
Abstract
Objective:
The establishment of childhood adversities as risk factors for non-affective psychosis has derived a need to consider alternative interpretations of several psychosis-related factors. This paper sought to examine premorbid adjustment trajectories and social outcome factors in relation to childhood adversities. Perceived support has been found to decrease the risk of post-traumatic stress disorder, and we wished to compare perceived support in people with first-episode psychosis to non-clinical control persons and explore its relation to childhood adversities.
Method:
Every individual presenting with a non-affective first-episode psychosis (F20–29, except F21) in Region Zealand over a 2-year period was approached for participation and the 101 consenting participants were matched to 101 people with no psychiatric disorders. Comprehensive demographic data were collected. Assessment instruments included the Premorbid Assessment Scale, the Global Assessment of Functioning scale and the Childhood Trauma Questionnaire. The latter represented the childhood adversities in addition to parental separation and institutionalization.
Results:
There were no associations between number of childhood adversities and different social or academic premorbid trajectories. Those with more adversities had lower global functioning the year prior to treatment start and reported lower rates of perceived support during childhood along with less current face-to-face contact with family members. Lack of peer support remained a significant predictor of psychosis when adversities were adjusted for; peer support diminished the risk of psychosis caused by childhood adversities by 10%.
Conclusion:
Childhood adversities may not predict specific premorbid trajectories, but have an effect on global functioning when the psychosis has begun. Perceived support, especially from peers, may be important in the development of psychosis, and those with more adversities may represent a vulnerable subgroup who need more assistance to increase and maintain supportive networks.
Introduction
Childhood adversities are established risk factors for non-affective psychosis (Varese et al., 2012). They may well add knowledge to our interpretation of other recognized socio-environmental risk and outcome factors and to our developmental models of psychosis. These factors include premorbid adjustment, years of education, global functioning and occupational and living status. Deterioration of premorbid social and academic adjustment has most often been presented as evidence of an underlying neurodegenerative encephalopathy (Allen et al., 2013; Larsen et al., 2004), but recent findings suggest that it may additionally be affected by childhood adversities. One first-episode psychosis (FEP) study found that premorbid social adjustment was associated with childhood sexual and/or physical abuse (Conus et al., 2010) and a study of people with long-lasting psychosis found relations between childhood adversity and premorbid school and peer difficulties (Schenkel et al., 2005). Another FEP study found that childhood adversity was associated with poorer premorbid social and academic adjustment, though not with change in adjustment from childhood to adolescence (Stain et al., 2014). In addition, an FEP study exploring age of exposure of sexual and/or physical abuse found that early exposure (age < 12 years) was related to both childhood and early adolescence premorbid social adjustment, while late exposure (12–15 years) only associated with worse early adolescence premorbid social functioning (Alameda et al., 2015).
Childhood adversities have also been found to be associated with decreased educational achievement (Boden et al., 2007) and lower employment rates (Widom, 2000) in the general population. In the psychosis literature, the investigation of childhood adversities’ relation to other social factors has only just begun and the findings are mixed. One study of people diagnosed with schizophrenia found that childhood adversities were associated with current overall but not social functioning (Gil et al., 2009). The FEP study by Alameda et al. (2015) found that early (age < 12 years) but not late (12–15 years) sexual and/or physical abuse was related to worse social and occupational functioning, while a 66% non-affective psychosis FEP study found no associations between childhood adversity and social activity (Duhig et al., 2015). Another study of people diagnosed with schizophrenia found that only some parts of social functioning (role functioning and intimacy) was poorer for those with a history of childhood sexual abuse compared to those without (Lysaker et al., 2001).
Also with regard to occupational status, Conus and colleagues found in a large study of 658 patients with FEP that those with sexual and/or physical abuse had lower rates of employment/occupation (Conus et al., 2010), while two smaller FEP studies found no association between childhood adversity and current employment (Campbell et al., 2013; Duhig et al., 2015). A third small schizophrenia study found that those with childhood adversity were more likely to be employed (Spence et al., 2006). However, Spence et al. excluded people with post traumatic stress disorder (PTSD) who have been found to experience the highest rates of childhood adversity and to represent up to 39% (95% CI = [23, 55]) of an FEP sample (Bendall et al., 2012). Thus, the study has low representativeness. Equally unclear are the findings concerning educational achievement where two FEP studies have found weak or no associations between childhood adversity and years of education (Ramsay et al., 2011 and Ucok and Bikmaz, 2007). These findings reflect the need for clarification of childhood adversities’ relation to both educational attainment and global and occupational status in people with non-affective psychosis, to increase our understanding of these outcomes.
In addition, factors of resilience have the potential to explain why some and not others develop psychiatric disorders. A meta-analysis of risk factors for PTSD found that having social support in the period after the triggering trauma decreased the risk of developing PTSD (Brewin et al., 2000). Furthermore, a prospective birth-cohort study found that having received paternal support and affection in childhood protected against the development of various psychiatric disorders at age 16–18 years (Lynskey and Fergusson, 1997), though no effect was found for maternal support and affection. In the psychosis literature, social support has mainly been represented by the size of current networks, which have been found to be smaller for people with psychosis than for non-clinical populations (Gayer-Anderson and Morgan, 2013). Some evidence suggests that the smaller networks represent a lack of close relations and not a lack of acquaintances (Macdonald et al., 2000). Having close relations is very similar to having perceived support as the latter also refers to the presence of confidants. Thus, it seems that there is indirect evidence that people with non-affective psychosis have lower levels of current perceived support. The importance of this proposition was recently established by a study of people with delusions, which showed that good current relationships were associated with increased cognitive flexibility, which was related to decreased levels of delusional experiences (Jolley et al., 2014). Correspondingly, a large population study of people from the age of 16 found associations between current lack of objective and perceived support and delusion-like experiences (Saha et al., 2012). These data suggest that there may be a lowered rate of perceived support during childhood and adolescence in people with non-affective FEP. In addition, the family is one of the primary sources of current support for people with psychosis (Jolley et al., 2014), and it seems that a large part of the childhood adversities that people with FEP report happen in the home-environment (Trauelsen et al., 2015). This means that lack of family contact may not be entirely negative in individuals who have experienced familial trauma and may serve to protect the individual from further traumatic experiences or memories thereof. As any negative impact of childhood adversity could reveal a plausible mechanism for decreased perceived support and a possible intervention object, we wished to examine how current family contact related to childhood adversities.
This paper aimed to examine associations between childhood adversities and premorbid adjustment trajectories and social outcome in a larger FEP sample. Furthermore, it sought to explore whether perceived support in childhood and adolescence affected the risk of psychosis and how it related to childhood adversities and whether childhood adversities affected current family contact in the FEP group.
Hypotheses
Childhood adversities will be associated with poorer premorbid adjustment trajectories and poorer global functioning in the year prior to treatment in the FEP group.
Childhood adversities will be associated with poorer occupational and living status and fewer years of education in both the FEP and a non-clinical control group.
Perceived support is associated with a lower risk of FEP and is associated with childhood adversities.
Childhood adversities are related to current family contact in patients with FEP.
Method
Participants
FEP group
The sample has previously been described by our research group (Trauelsen et al., 2015, n.d.). Denmark has a nationwide early intervention program (OPUS) for people with FEP. Inclusion criteria for OPUS during the study were an International Classification of Diseases (ICD)-10 diagnosis F20–29, except F21, and an age of 18–35 years. Exclusion criteria were a previous diagnosis of non-affective psychosis. The catchment area was Region Zealand (population = 816,359) and everyone who was included in OPUS between 1 April 2011 and 1 April 2013 was approached for participation. Additional criteria for the study were sufficient Danish skills to complete the interviews.
Control group
Inclusion criteria were living in the catchment area and being 17 to 36 years of age. Exclusion criteria were previous or current psychiatric disorders and insufficient Danish skills to complete an interview. Control persons were matched 1:1 by gender, age (±1 year), and parental vocational education (±1 one on a 5-point scale). Control persons were recruited through advertisements in newspapers, at educational institutions, libraries and sport clubs and by word of mouth. They were included from 1 October 2013 to 22 May 2014.
Measures
Childhood adversity and perceived support
The Danish validated version of Childhood Trauma Questionnaire (CTQ) was used for adversity assessment (Bernstein and Fink, 2011). The CTQ consists of five subcategories, each represented by five questions. The CTQ subcategories were dichotomized to include adversities that were at least severe, as suggested by Bernstein and Fink (2011). Separation and institutionalization were assessed with the Childhood Experience of Care and Abuse Questionnaire (CECA.Q) (Bifulco et al., 2005; Smith et al., 2002). Separation that was primarily due to divorce was not included. Number of adversities ranged from zero to seven and was calculated by combining the five CTQ subcategories with separation and institutionalization. The assessed adversities included exposure before the age of 18 years. Perceived support during childhood and adolescence was also assessed with questions from the CECA.Q. They read ‘Did you have any adults you could talk to about your problems or feelings, as a child and teenager?’ and ‘Did you have any peers you could talk to about your problems or feelings, as a child and teenager?’
Sociodemographic data
Highest parental vocational education was chosen as a matching parameter due to its association with both childhood adversities and psychosis (Croudace et al., 2000; Sidebotham and Heron, 2006). It was measured on a 5-point scale. First-degree psychiatric illness included any psychosis, depression, bipolar and autism disorder and was assessed by interview.
Years of education referred to elementary school and high school and not vocational or university education. Family contact, living and occupational status were based on the Lehman Quality of Life Interview, translated by the The Early Treatment and Identification of Psychosis (TIPS) research group (Lehman, 1988; Melle et al., 2010). Family contact concerned the year prior to treatment and was assessed with a 5-point scale ranging from 1 (everyday) to 5 (never). Living status concerned status at treatment start and was assessed with a 4-point scale: 1 = Independent 2 = Independent w. support, 3 = Institution and 4 = Without housing. Occupational status was organized into three categories, namely 1= High level (working, studying or homeworking), 2 = Intermediate (available) and 3 = Low level (receiving welfare (pension or sick leave)).
Psychopathology
The operational criteria (OPCRIT) checklist for psychotic and affective illness diagnostic system was used to obtain ICD-10 diagnoses, based on patient records and a Positive and Negative Symptom Scales (PANSS) interview (Kay et al., 1987). The latter was extended to include life-long symptoms (McGuffin et al., 1991). Seventeen PANSS interview videos and vignettes were randomly drawn and rated by the four raters (A.M.T., J.E.J., M.B.P. and C.T.L.). For diagnoses, there was an overall agreement of 82% and a median kappa of 0.52.
Control participants were screened with the Mini International Neuropsychiatric Interview (MINI) 6.0 for any prior and present psychiatric diagnoses (Sheehan et al., 2008: 0).
Premorbid and current functioning
The Premorbid Adjustment Scale (PAS) (Cannon-Spoor et al., 1982) was used for assessment of premorbid social and academic adjustment. The PAS has shown good validity and reliability (Van Mastrigt and Addington, 2002). The social and academic parts of the scale have been found to be associated with different variables and are therefore recommended to be considered as independent factors (MacBeth and Gumley, 2008). Thus, all analyses were performed on social and academic scores independently. The different PAS periods are childhood (0–11 years), early adolescence (12–15 years), late adolescence (16–18 years) and adulthood (19 years). Several FEP studies have delineated these periods into trajectories to provide more dynamic functional categories in addition to average scores (Addington et al., 2013; Larsen et al., 2004). For the premorbid trajectories to reflect the whole premorbid period, we chose to define them as suggested by Larsen et al. (2004). This includes a premorbid period from birth up until 6 months before psychotic symptom onset or treatment instigation Larsen et al. (2004).
The Global Assessment of Functioning scale (GAF) was used to assess functioning the year prior to treatment entry and represents the best month of that year (Karterud et al., 1998; Pedersen et al., 2007). The interviewee provided this information and the assessor rated the level of functioning. We chose this measure instead of GAF at baseline, as it is more likely to represent a baseline level of functioning that is not affected by psychotic symptoms. Reliability for GAF 1 year was based on 17 randomly drawn cases and gave an intra-class correlation coefficient (ICC) (2,k) factor of 0.82 (0.60–0.93), which corresponds to excellent reliability (>0.75).
Ethics
All participants received oral and written information about the study. For the FEP participants, it was clearly stated that they could withdraw their consent at any time, and that participation did not impact their treatment. Control participants received DKK 400 equal to EURO 54 as compensation for their time and contribution. The protocol was submitted to the Regional Ethics Committee and pre-approval was found unnecessary as it only implicated questionnaires and interviews. The Data Protection Council, Region Zealand, approved data management (journal no. 12-000660).
Statistical analysis
Frequency graphs for continuous measures were inspected visually to determine the approximation of the normal distribution and Levene’s test was used to determine equality of variance for group comparisons. The Student’s t-test and the Mann–Whitney U test were used for comparisons between the FEP and the control group. Spearman Rank Correlation analyses were performed for all variables. All significance tests were two-tailed and the α-level set at 0.05.
The K-Means cluster analysis was applied for the identification of groups based on premorbid social and academic change. The K-means cluster analysis seeks to create groups with minimal difference within groups relative to between groups. As suggested by Larsen et al., the clusters were identified by change from childhood to the last PAS score. The ratings in childhood were labeled good (<1.50), intermediate (1.50–2.99) or poor (⩾3.00), while the changes were labeled stable (<1.00), slightly deteriorating (1.00–1.99) and clearly deteriorating (>2.00) (Larsen et al., 2004). The change values were standardized for the modeling and there were no clear outliers. The best number of groups was based on the number of distinct patterns identified by the analyses, as suggested by (Larsen et al., 2004).
Analysis of variance (ANOVA) and the Kruskal–Wallis test (for non-normal distributions of the number of adversities) was performed to test for differences between the groups on number of adversities. The IBM SPSS Statistics for Windows, Version 22.0 was used for all analyses.
Results
Sample characteristics
We included 101 (48%) out of 198 eligible FEP participants. The reasons for the nonparticipation were unwillingness to participate (N = 51) or to finish the line of interviews (N = 14), inability to obtain contact (N = 18), poor Danish skills (N = 3), and inclusion before the CTQ was included in the protocol (N = 11). This paper had additional missing data for 21 people due to the premorbid adjustment: 14 had such an early onset of psychosis that no trajectory could be calculated and seven had incomplete data assessment. When combining those without PAS with those who were excluded, the remaining group (N = 80) was 1.5 years younger (Mann–Whitney U 3750, p = 0.013), had fewer females (19% compared to 46%, χ2 = 15.3, p < 0.01) and more diagnoses of schizophrenia (93% compared to 70%, χ2 = 18.2, p = 0.01). The FEP participants were assessed as soon as possible. The median time from treatment start to assessment was 94 days (range 456 days). Forty-one percent were psychotic in the week prior to either the first or second interview, defined as a score of at least four on the PANSS. The sample characteristics are represented in Table 1.
Sociodemographic and baseline data for persons with first-episode psychosis (N = 101) and matched control persons (N = 101).
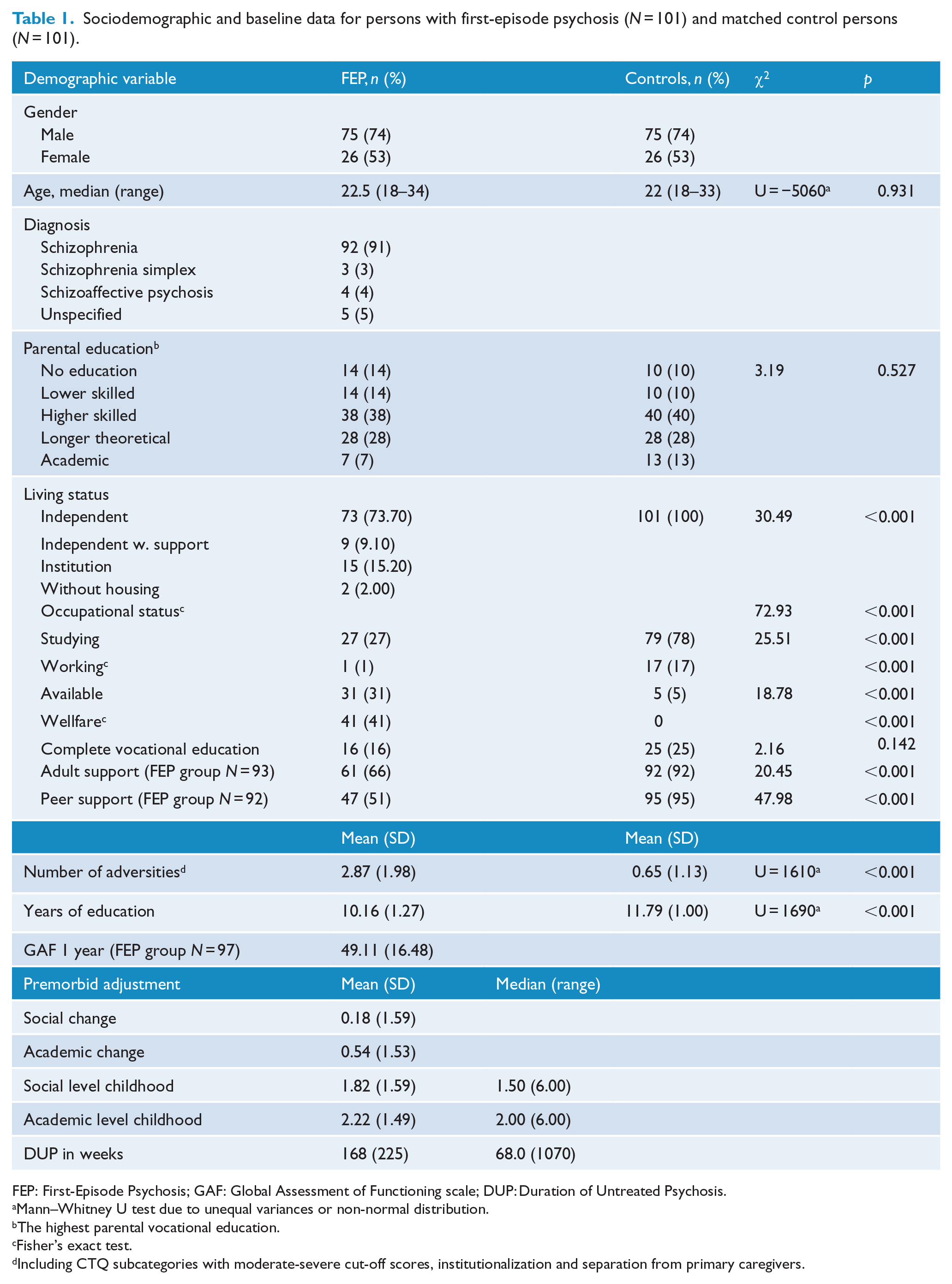
FEP: First-Episode Psychosis; GAF: Global Assessment of Functioning scale; DUP: Duration of Untreated Psychosis.
Mann–Whitney U test due to unequal variances or non-normal distribution.
The highest parental vocational education.
Fisher’s exact test.
Including CTQ subcategories with moderate-severe cut-off scores, institutionalization and separation from primary caregivers.
Premorbid trajectories and social factors
The K-mean cluster analyses identified three groups for social premorbid adjustment and four groups for academic. The premorbid trajectories are depicted in Figures 1 and 2. The social groups were (1) good stable (N = 45), (2) good, clearly deteriorating (N = 19) and (3) poor, slightly improving (N = 16). The academic groups were (1) intermediate stable (N = 38); (2) good, clearly deteriorating (N = 11); (3) poor, clearly improving (N = 4) and (4) good, slightly deteriorating (N = 27). There were no statistically significant differences in the number of adversities between the FEP groups based on premorbid social adjustment, F(2,77) = 1.460, p = 0.24, or premorbid academic adjustment, χ2(3, N = 80) = 4.46, p = 0.22. These analyses are represented in Table 2.
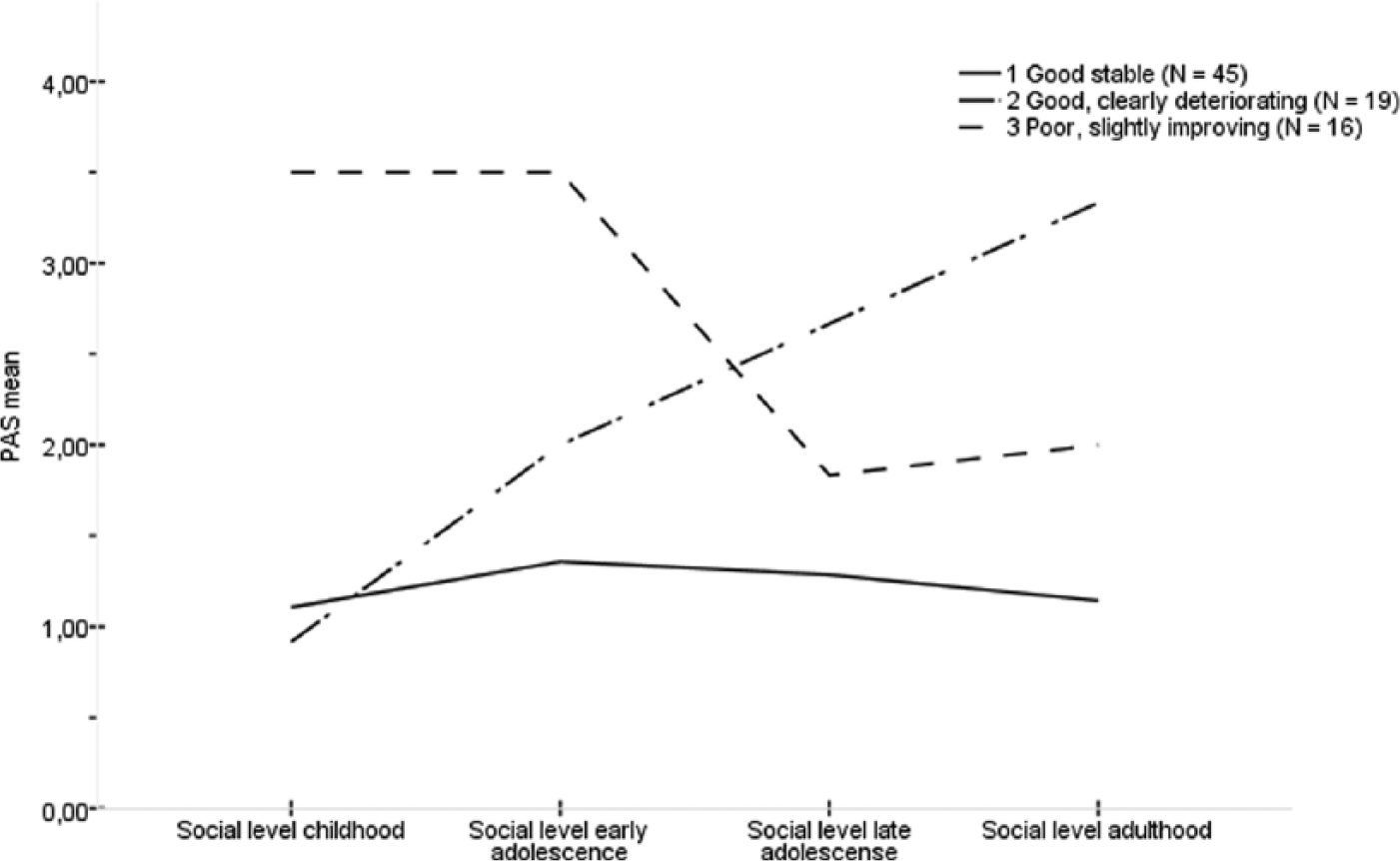
Premorbid Adjustment Scale (PAS) trajectories for the social clusters (N = 80).
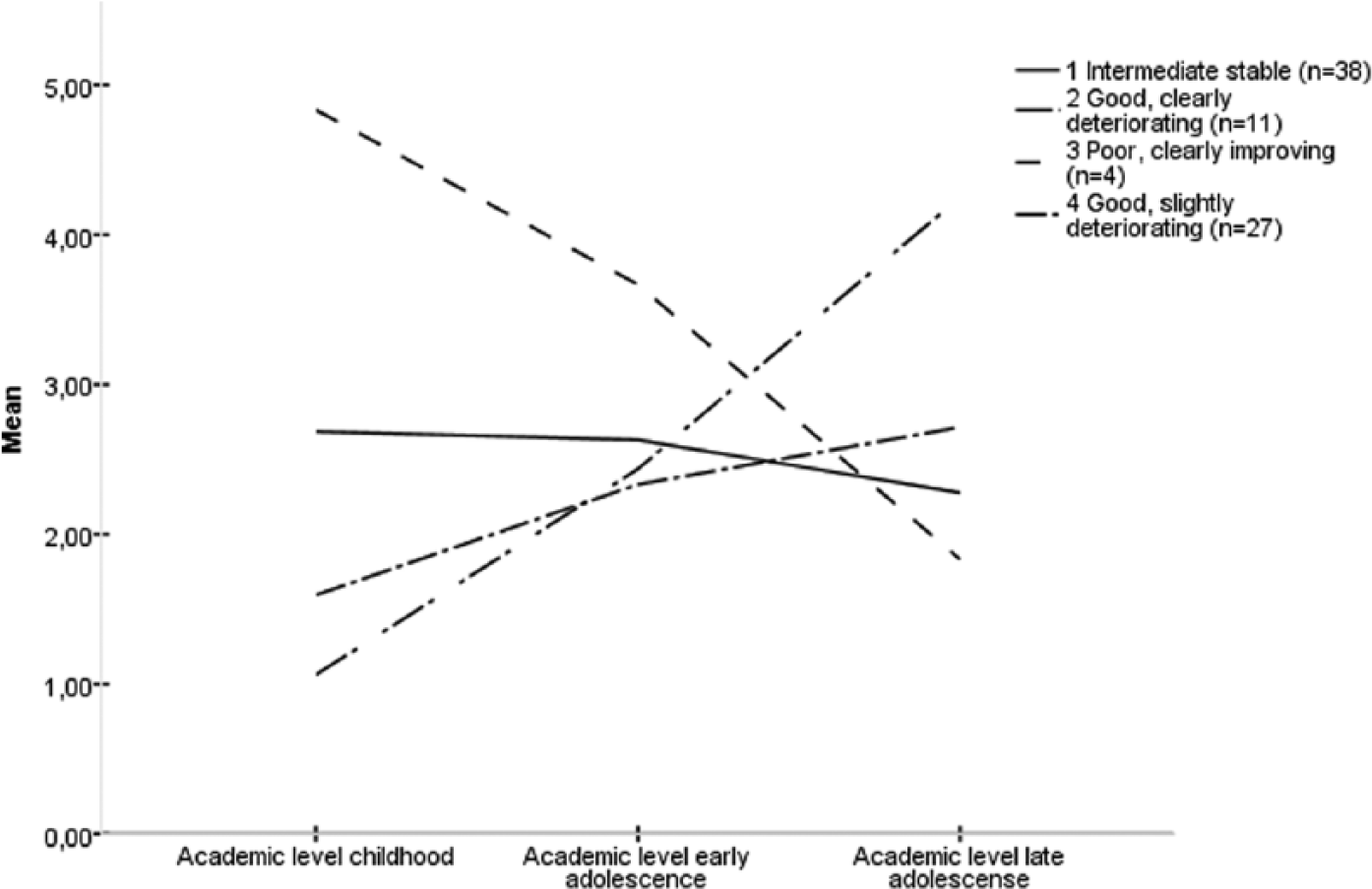
Premorbid Adjustment Scale (PAS) trajectories for the academic clusters (N = 80).
Number of adversities in the groups based on social premorbid adjustment (PAS) change (N = 80) and on academic premorbid adjustment (PAS) change (N = 81).
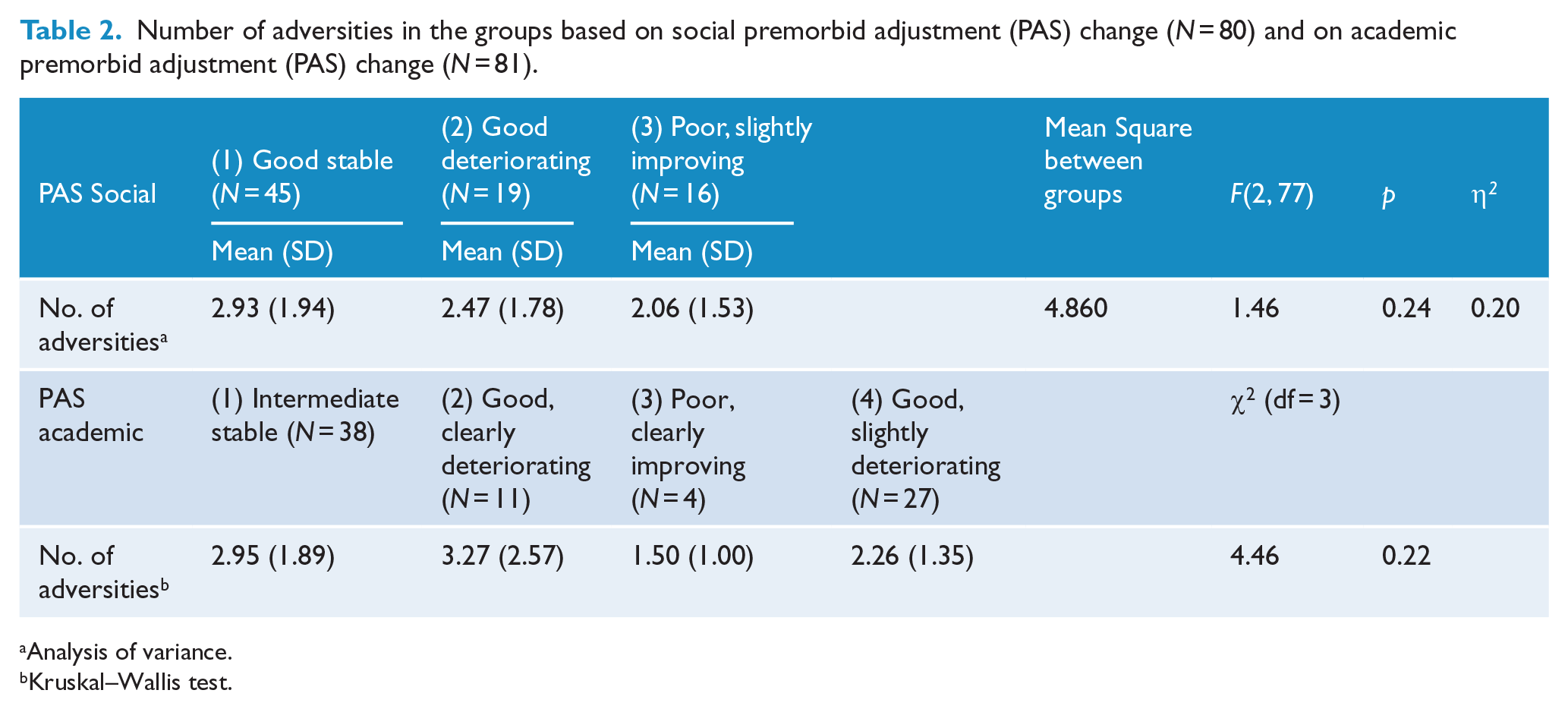
Analysis of variance.
Kruskal–Wallis test.
For both the FEP and the control group, there were no associations between number of adversities and years of education, rs(100) = 0.05 and rs(99) = −0.07, current occupational, rs(100) = 0.06 and rs(99) = −0.06, and living status, rs(98) = 0.18. In the FEP group, GAF function 1 year was negatively correlated to the number of childhood adversities, rs(97) = −0.22, p = 0.04, so that more adversities were related to worse functioning the year prior to treatment. The missing data here were due to incomplete data assessment. The correlation analyses are represented in Tables 3 and 4.
Associations between premorbid adjustment, childhood adversities and social outcome factors in the FEP group (N = 72–101).
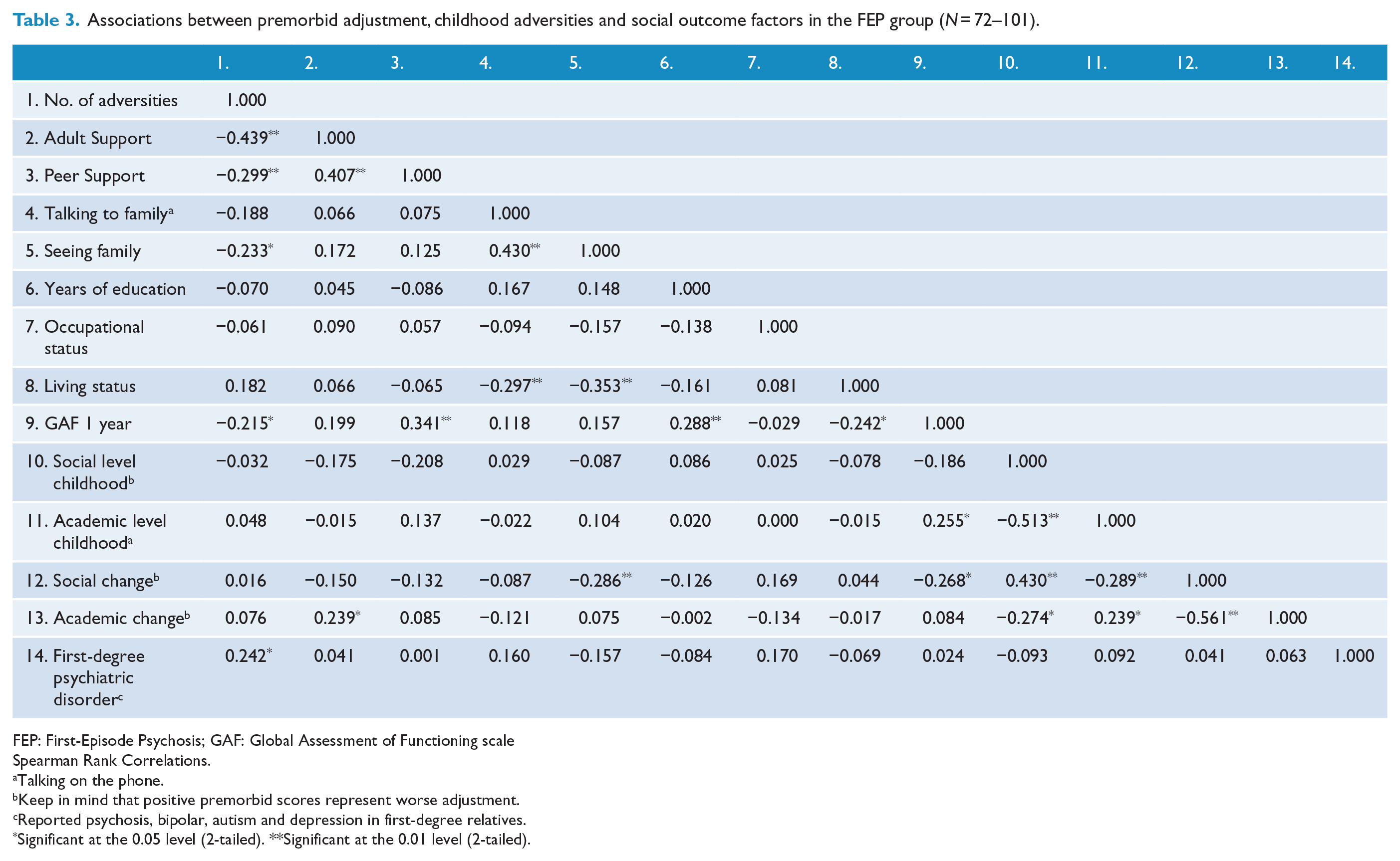
FEP: First-Episode Psychosis; GAF: Global Assessment of Functioning scale
Spearman Rank Correlations.
Talking on the phone.
Keep in mind that positive premorbid scores represent worse adjustment.
Reported psychosis, bipolar, autism and depression in first-degree relatives.
Significant at the 0.05 level (2-tailed). **Significant at the 0.01 level (2-tailed).
Associations between childhood adversities and social factors in the control group (N = 93–101). a
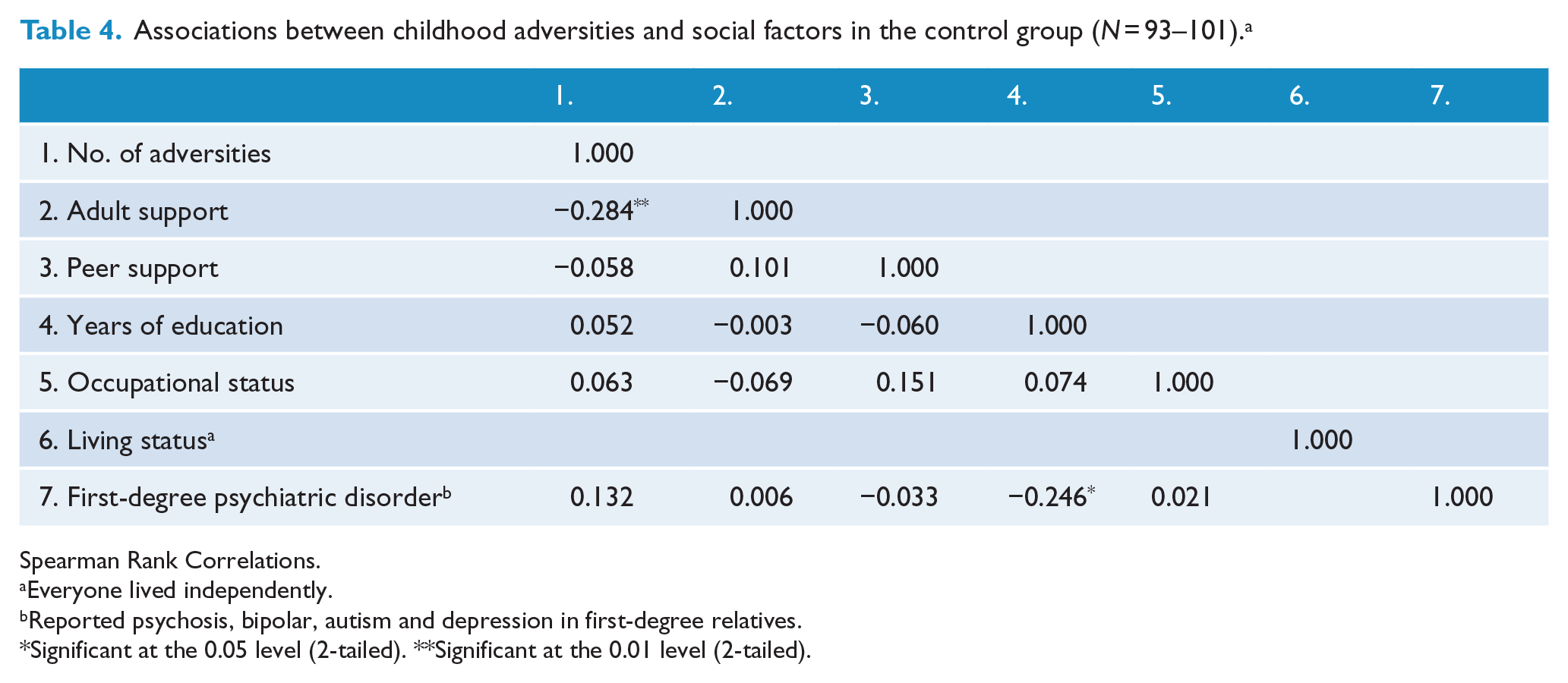
Spearman Rank Correlations.
Everyone lived independently.
Reported psychosis, bipolar, autism and depression in first-degree relatives.
Significant at the 0.05 level (2-tailed). **Significant at the 0.01 level (2-tailed).
Perceived support and family contact
The FEP group reported lower rates of peer and adult support during childhood and adolescence than the control group (p < 0.001). This is represented in Table 1. Forty-four percent of the FEP group reported having had both peer and adult support compared to 88% of the control group, and 24% of the FEP group and 1% of the control group reported having had neither. Number of adversities was negatively correlated with adult support for both the FEP, (rs = −0.44, p < 0.01) and the control group (rs = −0.28, p < 0.01), while it only correlated negatively with peer support in the FEP group (rs = −0.30, p < 0.01). When perceived support was adjusted for number of adversities, only peer support remained significantly lower in the FEP group, odds ratio (OR) = 0.12, p < 0.001. When number of adversities was adjusted for adult and peer support, it remained significantly higher for the FEP group (ORs = 2.64 and 2.30, p < 0.001), but peer support diminished the risk caused by childhood adversities by 10%. There were no significant interactions between the number of adversities and perceived support. Perceived support analyses are represented in Table 5. There was a negative correlation between number of adversities and face-to-face contact with a family member, rs (97) = −0.23, p < 0.05, but not telephone contact, rs (97) = −0.19, NS, in the FEP group. Family contact correlations are represented in Tables 3 and 4.
Perceived support and adversities during childhood and adolescence on risk of psychosis in persons with FEP (N = 92/93) and non-clinical control persons (N = 100).
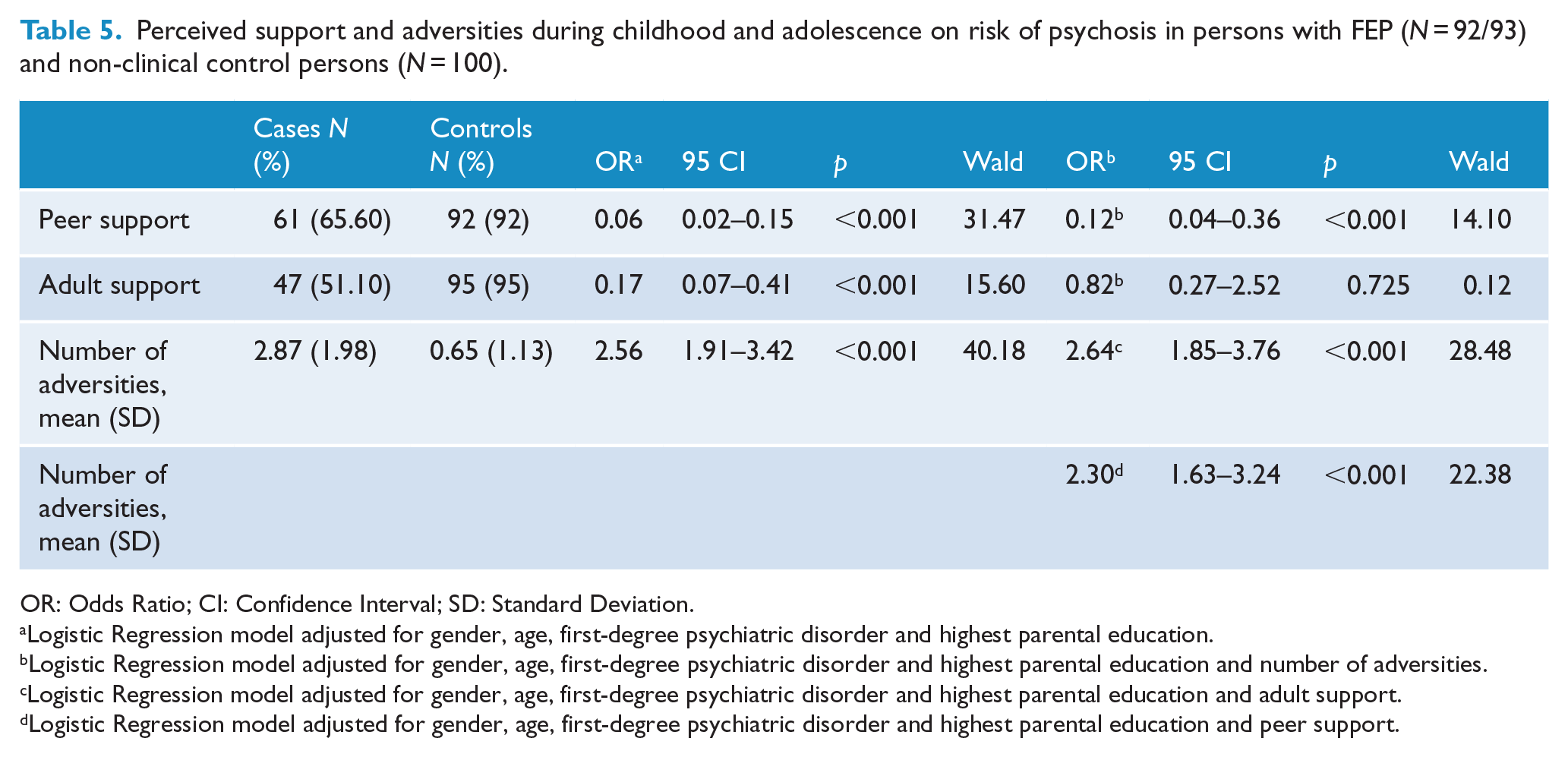
OR: Odds Ratio; CI: Confidence Interval; SD: Standard Deviation.
Logistic Regression model adjusted for gender, age, first-degree psychiatric disorder and highest parental education.
Logistic Regression model adjusted for gender, age, first-degree psychiatric disorder and highest parental education and number of adversities.
Logistic Regression model adjusted for gender, age, first-degree psychiatric disorder and highest parental education and adult support.
Logistic Regression model adjusted for gender, age, first-degree psychiatric disorder and highest parental education and peer support.
Discussion
This study explored childhood adversities in relation to premorbid and current social factors and perceived support in people with non-affective FEP and a matched control group. We hypothesized—but did not find—that those with worse premorbid trajectories had experienced more childhood adversities. Childhood adversity was not associated with occupational or living status or years of education. Lack of perceived peer support during childhood and adolescence increased the risk of psychosis independent of childhood adversities and peer support diminished the risk of psychosis caused by childhood adversities. In addition, those with more childhood adversities had less current face-to-face contact with their family.
Premorbid trajectories and social outcome factors
We hypothesized but did not find that those with worse premorbid trajectories had experienced more childhood adversities. Our hypothesis was based on studies that found childhood adversity to be associated with worse premorbid adjustment in different premorbid time periods and on average (Alameda et al., 2015; Conus et al., 2010; Schenkel et al., 2005; Stain et al., 2014) along with the rational consideration that severe adversity would decrease functioning. The most established theory, however, is the neurodevelopmental, which considers premorbid deterioration to be a sign of decreasing brain function, which in turn is thought to be caused by genetic or biological factors. To explore this theory, we performed a post-hoc test to see if first-degree psychiatric illness was associated with deterioration. We found no differences between the groups based on social, χ2(2, N = 70) = 2.81, p = 0.25, and academic adjustment, χ2(3, N = 69) = 1.83, p = 0.61. Thus, both childhood adversities and familial risk were equally distributed across the identified trajectories, suggesting either a complex, or no relation between the factors. There are a few reasons why childhood adversity may not cause a deteriorating trajectory. For example, cessation of adversity could cause temporary functional improvement, which is supported by a longitudinal study by Kelleher et al. (2013) who found that the amount of psychotic experiences decreased in accordance with bullying and physical abuse. Other reasons include the recognition of academic difficulties with an instigation of adequate assistance. However, it is also possible that we found no relation between childhood adversity and premorbid trajectories because we were unable to take age at adversity into consideration. This is supported by the FEP study of Alameda et al. (2015) who found that early (before age 12) but not late (age 12–15) sexual and/or physical abuse related to childhood premorbid adjustment. Therefore, it is possible that a relation also exists with the premorbid trajectories if we take age of adversity into consideration.
As hypothesized, we found that having experienced more childhood adversities was associated with a lower level of global functioning. Global functioning represents the best consecutive month the year prior to treatment onset (average age = 22 years) and thus differs from premorbid adjustment, which ends 6 months before the onset of psychotic symptoms (average age = 17 years). In addition to the few and mixed findings from previous studies (Addington et al., 2013; Alameda et al., 2015; Duhig et al., 2015; Gil et al., 2009; Lysaker et al., 2001), our results suggest that further research is needed to establish whether childhood adversities predict worse global functioning in people with FEP. The Alameda et al. (2015) study found that early (before age 12) and not late (12–15 years) sexual and/or physical abuse was related to worse GAF functioning at baseline and through 3 years’ follow-up (Alameda et al., 2015). Thus, it is possible that age at adversity plays an important role for this relation too, and that future studies may find an impact for global functioning the year prior to treatment onset if this approach is applied.
The lack of associations between number of adversities and educational length, current occupational and living status was against our assumptions. The occupational status finding was similar to two studies (Campbell et al., 2013; Duhig et al., 2015) and dissimilar to two studies who found negative (Conus et al., 2010) and positive effects of childhood adversity (Spence et al., 2006). The dissimilarities may be due to study designs. Conus et al. was a file-audit study that included sexual and physical abuse, which makes their analysis very different from ours and their results less comparable. It is possible that their group with no sexual/physical abuse had been exposed to other childhood adversity, which could have given different results. Spence et al.’s group consisted of people with non-FEP and a mean age of 43 years who had been service-users for an average of 15 years. It is likely that occupational status was severely affected by the different interventions people had received, which again is very different from our study group. Thus, it may be that occupational status is not affected by childhood adversities in people with FEP.
With regard to livings status, any effect of childhood adversities may have been overshadowed by previous institutionalization in childhood and adolescence. If a young person in Denmark is institutionalized at age 18 years, he/she has the right to receive comparable housing until the age of 23 years. This hypothesis is supported by a post-hoc analysis that showed a significant correlation between living status and institutionalization, rs(95) = 0.35, p < 0.01. It is also possible that any relation between childhood adversities and years of education were affected by the Danish social system, which highly prioritizes assistance to those with special needs and is considered to be equitable (Education Policy Outlook Highlights: Denmark—OECD, n.d.: 6; 16). In order to be certain that childhood adversities do not affect years of education, occupational and living status, more comprehensive and preferably longitudinal studies of non-affective FEP are needed.
Social support
Perceived peer and adult support during childhood and adolescence decreased the risk of psychosis and thus may add knowledge to our current models of psychosis. Half of the FEP group reported having had no peer support compared to 5% of the control group, which corresponds to an unadjusted 17 times (1/0.06) increased risk of psychosis by the lack of peer support. It means that half of the FEP group felt they had no peers to talk to about emotions and problems for the majority of their childhood and adolescence. Peer support alone remained a significant risk factor when childhood adversity was adjusted for, suggesting it is more independent of childhood adversity than adult support is. Peer support decreased the risk of psychosis caused by childhood adversities by 10%, while adult support did not change the risk. Thus, there was a buffering effect of having peer support during childhood and adolescence. Neither type of support interacted with childhood adversities. Thus, we did not find a diminishing effect of social support with increasing adversity severity, as it has been found for adult social support on trauma symptomatology and PTSD (Evans et al., 2013; Scarpa et al., 2006).
Adult support represented having any adult, within or outside the family, to talk to about problems and feelings. One-third of the FEP group reported lack of adult support, compared to 8% of the control group, which corresponds to a six times (1/0.17) increased risk of psychosis by the lack of adult support. Children use their parents for support and most of the assessed adversities happened within the home-environment (Trauelsen et al., 2015), making it likely that these factors were associated. It may have been difficult to obtain support in an abusive and/or neglectful home environment (Jansen et al., 2015) and it is possible that there was a conceptual overlap between adult support and adversity. Adult support was correlated with number of adversities, post-hoc analysis: rs(93) = −0.44, p < 0.01. Of the CTQ subcategories, we found that emotional neglect had the highest association with adult support, post-hoc analysis: rs(93) = −0.48, p < 0.01, and that one of the questions regarding emotional neglect read, ‘My family was a source of strength and support’. No other CTQ question directly concerned support, so the overlap could at most have represented a fifth of emotional neglect and none of the other subcategories. Thus, it seems that co-occurrence is the more likely explanation for the association between adversity and adult support. It may have represented a similar increase in feelings of hopelessness and social defeat as peer support. We have found no studies that examine perceived support and adversities during childhood and adolescence in people with psychosis, but an 18-month follow-up population study found that having a small primary support group increased the risk of psychotic symptoms independent of adversity (Wiles et al., 2006). Peer support only correlated with one CTQ subcategory—post-hoc analysis: emotional neglect, rs(92) = −0.26, p < 0.05.
As hypothesized, those in the FEP group with more childhood adversities saw their family less at the time of treatment entry, suggesting that adversities may have affected these relationships. It is plausible that childhood adversity that has not been dealt with and may even still be happening to some degree makes it difficult to see the family. A qualitative study of our FEP group actually found that some mention that it can make them feel bad to spend time with their family (even though they love them) (Jansen et al., 2015).
Strengths and limitations
A cross-sectional and retrospective study design has certain limitations. Causal relationships are difficult to establish and recall bias are likely to occur. Recall bias could especially have affected premorbid adjustment, childhood adversities and perceived support in our study, as these factors represent the entire childhood. Studies have found that people with and without psychopathology, including psychosis, give equally valid and reliable reports, but that underreporting is very common (Fergusson et al., 2000; Fisher et al., 2011). Underreporting can both decrease the chance of finding associations and confound the actual findings. The CTQ uses the number of different events in the same subcategory and the frequency of events to assess adversity severity. It does not assess the age of events. Therefore, we have not been able to explore the impact of age at adversity.
We have previously discussed the effects of the differences between those who were included (52%) and excluded from the whole catchment area (Trauelsen et al., 2015). The approached group is thought to represent almost all cases of FEP in Region Zealand because of the Danish Health Service and our close contact with it, and we regard the FEP group representative of the catchment area even though 48% of the eligible participants were not included. Beyond our previous discussion (Trauelsen et al., 2015), we wish to mention that the low representation of women with PAS data could have decreased our chances of finding any differences between the premorbid trajectories, because women with psychosis report more childhood adversities than men (Fisher et al., 2009).
We did not include a comprehensive assessment of social factors in this study. Possible important confounders include family poverty, intelligence quotient (IQ) and cognitive and executive functioning (Campbell et al., 2013).
Conclusion and implications
Overall, childhood adversities were associated with global functioning the year prior to treatment, but neither to premorbid trajectories or social outcome factors. It would be preferable to examine these factors in longitudinal studies where resilience and risk factors can be assessed simultaneously and may be more closely examined. Both perceived support from peers and adults during childhood and adolescence was highly related to the risk of psychosis and adult support with the number of childhood adversities. Perceived support seems to be an area with great potential, especially with regards to prevention and early intervention. Since the family is a large part of the social network for people with FEP (Jolley et al., 2014), the association between childhood adversity and family contact may have clinical implications. We suggest that the assessment and treatment of childhood adversity should be included in the early intervention family work and that assistance is provided to increase the social networks of those who need it.
Footnotes
Acknowledgements
The authors would like to thank the interviewees and clinicians who contributed to the study. This paper is part of the OPUS Zealand research project: Family Intervention in First-episode Psychosis. An investigation of metacognition, expressed emotion and caregiver experiences. From 1 January 2012, the project has the following research group: Erik Simonsen, MD, PhD (PI). Ulrik Haahr, MD (PI). Christopher Hoeier Trier, MSc in Psychology. Marlene Buch Pedersen, MSc in Psychology. Hanne-Grethe Lyse Nielsen, RN. Mette Sjoestroem Petersen, MA (ed) in Educational Psychology, Jens Einar Jansen, PhD. Ulf Soegaard, MD. Anne Marie Trauelsen, MD. From 1 September 2014, Signe Dunker Svendsen, RN. From Psychiatric Research Unit, Psychiatry Region Zealand, Denmark. Early Psychosis Intervention Center, Psychiatry East Region Zealand, Denmark.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by The Regional Health and Research Foundation, Zealand (AMT Grant number 12-000095); and The Lundbeck Foundation (AMT Grant number R93-A8804).