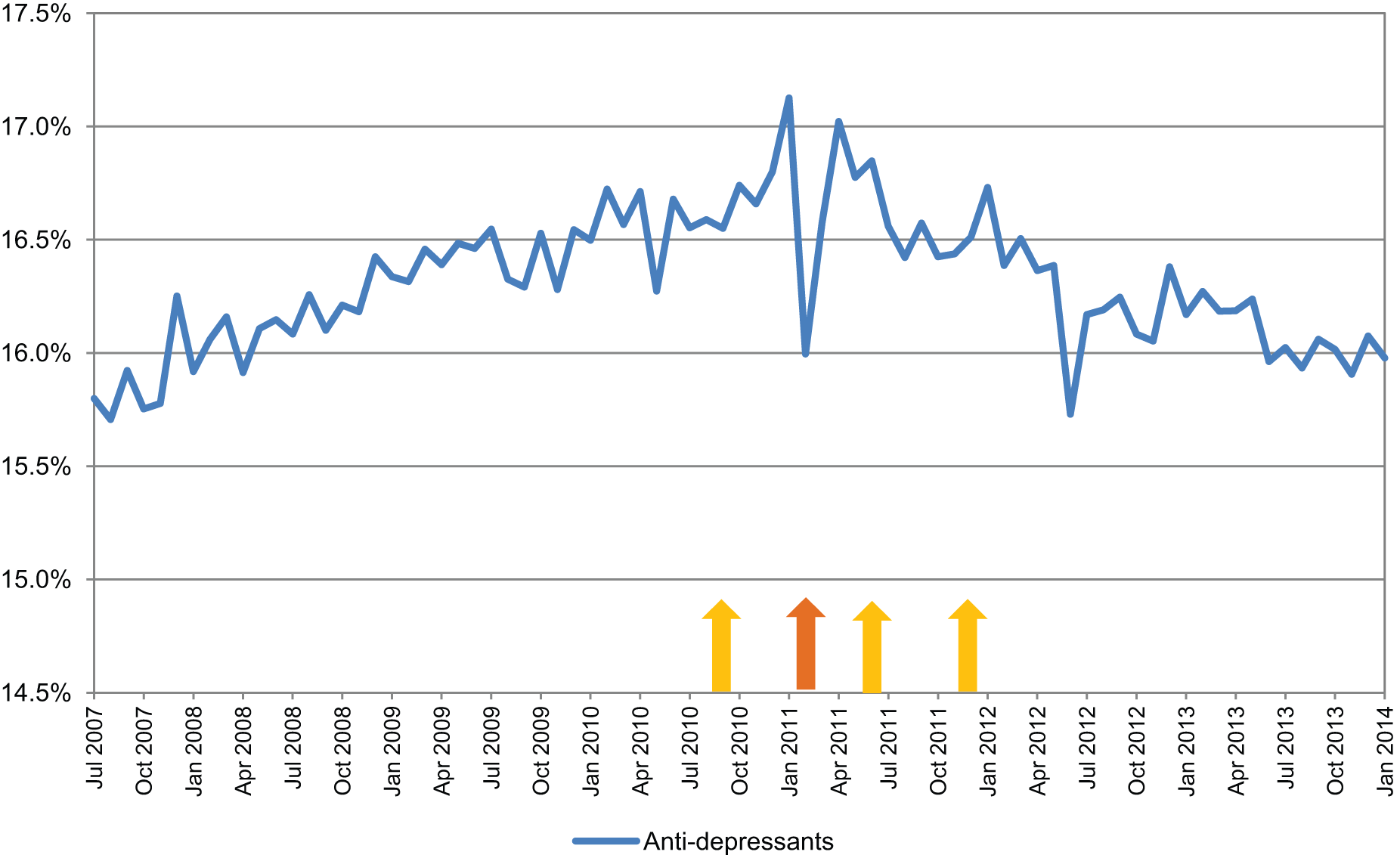
Antidepressant dispensing by Canterbury DHB as percentage of national dispensing.
For the class of sedatives/hypnotics, increased dispensing occurred nationally over the study period, predominantly during the time frame of 2010–2011. For the Canterbury DHB, a brief period of increased dispensing was evident after the February 2011 earthquake (Figure 3). When Canterbury DHB dispensing of sedatives/hypnotics was expressed as a population-adjusted percentage of national dispensing, a marked short-term increase in dispensing occurred after the February earthquake. However, this was not sustained, and dispensing by the Canterbury DHB as a percentage of national dispensing did not change over the study period (Figure 6).
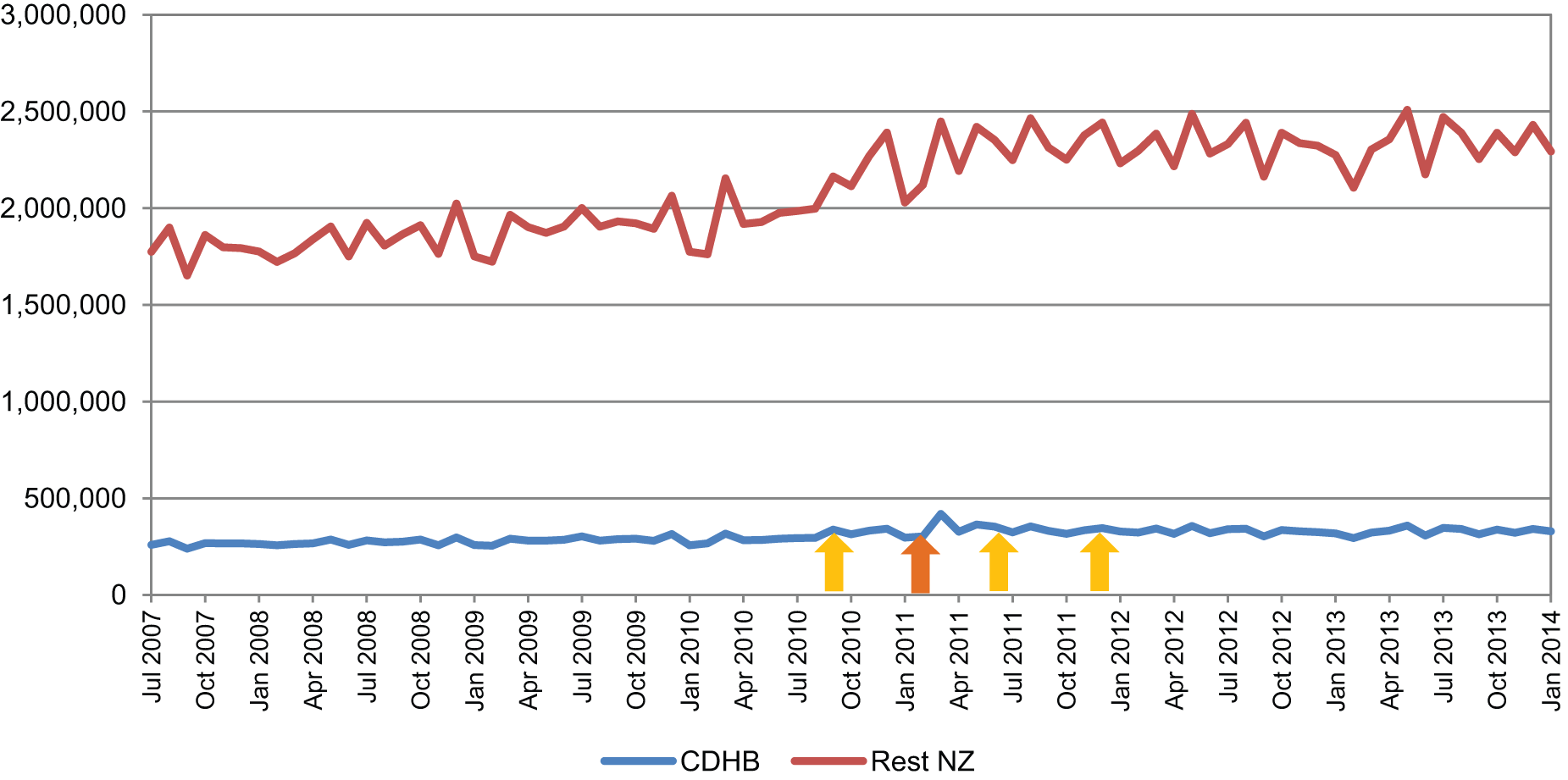
Units of sedatives/hypnotics dispensed.
For the class of Anxiolytics, similar trends to the class of sedatives/hypnotics were observed locally, nationally and when the Canterbury DHB was compared to national figures as a percentage of population-adjusted national dispensing (Figures 4 and 6).
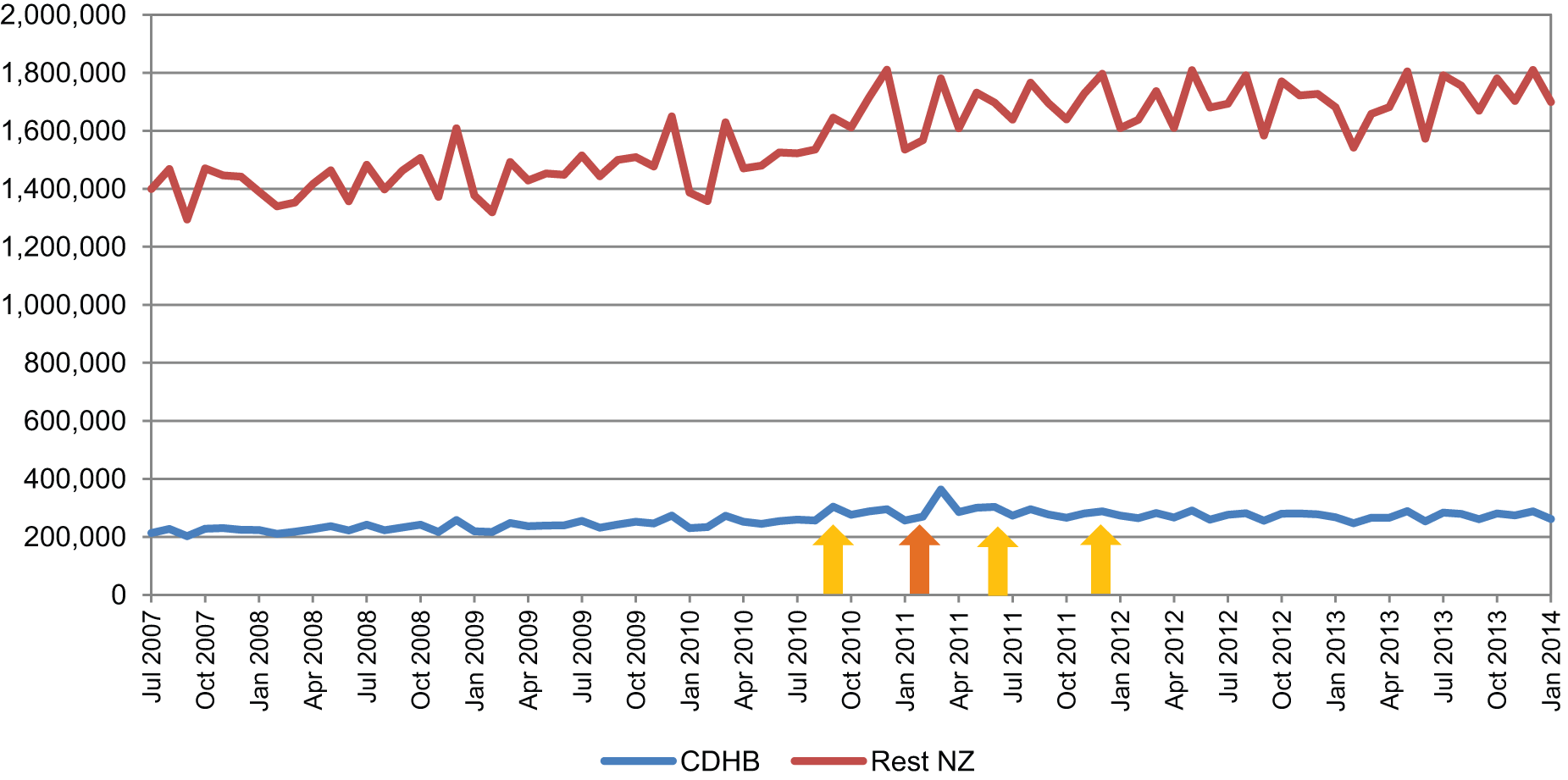
Units of anxiolytics dispensed.
For the class of antipsychotics, there was an overall trend for increased dispensing nationally over the study period. This was reflected to a lesser degree in the Canterbury DHB data which showed a small increase in dispensing over the same time period (Figure 5). When the Canterbury DHB was compared to national figures as a percentage of population-adjusted national dispensing, no clear effects were seen relating to the earthquakes (Figure 6).
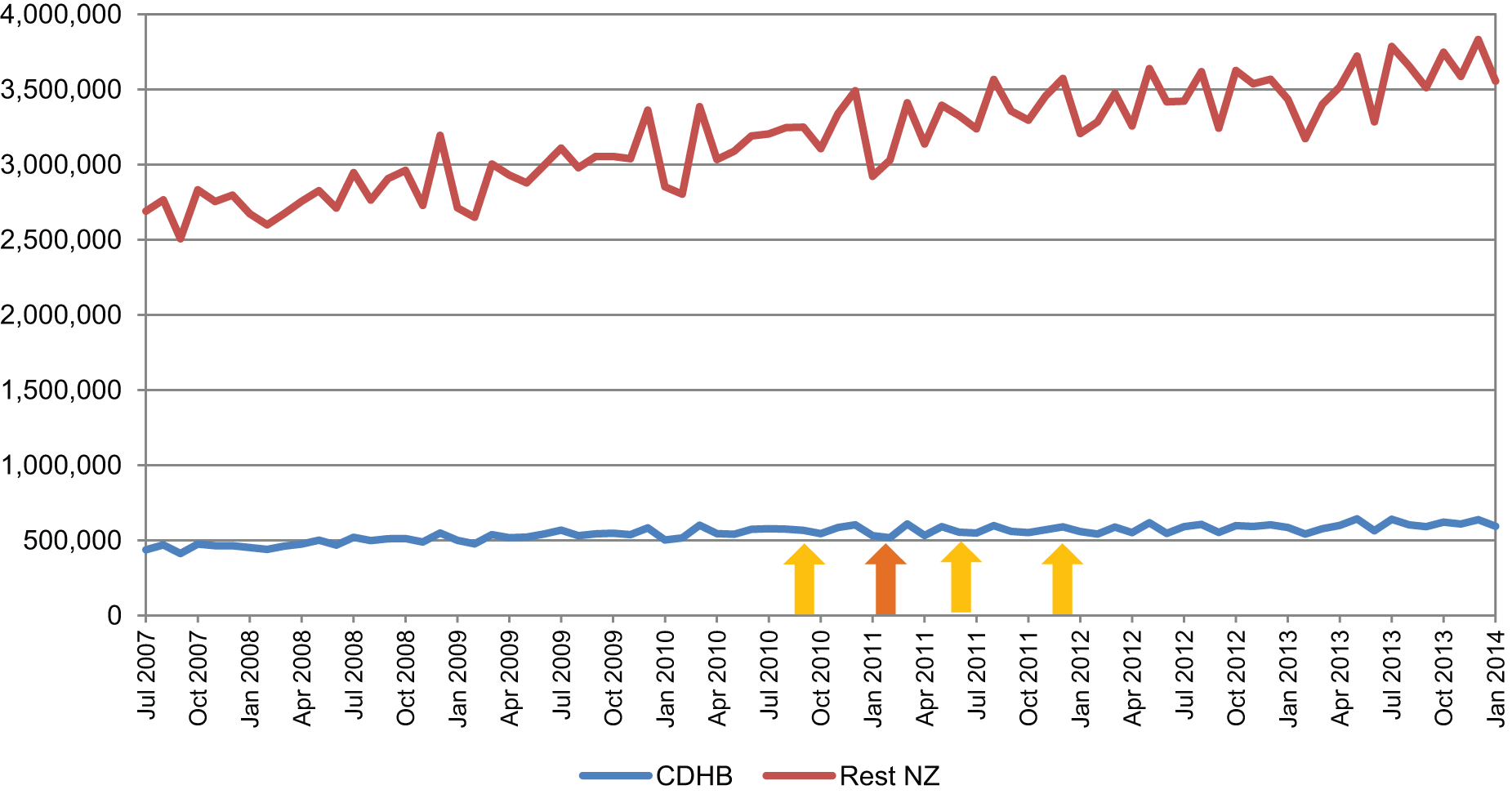
Units of antipsychotics dispensed.
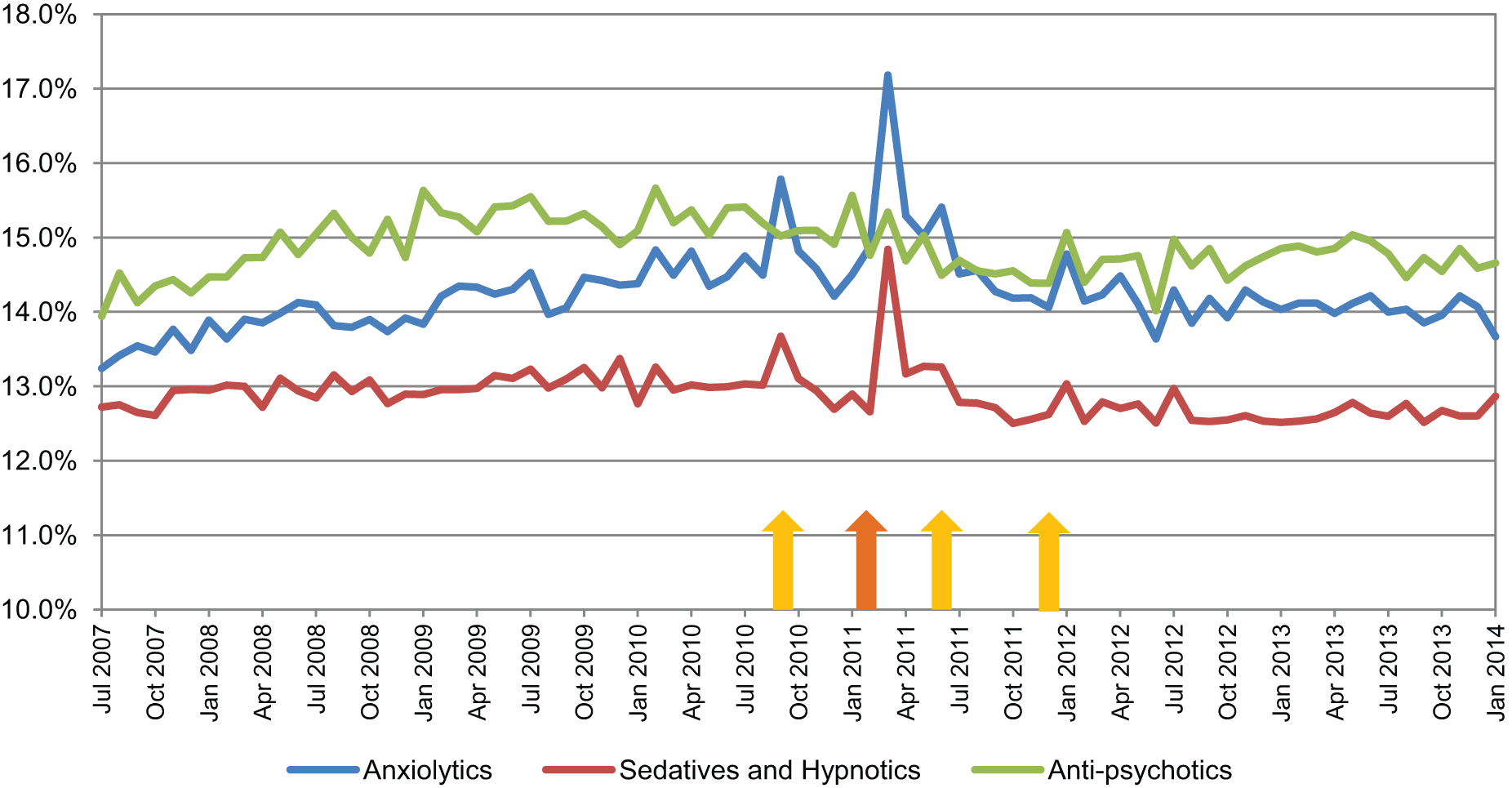
Sedatives/hypnotics, anxiolytics and antipsychotics dispensed by Canterbury DHB as a percentage of national dispensing.
When quetiapine as an antipsychotic was considered more specifically, there was a strong trend for increased dispensing of total quetiapine and the lower dose 25 mg tablets nationally over the entire period. Although there was an upward trend for the Canterbury DHB, this was less marked than the national trend (reflected by the declining percentage of national dispensing over time) (Figure 7). This figure also shows no clear effects as a result of the earthquakes on Canterbury dispensing.
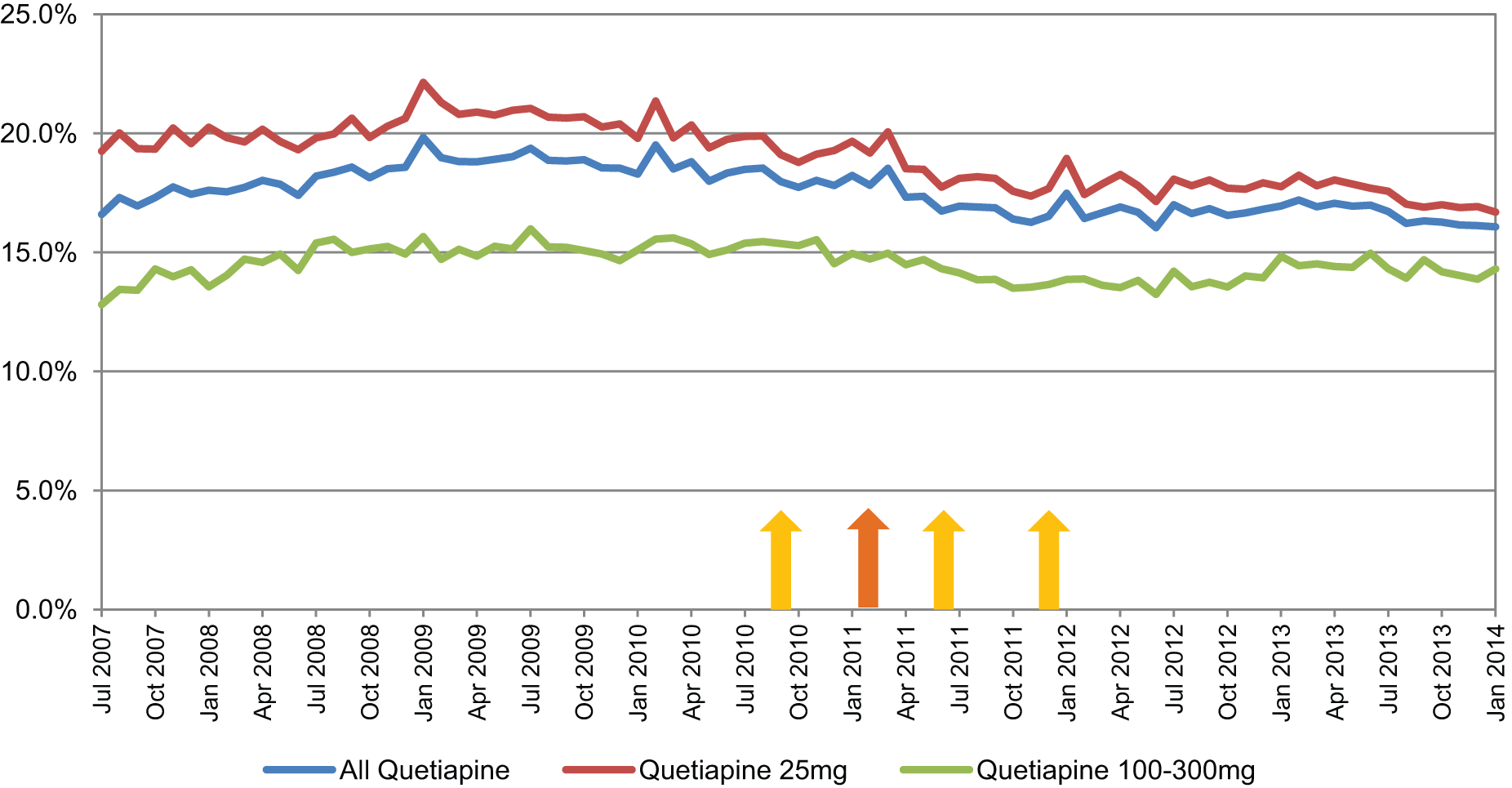
Quetiapine dispensed by Canterbury DHB as a percentage of national dispensing.
Discussion
This study examines the impact of the Canterbury earthquakes on dispensing of psychotropic medication for the population served by the Canterbury DHB. The dataset described captures all prescriptions dispensed in a region that was affected by a series of major earthquakes, one of which caused significant loss of life, destruction and major disruption over a prolonged period.
Health services remained largely intact despite the earthquakes. Despite a significant proportion of pharmacies operating in makeshift conditions, 96% of pharmacies were open within 24 hours of the devastating February 2011 earthquake and 95% General Practices were operational over a similar time period (despite a number of practices being destroyed). As a consequence, the data provided can be considered an indirect measure of the mental health effects of the earthquakes (Usher et al., 2012). The study was strengthened by the ability to present longitudinal data for all relevant psychotropic medication classes over an extended period between July 2007 and January 2014. This database therefore predated the onset of the earthquakes and is relatively unique in the disaster literature in that it allows robust comparisons between pre- and post-disaster effects to be made. It was also enhanced by the ability to compare Canterbury DHB dispensing with national trends. As a consequence, the impact of the earthquakes was able to be clarified against other local and national changes in dispensing.
The predominant findings were of short-term increases in the prescribing of the classes of anxiolytics and sedatives/hypnotics (primarily benzodiazepines) following the most destructive February earthquake. This confirms similar reports in the literature of short- but not long-term increases in benzodiazepine prescribing (Dorn et al., 2007; McCarter and Goldman, 2002). We found that there was no increase in the dispensing of antidepressants. Previous studies have reported variable findings with regard to antidepressants. Some have found no change (McCarter and Goldman, 2002; Trifiro et al., 2013), while others have reported an increase in prescribing, although these studies have not made comparisons with national trends over the relevant time period which makes attribution of the increases solely to the disasters uncertain (DiMaggio et al., 2007; Rossi et al., 2011; Usher et al., 2012). We also found that there was no increase in the dispensing of antipsychotics. A previous study has reported a short-term increase in prescribing of antipsychotics suggestive of use for agitation or stress-related behaviours (Trifiro et al., 2013). In our study, we looked specifically for an increase in low-dose quetiapine dispensing (often used off-label for anxiety and agitation) but found that no effects of the earthquakes on dispensing were observed.
The Canterbury DHB comprised approximately 11.5% of the national population over the study period, meaning that the psychotropic medicines studied were dispensed at a higher rate for the Canterbury DHB throughout the study period compared to the rest of New Zealand (including predating the onset of the earthquakes). A number of factors may have contributed to this finding. People with higher health need may be attracted to Canterbury DHB as a tertiary health service for the South Island of New Zealand. Organised and innovative general practice has also been a strength of Canterbury (Phillips et al., 2010). This may have resulted in early adoption of new pharmaceuticals (Tansella and Thornicroft, 2009). While dispensing in Canterbury was relatively stable over the period of data collection, dispensing in the rest of New Zealand increased more quickly resulting in a closing of relative dispensing rates between the two areas.
Our finding of short-term increases in benzodiazepine and hypnotic dispensing confirms previous reports in other disasters. However, it remains of interest why there were not more changes observed in prescribing over the period of the earthquakes. This dataset did not provide answers to this question, but it is possible to speculate on a number of possibilities. Although mental health symptoms and disorders are commonly reported sequelae of disasters, the impact on a population varies significantly between studies. This study provided an evaluation of the total population serviced by the Canterbury DHB which includes those with greater and lesser degrees of exposure to the earthquakes. It is possible that sub-populations, for example, relatives of those who suffered serious injury or death and those who were personally affected to a greater degree, would have more significant changes in psychotropic utilisation, but any effects were lost in our examination of the wider population. It may also be that those vulnerable to the effects of the earthquakes were over-represented in the population shifts after the earthquakes and were not represented by the dispensing data within the Canterbury DHB area.
Following a disaster, many people do not seek help for the mental distress they may be experiencing. Despite there being an intact healthcare service in Canterbury throughout the period in which earthquakes occurred, those affected may have chosen not to seek help for a variety of reasons. Reasons for individuals not seeking help in other settings include not believing they had a problem or wanting to solve the problem on their own, perceiving others to have more serious health needs than their own and difficulty accessing care for financial or other reasons (Boscarino et al., 2005).
It is also possible that the overall impact of the earthquakes on the mental health of the population serviced by the Canterbury DHB was minimal or not to a level that resulted in psychotropic medication prescribing. As noted previously, the majority of a population exposed to a disaster do not experience increased rates of mental disorder (Fergusson and Boden, 2014). Despite local population surveys reporting that up to 20% of the population are identifying as feeling stressed and functioning less well than before the earthquakes (Canterbury Earthquake Recovery Authority [CERA] wellbeing surveys), this level of stress and dysfunction does not necessarily equate to a level of severity that requires medication, and these surveys are vulnerable to selection and other biases. In Greater Christchurch, free counselling, increased primary healthcare services and a range of other social supports were provided for those dealing with earthquake-related difficulties; these interventions may have reduced the demand for specialist mental health services by preventing the progression to mental disorders or provided other means of managing symptoms without the use of psychotropic medication.
Although negative consequences of disasters are most commonly reported, there may also be beneficial effects from a disaster on the mental health of a population through mechanisms such as increased community cohesiveness and support for those who are vulnerable. This is consistent with reports of reduced suicides in times of adversity (Lester, 1993; Nishio et al., 2009). A reduction in suicide rate was also reported in Canterbury for the first year following the February earthquake (Ministry of Justice, 2011) although when viewed over a longer time frame, this effect is less clearly demonstrated (Ministry of Justice, 2013).
In summary, only short-term increases in dispensing of anxiolytics and sedatives/hypnotics were found after the most devastating February 2011 earthquake. No long-term increases in anxiolytics, sedatives/hypnotics, antidepressants or antipsychotics were observed as a result of the Canterbury earthquakes. These findings do not match expectations of significantly increased demand for mental health services by public and health professionals but are in keeping with a review of the literature. The absence of long-term increases in dispensing may reflect a number of factors including minimal overall effects of the earthquakes on the mental health of the population, minimal help-seeking in medical settings, a possible beneficial impact of increased availability of free counselling, primary healthcare services and a range of other social supports, and possible beneficial effects of disasters on the mental health of the population.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.