
Abstract
Objective:
Subjective quality of life is an important outcome of psychotic disorders. However, longitudinal course of subjective quality of life in the early illness stage is under-studied. We aimed to investigate the patterns and baseline predictors of subjective quality of life trajectories over 3 years in early psychosis patients, utilizing growth mixing modeling analysis, in the context of a 3-year follow-up of a randomized controlled trial comparing 1-year extension of early intervention with step-down psychiatric care for first-episode psychosis.
Method:
One hundred sixty Chinese patients were recruited from specialized early intervention program for first-episode psychosis in Hong Kong after they had completed this 2-year early intervention service, and underwent 1-year randomized controlled trial as well as 2-year post–randomized controlled trial follow-up (i.e. 3-year follow-up). Assessments on premorbid adjustment, onset profile, psychopathology, functioning and treatment characteristics were conducted. Individual class membership of subjective quality of life trajectory derived from growth mixing modeling was based on the 36-Item Short Form Health Survey mental component summary scores measured at four different time-points (baseline, 1, 2 and 3 years) among 142 participants across 3-year follow-up.
Results:
Three distinct subjective quality of life trajectories were identified including higher-improving (68.3%, n = 97), lower-stable (24.6%, n = 35) and deteriorating (7%, n = 10) trajectories. Age of onset; duration of untreated psychosis; depressive, positive and negative symptoms; and intervention condition were significantly different between good (higher-improving trajectory) and poor (combined lower-stable and deteriorating trajectories) trajectory groups. Multiple regression analysis revealed that younger age of onset, more severe depression and receipt of step-down care independently predicted poor subjective quality of life trajectory.
Conclusion:
Approximately one-third of patients displayed poor subjective quality of life trajectory in the early phase of psychotic illness. Our results affirm depression as a critical determinant of prospective subjective quality of life and underscores positive effect of extended early intervention on sustained subjective quality of life improvement. Further longitudinal research is warranted to facilitate better characterization of subjective quality of life course patterns and development of targeted intervention to optimize subjective quality of life in patients with early psychosis.
Introduction
Subjective quality of life (SQoL) is an important outcome in psychotic disorders (Eack and Newhill, 2007). The SQoL is generally conceptualized as a multi-dimensional construct which refers to individuals’ subjective perception of satisfaction in various life domains encompassing mental wellbeing, social functioning and physical health (Lehman, 1996). It is acknowledged that one of the most fundamental features underlying SQoL construct is its subjective nature which captures patients’ life circumstances through their own perspectives (Lehman, 1996). In fact, treatment focus in psychotic disorders has recently been expanded to both objective (e.g. clinical and real-world functional status) and subjective (patient-reported) outcomes. Literature has shown that patients with psychotic disorders, including those in the initial course of illness, display lower levels of satisfaction across most SQoL domains than the general population (Law et al., 2005; Watson et al., 2018). Accumulating evidence has demonstrated that SQoL is associated with symptom remission, relapse and functional outcome in schizophrenia (Boyer et al., 2013b; Lambert et al., 2007). Previous research has also found that improved SQoL may contribute to a greater sense of self-perceived (personal) recovery (Roe et al., 2011). Furthermore, recent data have indicated clinical utility of integrating SQoL assessment with feedback in routine clinical care for schizophrenia patients to enhance therapeutic alliance; service satisfaction and engagement; and treatment adherence (Boyer et al., 2013a). This thus underscores the clinical significance of SQoL as a critical treatment target for enhancing patients’ overall life satisfaction and other treatment outcomes.
An increasing number of research studies have recently been conducted to assess the determinants of SQoL in patients with early psychosis (Watson et al., 2018). The majority of previous studies found that depressive symptoms predicted poorer SQoL in first-episode psychosis (FEP) samples (Cotton et al., 2010; Kwong et al., 2017; Malla et al., 2004; Melle et al., 2005; Renwick et al., 2012). Less consistent findings were observed regarding the relationships of SQoL with other symptom dimensions, with some studies demonstrating positive symptoms (Cotton et al., 2010; Kwong et al., 2017; Thorup et al., 2010) and negative symptoms (Cotton et al., 2010; MacBeth et al., 2015; Malla et al., 2004; Thorup et al., 2010) as independent factors associated with SQoL, but not others. Similarly, literature assessing the impact of duration of untreated psychosis (DUP) on SQoL yielded mixed results. Some reports revealed that DUP was inversely related to SQoL (Górna et al., 2008; Malla et al., 2004; Melle et al., 2005), while others failed to find any significant association between these two variables (Cotton et al., 2010; Law et al., 2005; MacBeth et al., 2015). Of note, most prior investigations on SQOL in early psychosis were cross-sectional in nature. Very few studies have evaluated the longitudinal course and predictors of SQoL in the early phase of illness (Chugh et al., 2013; Gardsjord et al., 2016; Melle et al., 2010; Priebe et al., 2000; Tan et al., 2019), and most had short follow-up duration (i.e. from 6 months to 2 years). Importantly, past longitudinal research examining prediction of SQoL in early psychosis defined an ‘outcome’ as either a continuous variable of SQoL levels (as group averages for analysis) measured from a single assessment conducted at the end-point of the study period or within-group average change in SQoL levels between baseline and follow-up. These conventional outcome-analysis approaches, however, are hampered by several methodological constraints, including not taking into consideration the course of SQoL across the entire follow-up period and masking the complexity of individual variation in SQoL over time. To address these limitations, recently, an individual-based longitudinal modeling, namely growth mixture modeling (GMM), has been increasingly applied in mental health research. GMM is a model-based statistical approach which allows for probabilistic classification of subjects into discrete subgroups based on their longitudinal trajectories (Ram and Grimm, 2009). The use of GMM in studying SQoL in early psychosis thus facilitates identification of a subgroup of patients who are at high risk of developing persistently poor SQoL levels and necessitate more intensive early intervention (EI) to prevent progression to this unfavorable outcome. Despite its methodological advantages, there has been no published report investigating the longitudinal course of SQoL in patients with early psychosis using this individual-based trajectory analysis. Alternatively, although EI service has been shown to significantly improve symptom and functional outcomes in FEP patients (e.g. Craig et al., 2004; Kane et al., 2016; Petersen et al., 2005), whether it is effective in enhancing SQoL, particularly after the specialized treatment has ended, remains to be clarified.
In Hong Kong (HK), a territory-wide, publicly funded specialized treatment program for young people with FEP, namely Early Assessment Service for Young People with Psychosis (EASY), has been established since 2001 (Chung and Chen, 2013). The program provided comprehensive evaluation and 2-year phase-specific EI to FEP patients aged 15–25 years, who were each assigned with a case manager with provision of protocol-based psychosocial interventions. Patients were transferred to a transitional step-down clinic in the third year of treatment with no case management provided, followed by generic psychiatric service for continuous care. We have previously conducted a 3-year follow-up of a randomized controlled trial (RCT) evaluating the efficacy of a 1-year extension of EI (extended EI or 3-year EI) vs step-down psychiatric care (SC or 2-year EI) in clinical and functional outcome improvement in a cohort of Chinese FEP patients who had completed 2-year treatment in EASY program (Chang et al., 2015, 2017) This is the first RCT follow-up study examining sustainability of therapeutic benefits of EI service for FEP on clinical and functional outcomes with its treatment period extended beyond 2 years. Results of this study showed that superior effects achieved by extended EI could not be maintained after termination of the specialized service (Chang et al., 2017).
Better understanding of the patterns and predictors of SQoL trajectories in the early course of illness facilitates identification of therapeutic targets and provision of effective intervention to promote SQoL in patients with early psychosis. In the current report, we sought to identify distinct trajectories of SQoL over 3-year follow-up using GMM analysis and to investigate baseline predictors discriminating between SQoL trajectories in early psychosis patients in the context of this 3-year RCT follow-up study. SQoL was measured by the 36-Item Short Form Health Survey (SF-36, Ware and Sherbourne, 1992) which is a well-researched, widely used self-rated questionnaire to assess health-related SQoL. Specifically, we focused on examining mental component of SQoL (mental SQoL) as literature indicates that SQoL construct measured by SF-36 can be divided into two distinct physical and mental health components, with the latter being sensitive to clinical manifestations and treatment response of psychiatric conditions (McHorney et al., 1993). Comprehensive assessments encompassing clinical, functional and treatment-related variables were incorporated to enable better clarification of baseline prediction profiles for longitudinal course patterns of mental SQoL.
Methods
Participants and setting
The current investigation was based on a 3-year follow-up of a single-blind RCT comparing a 1-year extension of specialized EI (a 3-year EI service) with a step-down care (a 2-year EI service) in FEP patients who had received 2-year treatment from EASY program (Figure 1). Details of the study methodology have been reported elsewhere (Chang et al., 2015, 2017). Briefly, 160 patients with the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnosis of psychotic disorder were recruited from EASY program upon completion of 2-year EI care between November 2010 and August 2011, randomly allocated to extended EI (n = 82) or SC (n = 78), and underwent 1-year clinical trial (Chang et al., 2015). Patients with substance-induced psychosis, psychotic disorder due to general medical condition or learning disability were excluded. In extended EI group, an additional year of specialized case management was delivered by a trained case manager, who took over the cases from EASY program and coordinated treatments with clinicians, allied health professionals and community centers. Case management provided closely aligned with EASY treatment protocols and specifically focused on functional improvement, with a view to facilitating participants to enhance social networks, resume leisure pursuits and return to work. Psychoeducation, supportive care and counseling on stress coping were also offered to participants’ caregivers by the case manager. Participants randomized to the SC group received medical follow-up with limited community support focusing primarily on crisis intervention, and no case management was provided. Participants from both treatment groups were managed by psychiatrists from their respective EASY clinical teams and did not differ in the intensity of psychiatric follow-up; prescription of antipsychotic medications; and availability of psychosocial interventions and community-based services. Participants were followed up and re-interviewed 2 and 3 years after inclusion to the trial (Chang et al., 2017, 2018) with data collection being finished in September 2014.
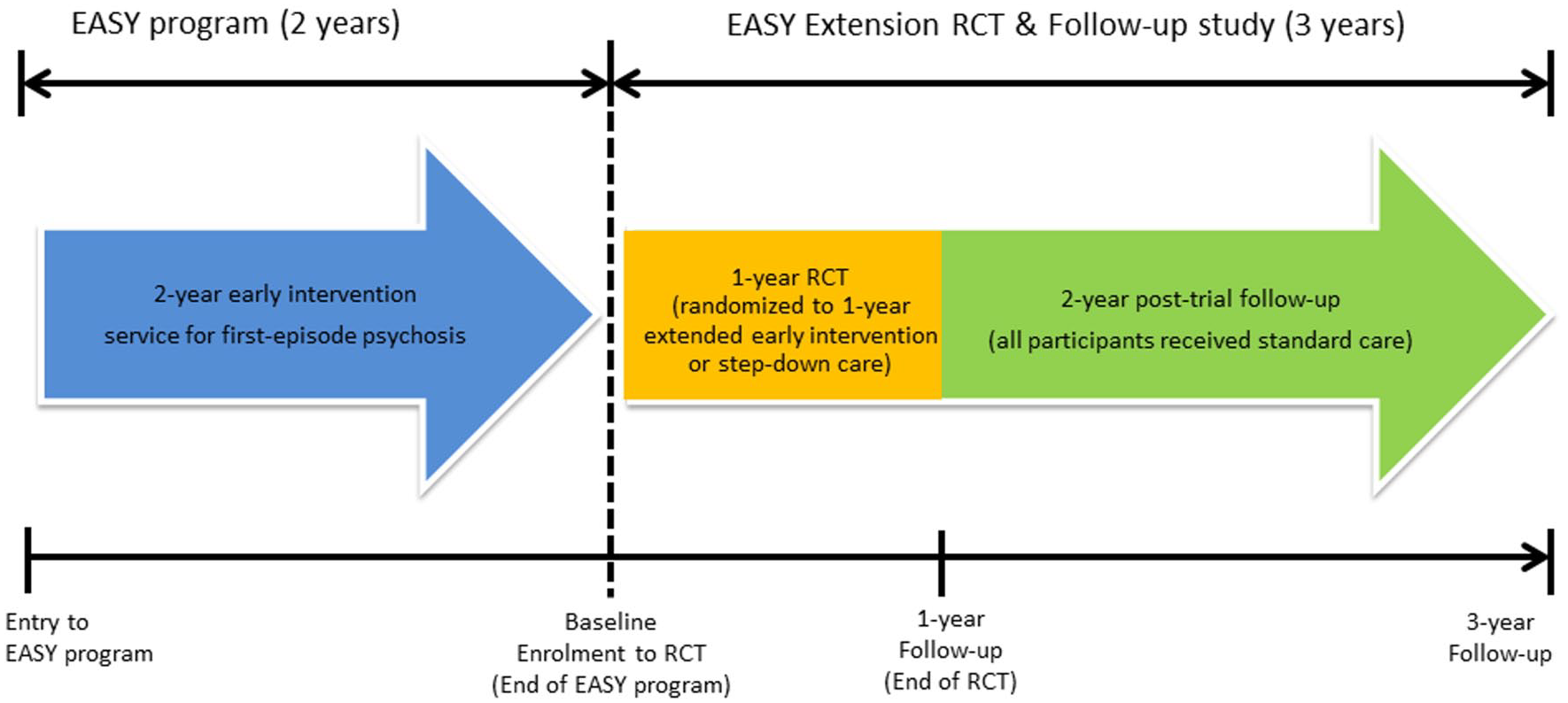
Flow diagram of EASY Extension trial and follow-up study.
In this report, we focused on investigating the patterns and predictors of trajectories of SQoL in 142 participants of the initial cohort who completed SQoL assessment at three or more of the four follow-up time-points over 3-year study period. Briefly, among the 18 excluded patients, 4 did not complete 1- and 2-year assessments, 11 did not complete 2- and 3-year assessments and 3 did not complete all the three follow-up assessments. Details of the study attrition over 3-year follow-up were described in our previous publication (Chang et al., 2017). The study was approved by the local institutional review boards. All participants provided written informed consent. For those under 18 years old, consent was also obtained from a parent or guardian.
Assessments
Diagnostic ascertainment of each participant was based on verifying all available information including Chinese-bilingual Structured Clinical Interview for DSM-IV (CB-SCID; So et al., 2003) conducted at study intake (baseline, i.e. upon completion of 2-year EASY care), 1- and 3-year follow-up, medical records and informant histories. Premorbid functioning was evaluated by the Premorbid Adjustment Scale (PAS; Cannon-Spoor et al., 1982), based on information obtained via interviews with patients and their caregivers. DUP, age and mode of psychosis onset were assessed by Interview for the Retrospective Assessment of the Onset of Schizophrenia (IRAOS; Häfner et al., 1992). Psychopathology was evaluated by Positive and Negative Syndrome Scale (PANSS; Kay et al., 1987) and Calgary Depression Scale for Schizophrenia (CDSS; Addington et al., 1993). Antipsychotic-induced motor side-effects were assessed using Simpson–Angus Scale (SAS; Simpson and Angus, 1970). A self-administered Drug Attitude Inventory (DAI; Awad, 1993) was employed to assess participants’ attitude toward antipsychotic treatment, with higher scores indicating more positive attitude. Psychosocial functioning was measured by Social and Occupational Functioning Assessment Scale (SOFAS). SQoL was evaluated using the Chinese version SF-36 (Lam et al., 1998; Ware and Sherbourne, 1992) which is a self-rated questionnaire covering multiple domains of health-related SQoL. SF-36 has been extensively used in clinical populations of physical and mental illnesses, and is shown to be a reliable and valid measure of health-related SQoL for patients with psychotic disorders (Leese et al., 2008). Chinese version of SF-36 was validated in healthy participants in a population-based study (Lam et al., 1998) and has been studied in Chinese FEP samples in HK (Kwong et al., 2017; Law et al., 2005). In this study, SF-36 mental component summary (MCS) score (McHorney et al., 1993), which comprises items assessing vitality, social functioning, role emotional and mental health domains, was computed as primary measure of mental SQoL, with higher score indicating better SQoL. Assessments on symptom severity, functioning, SQoL and treatment characteristics were conducted at baseline, 1-, 2- and 3-year follow-up. Intensive training in the use of study instruments was provided to research assistants who administered all assessments. Ongoing supervision by senior research psychiatrists and regular clinical rating reliability meetings (on a monthly basis) were arranged to maintain quality assurance. Videotaped interviews of 10 participants were independently rated by all research assistants for inter-rate reliability evaluation. Intra-class correlation coefficients (ICCs) for DUP, PANSS general psychopathology, positive and negative symptom subscale, CDSS and SOFAS scores were 0.78, 0.92, 0.95, 0.79, 0.96 and 0.91, respectively, indicating good inter-rater reliability.
Statistical analysis
We employed GMM to identify distinct trajectories of patients’ mental SQoL over 3-year follow-up. GMM is a person-centered statistical approach used to delineate homogeneous subgroups (latent classes) of individuals with similar patterns of change over time (Ram and Grimm, 2009). In the current analysis, individual class membership was assigned on the basis of SF-36 MCS scores at four time-points over 3 years, i.e. at intake, 1 year and 2 and 3 years of follow-up, utilizing full information maximum likelihood estimation to account for missing data with the assumption that data were missing at random (Little and Rubin, 2002). To determine the optimal number of trajectory classes, models with increasing number of latent classes (from 1 to 5 class models) were fitted to the data and the best-fitting model was selected according to the following goodness-of-fit indices: Akaike information criterion (AIC), Bayesian information criterion (BIC), sample-size-adjusted BIC (aBIC), bootstrap likelihood ratio test (BLRT), Lo–Mendell–Rubin likelihood ratio test (LMR-LRT) and entropy. Lower values of AIC, BIC and aBIC suggest a more parsimonious model, while a significant BLRT and LMR-LRT (based on p < 0.05) indicate that this model (e.g. a K-class model) has a better fit than a model with one fewer latent classes (i.e. a K–1 class model). Higher entropy also indicates better model fit. GMM analyses were performed on Mplus, version 7.
To examine baseline predictors of mental SQoL trajectory membership, the estimated latent classes derived from GMM were imported to SPSS, version 25, for a two-step analysis. Candidate predictor variables including demographics; premorbid adjustment; illness onset profiles; and baseline symptom, functional and treatment characteristics were compared between good and poor trajectory groups using independent samples t test and chi-square test, as appropriate. Those variables that were found to be found to be statistically significant in preceding analyses were then entered into a multiple binary logistic regression model to determine which candidate factors independently predicted SQoL trajectory.
Results
Characteristics of the sample
Of 142 participants included in the study, 53.5% were male. The mean age of the sample was 22.9 years (SD = 3.2) and the median DUP was 13 weeks (M = 33.5, SD = 48.0, interquartile range = 3.7–52.1). Attrition analysis revealed no significant difference between completers and non-completers in demographics, allocated treatment condition or baseline clinical, functional and treatment variables.
Latent classes of SQoL trajectories
Table 1 presents the fit statistics for all the tested growth mixture models. Overall, a 3-class solution was selected as the most parsimonious model. The 3-class solution outperformed the other models in terms of fit indices, yielding lower values in AIC and BIC and significant BLRT and LMR-LRT (indicating better fit than 2-class solution, with 4-class solution showing non-significant BLRT and LMR-LRT). Entropy of 3-class solution (0.84) was higher than all other models. The average class probabilities for the 3-class model were high (0.83–0.98), indicating high likelihood of correctly assigning participants to their respective latent class.
Goodness-of-fit statistics of GMM models for one-to-five class solutions of SQoL trajectories.
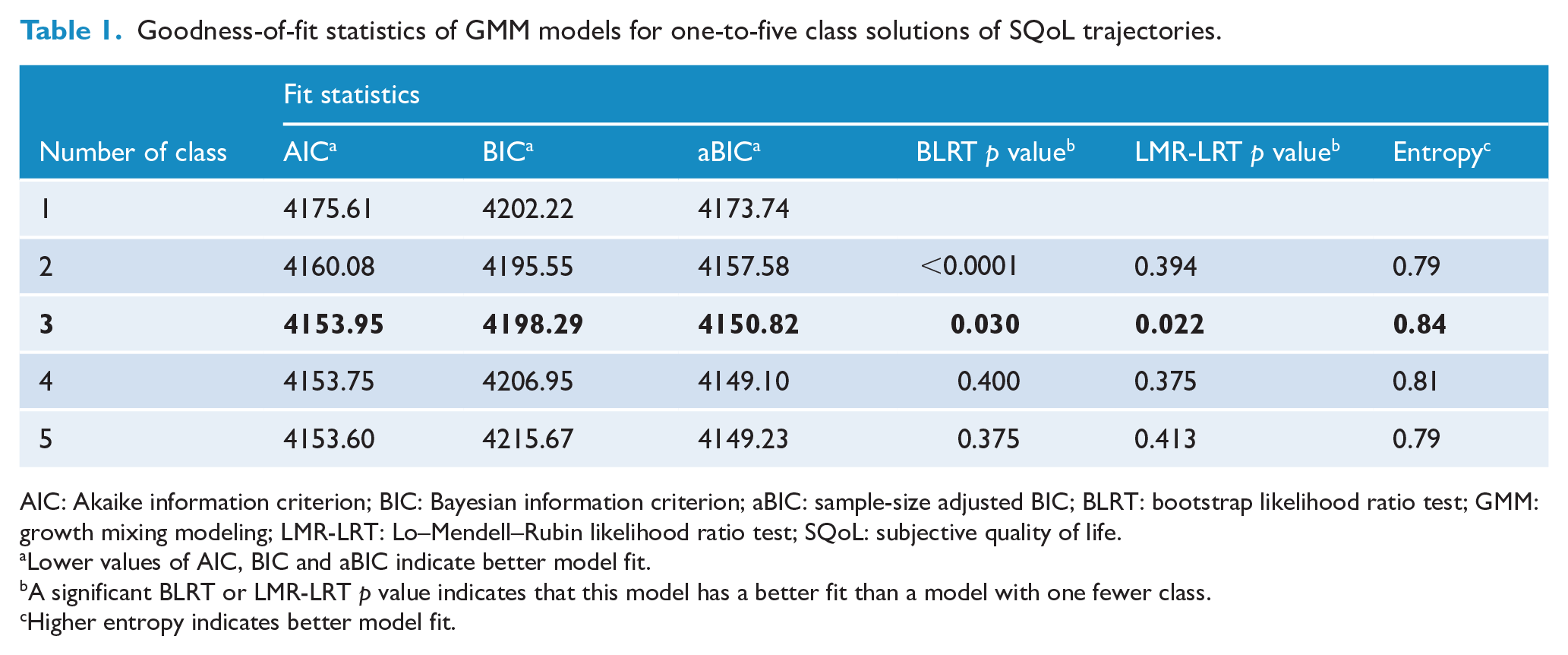
AIC: Akaike information criterion; BIC: Bayesian information criterion; aBIC: sample-size adjusted BIC; BLRT: bootstrap likelihood ratio test; GMM: growth mixing modeling; LMR-LRT: Lo–Mendell–Rubin likelihood ratio test; SQoL: subjective quality of life.
Lower values of AIC, BIC and aBIC indicate better model fit.
A significant BLRT or LMR-LRT p value indicates that this model has a better fit than a model with one fewer class.
Higher entropy indicates better model fit.
Mental SQoL trajectories identified in the 3-class solution are illustrated in Figure 2. The first class was referred to as higher-improving trajectory (68.3%, n = 97) which was characterized by comparatively higher baseline SF-36 MCS scores followed by further gradual improvement in SQoL over 3 years. The second class was termed as lower-stable trajectory (24.6%, n = 35) in which patients displayed relatively lower SF-36 MCS scores at intake and then maintained a stable course of SQoL throughout the 3-year follow-up. The third class was referred to as deteriorating trajectory (7%, n = 10) in which patients initially had SF-36 MCS scores comparable to those with high-improving trajectory at baseline followed by progressive decline, resulting in exhibiting the lowest levels of SQoL among three trajectory classes by the end of the 3-year study period.
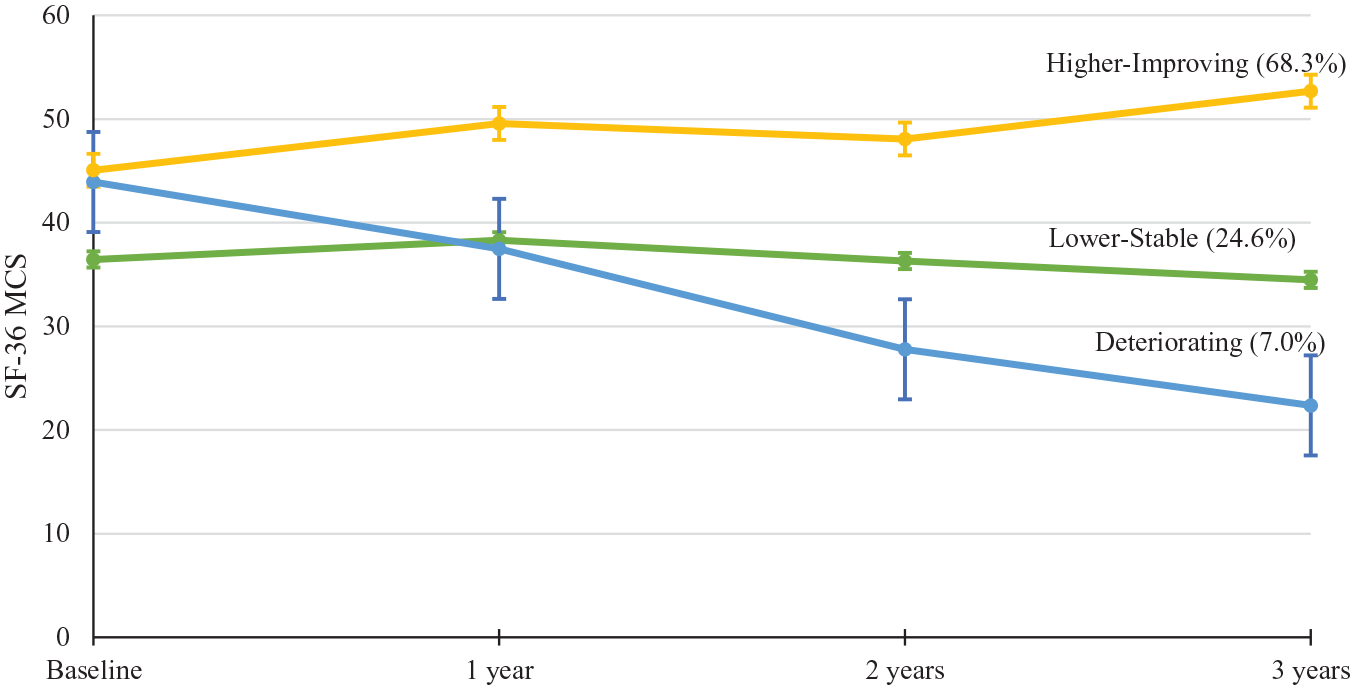
SQoL trajectories over 3-year follow-up derived from growth mixture modeling.
Predictors of SQoL trajectories
Owing to sample size constraint on deteriorating trajectory class (n = 10), we combined patients in lower-stable and deteriorating trajectory classes into poor SQoL trajectory group, and compared with patients in higher-improving trajectory class (termed as good SQoL trajectory group) for analysis of predictor identification. Our supplementary analyses comparing the three trajectory classes found no significant difference between lower-stable and deteriorating trajectory classes in any of the demographic and baseline variables (Supplemental Table S1). As shown in Table 2, patients in the good SQoL trajectory group were significantly older at study entry and at onset of psychosis; had shorter DUP; fewer positive, negative and depressive symptoms; and a higher likelihood to receive extended EI relative to those in the poor SQoL trajectory group. Multiple binary logistic regression analysis revealed that older age of onset, lower levels of depressive symptom severity at baseline and receipt of extended EI independently predicted good SQoL trajectory over 3-year follow-up, with extended EI treatment condition representing the strongest predictor of good SQoL trajectory class (Table 3).
Baseline comparison between good and poor SQoL trajectory classes in demographics, onset and illness characteristics, premorbid adjustment, symptom severity and functioning and treatment characteristics. a
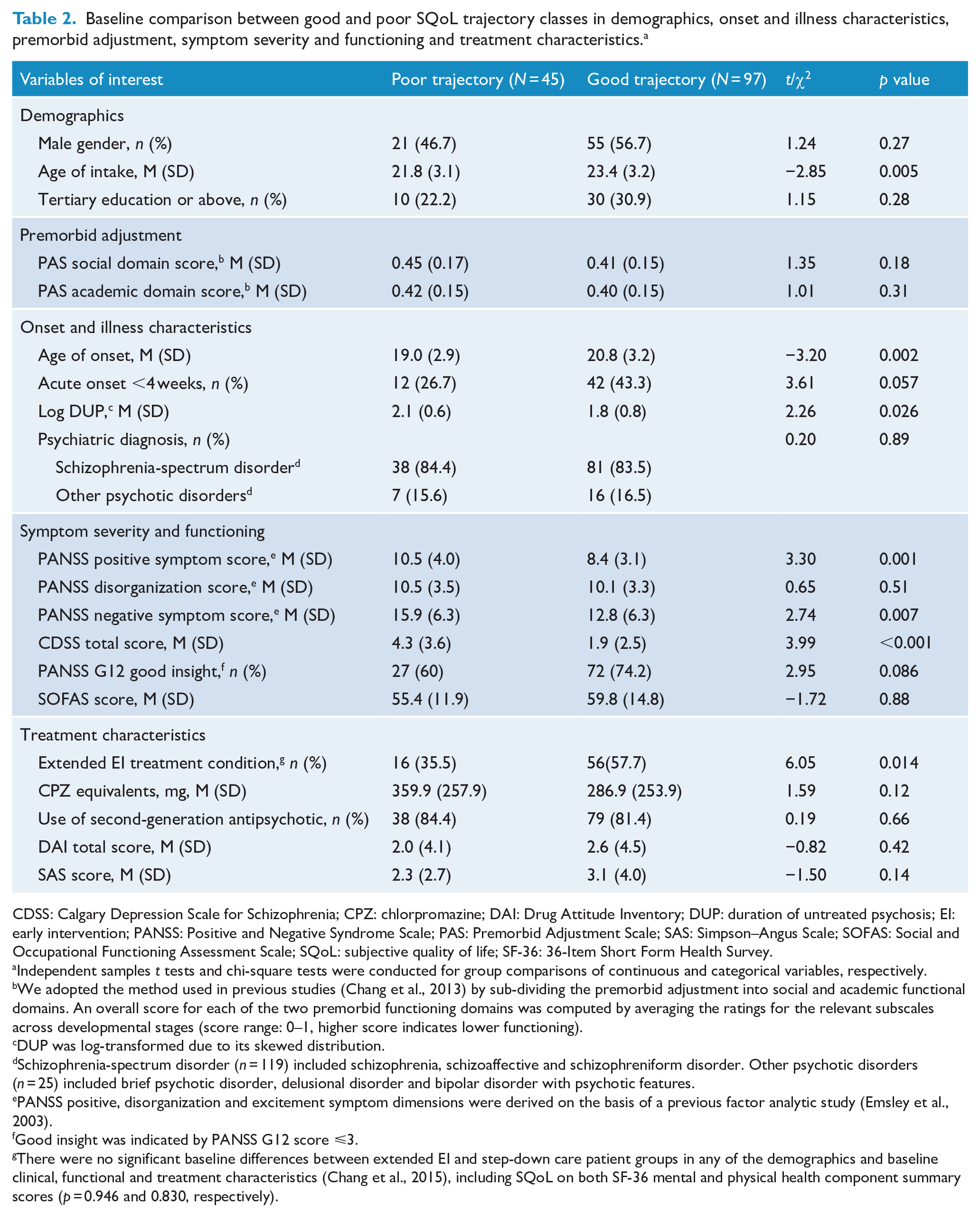
CDSS: Calgary Depression Scale for Schizophrenia; CPZ: chlorpromazine; DAI: Drug Attitude Inventory; DUP: duration of untreated psychosis; EI: early intervention; PANSS: Positive and Negative Syndrome Scale; PAS: Premorbid Adjustment Scale; SAS: Simpson–Angus Scale; SOFAS: Social and Occupational Functioning Assessment Scale; SQoL: subjective quality of life; SF-36: 36-Item Short Form Health Survey.
Independent samples t tests and chi-square tests were conducted for group comparisons of continuous and categorical variables, respectively.
We adopted the method used in previous studies (Chang et al., 2013) by sub-dividing the premorbid adjustment into social and academic functional domains. An overall score for each of the two premorbid functioning domains was computed by averaging the ratings for the relevant subscales across developmental stages (score range: 0–1, higher score indicates lower functioning).
DUP was log-transformed due to its skewed distribution.
Schizophrenia-spectrum disorder (n = 119) included schizophrenia, schizoaffective and schizophreniform disorder. Other psychotic disorders (n = 25) included brief psychotic disorder, delusional disorder and bipolar disorder with psychotic features.
PANSS positive, disorganization and excitement symptom dimensions were derived on the basis of a previous factor analytic study (Emsley et al., 2003).
Good insight was indicated by PANSS G12 score ⩽3.
There were no significant baseline differences between extended EI and step-down care patient groups in any of the demographics and baseline clinical, functional and treatment characteristics (Chang et al., 2015), including SQoL on both SF-36 mental and physical health component summary scores (p = 0.946 and 0.830, respectively).
Final binary logistic regression model for the predictor of SQoL trajectoriesa,b.
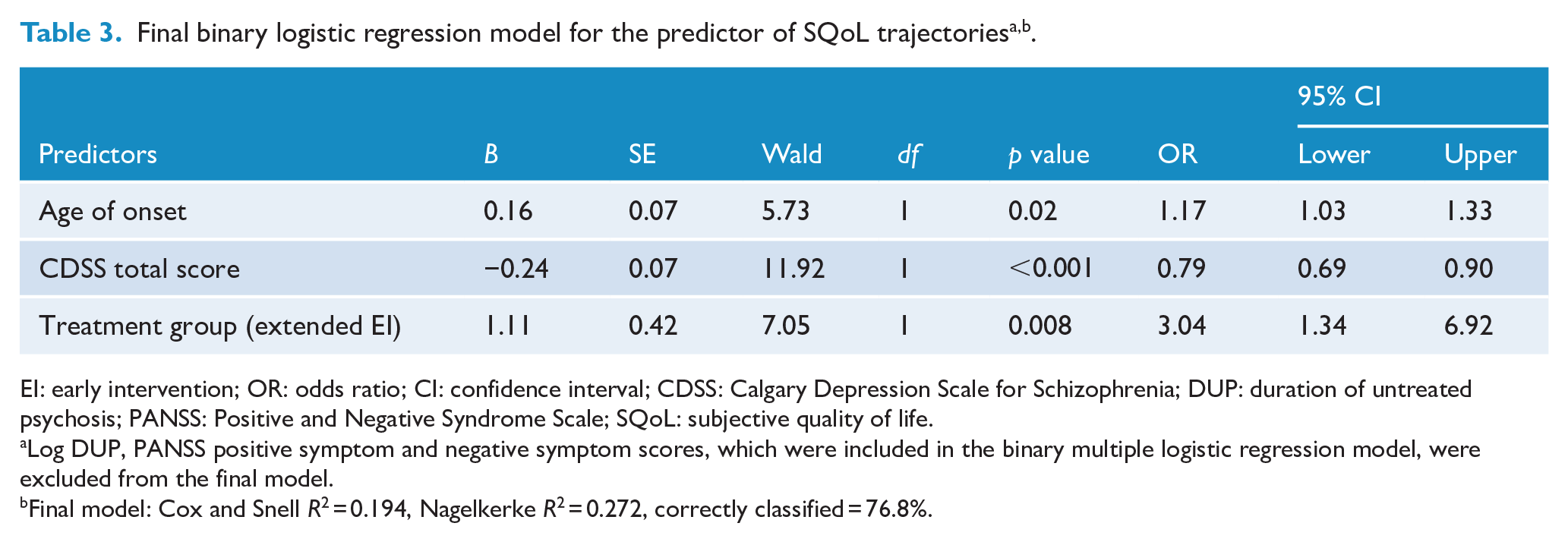
EI: early intervention; OR: odds ratio; CI: confidence interval; CDSS: Calgary Depression Scale for Schizophrenia; DUP: duration of untreated psychosis; PANSS: Positive and Negative Syndrome Scale; SQoL: subjective quality of life.
Log DUP, PANSS positive symptom and negative symptom scores, which were included in the binary multiple logistic regression model, were excluded from the final model.
Final model: Cox and Snell R2 = 0.194, Nagelkerke R2 = 0.272, correctly classified = 76.8%.
Discussion
This study, to our knowledge, is the first to examine longitudinal course patterns of mental SQoL in early psychosis patients using individual-based trajectory analysis. Our results revealed three distinct SQoL trajectories across a 3-year study period. Specifically, although we found that the majority of patients (classified as high-improving trajectory) ran a relatively favorable course of SQoL with further gradual improvement over time, 24.6% were categorized as displaying low-stable trajectory with persistently poorer SQoL across the entire follow-up. Furthermore, 7% of our cohort (classified as deteriorating trajectory) experienced progressive decline in SQoL over 3 years, resulting in having the lowest levels of psychological wellbeing by the end of the study follow-up among the three trajectory classes. Overall, our findings indicate the heterogeneity of longitudinal SQoL course in the early stage of psychotic illness, and suggest that a significant proportion of patients still exhibit poor SQoL after receipt of at least 2-year EI service (i.e. EASY program) for their first psychotic episode.
There is evidence that patients who received EI service have better SQoL than those treated in generic psychiatric care (Garety et al., 2006; Petersen et al., 2005). Our results further revealed that extended EI (i.e. 3-year EI), relative to step-down care (i.e. 2-year EI), was independently associated with good SQoL trajectory over 3 years of follow-up. This thus suggests that the positive effect of extended EI on SQoL was maintained after the specialized service was terminated. Intriguingly, such therapeutic gains on SQoL were observed even though the superiority of extended EI on symptom and functional outcomes disappeared after service withdrawal. On the other hand, it is suggested that patients’ perception on levels of service satisfaction, self-stigma, sense of empowerment, illness beliefs and coping styles may substantially influence SQoL appraisal (Lien et al., 2018; Sibitz et al., 2011; Theodore et al., 2012). It might be possible that these psychological factors might also benefit significantly from extended EI and in turn contribute to sustained SQoL improvement. Alternatively, our findings highlight the importance of incorporating patient-reported outcomes in treatment and service evaluation for early psychosis as subjective measures, in particular SQoL, are complementary with yet distinct from objective (clinician-assessed) measures, and can guide subsequent treatment decision-making by taking into consideration patient-oriented perspectives. A recent meta-analysis also indicated a significant but small association between clinical and personal recovery, and suggested that both constructs should be considered in outcome monitoring of patients with psychotic disorders (van Eck et al., 2018). Nonetheless, owing to the paucity of existing data, further research is warranted to verify our findings of the relationship between extended EI and SQoL course patterns, as well as to identify other variables that may potentially mediate the beneficial effect of extended EI on SQoL in early psychosis patients.
Our results indicate the critical role of depression in determining SQoL among early psychosis patients by demonstrating that greater baseline depressive symptom severity prospectively predicted poor SQoL trajectory. This is consistent with most previous longitudinal (albeit very few being conducted) (Gardsjord et al., 2016; Melle et al., 2010; Priebe et al., 2000) and cross-sectional studies (Cotton et al., 2010; Kwong et al., 2017; Malla et al., 2004; Melle et al., 2005; Renwick et al., 2012) showing that depressive symptoms were inversely related to SQoL in first-episode samples. Although it is suggested that the observed association between depression and SQoL might partly reflect conceptual and measurement overlaps between these two variables, literature generally indicates that SQoL and depression constitute related but distinct constructs (Berlim and Fleck, 2007). It is also posited that depressed patients have higher tendency of negative self-appraisal, which may lead to their lower satisfaction with various life domains, particularly psychological wellbeing (Renwick et al., 2012). Importantly, given that depression represents a major determinant of SQoL and is prevalent in the early phase of illness (Herniman et al., 2019), comprehensive evaluation and regular monitoring of depressive symptoms should be integrated in EI service to facilitate early detection and intervention which will in turn promote patients’ SQoL. Alternatively, our analysis found that patients with younger age at onset of psychosis exhibited poor SQoL trajectory. This in fact echoes with literature which has generally found that younger age of onset is associated with worse clinical and functional outcomes in psychotic disorders (Immonen et al., 2017).
Our final regression model failed to support DUP, baseline positive and negative symptoms as independent predictors of 3-year trajectory of SQoL (albeit being statistically significant in univariate analyses). In fact, discrepant findings were observed regarding the relationship between DUP and SQoL in early psychosis samples, with many, though not all, previous cross-sectional studies showing null findings in this respect (Cotton et al., 2010; Law et al., 2005; MacBeth et al., 2015). Our earlier analysis on clinical correlates of SQoL in the initial cohort of this study also found that DUP was not significantly related to SQoL at baseline (Kwong et al., 2017). Notably, only one prior longitudinal study has examined the effect of DUP on prospective SQoL and revealed insignificant association between these two variables (Melle et al., 2010). One possible explanation is that the comparatively short DUP (median DUP: 13 weeks) of our cohort (relative to those studies conducted without the context of EI service for psychosis) might obscure the potential negative impact of prolonged untreated psychosis on SQoL trajectory. In addition, the influence of DUP on SQoL might diminish over the course of illness after initial presentation, and might therefore become no longer significant at long-term follow-up. Conversely, our results concur with all those previous longitudinal studies which have consistently shown that baseline positive and negative symptom severity did not predict SQoL at follow-up in patients with early psychosis (Chugh et al., 2013; Gardsjord et al., 2016; Melle et al., 2010; Priebe et al., 2000; Tan et al., 2019). This thus further affirms that depression plays a more important role than the core symptoms (i.e. positive and negative symptoms) of psychotic disorders in determining the levels of concurrent and prospective SQoL.
Several methodological limitations warrant consideration in interpreting the study results. First, the relatively modest sample size of our cohort precludes us from further clarifying differential baseline prediction profiles for low-stable and deteriorating SQoL trajectories. Second, our results were based on secondary analysis and the study was not designed to specifically examine patterns and predictors of SQoL trajectories in early psychosis patients. Hence, some potentially important candidate predictive variables of SQoL such as self-stigma, illness beliefs and cognitive deficits (Lien et al., 2018; Theodore et al., 2012) were not included and measured in this study. Third, SF-36 is a generic SQoL instrument which may not adequately capture SQoL domains that are specifically relevant to patients with psychotic disorders. Fourth, the study sample was recruited from EASY program which provided EI to patients aged 15–25 years. Hence, our results may not be generalizable to those with older age of psychosis onset. Fifth, the current analysis only focused on 3-year SQoL trajectories, and a longer follow-up duration is required to capture potentially more complex long-term longitudinal patterns of SQoL along the course of illness.
In conclusion, our results indicate a heterogeneous course of mental SQoL in young people with early psychosis, with approximately one-third of the cohort exhibiting poor trajectory of psychological wellbeing throughout the 3-year follow-up. Depression, younger age of onset and lack of access to extended EI independently predicted poor SQoL trajectory. Our findings thus underscore depression as a pivotal therapeutic target for enhancing prospective SQoL in the early course of illness. Further investigation is required to identify active treatment elements in extended EI contributing to sustained improvement in SQoL. In addition, a more comprehensive array of candidate predictive factors including cognitive functions and psychological variables (e.g. self-stigma and illness coping styles) should be incorporated in future prediction model for SQoL trajectory so as to facilitate identification of treatment targets and development of specific interventions to optimize SQoL in early psychosis patients.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211009603 – Supplemental material for Patterns and predictors of trajectories for subjective quality of life in patients with early psychosis: Three-year follow-up of the randomized controlled trial on extended early intervention
Supplemental material, sj-docx-1-anp-10.1177_00048674211009603 for Patterns and predictors of trajectories for subjective quality of life in patients with early psychosis: Three-year follow-up of the randomized controlled trial on extended early intervention by Candice Tze Kwan Kam, Wing Chung Chang, Vivian Wing Yan Kwong, Emily Sin Ki Lau, Gloria Hoi Kei Chan, Olivia Tsz Ting Jim, Christy Lai Ming Hui, Sherry Kit Wa Chan, Edwin Ho Ming Lee and Eric Yu Hai Chen in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We thank all the coordinating clinicians and staff from the psychiatric inpatient and outpatient units, as well as the medical records departments for their kind assistance. We are also grateful to the individuals who participated in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: E.Y.H.C. has participated in the paid advisory board for Otsuka, has received educational grant support from Janssen-Cilag and has received research funding from AstraZeneca, Janssen-Cilag, Eli Lilly, Sanofi-Aventis and Otsuka. The other authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by grants from the Commissioned Research on Mental Health Policy and Services (SMH-29), and Health and Medical Research Fund (HMRF no. 11121881) of the Food and Health Bureau, the Government of Hong Kong Special Administrative Region. The funding body had no involvement in any aspect of the study or manuscript preparation.
Supplemental material
Supplemental material is available online for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.