
Abstract
Background:
Sleep disturbances are highly prevalent in adolescents with depressive disorders. To date there is limited evidence of the extent to which sleep disturbances are associated with treatment response in adolescents. This study aimed to examine the extent to which self-reported sleep disturbances are associated with treatment response in adolescents with depression.
Method:
Sleep data were gathered from a sample of 166 adolescents (aged 12–18 years) with a diagnosis of a DSM-IV depressive disorder who underwent 3 months of treatment (psychosocial and/or pharmacotherapy (sertraline)) in community-based research programs. The subjective report of sleep disturbance within depressive disorders was assessed using the Kiddie Schedule for Affective Disorders and Schizophrenia for School Age Children at three time points: pre-treatment, post-treatment and 6-month follow-up.
Results:
Sixty-nine percent of participants had a sleep disturbance pre-treatment and approximately 75% of these participants had threshold symptoms. Threshold sleep disturbances that persisted from pre- to post-treatment assessments were positively associated with depression at the 6-month follow-up. An ordered logistic regression model controlling for gender, treatment group and comorbid anxiety estimated a 70% risk of depression or partial remission for those with persistent sleep disturbance. Treatment group, anxiety and gender generally had no significant effect on the relationship between sleep and depression.
Conclusion:
Sleep disturbances were highly related to depressive state and were associated with poorer treatment response in adolescents with depression. These results provide a rationale for further exploration of sleep-related treatments for adolescents with depression. Knowledge of patient-reported persistent sleep disturbances can help clinicians to predict treatment outcomes and may direct them to augment treatment or focus on sleep-related treatment strategies.
Introduction
Sleep has a bi-directional relationship with depressive disorders (Lustberg and Reynolds, 2000). Sleep disturbances and depression appear to aggravate and maintain each other (National Institutes of Health, 2005; Stepanski and Rybarczyk, 2006). Insomnia is common in adolescents with depressive disorders and is a risk factor for the development of new onset or recurrent depression (Buysse et al., 2008; Ford and Kamerow, 1989; Liu et al., 2007; Riemann and Voderholzer, 2003), even after controlling for prior depressive symptoms (e.g. psychomotor retardation or agitation, suicidal ideation) (Breslau et al., 1996). Furthermore, there is a significant temporal relationship between sleep disturbances and completed suicide in adolescents (Goldstein et al., 2008). While subjective sleep disturbance has been found to be a predictor of the occurrence, recurrence and severity of depressive episodes in adults and adolescents alike (Emslie et al., 2001; Ford and Cooper-Patrick, 2001; Ohayon and Roth, 2003), objective electroencephalographic measures of sleep have not provided consistent results in adolescents (Bertocci et al., 2005).
Depression that occurs during adolescence has substantial continuity, morbidity and potential mortality from suicide into adulthood (Weissman et al., 1999). Early detection and treatment is of considerable importance. Only about 60% of adolescents with depression respond to established treatments including cognitive behavioural therapy (CBT) and selective serotonin re-uptake inhibitors (SSRIs) (Birmaher and Brent, 2007; Birmaher et al., 2007; Goodyer et al., 2007; Kennard et al., 2006; Melvin et al., 2006; Rey and Hazell, 2009).
Given the bi-directional association between sleep disturbance and depression, addressing sleep disturbances specifically may enable better outcomes of treatment for depression in adolescents (Stepanski and Rybarczyk, 2006; Thase, 2005). Insomnia-focused CBT improves depressive symptoms as well as insomnia (Lichstein et al., 2000; Manber et al., 2011; Morin et al., 1994; Stepanski and Rybarczyk, 2006). In contrast, SSRIs appear to improve some of the abnormalities of sleep found in adolescent major depressive disorder but are frequently associated with insomnia (Anderson et al., 2000). Polysomnographic sleep studies show that in youth, SSRIs increase rapid eye movement (REM) sleep latency and reduce the amount of REM sleep early in treatment, although these changes show rebound effects after cessation of treatment (Wilson and Argyropoulos, 2005).
Few have examined the extent to which sleep disturbance is associated with the response to treatment of depression in adolescents. Kennard et al. (2006) found that sleep disturbance was the most common residual symptom in adolescents who failed to remit after 12 weeks of treatment for depression. In another study, reduced sleep quality, assessed by polysomnography, was found to be a predictor of the recurrence of depressive disorders in adolescents (Emslie et al., 2003); however, studies using objective measures of sleep in depressed patients have produced conflicting results (Jarrett et al., 1990; Rao and Poland, 2008; Simons and Thase, 1992; Thase et al., 1997). Subjective measures of sleep are important because they provide a clinically useful indicator of the phenomena of sleep disturbance experienced by the patient (Argyropoulos et al., 2003) and may be an important early marker of depressive disorders (Gillin, 1998).
Augmenting an antidepressant medication with a brief, symptom-focused CBT for insomnia could improve outcomes for adolescents in terms of alleviating both depression and insomnia (National Institutes of Health, 2005). The potential contribution of insomnia to the continuity of depressive symptoms during and after antidepressant treatment warrants further examination. Clinical care could potentially be advanced by exploration of variables that predict a positive response to any treatment as well as variables that indicate which youths are most likely to benefit from one treatment compared with another (Curry et al., 2006).
The aim of this study was to examine the extent to which subjective sleep disturbances are associated with treatment response in adolescents diagnosed with a depressive disorder and treated with the SSRI sertraline, CBT, or with both treatments combined. It was hypothesised that the presence of sleep disturbance at baseline (pre-treatment) would be associated with an increased rate of depressive diagnosis post-treatment regardless of the treatment type.
Methods
Participants
The sample comprised 166 adolescents (aged 12–18 years, mean 15.0 years, standard deviation 1.5 years) with depressive disorders, who participated in two separate trials assessing the efficacy of the SSRI sertraline, CBT, or sertraline and CBT combined, on depressive symptoms (Melvin et al., 2006; Tonge et al., unpublished observations). It was deemed appropriate to combine data from the two trials for the purposes of the present study, as the inclusion/exclusion criteria and the treatment regimes were comparable (see below). Both trials were approved by the Southern Health Human Research Ethics Committee. Written informed consent was obtained from participating parents and assent obtained from adolescents. Participants were referred by physicians or school counsellors for assessment of possible depression. Both trials involved similar recruitment procedures and random allocation to treatments (see, Melvin et al., 2006). Eligible participants were required to have a DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition) diagnosis of major depressive disorder (MDD), dysthymic disorder (DD), or depressive disorder not otherwise specified (DDNOS). Exclusion criteria included major physical illness or epilepsy, bipolar disorder, organic brain syndrome, intellectual disability of sufficient severity to preclude participation in therapy, psychotic disorder, a primary diagnosis of substance abuse disorder, active suicidality or other severe psychiatric disturbance that required acute hospital admission, and current antidepressant or psychotropic medication treatment. For participant demographics and clinical characteristics of the treatment groups, see table 1.
Demographics and clinical characteristics of the treatment groups (pre-treatment).
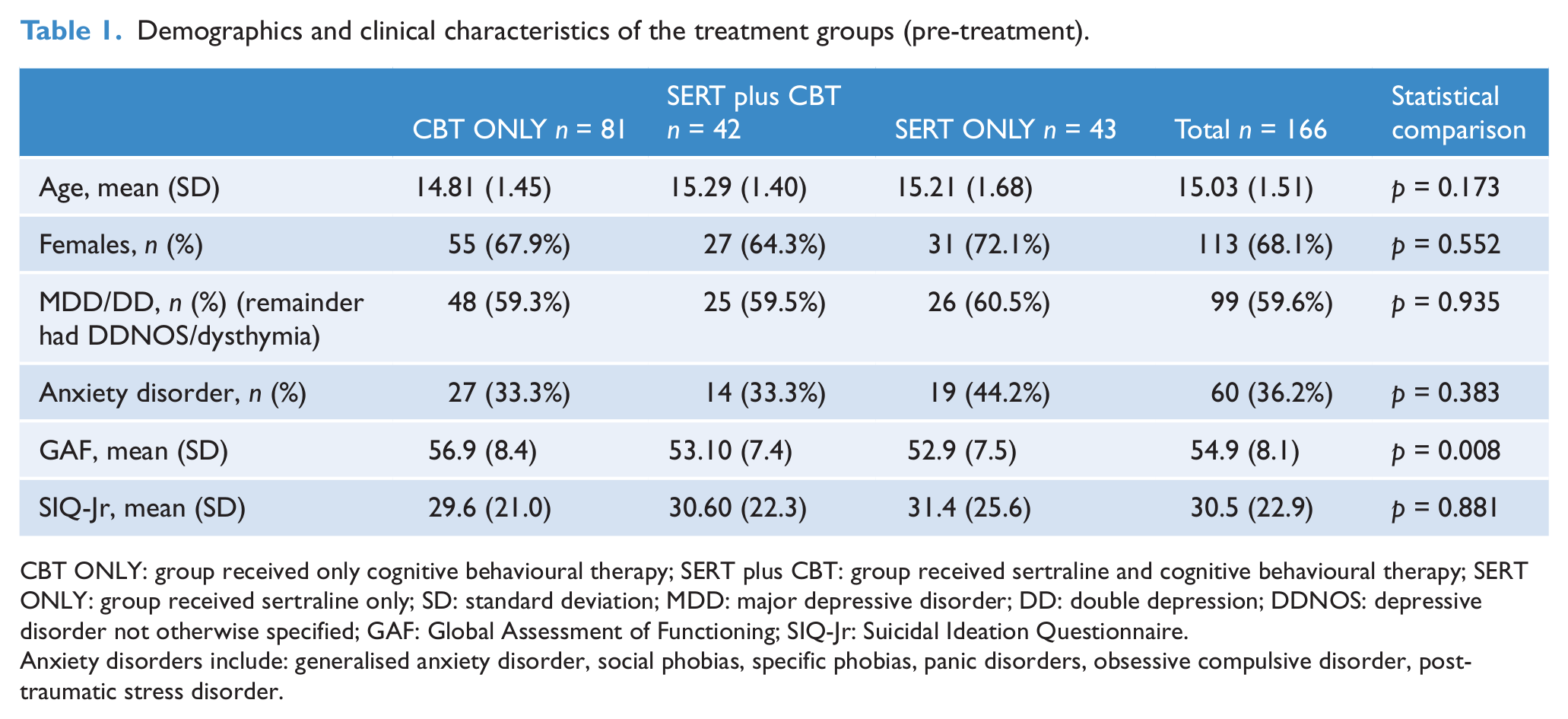
CBT ONLY: group received only cognitive behavioural therapy; SERT plus CBT: group received sertraline and cognitive behavioural therapy; SERT ONLY: group received sertraline only; SD: standard deviation; MDD: major depressive disorder; DD: double depression; DDNOS: depressive disorder not otherwise specified; GAF: Global Assessment of Functioning; SIQ-Jr: Suicidal Ideation Questionnaire.
Anxiety disorders include: generalised anxiety disorder, social phobias, specific phobias, panic disorders, obsessive compulsive disorder, post- traumatic stress disorder.
Treatments
Treatments were administered at clinics associated with public child and adolescent mental health services in metropolitan Melbourne (Frankston and Clayton) and regional Victoria (Geelong).
Sertraline (SERT) (n = 43)
Sertraline was administered for 12 weeks with weekly medication review sessions. Sertraline was administered on a sliding dose regime, starting at 25 mg, and increased appropriately according to the response of the individual up to a maximum of 100 mg. Adverse events were actively monitored at each review session.
Cognitive behavioural therapy (CBT) (n = 81)
Treatment consisted of 12 weekly sessions of CBT for adolescent and parents or adolescent alone followed by three monthly ‘booster’ sessions. The CBT treatments involved goal setting, psychoeducation, pleasant event scheduling, relaxation training, cognitive therapy, social skills training and communication skills (Melvin et al., 2006). The parent sessions focused on psychoeducation, communication, problem-solving skills training, and behaviour management skills designed to assist parents in the management of their child’s depressive illness.
Cognitive behavioural therapy and sertraline combined (CBT + SERT) (n = 42)
Treatment consisted of 12 weekly sessions of CBT for parents and adolescent concurrently with 12 weeks of sertraline, with weekly medication review sessions, as per the protocols described above.
Assessments
An assessment battery was administered pre-treatment, post-treatment, and at a 6-month follow-up session. All participants who were randomised to treatment were included in the analysis, regardless of treatment compliance. Non-blinded treating clinicians completed assessments with the exception of a few cases where blinded independent assessors were available. Figure 1 illustrates the participant disposition and protocol.
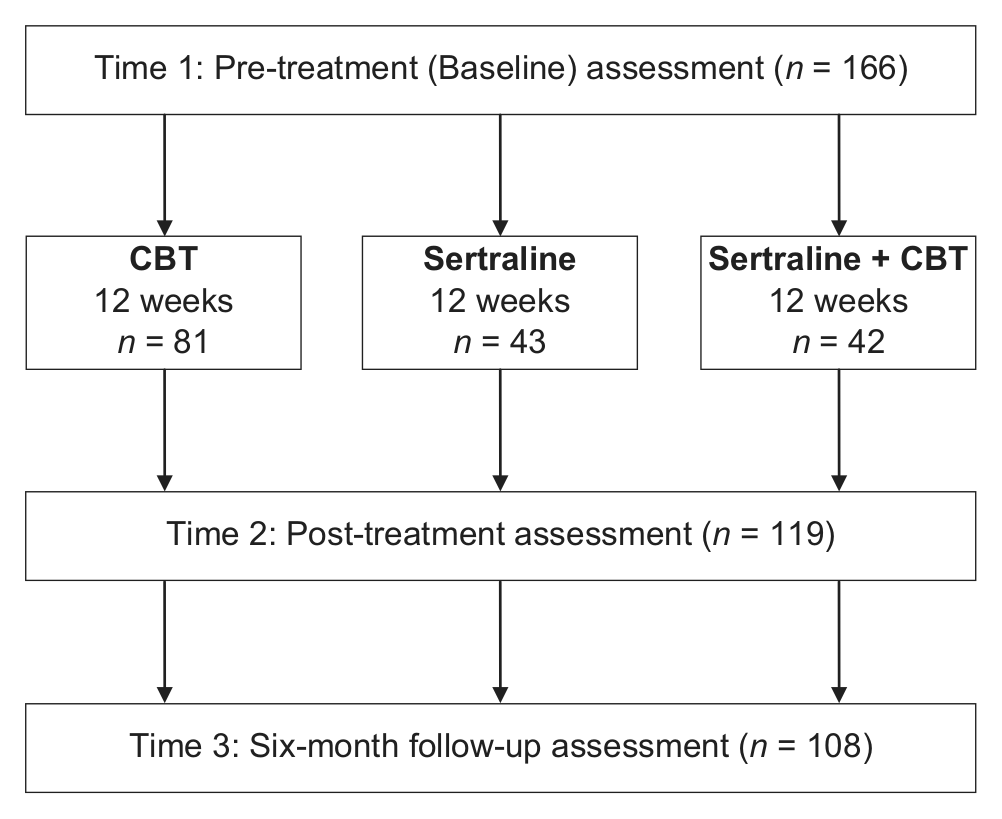
Participant disposition and study design.
Outcome measures
The primary outcome measures of the DSM-IV-TR (American Psychiatric Association, 2000) depressive diagnosis were used as it is a widely agreed upon definition of depression and is an outcome of interest to clinicians. It was assessed using the Schedule for Affective Disorders and Schizophrenia for School Age Children—Lifetime Version (K-SADS), a semi-structured diagnostic interview administered by clinicians. The K-SADS is reported to have good psychometric properties including inter-rater and test-retest reliability, and predictive and construct validity (Ambrosini, 2000; Kazdin and Peiti, 1982). Depressive outcomes were classified as full remission (8 weeks asymptomatic), in partial remission (a reduction in symptoms or no symptoms for less than 8 weeks) or depressed (APA, 2000).
Subjective sleep disturbance was measured using the K-SADS items on insomnia and hyposomnia. This instrument has been used in a similar way in a previous study of adolescents with depression (McConville et al., 1996). The subjective complaint of insomnia and hypersomnia are included in the DSM-IV-TR definition of sleep disturbance in a depressive diagnosis (American Psychiatric Association, 2000). In the present study, insomnia and/or hypersomnia were classified as absent, subthreshold or threshold using the following definitions provided by the K-SADS. Threshold insomnia was considered to be 2 or more hours of initial insomnia or 30 minutes or more of middle or terminal insomnia. Hypersomnia was considered to reach threshold if the young person slept more than 11 hours in a 24-hour period several times a week, or regularly would if they were not awoken by a parent and actually did so when left to sleep. Only threshold sleep disturbance (threshold symptom of insomnia and/or hypersomnia) was used in regression analyses so that any associations identified would be based on clinically significant sleep disturbance rather than more modest disturbances. Parent and young person reports about sleep disturbance were recorded separately. If a young person’s report was missing, parental reports were used. The inter-rater reliability of this method of classifying sleep disturbance was tested among three trained raters in a random sample of 10 cases. The kappa statistic between raters ranged from 0.59 to 0.77 (mean = 0.66, p < 0.01 in all cases). Using a consistency definition the intraclass coefficient for single measures was 0.66 and for average measures was 0.85, p < 0.01.
Clinicians completed the Global Assessment of Functioning (American Psychiatric Association, 2000) at each of the assessment points. Details of other assessment tools used during the assessment periods not relevant to this study are reported elsewhere (Melvin et al., 2006).
Statistical analysis
Data were analysed using the Statistical Package for Social Sciences Version 17 (SPSS Inc., Chicago, IL, USA) and STATA Version 9 (StataCorp LP, College Station, TX, USA). Initial analyses examined clinical characteristics and rates of depressive diagnoses in all groups at baseline. Chi-squared test and analysis of variance (ANOVA) were used, as appropriate, to compare differences between treatment groups. Random effects logistic regression was used to model the probability of threshold sleep disturbance as a function of depression status and comorbid anxiety at pre-treatment, post-treatment and 6-month follow-up, controlling for gender and treatment group. Ordered logistic regression was used to model the dependence of depressive outcomes in the long term on the presence of threshold sleep disturbance at earlier stages.
Results
Sleep outcomes
At pre-treatment assessment the majority of participants (69.3%) had sleep disturbances, of which most were at a threshold level (Table 2). Specifically, 48.2% of participants in the total sample had threshold insomnia and 6.0% had threshold hypersomnia pre-treatment. Few participants reported threshold symptoms of both insomnia and hypersomnia (n = 16). Overall, participants had lower rates of threshold sleep disturbance immediately post-treatment and at the 6-month follow-up assessment; 27.7% of participants had subthreshold or threshold sleep disturbance at the 6-month follow-up.
Sleep disturbance across time points, classified as threshold and subthreshold symptoms of insomnia or hypersomnia, n = 166.
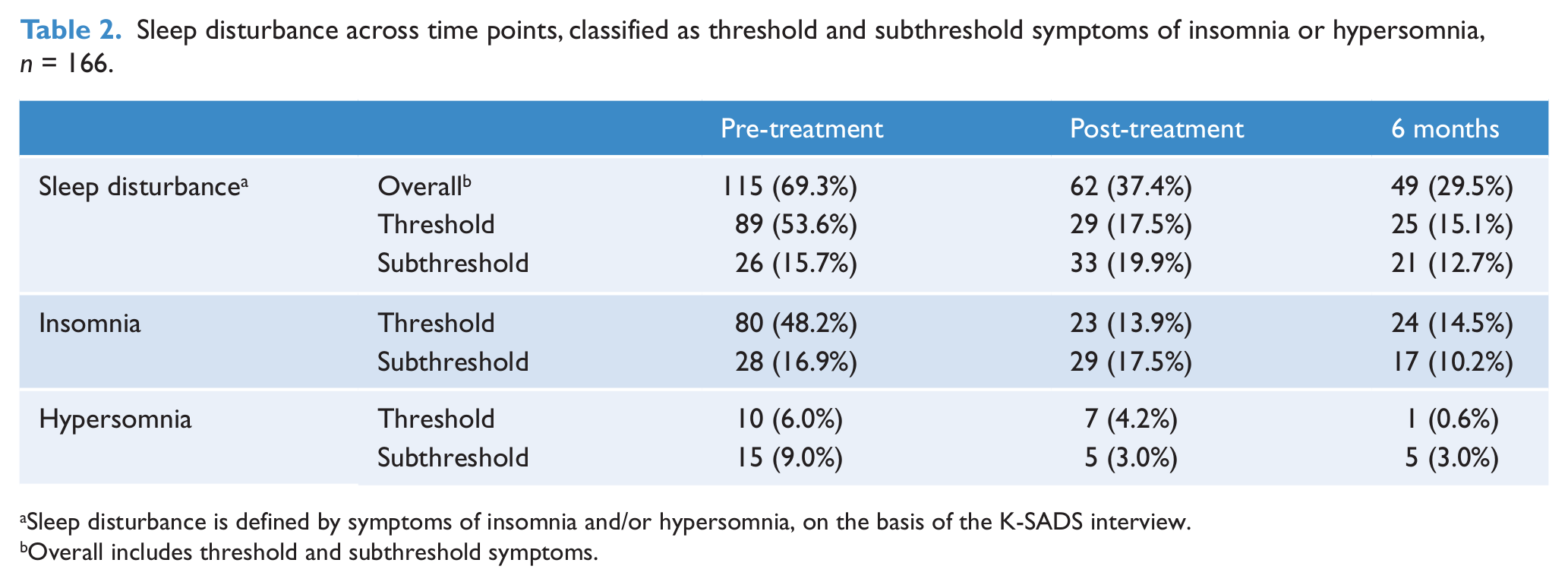
Sleep disturbance is defined by symptoms of insomnia and/or hypersomnia, on the basis of the K-SADS interview.
Overall includes threshold and subthreshold symptoms.
Relationships between sleep and depression
Of the 38 in the total sample who were classified as in full remission at post-treatment assessment, one (2.6%) had threshold sleep disturbance. In contrast, 10 (23.8%) of those in partial remission and 18 (48.6%) of those who were still depressed had threshold sleep disturbance post-assessment. At the 6-month follow-up, threshold sleep disturbance was present in only 9.2% of those who were in full remission compared with 39.1% of those in partial remission, and 58.8% of those who were depressed.
A random effects logistic regression model was used to investigate the association of depression status with sleep disturbance over time. Those in partial remission had 5.3 times the odds of threshold sleep disturbance of those in full remission, and those who were depressed had 25.1 times the odds of those in full remission. Treatment group, comorbid anxiety and gender did not show evidence of association with threshold sleep disturbance (Table 3).
Random effects logistic regression of threshold sleep disturbance on depression status, comorbid anxiety, gender and treatment group, over three time points.
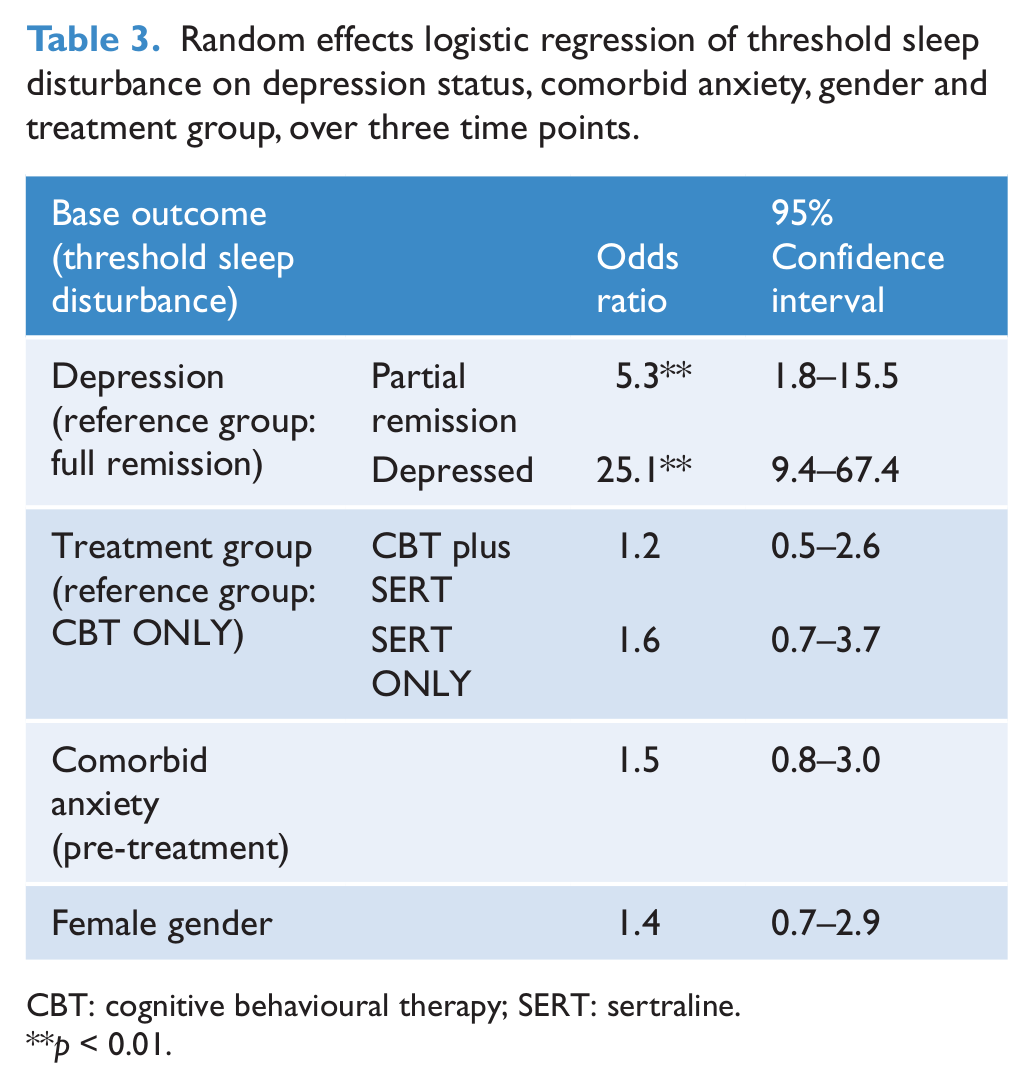
CBT: cognitive behavioural therapy; SERT: sertraline.
p < 0.01.
Persistent sleep disturbance as a predictor of treatment outcome
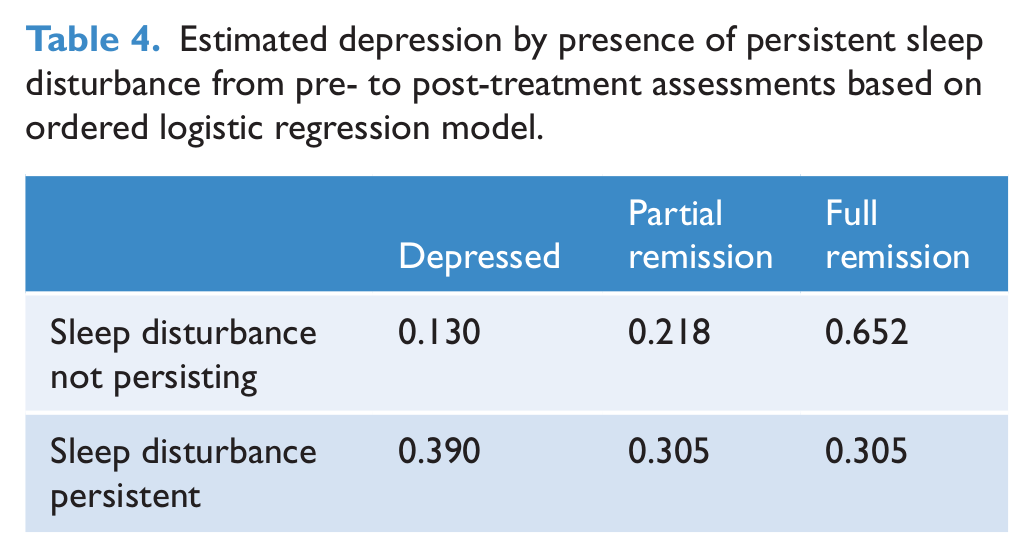
Depression status at the 6-month follow-up (full remission, partial remission, depression) was modelled via ordered logistic regression as a function of persistent threshold sleep disturbance at pre- and post-treatment, comorbid anxiety and treatment group. Depression status at the 6-month follow-up was positively associated with persistent threshold sleep disturbance at pre- and post-treatment (p = 0.001), but not associated with comorbid anxiety nor with treatment group. Predicted risks of depression, partial remission and full remission from the ordered logistic model are given in Table 4. For those with persistent threshold sleep disturbance the estimated risk of depression or partial remission at the 6-month follow-up is 0.70, while for those without persistent threshold sleep disturbance the risk of depression or partial remission is 0.35.
Estimated depression by presence of persistent sleep disturbance from pre- to post-treatment assessments based on ordered logistic regression model.
Discussion
Initial rates of insomnia and hypersomnia in this sample of adolescents with depression were similar to those reported in previous studies (Liu et al., 2007; Roberts et al., 2008). A large proportion of our sample (69.3%) had sleep complaints and the majority of these were deemed to be at threshold level. Although the proportion of individuals with sleep disturbances decreased markedly following treatment, sleep disturbances persisted in approximately half the sample up to the 6 months after treatment ended. In our study, a relatively small number of participants reported threshold symptoms of both hypersomnia and insomnia. Similar phenomenology has been reported in other studies, with approximately 10% of adolescents reporting both hypersomnia and insomnia (Liu et al., 2007).
We found that sleep disturbances were strongly associated with depressive state. Those who were depressed had 25 times the odds of having threshold sleep disturbance than those who were in full remission. Threshold sleep disturbances which persisted from pre- to post-treatment assessments were positively associated with depression at the 6-month follow-up. This information shows that clinicians should anticipate poorer treatment outcomes in depressed individuals who present with sleep disturbance. Strategies to optimise and individually tailor treatment programs should be developed (Horowitz and Garber, 2006; Kraemer et al., 2002) and these strategies may need to include treatment of sleep disturbance.
Treatment type did not appear to differentially affect sleep disturbance. Across time, patterns of sleep disturbance remained statistically similar between groups, and treatment type did not affect the relationship between sleep disturbance and depression in the ordered logistic regression. SSRIs may cause insomnia side effects in adolescents (McConville et al., 1996; Zisapel and Laudon, 2003); however, fluoxetine and paroxetine have more adverse effects in adolescents compared with sertraline (Armitage et al., 1997; Wilson and Argyropoulos, 2005). It is possible that the relatively low maximum dose of sertraline prescribed in this trial (100 mg) has contributed to this result as others (McConville et al., 1996) found trouble sleeping and drowsiness to be the most common side effects in a small sample of adolescents (n = 13). CBT has shown to improve subjective sleep outcomes and some objectively measured sleep variables (sleep efficiency, REM latency, REM density) in depressed adults (Buysse, et al., 1992; Thase et al., 1998) but few have investigated these effects in adolescents. These results prompt further consideration of sleep-related issues in the pharmacological and psychosocial treatment of adolescent depression.
We acknowledge that a limitation of this study was the lack of inclusion of specific sleep measures. Previous researchers have used various techniques (sleep and medical history questionnaires, sleep logs and semi-structured interviews) to measure subjective reports of sleep; however, there is much debate about which is the best method for measuring sleep (Libman et al., 2000). The findings of the present study suggest that standardised sleep questionnaires may be useful in depression trials, to enable more accurate assessment of the relationship between sleep disturbance and treatment outcome. Further, it is acknowledged that investigating the association between depression and sleep disturbance involves some redundancy (in that depressive disorder diagnosis may depend on the presence of sleep disturbance). Future studies may be able to address this issue.
As with all clinical trials, rates of attrition can be problematic. There were no significant differences in attrition rates between treatment groups even though group sizes were different at baseline. Follow-up assessments were offered to all participants who began treatment irrespective of treatment completion. In most cases treating clinicians completed assessments rather than independent raters blind to treatment allocation due to resource limitations. Independent raters may have reduced the risk of experimenter bias in assessments; however, independently rated self-report and parent-report measures produced broadly consistent findings with diagnostic interviews (Melvin et al., 2006). Over-endorsement of symptoms by adolescents that could potentially inflate the association between sleep and depressive disorder was not suspected given the proportion diagnosed with DD and DDNOS (40%). In addition, parents participated in diagnostic interviews about their teenager which would also limit any impact of adolescent over-reporting.
CBT focused on insomnia can help the patient to manage both sleep- and depression-related symptoms and change maladaptive cognitions about sleep (Carney et al., 2007; Lichstein et al., 2000; Morin, et al., 1994; Mystakidou, et al., 2009; Stepanski and Rybarczyk, 2006). Augmenting an antidepressant medication with a brief, symptom-focused CBT for insomnia may help to alleviate insomnia and improve treatment response long-term outcomes (Manber et al., 2003). However, these approaches are yet to be widely investigated in adolescents.
Optimal pharmacotherapies for depression would reverse the sleep abnormalities and concurrently improve subjective sleep disturbance. Further research into the sleep-related effects of antidepressants is warranted considering the interconnected neurobiology underlying sleep and depression. In this study, sertraline was not shown to have significant negative effects on sleep-related symptoms, and trends towards poorer sleep outcomes warrant further investigation.
Circadian disturbance also underlies the pathology found in affective disorders, and attention to improving circadian function will improve both daytime and night-time sleep-related symptoms (Monk et al., 1994). Sleep–wake behaviour can be improved by keeping regular daily routines, appropriately timed exercise and meal times, and allowing adequate sleep opportunity with good sleep hygiene (Boivin, 2000). These lifestyle issues are already part of common practice in the community treatment of depression. Light therapy for MDD in adults is an area that has been explored in recent years and novel light therapies are currently being developed for community and inpatient settings (Golden et al., 2005; Martiny, 2004; Wirz-Justice et al., 2005).
The findings in this study raise the need for aetiological and treatment studies that address the causes of sleep disturbances in depression, providing support for focused treatment of sleep disturbances in adolescent depression.
Footnotes
Funding
The study was funded by research grants from the Victorian Department of Human Services, beyondblue, the national depression initiative, National Health and Medical Research Council, and Monash University.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.