
Abstract
Objective:
Functional impairments are debilitating concomitants of psychotic disorders and are present early in the illness course and, commonly, prior to psychosis onset. The factors affecting social and role functioning in early psychosis (EP) following treatment are unclear. We evaluated whether six months of participation in the PREPR, Boston, EP treatment program, part of a public-academic community mental health center, was related to improvements in social and role functioning and whether premorbid adjustment in adolescence, baseline neurocognition, and depression symptoms predicted functional improvement.
Method:
The Global Functioning Social and Role scales, MATRICS neurocognitive battery, and Calgary Depression Scale were assessed at baseline and six months during naturalistic treatment, while premorbid adjustment was measured at baseline. All participants were psychotic disorder patients in PREPR (n = 46 with social functioning and 47 with role functioning measures at both time points).
Results:
Large improvements were observed in role functioning (d = 0.84) and medium to large improvements were observed in social functioning (d = 0.70). Models consisting of adolescent premorbid adjustment and change in depression symptoms predicted social and role functioning change, whereas neuropsychological functioning did not.
Conclusions:
Substantial improvements in social and role functioning were observed among this sample participating in a recovery-based EP program. The impact of clinical factors on social and role functioning was highlighted. Further studies of premorbid adjustment in adolescence and the treatment of depression in EP programs in controlled treatment trials are needed to confirm these findings.
Introduction
Functional impairments in social, occupational, and educational domains are often present premorbidly and during the prodrome to psychosis (Allen et al., 2005; Carrión et al., 2013; Cornblatt et al., 2003; Cornblatt et al., 2012; Meyer et al., 2014), and are quite prominent by the early phase of psychosis (Addington et al., 2006; Woods et al., 2009). They are among the most disabling components of psychotic illnesses (Wu et al., 2005). Accordingly, in attempting to ameliorate the impact of psychosis on functioning, there has been increased shift toward treating psychosis in earlier stages, including during the clinical high-risk phase. Substantial evidence indicates that early intervention leads to improved outcomes (Menezes et al., 2006; Preti and Cella, 2010).
Specialized clinical programs for early psychosis (EP) have been emerging over the past decade (Caplan et al., 2013) and it is important to evaluate outcomes of those programs. Several studies have assessed change in functioning in EP outside of specialized treatment programs (Austin et al., 2013; Goulding et al., 2010), whereas others have compared changes in functioning between samples receiving EP specific interventions with those receiving treatment as usual (Baksheev et al., 2012; Petersen et al., 2005). Few studies have reported on functional improvements from a clinic specializing in EP treatment in a community mental health center. Reports from ‘real world’ EP clinics have documented improvements in social (Addington and Addington, 2009; Malla et al., 2001; McGorry et al., 1996) and role (Addington et al., 2003; Iyer et al., 2010) functioning from baseline to follow-up. However, there is a paucity of research highlighting the factors that predict these improvements. In this paper, we address the extent to which improvements in functioning occur in a real world EP clinic and which factors predict changes in functioning.
Premorbid adjustment, neurocognition, and depression symptoms are three factors that have been linked with social and role functioning in individuals with psychosis. Regarding premorbid adjustment, declining social and role functioning is often detectable prior to the onset of psychosis (Allen et al., 2005; Monte et al., 2008). In their study of 95 EP subjects, Monte and colleagues reported significant deterioration in participants’ social abilities between childhood and early adolescence. They also found that poor premorbid adjustment during early adolescence, but not childhood or late adolescence, was associated with an earlier onset of prodromal symptoms. Whereas early adolescence appeared to be a critical period for social functioning, the sharpest role functioning declines were observed during late adolescence.
Neurocognition has also been closely tied to functioning in psychosis, as researchers have suggested that neurocognitive abilities are better predictors of functional changes than positive psychotic symptoms (Green, 1996; Leung et al., 2008; Malla et al., 2002). However, a lack of consensus exists concerning the strength of the neurocognition–functioning relationship in EP. This is particularly true in regard to social functioning, where there are a handful of studies with both positive (Malla et al., 2002; Milev et al., 2005) or null (Popolo et al., 2010; Stirling et al., 2003) associations. A significant relationship between neurocognition and role functioning has been more consistently reported, as there are considerably more positive (Dickerson et al., 2008; González-Blanch et al., 2010; Milev et al., 2005; Nuechterlein et al., 2011) than negative studies (Stirling et al., 2003; Tandberg et al., 2012).
Depression symptoms are a third factor related to functioning in EP. Depression often predates psychotic symptoms and can be an early signal of declining social functioning (Häfner et al., 1999; Cornblatt et al., 2003). Significant social functioning–depression associations have been observed in several EP studies (Chudleigh et al., 2011; Gorna et al., 2008; Goulding et al., 2010). In one study, scores on a depression scale predicted social functioning up to six years after initial screenings in 74 EP subjects (Gorna et al., 2008). There is also evidence that role functioning and depression symptoms are associated in EP (Rinaldi et al., 2010). A recent study comparing employed and unemployed EP groups found that depression was significantly elevated in the unemployed, but not currently employed, group (Tandberg et al., 2011).
Objectives and hypotheses
This study describes the clinical and demographic characteristics of the population in Boston’s Prevention and Recovery in Early Psychosis (PREPR) program, an intensive outpatient EP service (see Caplan et al., 2013 for a description of the PREPR treatment model). Our primary aim was to investigate whether clinician-rated social and role functioning, along with several clinician-rated and self-reported clinical variables, and neurocognitive functioning, improved following six months of treatment in PREPR. Our secondary aim was to identify predictors of improvements in social and role functioning. We sought to identify the best fitting models to predict change in both social and role functioning. Based on prior research, we expected a model consisting of premorbid adjustment in adolescence, baseline neurocognition, and reduction in depression to account for significant variance in social and role functioning change.
Method
Participants
PREPR is a public clinic that exists in the context of a longstanding academic collaboration with the Massachusetts Mental Health Center (MMHC). It is located within a diverse, urban setting and has a history of treating patients with a wide range of ethnic diversity, diagnoses, and co-morbidity. Participants were consecutively admitted adolescents and young adults. To be eligible for PREPR services, participants had to have an onset of psychotic symptoms in the three years prior to admission, be 16–30 years old, and participate in an intensive outpatient program involving individual therapy, group and family treatment, psychopharmacology with preventative health counseling, as well as case management and care coordination (see Caplan et al., 2013). The current study includes a mixed diagnostic EP sample; research designs using mixed samples often contain considerable heterogeneity and are an efficient method for describing populations commonly seen in community mental health clinics (Verdoux et al., 2002).
As part of the standard clinical protocol at PREPR, which is influenced by the research programs at MMHC, all clients completed an assessment battery at two time points (baseline, six months). Following approval by the Beth Israel Deaconess Medical Center and Massachusetts Department of Mental Health Institutional Review Boards, a PREPR clinician entered clinical outcomes data into a research database after removing all identifying information. To date, 153 clients have entered the clinic, including 78 who had some data on the functioning measures, of whom 46 completed the social functioning measure and 47 completed the role functioning measure at both time points. Thus, our main analyses of change focus on the 46 and 47 participants with baseline and six month follow-up assessments. When demographic and baseline clinical descriptors were compared for clients with and without functioning ratings at both time points, no baseline clinical characteristics differed significantly between groups. Participants who completed functioning measures at both time points were significantly less likely to be diagnosed with Schizoaffective Disorder, more likely to have a diagnosis of Major Depressive Disorder with psychotic features, and more likely to be working part-time or full-time at follow-up.
Functioning measures were added to the standard assessment a few years into the PREPR program. Reasons for not having functioning ratings at both time points included: client could not be scheduled within one month of clinical intake (n = 9), client dropped out of PREPR or could not be scheduled within one month of six month testing date (n = 14), client was not yet due for six month evaluation at the time of these analyses (n = 7), and data error on social functioning scale (n = 1). All clients with functioning ratings at two time points were involved with treatment at PREPR for a minimum of six months. All PREPR clinicians completing six month assessments were non-blinded to baseline scores.
Prior to testing, PREPR clinicians completed training on all battery measures. PREPR clinicians worked with clinical researchers who have 20 years of experience with clinical research of early psychosis patients. This work was concurrent with a large NIMH Center grant (L.J.S., principal investigator of the clinical core which used these instruments), and clinicians had contact with research staff. Regular meetings were held to discuss all clinical measures (e.g. functioning, depression) and to arrive at a consensus on ratings. For neurocognitive measures, weekly consensus meetings were held (see Measures for more information). In total, 16 raters collected data for this battery. To ensure reliability, ratings for all measures were checked by one PREPR clinician (Y.J.L.) and returned to raters in the event of any scoring errors.
Measures
The clinician-administered Global Functioning Scale: Social (GFS; Cornblatt et al., 2007) and Global Functioning Scale: Role (GFR) measures were utilized to assess social and role functioning. The GFS assesses age appropriate levels of social contact and friendships outside of the family and the GFR measures performance level and supports provided in a person’s primary role (typically school or work). Both are rated on 10-point scales, with greater scores representing higher functioning (see Figures 1 and 2 for additional scale information). Both scales have demonstrated high interrater reliability and construct validity in clinical high risk (Cornblatt et al., 2007) and EP (Piskulic et al., 2011) populations. Masters and doctoral level clinicians with experience in EP administered these measures after receiving training in their administration by EP experts, some of whom had participated in the NAPLS study in which these instruments were developed (M.F-Y., L.J.S.). Each participant’s primary clinician completed these scales; consensus for challenging cases was reached at staff meetings.
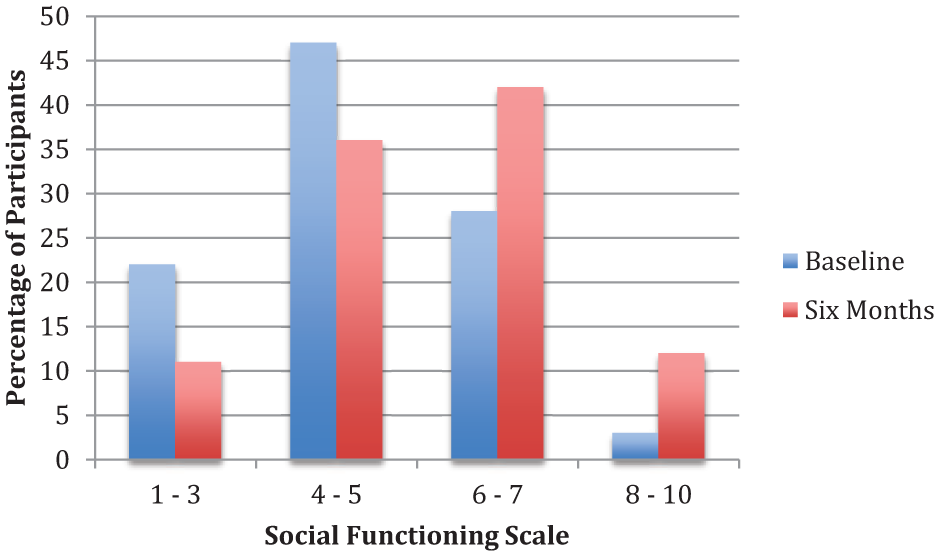
Distribution of social functioning (n = 46) ratings at baseline and after six months of treatment. 1 – 3: extreme social isolation to marginal ability to function. 4 – 5: major or severe impairment (< 1 friend). 6 – 7: moderate to mild impairment (⩾ 1 friend). 8 – 10: good to superior functioning.
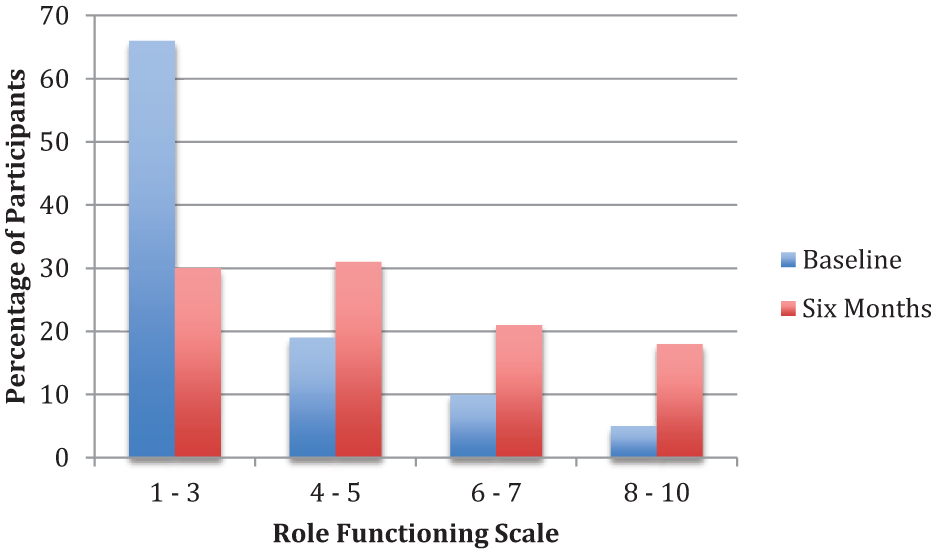
Distribution of role functioning (n = 47) ratings at baseline and after six months of treatment. 1 – 3: extreme dysfunction to marginal ability to function. 4 – 5: major or severe impairment. 6 – 7: moderate to mild impairment. 8 – 10: good to superior functioning.
The Premorbid Adjustment Scale (PAS; Cannon-Spoor et al., 1982, using modifications for EP from van Mastrigt and Addington, 2002) is a clinician-administered measure of functioning prior to onset of psychosis in several domains (social, interpersonal, academic, occupational) at four distinct time points: 1) Childhood (ages 6–11), 2) Early Adolescence (ages 12–15), 3) Late Adolescence (ages 16–18), and Adulthood (ages 19 and above). Ratings are calculated until one year prior to conversion to psychosis, with lower ratings indicating higher functioning. Clinicians made PAS ratings based on clinical interview and clinical record review.
The Calgary Depression Scale (CDS; Addington et al., 1993) is a 9-item structured interview that was used in this study to assess depression symptoms. For each item, clinicians rated symptoms on a 4-point scale, with greater scores reflecting more severe depression. The CDS was designed specifically to differentiate depression from negative symptoms in individuals with schizophrenia and has demonstrated good reliability and validity (Addington et al., 1993).
To assess neurocognition, the Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS; Nuechterlein et al., 2008) battery was utilized. Ten subtests are included in the MATRICS battery, which measure seven domains: processing speed, attention, working memory, verbal learning, visual learning, reasoning and problem solving, and social cognition. PREPR staff was trained in administering the MATRICS battery by experts in neurocognition in EP (M.F-Y., L.J.S.). Scoring issues were resolved in weekly meetings led by two staff psychologists under the supervision of M.F-Y. Raw scores are reported here instead of standard scores, as several participants were below age 20 (n = 13, age range, 16–19), which is the youngest age for which MATRICS norms have been reported.
Statistical analyses
Descriptive analyses were utilized to examine participant characteristics. Independent-samples t-tests were used to compare baseline characteristics between those who completed the functioning measures at follow-up with those who did not. All further analyses only included the group completing functioning measures at both time points (n = 47). Next, paired-samples t-tests were used to compare baseline and six-month data for clinical variables assessed at both time points. To control for multiple comparisons, an alpha level of .01 was used to determine significance for t-tests. Then, change scores were computed using linear regression by regressing baseline variables (independent variable) onto six month variables (dependent variable) and saving the residual scores. Finally, linear regressions were conducted to examine predictors of change in social and role functioning. Predictor variables were premorbid adjustment in adolescence (early/late; step one), baseline neurocognition (step two), and change in depression scores (step three). To reduce the number of analyses among neurocognitive subtests, an initial correlation matrix was conducted and neurocognitive predictor variables were selected based on a trend level relationship (p < .10) between baseline neurocognition and functional change. One neurocognitive subtest met the criteria for each model: spatial span demonstrated a significant relationship with change in social functioning, r = 0.35, p = .03, and symbol coding exhibited a trend level relationship, r = 0.28, p = .07, with change in role functioning. These subtests were entered into step two of corresponding models. After observing that neurocognition was not a significant predictor in any model, we conducted two post hoc analyses removing this variable and inserted change in depression into step two.
Results
Demographic and baseline clinical variables
Demographic and baseline clinical descriptors for participants are presented in Tables 1 and 2, respectively. The majority of diagnoses are on the Schizophrenia-spectrum. On average, participants developed prodromal symptoms in middle teenage years and sought treatment at PREPR two and a half years after initial onset of psychosis. At baseline, 69% of patients exhibited major social impairment and 85% exhibited major role impairment (see Figures 1 and 2).
Demographic data of early psychosis clients with functioning ratings at baseline and six months.
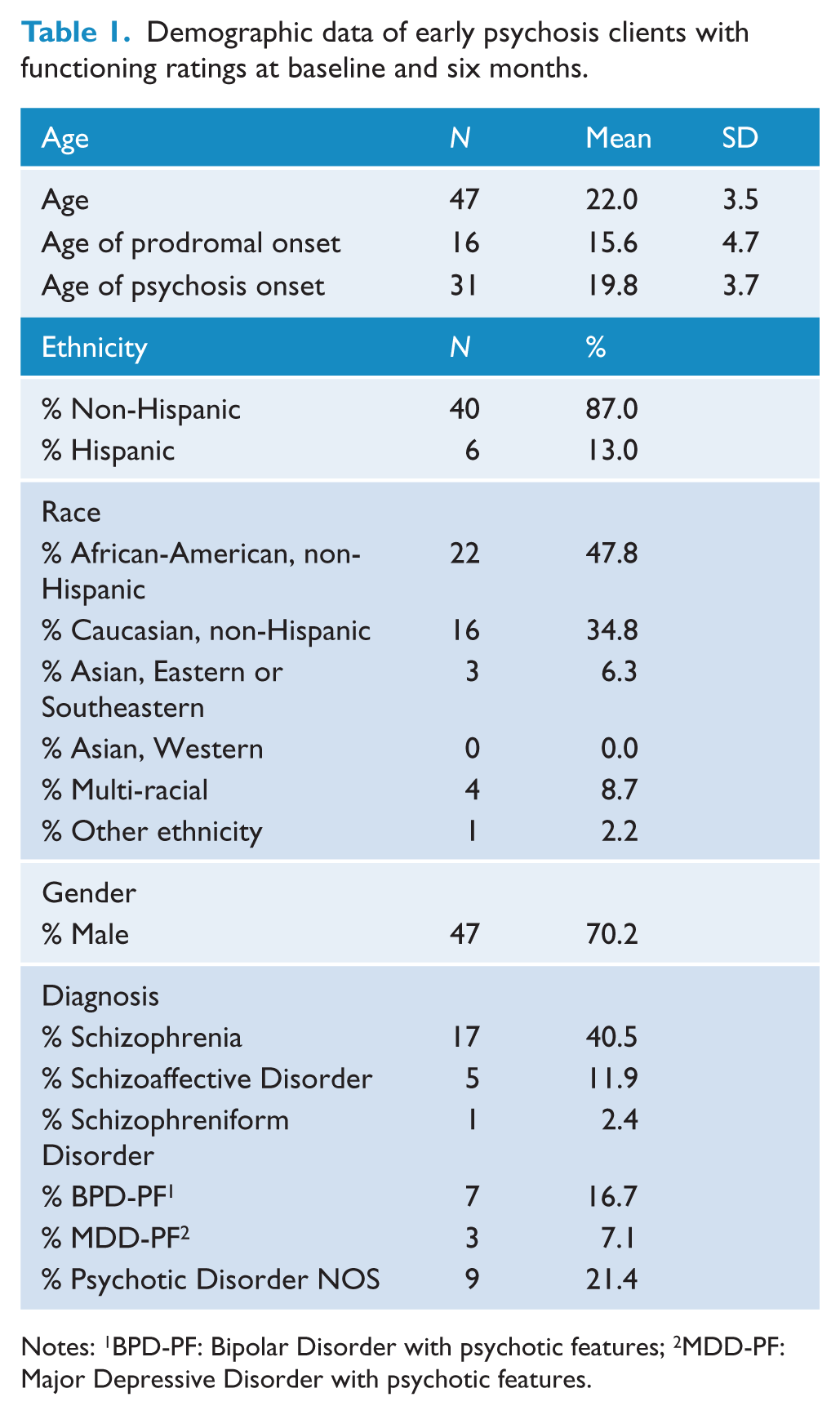
Notes: 1BPD-PF: Bipolar Disorder with psychotic features; 2MDD-PF: Major Depressive Disorder with psychotic features.
Baseline clinical data of early psychosis clients with functioning ratings at baseline and six months.
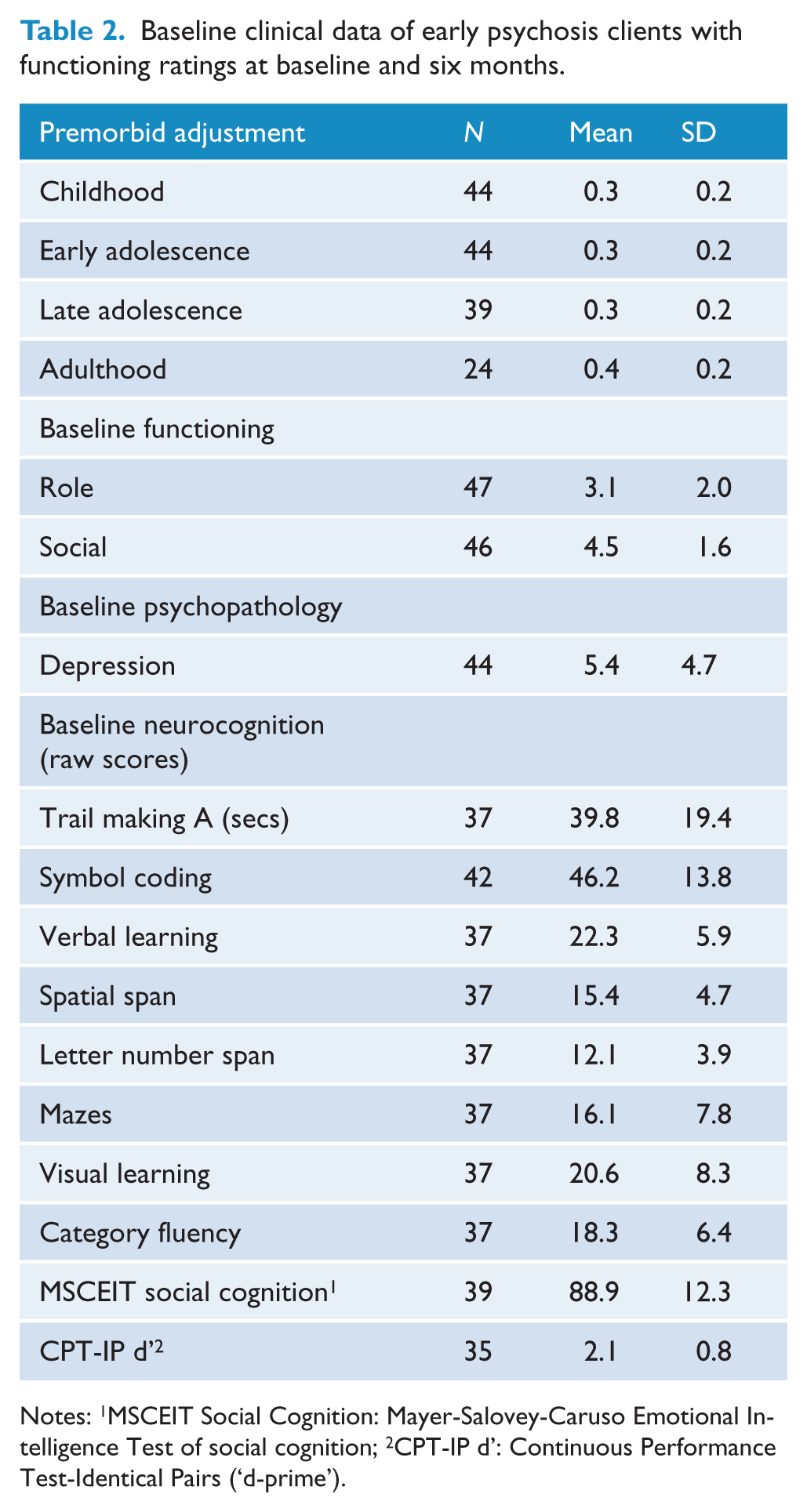
Notes: 1MSCEIT Social Cognition: Mayer-Salovey-Caruso Emotional Intelligence Test of social cognition; 2CPT-IP d’: Continuous Performance Test-Identical Pairs (‘d-prime’).
Changes in clinical variables at six months
Significant improvements from baseline to six months were observed in role functioning, t(46) = 4.88, p < .01, d = 0.84 and social functioning, t(45) = 4.16, p < .01, d = 0.70 (see Table 3; Figures 1 and 2 for score distributions). Some functional improvement was observed in two-thirds of participants, with approximately half of the sample exhibiting a two point or greater increase on GF scales. No significant differences between baseline and six month assessments were observed for neurocognitive subtests or depression symptoms.
Clinical data of early psychosis clients at baseline and after six months of treatment.
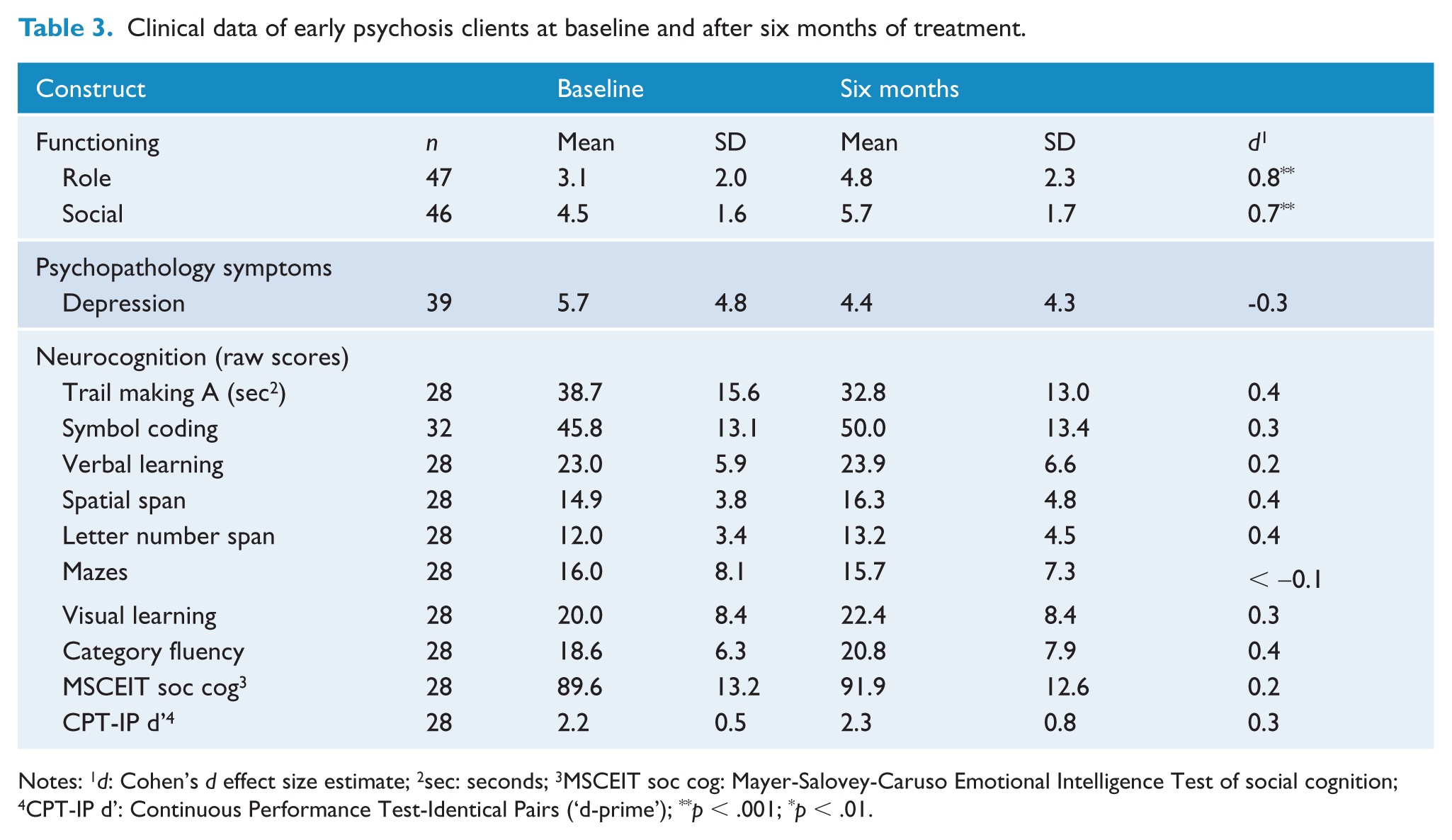
Notes: 1d: Cohen’s d effect size estimate; 2sec: seconds; 3MSCEIT soc cog: Mayer-Salovey-Caruso Emotional Intelligence Test of social cognition; 4CPT-IP d’: Continuous Performance Test-Identical Pairs (‘d-prime’); **p < .001; *p < .01.
Predictors of functional improvement in early psychosis
Our expectation that models consisting of premorbid adjustment in adolescence, baseline neurocognition, and change in depression would account for significant variance in the change in social and role functioning was not fully supported. Across models, baseline spatial span did not account for significant additional variance for change in social functioning when either early, β = 0.30, t(27) = 2.02, p = .06, or late adolescence, β = 0.27, t(25) = 1.73, p = .10, was entered as the first step. For change in role functioning, baseline symbol coding did not account for significant variance when either early, β = 0.20, t(29) = 1.27, p = .21, or late adolescence, β = 0.18, t(27) = 1.14, p = .27, was entered as the first step. Based on these findings, we conducted post hoc analyses removing baseline neurocognition as a predictor. The results indicated that premorbid adjustment in early and late adolescence and change in depression accounted for significant variance in change in social and role functioning (see Table 4).
Premorbid adjustment in adolescence and change in depression predict change in social and role functioning for early psychosis clients.
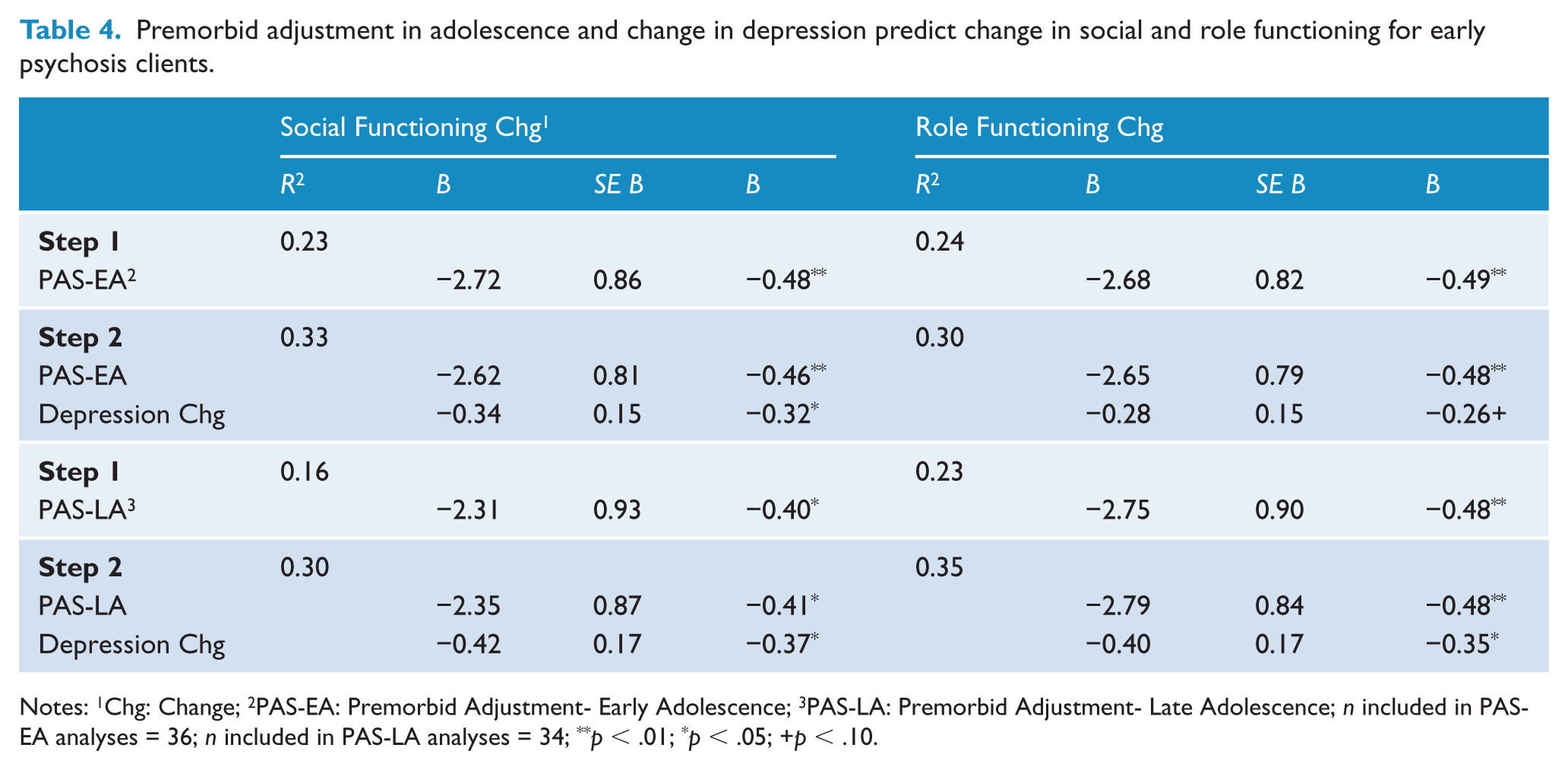
Notes: 1Chg: Change; 2PAS-EA: Premorbid Adjustment- Early Adolescence; 3PAS-LA: Premorbid Adjustment- Late Adolescence; n included in PAS-EA analyses = 36; n included in PAS-LA analyses = 34; **p < .01; *p < .05; +p < .10.
Discussion
Our primary goals were to examine whether social and role functioning improved following six months of specialized treatment for EP and, if so, which factors predicted improvement. Two key findings emerged. First, we observed significant improvements in social and role functioning. Second, although our initial model was not fully supported, we observed that significant variance in change in both social and role functioning was accounted for by premorbid adjustment in adolescence and change in depression scores once neurocognitive variables were removed from the model.
We expected that social and role functioning would increase following six months of treatment; however, the magnitude of improvement was surprising. Over 69% of patients exhibited major social impairment at baseline, and were unable to report having even one friendship. At follow-up, however, more than half of participants were able to identify at least one friendship. Improvements in role functioning were even more striking. At baseline, approximately two-thirds of clients exhibited extreme dysfunction, characterized by not being engaged in any structured weekly activities or, at best, functioning poorly in structured activities even with major supports in place. At six month follow-up, less than one-third of clients fell into this category, and over 40% were working or in school at least part-time. This suggests that participants benefitted from the treatment they received in PREPR, a specialized, recovery-based EP treatment program, although the lack of a control group prohibits drawing strong inferences regarding efficacy. Since the most profound functional deteriorations occur prior to or early in the course of psychosis (Häfner et al., 1999; Lieberman et al., 1992), recovery-based approaches focusing on EP may help mitigate the effects of psychosis on functioning. In support of this reasoning, many of the most promising functional outcomes for EP clients have also been found in clinics specializing in EP treatment (Addington et al., 2003; Malla et al., 2001; McGorry et al., 1996).
A previous mixed-sample design study of 257 EP participants helps provide context for our results (Tohen et al., 2000). In that study, Tohen and colleagues assessed symptoms and functioning in EP participants following their first psychiatric hospitalization and again six months later. Treatment was not controlled by the investigators and it is likely that few, if any, participants received treatment in an EP treatment program. They found that over three-fourths of subjects demonstrated reductions in symptoms, but that nearly two-thirds did not exhibit improvements in functioning. This is in sharp contrast with our results, where some functional improvement was found in over two-thirds of participants and a 2-point or greater increase on GF scales was found in approximately half of our sample. This suggests that treatment in a specialized EP clinic likely played some role in the functional improvements observed here.
To our knowledge, this was the first study to investigate the roles of premorbid adjustment and depression as predictors of functional improvement in EP participants. Our finding that models consisting of premorbid adjustment in adolescence and change in depression symptoms accounted for a third of the variance in change in social and role functioning is particularly meaningful from the standpoint of prevention and treatment. It points to the importance of identifying individuals experiencing declines in social and academic performance early, prior to the onset of psychosis. Early treatment is also key for reducing depression symptoms, which often predate psychotic symptoms (Häfner et al., 1999). For individuals who have developed psychosis, one suggested strategy is to treat affective symptoms at the outset, with the goal of increasing social functioning (Chudleigh et al., 2011; Cornblatt et al., 2003). This may be especially beneficial in EP populations, as their social networks often evolve considerably during this developmental period (Chudleigh et al., 2011).
Unexpectedly, baseline neurocognitive functioning did not predict functional changes. This was surprising, as researchers have demonstrated that neurocognitive functioning is a better predictor of functioning than psychotic symptoms in a substantial number of studies (Green, 1996; Leung et al., 2008; Malla et al., 2002; Milev et al., 2005) and there are only a handful of EP studies where a significant relationship was not observed (Stirling et al., 2003; Tandberg et al., 2012). Participants in this study showed few improvements in neurocognitive functioning between baseline and six months, especially when taking into account the practice effects that could have some role in many of these marginal improvements (see Nuechterlein et al., 2008). These results are in line with neurodevelopmental models of schizophrenia (Seidman, 1990; Weinberger, 1987), which suggest that those with psychosis experience a deterioration in neuropsychological functioning by their first episode of schizophrenia followed by a leveling off, or slight improvement, in performance once clinically stabilized (Mesholam-Gately et al., 2009).
A strength of this study is the unselected sample from a real-world, community mental health care setting, which is likely to be more reflective of the patients that clinicians encounter than those in a controlled clinical trial. This sample is also likely to have particularly severe impairments in a number of areas, including social and role functioning, as reflected in their low social and role scores at baseline. Although providing descriptive information for a community mental health cohort was a goal of this study, the use of a clinical population did impose some limitations. One limitation is that only a modest proportion of patients were tested at both time points, especially early in PREPR’s development, in part due to the inherent obstacles of conducting comprehensive assessments in a real-world clinic setting. This could raise concerns about the generalizability of this data; however, no significant differences were observed on any baseline clinical characteristic when PREPR patients with follow-up functioning ratings were compared to those without follow-up ratings. A second limitation related to this study’s clinic setting is that follow-up assessments were non-blinded. However, because the assessments were carried out as part of standard clinical practice over five years, patients and examiners were blind to the hypotheses of the subsequent research. Additionally, no long-term follow-up assessment was conducted. Although it is useful to compare clinical variables at baseline and six months, it would also be beneficial to examine whether improvements endured as participants continue their involvement in PREPR and after they leave the program. A third limitation is that we could not assess overall neurocognition in our analyses, given that the MATRICS does not have published norms for individuals less than 20 years old. Although raw scores were used here, age corrected scores would be ideal to control for the role of age on neurocognitive abilities in future studies. The absence of a negative symptoms measure or a more comprehensive instrument to assess psychotic symptoms is a fourth limitation. Though positive psychotic symptoms are not thought to be as predictive of functional improvement compared to other variables measured here, there is substantial evidence that negative symptoms are more strongly linked to functioning than positive symptoms in EP samples (Gorna et al., 2008; Goulding et al., 2010; Milev et al., 2005; Monte et al., 2008). PREPR recently introduced the Brief Psychiatric Rating Scale (Lukoff et al., 2002) to the clinical battery, in part, to address this limitation in future studies.
Finally, several avenues for future research should be mentioned. First, researchers ought to assess which treatment characteristics predict functional improvements. For example, examining how treatment attendance or specific interventions affect functioning (with medication adherence as a potential moderator) would be useful for both clinicians and researchers. Second, it will be useful to continue exploring the role of earlier intervention. Decreasing the duration of untreated psychosis is associated with better long term functioning (Perkins et al., 2005), so focusing on methods to identify individuals experiencing EP symptoms and those at risk for psychosis is critical. Third, continuing to delineate the relationship between functioning and neurocognition in EP is important, particularly with respect to specific neurocognitive domains and the relationship between neurocognition and symptoms. It is essential to continue to examine longitudinal relationships between functioning and many of the constructs measured here across the psychosis-spectrum (Carrión et al., 2013; Meyer et al., 2014). Doing so carries the promise of identifying potential clinical risk markers of psychosis and developing ways to improve long-term functioning in individuals with early and chronic psychoses. Finally, further study of the treatment of depression in EP programs in controlled treatment trials is needed to confirm these naturalistic findings.
Footnotes
Acknowledgements
We especially thank the patients and their families for working with us to build this program over the past decade or more. We thank as well the many faculty, staff, and trainees of the Massachusetts Mental Health Center and the Beth Israel Deaconess Medical Center Department of Psychiatry, and Massachusetts Department of Mental Health personnel for their contributions to building this program and carrying out assessments and treatment.
Funding
This work was supported in part by The Commonwealth of Massachusetts (SCDMH82101008006, L.J.S.) and the Sidney R. Baer Jr. Foundation (L.J.S.).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.