
Abstract
Objective:
Following the devastating earthquake in Christchurch, New Zealand, there was the widespread perception that the demand for inpatient mental health services would increase. However, our clinical observation was to the contrary, with substantial reductions in inpatient utilisation being noted. We therefore examined psychiatric bed occupancy and admission data to improve understanding of the impact of the disaster on mental health services.
Method:
We audited acute psychiatric bed occupancy and admission rates prior to and following a major earthquake.
Results:
After the earthquake, total bed occupancy reduced from an average of 93% to 79%. Daily admissions also reduced by 20.2% for the 30 days following the earthquake. All diagnostic groups, with the exception of the ‘Schizophrenia, schizotypal and delusional disorders’ category, contributed to the reduction. No rebound to increased occupancy or admissions was seen over the study period.
Conclusion:
The study confirmed our clinical observation that demand for acute inpatient psychiatric services were markedly reduced after the February 2011 earthquake.
Introduction
This paper discusses the impact of the 22 February 2011 Christchurch earthquake on the demand for acute inpatient mental health services. This earthquake was one of a series of earthquakes starting with a 7.1 magnitude earthquake on 4 September 2010 and continuing for more than 2 years with over 10,000 aftershocks. The February earthquake was the most devastating of the series of earthquakes, resulting in significant loss of life, multiple injuries, and widespread damage to property and infrastructure as well as the declaration of a national state of emergency (Ardagh et al., 2012).
In this context, there was the widespread perception amongst the public and health professionals that mental health services would be inundated. Many offers of support were made and planning was undertaken to respond to the anticipated increase in workload for primary and secondary mental health services. However, our clinical experience working in secondary services was to the contrary, with large lulls in demand for psychiatric care being noted.
There is an extensive literature focusing on the effects of disasters on communities. Increased rates of mental health disorders in the form of post-traumatic stress disorder (PTSD), depression, anxiety and somatic complaints are reported to be the most frequent complications of disasters (Bryant et al., 2014; David et al., 1996; Kuo et al., 2003; Norris et al., 2002; Salcioglu et al., 2003). However, the extent to which mental disorders are reported to increase following disasters varies. Some studies find little or minimal measurable impact from disasters (Canino et al., 1990; Fergusson and Boden, 2014), whereas others report significantly increased rates of mental disorder following disasters (North et al., 1999). The variation in these findings is likely to relate to the unique effects of disasters on communities as well as differences in study design. For example, many studies do not have a pre-disaster baseline with which to compare prevalence and a number of studies rely on cross-sectional methodology with wide variations in the timing of sampling and degree of exposure to the disaster.
The literature on the impact of disasters on mental health service use is much less extensive. The most common study design is a comparison of service use between populations with a higher degree of disaster exposure and populations with a lesser degree of exposure. Some studies also make pre- and post-disaster service use comparisons. Comparisons are made either through the use of population databases or surveys of selected groups exposed to the disaster. Findings from these studies also vary, with one study showing slightly reduced service use in those exposed to the disaster (Boscarino et al., 2004), another showing no significant difference in service use (Rosenheck and Fontana, 2003) and others reporting a slight increase in service utilisation (Fried et al., 2005). The impact of disasters on psychiatric admissions is rarely reported but studies that do report data did not find an increase in admissions (Rosenheck and Fontana, 2003) or reported a drop in admissions after the disaster (Fried et al., 2005).
In light of this literature and our clinical observation, we examined the inpatient mental health bed occupancy and inpatient admission data before and after the earthquake in February 2011. We examined both short- and long-term effects to clarify the impact of the earthquake on local inpatient mental health services, and to provide guidance for those involved in planning a response to future disasters elsewhere.
Methods
This study was conducted using data from the sole provider of adult mental health services in Christchurch, New Zealand, which were well established prior to the earthquakes. The service included a 64-bed acute inpatient unit, a 51-bed rehabilitation ward, community mental health teams, a 24-hour psychiatric emergency service, and a range of specialist services. As a result of the February earthquake, the premises for most outpatient community mental health teams were unusable but staff were relocated to sites within the grounds of the psychiatric hospital. The inpatient facilities were relatively undamaged. Despite disruption, all services continued to be delivered from the day of the earthquake onwards. In addition to usual services, an outpatient service to treat serious earthquake-related mental disorder was set up and provided outpatient care over the study period and beyond.
The acute adult inpatient service routinely collects data on bed occupancy and admissions to the unit. Total bed occupancy is calculated each night on the basis of the number of individuals sleeping on the psychiatric ward at midnight. Bed occupancy reflects both new admissions and duration of stay, while admission data record new admissions every 24-hour period. The admission data are subsequently linked to the International Classification of Diseases, 10th Revision (ICD-10) diagnoses by clinical coding staff. This allows grouping of admission data to the most common ICD categories on an inpatient ward (Mood (affective) disorders; Schizophrenia, schizotypal and delusional disorders; Disorders of adult personality and behaviour; Neurotic, stress-related and somatoform disorders; and Mental and behavioural disorders due to psychoactive substance use). These measures allowed us to examine the acute and longer-term impacts of the earthquake by tracking and comparing the bed occupancy, admission rates, and diagnostic data for the years prior to and after the earthquake.
The bed occupancy in the month after the earthquake was compared to the pre-earthquake level using a z-test which included the month-to-month variability for the 5 years prior to the earthquake to provide an estimate of the standard deviation for the monthly rates. We also examined bed occupancy for the 18 months following the February earthquake to assess for changes over this period.
We studied the effect on admissions by comparing the mean number of daily admissions for the 30 days preceding and following the earthquake. We compared the admission data following the earthquake with the previous 5 years to control for seasonal changes in admissions and to examine longer-term effects. We repeated this according to diagnostic grouping in order to determine whether or not there were specific effects relating to diagnosis.
No ethics approval was required for this study because this was a clinical audit.
Results
Bed occupancy was relatively stable prior to the major earthquake in February 2011, varying between 87% and 98% with an average of 93% occupancy. In the month after the earthquake, total bed occupancy showed a marked reduction to 79% (–z = 7.5, p<0.001) (Figure 1). A similar reduction was seen for total daily admissions, which fell by 20.2% for the mean number of admissions in the 30 days after the earthquake compared with the mean for the 30 days preceding the earthquake (3.1 admissions/day prior to the earthquake fell to 2.5 admissions/day). All diagnostic groups contributed to the reduction with the exception of the ‘Schizophrenia, schizotypal and delusional disorders’ category, which showed a small non-significant increase in the number of admissions from 0.9/day to 1.0/day.
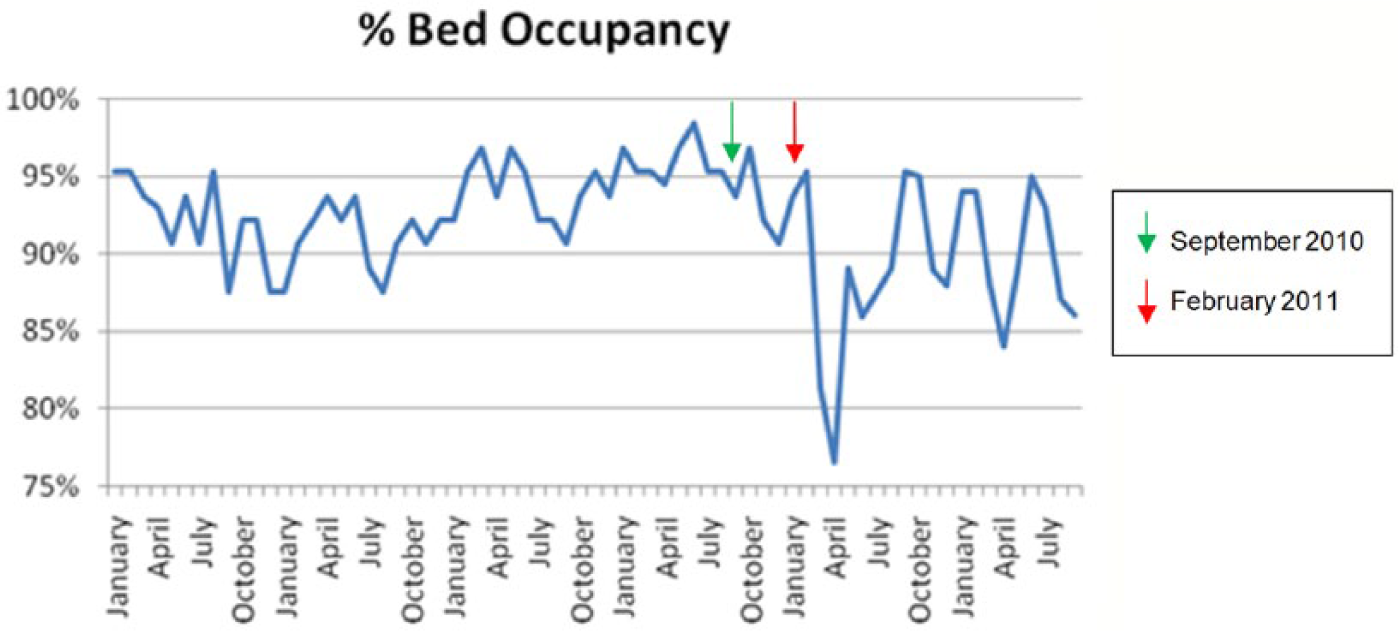
Percentage bed occupancy prior to and for 18 months following the February 2011 earthquake.
We also examined whether there was a rebound to increased bed occupancy and admissions in the longer term following the earthquake. However, there was no rebound to increased bed occupancy in the 18 months after the February earthquake (Figure 1). In addition, the monthly total admission data showed a 10% decline (z = −2.9, p<0.01) for the year after the earthquake, compared with the 5-year average preceding the earthquake. All of the major diagnostic groups were represented in reduced monthly admissions for the year following the February earthquake compared to the previous 5 years (Figure 2). The biggest percentage drop was 25.9% for the category of ‘Disorders of adult personality and behaviour’ (from 14.5/month to 10.7/month), although this represented a small proportion (14%) of the total daily admissions. ‘Mood (affective) disorders’, representing 40% of total admissions, showed a 9.8% reduction in average monthly admissions (from 40.4/month to 36.4/month) and ‘Schizophrenia, schizotypal and delusional disorders’ a 5.0% reduction. Other categories only contributed a very small proportion of the total admission data.
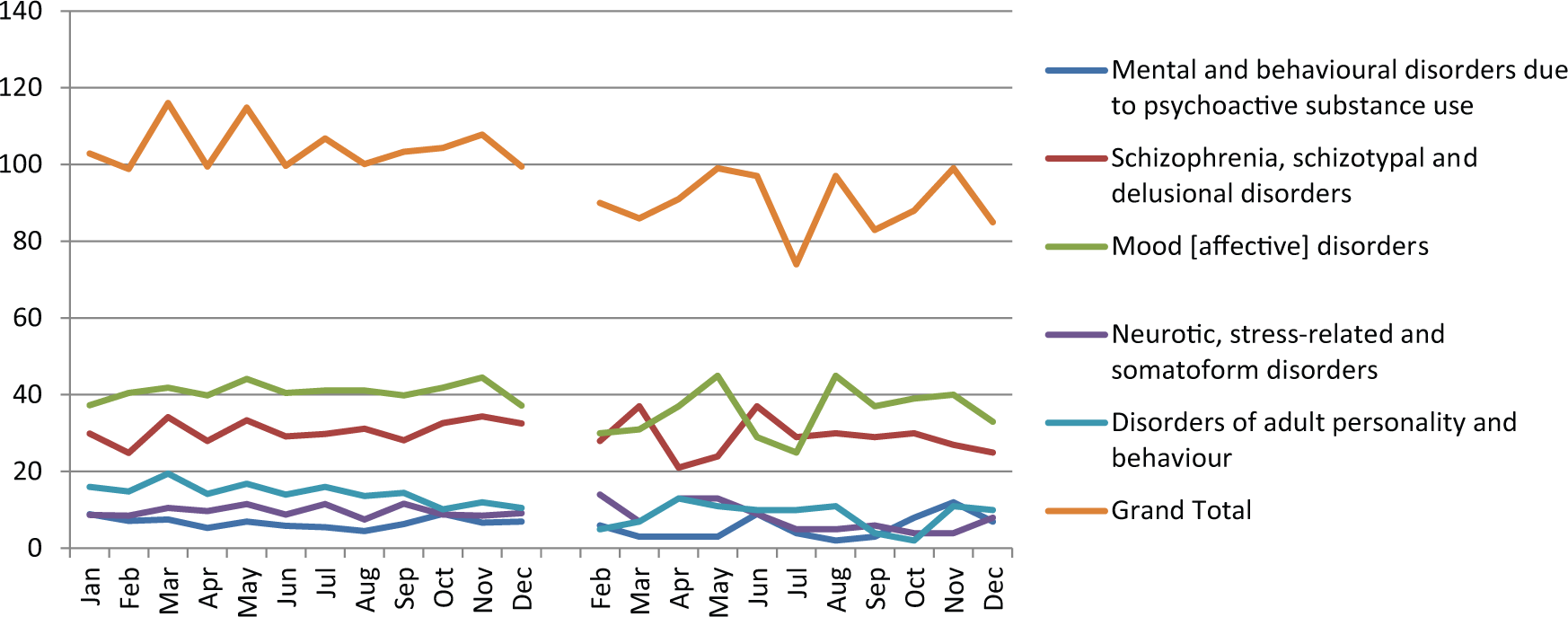
The first year on this plot shows the average monthly admissions for the 5 years preceding the February 2011 earthquake. The second year shows the monthly admissions for 2011 following the February 2011 earthquake.
Discussion
The aim of this paper was to examine the inpatient mental health bed occupancy and admission data before and after a major disaster. The data confirmed our clinical observations that demand for acute inpatient mental health services was reduced after the February 2011 earthquake. This was reflected by falls in both bed occupancy and admission data. The drop in occupancy and admissions occurred in the short term following the disaster and did not rebound over the study period. The reduction in service use was at odds with widespread assumptions that mental health services would face increased demand.
Although not reported in this paper, referrals to outpatient specialist mental health services appeared to mirror the inpatient findings with a marked reduction in referral rate in the short term following the February earthquake (information available on request). We do not report this in detail because although outpatient services were well established, their system for collecting referral data changed just prior to the earthquakes and we were unable to make the same historical comparisons as the inpatient data.
Our analysis did not provide us with explanations as to why admissions after the earthquake were reduced acutely and failed to return to previous levels. However, it is possible to speculate on a number of influencing factors. Disasters are most strongly associated with increased rates of PTSD and depression, which are disorders that are typically managed in the community and which are less likely to require inpatient admission. As a consequence, an increase in community morbidity may not have been expected to have been reflected in our inpatient data. However, the category of ‘Mood (affective) disorders’ includes patients who require admission for depression, and post-earthquake falls in admissions were recorded both acutely and in the longer term for this category. The category of ‘Neurotic, stress-related and somatoform disorders’ represented only a small proportion of inpatients at any one time and also did not appear to change significantly over the study period.
However, a key finding of our study is not only that there was no increase in bed occupancy and admissions, but that these were reduced acutely and in the longer term. This is despite Canterbury continuing to experience frequent aftershocks over a prolonged period. In addition, there have also been persistent secondary stressors (insurance disputes and damage to housing and infrastructure) facing the population. A possible explanation for the reduction in admissions may be that free counselling, increased primary health care services, and a range of other social supports were provided for those dealing with earthquake-related difficulties. These interventions may have reduced the demand for specialist mental health services by preventing the progression of mild to moderate severity disorders and providing more support for those with severe mental disorders. In addition, the disaster literature also describes some beneficial effects of disasters for mental health through mechanisms such as increased community cohesiveness and support for those who are vulnerable. This is supported by the finding of reduced suicidal ideation (Kessler et al., 2006) and suicides in times of adversity (Lester, 1993; Nishio et al., 2009), although this finding has not always been consistently replicated (Henderson et al., 2006; Krug et al., 1998). In Canterbury, a reduction in suicide rate for the first year following the February 2011 earthquake was reported (Ministry of Justice, 2011), although when viewed over a longer time frame this effect is less clearly demonstrated (Ministry of Justice, 2013). Our study showed that all major diagnostic categories were represented in the reduction of mean monthly admissions, with the effect being most marked for the category ‘Disorders of adult personality’. It is therefore possible to speculate that people with personality disorders were most responsive to the interventions that increased social cohesion in the aftermath of the earthquake.
It is also important to note that many people do not seek or receive treatment for the mental health sequelae of disasters (Boscarino et al., 2005; Bramsen and van der Ploeg, 1999). The degree of exposure to the disaster, the severity of psychopathology, and sociodemographic factors appear to be important in predicting help seeking (Gavrilovic et al., 2005). In one study, the most common reason for not seeking care was not believing there was a problem requiring treatment, with other factors such as wanting to solve the problem themselves, difficulty accessing care, financial problems, and fear of treatment also being relevant (Boscarino et al., 2005). Our dataset did not allow us to explore individual or sociodemographic factors to establish whether or not these factors were relevant in our local setting.
The earthquakes resulted in people leaving the city, with the population of Christchurch dropping by 8900 people (2.4%) in the June 2011 year (Statistics New Zealand, 2011). Although this is insufficient to explain the degree of observed reduction in service utilisation, it is possible that vulnerable subgroups, for example those with mental illness, were over-represented in the numbers that left. However, personal communication from a neighbouring mental health service suggests that there was no significant increase in Christchurch-domiciled patients using their inpatient service over the relevant time period.
In conclusion, admissions to the acute inpatient service reduced after the February 2011 earthquake. We were able to confirm these data acutely and over an extended time period following the earthquake. We were also able to make pre-earthquake comparisons through the use of longitudinal records. This finding extends the small literature that examines mental health service utilisation following disasters but is counterintuitive to widely held perception and is helpful for those planning service provision after subsequent disasters.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.