
Abstract
Background:
The Remission in Schizophrenia Working Group (RSWG) has proposed remission criteria for schizophrenia, which were shown to be valid in terms of functional and clinical outcomes. However, studies investigating the association between dynamics in remission status in relation to longitudinal functional and clinical outcome are scarce.
Methods:
A total of 648 patients were allocated to four change-in-remission groups, i.e. remission/remission, remission/no-remission, no-remission/remission, and no-remission/no-remission. Remission status was based on PANSS ratings. Multilevel linear modelling techniques were used to investigate whether enduring remission was associated with more improvement in functional outcome at follow-up. Further, change in functional and clinical outcome at follow-up measurement was assessed for each remission category separately.
Results:
Both at baseline and at follow-up, remission status was associated with better functioning. At baseline, patients who subsequently moved out of remission status could be characterized by more severe psychopathology, disabilities, unmet needs and worse quality of life (QoL) compared with patients who continued to be in remission. The stable in-remission group was characterized by significantly better functioning and QoL, both at baseline and follow-up compared with all other remission groups. Nevertheless, QoL increased in all four patient categories.
Conclusions:
In a large sample of patients with a non-affective psychotic disorder, stable remission or moving into remission over time, based on the RSWG criteria, was associated with a favourable functional outcome and QoL, providing further support for the clinical validity of the RSWG remission criteria. The findings also suggest growing adaptation and self-management over time, despite ongoing difficulties.
Introduction
The inevitability of poor outcome for patients with schizophrenia has been successfully challenged (De Hert et al., 2007), suggesting that the course of illness is more variable than previously understood. Approximately 80% of the patients with schizophrenia are not characterized by a decline (Bellack, 2006). This has led to a more optimistic perspective on the possibilities of many patients with schizophrenia and paved the way for the conceptualization of remission criteria.
In 2005, the Remission in Schizophrenia Working Group (RSWG) (Andreasen et al., 2005) conceptualized the remission criteria for schizophrenia. Remission was defined by both a severity and a time criterion, i.e. remission is achieved when eight symptoms do not exceed a score of mild (severity criterion) for at least 6 months or more (time criterion). These core symptoms together represent the psychotic, disorganized and negative symptom dimensions of schizophrenia (Andreasen et al., 2005; Van Os et al., 2006). The remission symptoms also align closely with the diagnostic criteria for schizophrenia specified in DSM-IV (American Psychiatric Association 1992, 2000; De Hert et al., 2007). In DSM-5, the diagnostic criteria for schizophrenia have not changed in essence, but remission criteria are underscored as an important addition in the diagnostic process. Longitudinal course specifiers indicate whether patients meet the active-phase criteria for schizophrenia and whether they are unremitted or in partial or complete remission (Tandon et al., 2013).
Several cross-sectional studies have investigated the validity of the RSWG remission definition by confirming associations with functional and clinical outcome measures relevant to schizophrenia. Patients who achieved RSWG remission were found to show higher levels of general and social functioning, less (unmet) needs for care and better quality of life (QoL) (Van Os et al. 2006), lower total consumption of healthcare services (Eberhard et al., 2009; De Hert et al., 2007), and better illness insight (Eberhard et al., 2009; De Hert et al., 2007). Also, patients who achieved remission were characterized by superior premorbid functioning and social cognition (Bobes et al., 2009). Longitudinal studies on RWSG remission status found that achieving remission status over time was associated with better medication adherence and symptomatic improvement; moreover, achieving remission was associated with improved psychosocial functioning (Chang et al., 2012; Lambert et al., 2010; Lin et al., 2012). Longitudinal studies also showed that that enduring symptomatic remission is important for actual functional improvement. Therefore, we need to increase our understanding of the association between the dynamics of remission status over time, in addition to knowledge on associations between symptomatic and functional outcome (Bellack, 2006; Green et al., 2013). Ciudad and colleagues (2009) demonstrated that achieving a stable remission status during a 1-year period was associated with better treatment adherence, improvement of depressive symptoms and social cognition. Similarly, Van Os and colleagues (2006) showed that changes in remission status over time were associated with changes in needs for care, global functioning and QoL (Van Os et al., 2006). Thus, there is some evidence that stable remission is associated with more favourable outcome and might be a first step towards recovery for patients with schizophrenia.
However, to our knowledge, studies to date have not specifically focused on the full dynamics of changes in remission status, such as patients who move out of remission status over time. We argue that being able to predict the consequences of change in remission status in either direction is clinically relevant. Early identification of patients prone to either positive or negative change in remission status may help clinicians predict course of illness, and intervene when possible or at an earlier moment in illness course. Also, studies on the consequences of persistent non-remission status are scarce. One recent study found only a small effect of psychopathology on the overall subjective well-being of patients with (chronic) schizophrenia, although it did contribute negatively to life satisfaction (Fervaha et al., 2013). Shedding light on the relation between persisting (non-)remission status and social functioning and QoL will likely increase understanding of the prospects for patients with more persistent schizophrenia spectrum disorders.
For the purpose of the current study, four aims were defined. First (i), we investigated the validity of the RSWG remission concept further by examining associations between symptomatic remission and clinical and functional variables at baseline and follow-up measurement separately. Second (ii), we aimed to identify relevant baseline demographical, clinical and functional associations with a favourable change (moving into remission status at follow-up) and an unfavourable change (moving out of remission at follow-up) in remission status over a 3-year period. Third (iii), we investigated whether enduring remission is associated with a more favourable outcome in terms of global functioning, unmet needs for care and QoL at follow-up compared with other scenarios. Last (iv), we wished to examine the change in functional and clinical state from baseline to follow-up for each remission category separately.
Methods
Population
The patients in this study were recruited as part of the Genetic Risk and OUtcome of Psychosis (GROUP) study, a large sample of patients with a psychotic disorder. GROUP is a naturalistic follow-up study in which 1120 patients with a psychotic disorder, 1057 of their siblings, 919 of their parents and 590 unrelated control subjects were included. Patients were selected from geographical areas in the Netherlands and Belgium and were identified by representative clinicians whose caseload was screened for inclusion criteria. Subsequently, a group of patients presenting consecutively at these services either as out-patients or in-patients were recruited for the study. For the current study, only the patient group was analysed. Inclusion and exclusion criteria, details on the procedure of recruitment and population characteristics of the GROUP study have been described in detail elsewhere (Korver et al., 2012).
We report here on a sample of patients based on two criteria; first DSM-IV diagnosis of either schizophrenia, schizofreniform and schizoaffective disorder at baseline was required. This is in line with previous studies investigating the validity of the RSWG criteria (Van Os et al., 2006). Diagnosis was based on the Diagnostic and Statistical Manual of Mental Disorder, Fourth Edition (DSM-IV) (American Psychiatric Association, 1992, 2000). DSM criteria were assessed with the Comprehensive Assessment of Symptoms and History (CASH) interview (Andreasen et al., 1992) or Schedules for Clinical Assessment for Neuropsychiatry (SCAN 2.1) (Wing et al., 1990). Second, availability of baseline and follow-up data on the Positive and Negative Syndrome Scale (PANSS) (Kay et al., 1987) was required to be included in the analyses (mean interval between assessments: 3.3 years; range: 1.5–5.9 years). A subsample of 648 patients was included based on two above-mentioned criteria.
Measures
Remission status
The severity criterion of the remission criteria is based on the severity of several core symptoms in schizophrenia (Andreasen et al., 2005). These symptoms correspond with the following items on the PANSS (Kay et al., 1987); (P1) delusions; (P2) conceptual disorganization; (P3) hallucinatory behaviour; (N1) blunted affect; (N4) passive apathetic social withdrawal; (N6) lack of spontaneity and flow of conversation; (G5) mannerism/posturing; (G9) unusual thought content. For remission, none of the items should exceed a score of 3 (mild). The time criterion of the remission criteria demands that this low symptom severity remains stable for at least 6 months. At baseline, we only use the severity criterion, since no data on symptom level were available for the period prior to inclusion. At follow-up, we used both the severity criterion and the time criterion to define remission status.
Clinical and functional variables
Symptom severity was measured with the PANSS (Kay et al., 1987). Items were rated on a 7-point scale (1=absent to 7=extremely severe). The PANSS consists of three subscales: positive scale, negative scale and general psychopathology. The level of premorbid functioning was evaluated by the Premorbid Adjustment Scale (PAS) (Cannon-Spoor et al., 1982) in two separate domains, i.e. academic and social. Higher scores indicate worse premorbid functioning.
For the assessment of functional impairment we used the Global Assessment of Functioning scale (GAF) with its psychopathology and impairment scale (American Psychiatric Association, 1992, 2000). Quality of Life was assessed with the World Health Organization Quality of Life (WHO-QoL) scale, a self-report scale that assesses QoL on four major domains (physical health, psychological health, social relationships, environmental conditions) (The WHOQOL Group, 1998). A QoL total score was computed by adding the mean scores of the subdomains (range 5–20). Need for care was assessed with the Camberwell Assessment of Need Short Appraisal Schedule (CANSAS) (Slade et al., 1996, 1999); the CANSAS assesses unmet needs for care on several life domains (range 1–13), i.e. food, self-care, money and daily activities. The PANSS, CANSAS and GAF were rated by trained clinicians.
Statistical analysis
Data were analysed with IBM SPSS Statistics 20.0.
Change-in-remission categories
Four change-in-remission categories were created based on the eight items of the PANSS, obtained at baseline and follow-up measurement: patients who did not fulfil the symptomatic remission criterion throughout the study (NN); patients who did not fulfil the symptomatic remission criterion at baseline patients but did at follow-up (NR); patients who did fulfil the symptomatic remission criterion at baseline but did not at follow-up (RN); and patients who fulfilled remission criteria at baseline and at follow-up (RR) (Table 1).
Measures of functioning and remission status at baseline and follow-up.
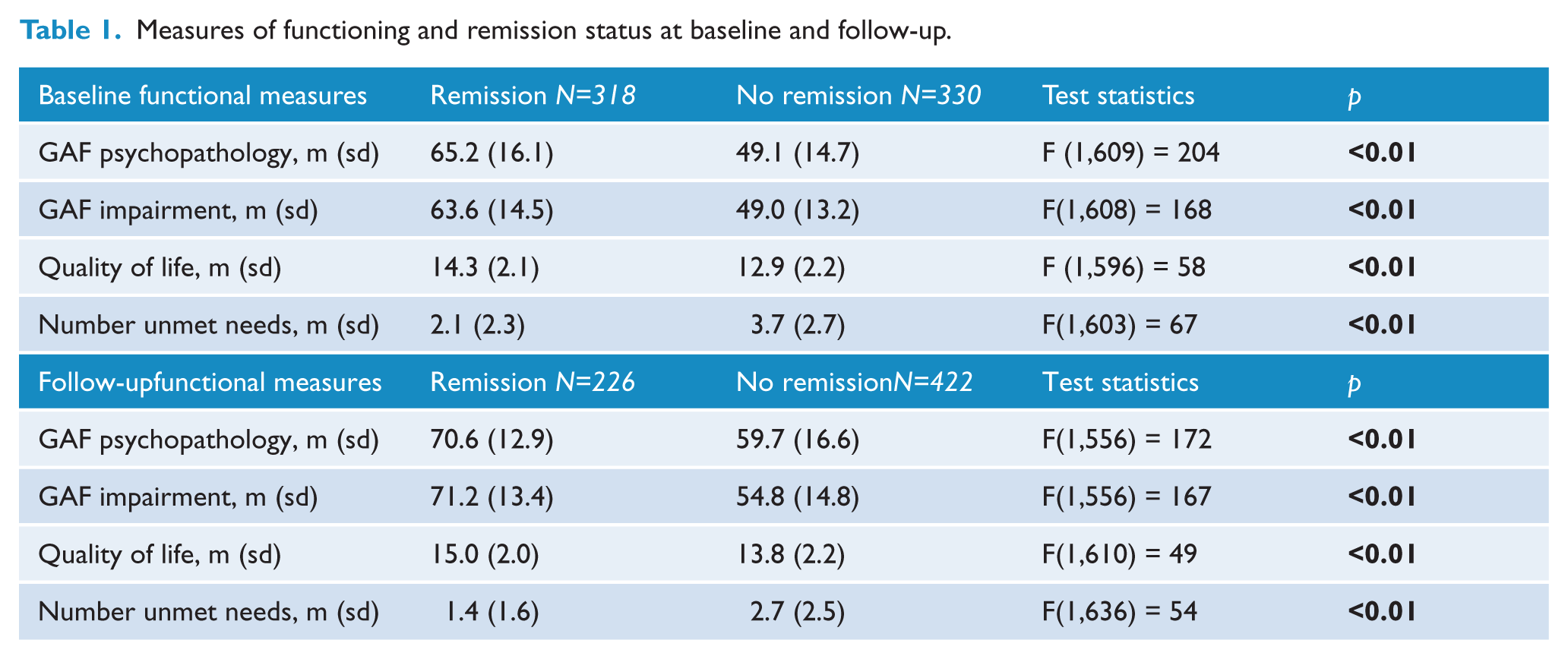
Associations between remission status and functioning, at baseline and follow-up (aim I)
Characteristics of general functioning were compared between patients who were in RSWG remission and those who were not, at both baseline and follow-up measurement separately. We performed one-way analyses of variance (ANOVA) to assess potential differences between patients who did and did not meet remission criteria at either time point on GAF, number of unmet needs and QoL.
Associations between change-in-remission status and baseline functioning (aim II)
One-way ANOVA were performed to compare baseline characteristics of patients with an unfavourable change (compared with stable remission; RR–RN comparison) and favourable change (compared with stable non-remission; NN–NR comparison). Age, sex, IQ, age at illness onset, duration of illness, number of psychotic episodes, living status, paid employment, PAS academic and social scores, as well as baseline GAF, unmet needs for care and QoL were taken in account. Odds ratios (OR) and effect sizes (Cohen’s d) are reported. An effect size below d=0.2 will be considered as small, around d=0.5 as medium, and d=0.8 or above as large (Cohen, 1988).
Associations between change-in-remission status and functional outcome (aim III)
We assessed potential differences between patients in the stable remission (RR) group versus patients in other groups regarding functional outcome at follow-up measurement. Multilevel linear modelling techniques were used to assess potential differences between the category RR and the other three categories in functional outcome variables at follow-up, correcting for baseline functioning. GAF, number of unmet needs for care and QoL at 3-year follow-up were used as dependent variables and change-in-remission category was used as independent variable, while adjusting for baseline value of the functional variables. The RR group was taken as the reference and effect sizes in the multilevel model were expressed as B, representing the fixed regression coefficient.
Functional and clinical outcome in the separate change-in-remission categories (aim IV)
Paired t-tests were performed to investigate changes in functioning and clinical outcome between baseline and follow-up measurement, for each remission category separately. Effect sizes are reported.
Results
Attrition
There were no significant differences between the patients for whom longitudinal PANSS data were available and those with missing follow-up assessment regarding sex, age, diagnosis or illness duration. The attrition group had, however, significantly higher PANSS scores at baseline on the positive, negative and general scale (respectively F(1,993)=13.7, p<0.01; F(1,990)=24.2, p<0.01; F(1,973)=30.7, p<0.01). In addition, the attrition group showed worse scores at baseline on GAF disabilities and unmet needs (respectively F(1,964)=7.6, p<0.01; F(1,965)=7.9, p<0.01), but no significant differences in terms of QoL.
Remission categories
At baseline, 318 (49%) patients fulfilled symptomatic remission criteria and 330 (51%) patients did not. Of the 330 patients who were not in remission at baseline, 260 (79%) were also not in remission at follow-up (NN), while 70 (21%) were (NR). Conversely, of the 318 patients who were in remission at baseline, 162 (51%) moved out of remission (RN) at follow-up and 156 patients stayed in remission at follow-up (RR).
Associations between remission status and functioning, at baseline and follow-up (aim I)
Due to missing values in the dependent variables or covariates, sample sizes for the various analyses varied, as reflected in the degrees of freedom (df). Table 1 shows that both at baseline and follow-up, patients who were in remission had higher GAF (psychopathology and impairment) scores, fewer unmet needs, and better QoL (p’s<0.01) than patients who were not in remission.
Associations between change-in-remission status and baseline functioning (aim II)
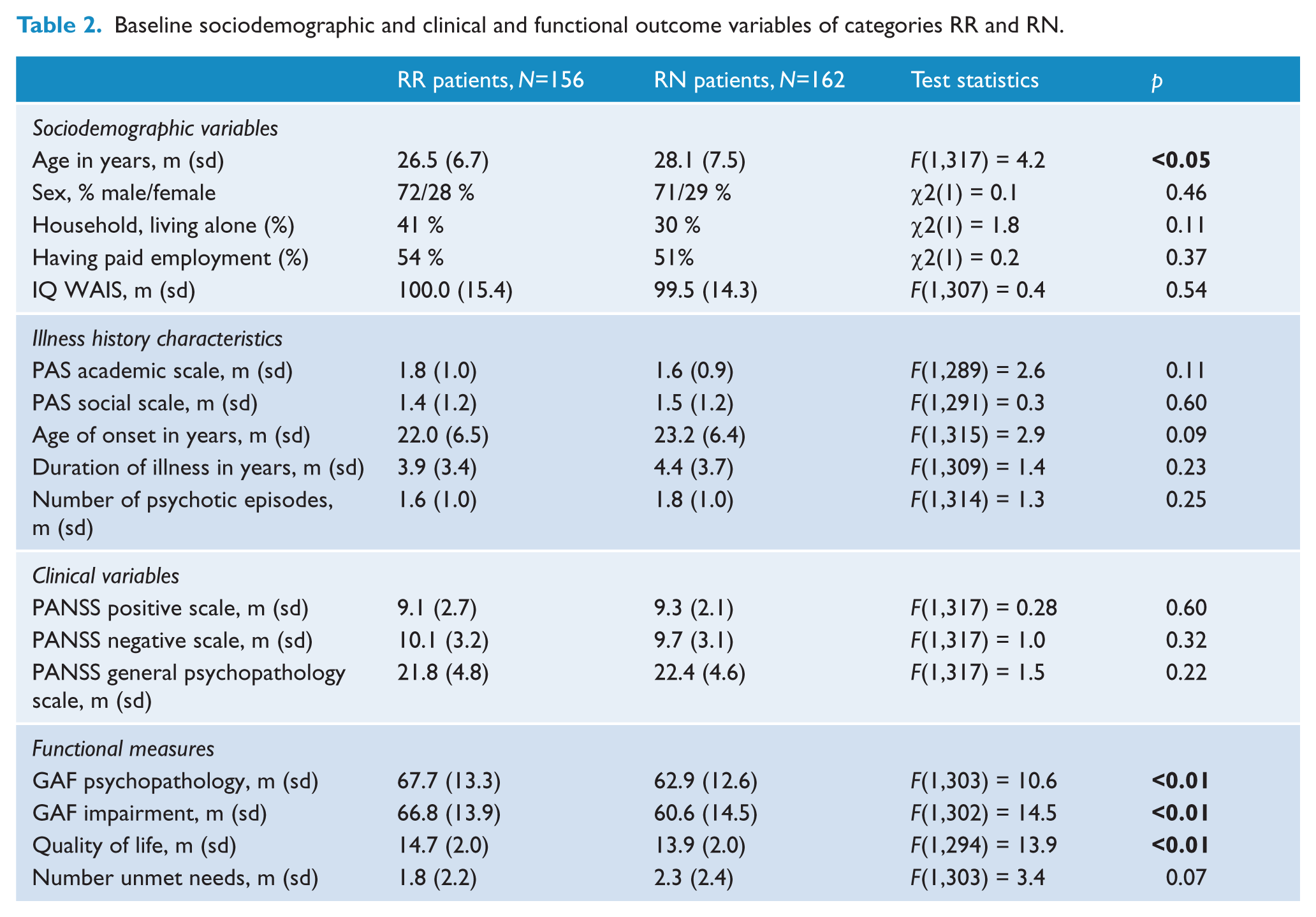
Remission–Remission versus Remission–No Remission
The only significant difference in baseline sociodemographic characteristics and clinical variables between categories RR and RN, was that RR patients were significantly younger (d=-0.22, p<0.05) Patients who lost their remission status at follow-up (RN patients) had significantly more functional impairment at baseline (GAF psychopathology: d=-0.37, p<0.01; GAF impairment: d=-0.43, p<0.01) and significantly worse baseline QoL (QoL: d=-0.40, p<0.01) compared with patients in stable remission (RR patients) (Table 2).
Baseline sociodemographic and clinical and functional outcome variables of categories RR and RN.
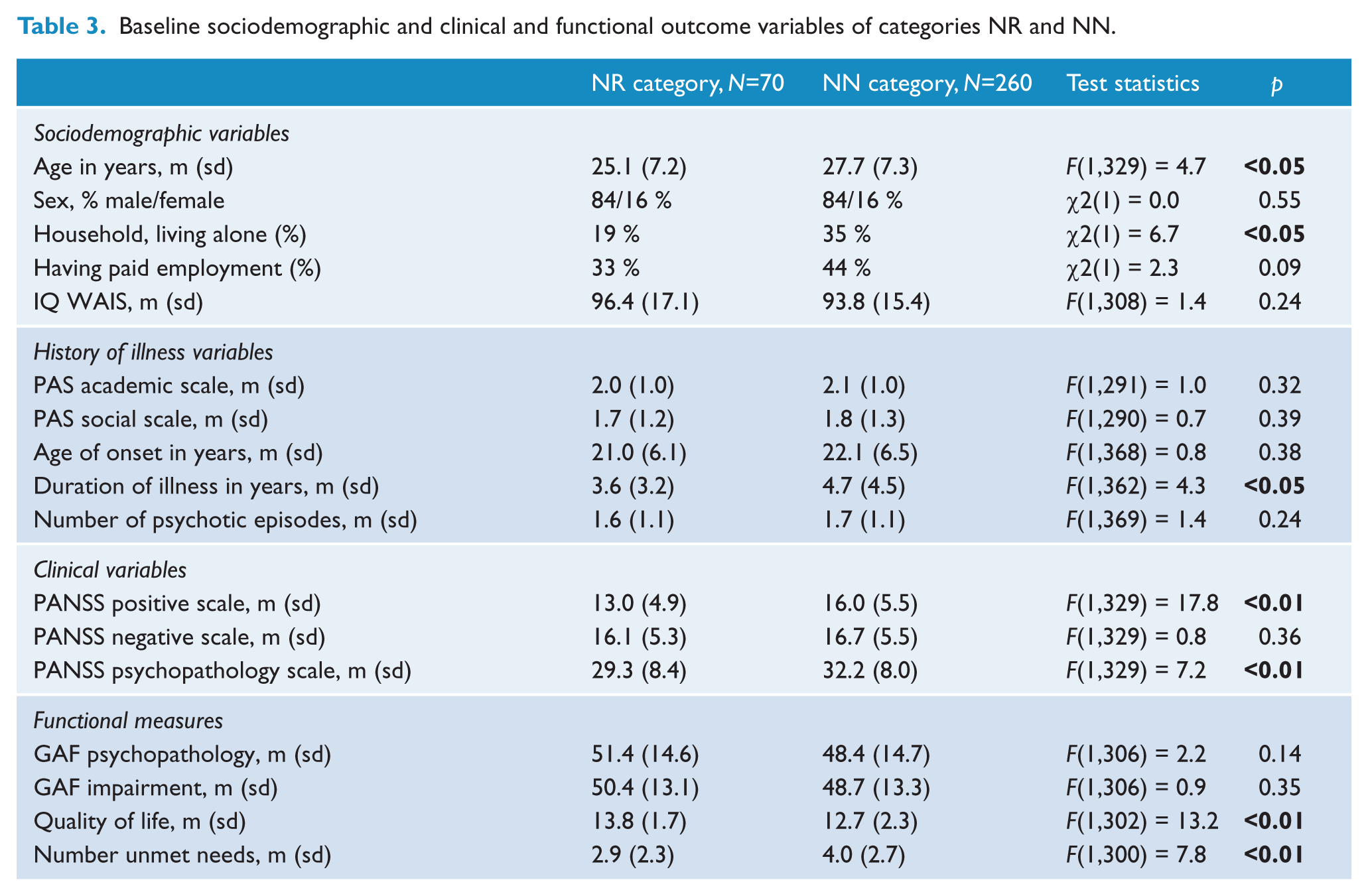
No Remission–Remission versus No Remission–No Remission
At baseline, NR patients were significantly younger (d=-0.36, p<0.05), lived more often with others (OR=0.4; 95% CI=0.22–0.82), had a shorter duration of illness (d=-0.28, p<0.05), showed less severe positive (PANSS positive scale: d=-0.58, p<0.01) and general symptoms (PANSS psychopathology scale: d=-0.35, p<0.01), rated their QoL as higher (QoL: d=0.54, p<0.01), and had fewer unmet needs (CANSAS unmet needs: d=-0.44, p<0.05) as compared with patients in the NN category (Table 3).
Baseline sociodemographic and clinical and functional outcome variables of categories NR and NN.
Associations between change-in-remission status and functional outcome (aim III)
A stable in-remission status (RR) was associated with significantly higher scores on the GAF (both psychopathology and impairment), better QoL, and fewer unmet needs compared with the other three categories. For example, at follow-up measurement GAF impairment scores were about 7 points lower and QoL was 1 point lower in NR patients as compared with RR patients, after adjustment for any baseline differences (Table 4).
Longitudinal remission status and functional outcome.
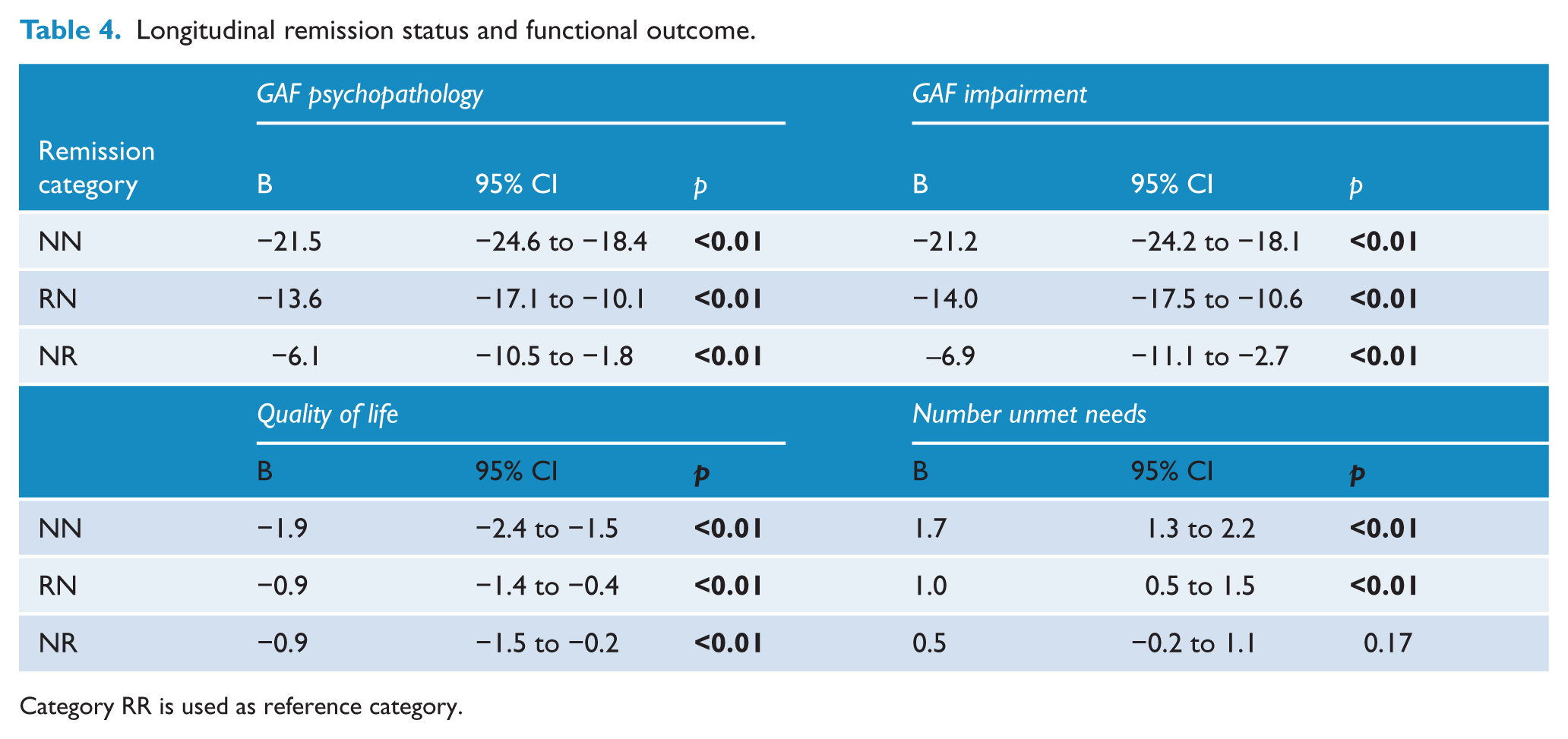
Category RR is used as reference category.
Functional and clinical outcome in the separate change-in-remission categories (aim IV)
Paired t-tests showed that mean GAF scores improved significantly during the 3-year interval in NN patients (GAF psychopathology: d=0.13, p<0.01; GAF impairment: d=0.21, p<0.05) and NR patients (GAF psychopathology: d=0.82, p<0.01; GAF impairment: d=0.88, p<0.01). RN patients showed no significant decline in GAF scores. All categories, however, reported a significant increase in QoL (NN: d=0.32, p<0.01; RN: d=0.27, p<0.01; NR: d=0.40, p<0.01; RR: d=0.34, p<0.01) and a decrease in unmet needs for care (NN: d=0.18, p<0.01; NR: d=0.24, p<0.05; RR: d=0.24, p<0.01) over a 3-year time interval (with the exception of RN patients who showed a small increase of unmet needs, d=-0.04). See Figures 1(a–d).
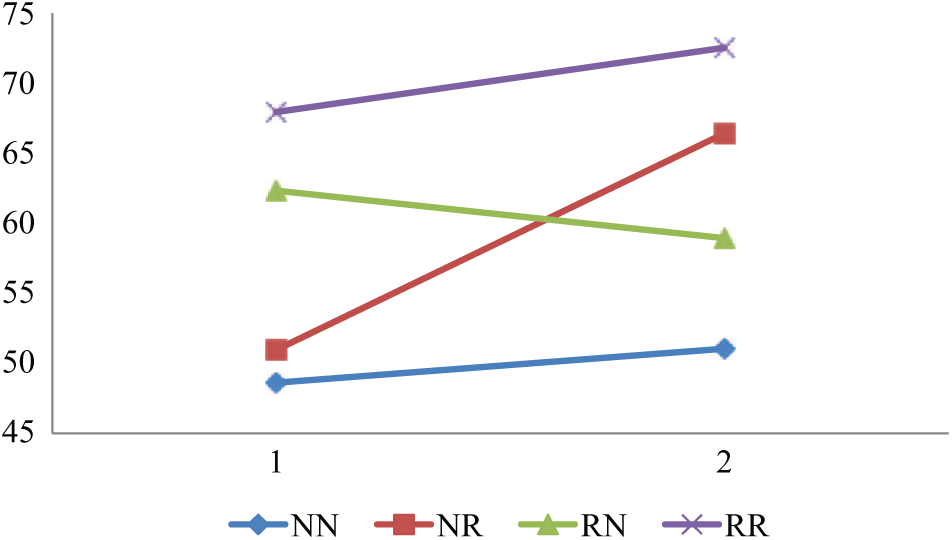
Mean GAF psychopathology.
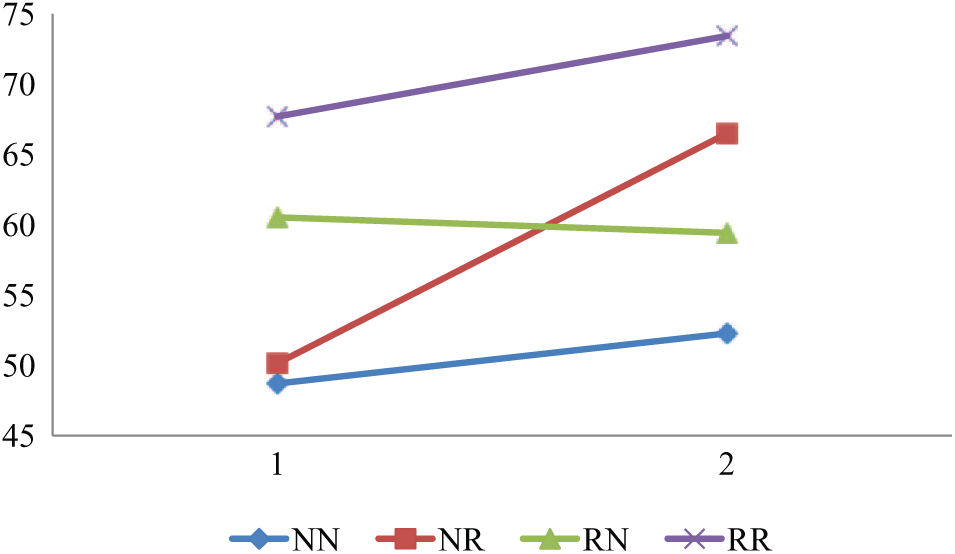
Mean GAF disabilities.
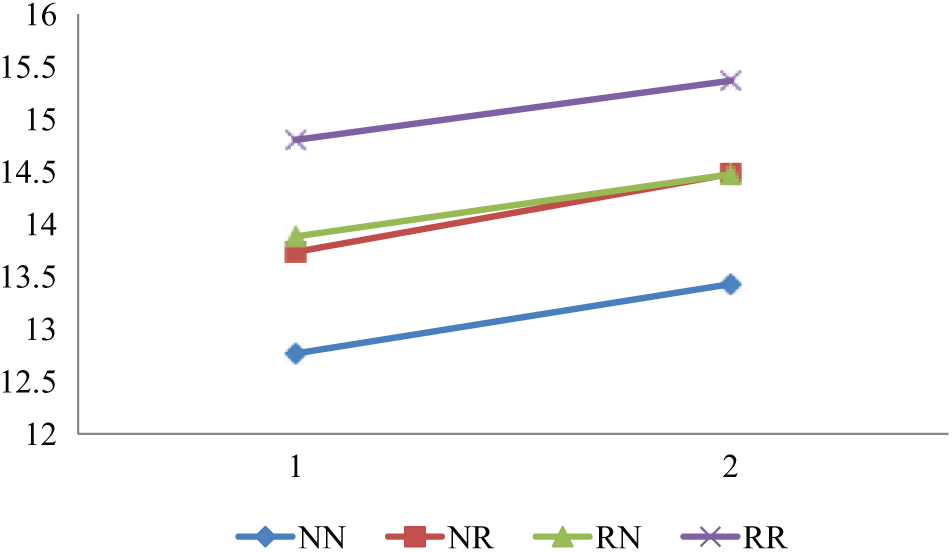
Mean general quality of life.
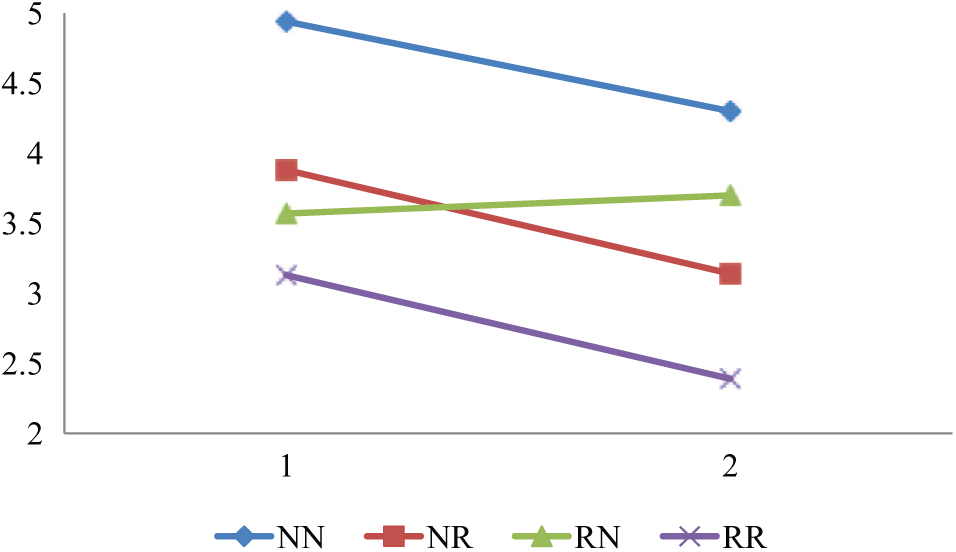
Mean number unmet needs.
Discussion
The aim of this study was to further investigate the validity of the remission criteria for schizophrenia developed by the RSWG (Andreasen et al., 2005) in a naturalistic follow-up study. Unfortunately, in the large sample of patients with a schizophrenia spectrum disorder, achieving remission status was not attainable for the majority of patients. At baseline, 49% of the sample was in remission according to the RSWG; at follow-up this rate was even lower (35%). Nevertheless, the results show a favourable course of overall well-being as all patient categories – on average – increased in QoL and had fewer unmet needs for care at follow-up. This suggests an adaptation in living, despite of ongoing psychopathology, in a sense that patients perhaps are able to adapt to ongoing symptoms, or alternatively this could indicate a lowering of expectations.
First, we showed that both at baseline and at follow-up, patients who obtained RSWG remission status functioned better in terms of global functioning, unmet needs and QoL, which is in line with earlier findings and supports the validity of the RSWG remission criteria (Barak and Aizenberg, 2012; Braw et al., 2012; Chang et al., 2012; Ciudad et al., 2009; De Hert et al., 2007; Eberhard et al., 2009; Lambert et al., 2010; Van Os et al., 2006). Another interesting finding was that we found an association between younger age at baseline and remission status at follow-up, indicating that increasing age at study entry is associated with a greater risk not to reach remission. The most plausible explanation for the relationship is that younger age at baseline is associated with recent episode status and that the propensity of remission in this group is higher than in older patients, who are more likely to be in a later and more chronic stage of the disorder. The association between illness duration and remission status did reach significance for patients who reached remission status only at follow-up (p<0.05).
Second, we showed relevant differences at baseline measurement associated with dynamics in remission status over time, suggesting that predicting which patients are likely to experience subsequent loss of remission status may be possible to a certain degree. Patients who were in remission at baseline but lost this status at follow-up (RN) already showed mean differences in terms of baseline overall functioning and QoL compared with the stable remission group. That is, patients with a stable in-remission status (RR) received showed better functioning and reported a more favourable QoL at baseline assessment than patients who lost the remission status over time. In contrast, these groups could not be differentiated in terms of illness duration and baseline severity of symptomatology. Perhaps low levels of overall functioning and low appraisal of QoL is associated with the risk of worsening of symptoms or even indexes risk of relapse. In contrast, of the patients who were not in remission at baseline, the ones who achieved remission at follow-up (NR) were characterized by a younger age, shorter illness duration and less severe symptoms than patients who did not achieve remission (NN). In addition, NN patients also had more unmet needs and lower QoL appraisal, already at baseline. These findings indicate that group differences in improvement in remission status can be predicted using clinical, psychological and functional outcome measures.
Previous research showed that fewer mental symptoms and less use of mental health services go hand in hand, and that both features are necessary for the pathway towards recovery (Green et al., 2013; Helldin et al., 2009). Recovery not only refers to absence of psychopathology (Andreasen et al., 2005; Bellack, 2006), but also contains elements of subjective appraisal of patients’ satisfaction with life and daily activities, and suitable functioning in everyday life (Bobes et al., 2009; Harvey and Bellack, 2009). In answering our third question, we showed that patients in stable remission (RR) were characterized by these elements. RR patients considered their QoL to be better, they reported fewer unmet needs of care, and clinicians rated their level of functioning significantly higher as compared with patients in other remission categories. This suggests that an enduring state of being without symptoms is essential for improvement in functioning and QoL. RR patients may therefore be considered to be on the road of recovery, although recovery also means adaptation to live ‘beyond’ your symptoms. Previous research using longitudinal information on remission status (Bobes et al., 2009; Van Os et al., 2006) showed similar results, in particular on number of unmet needs for care. Van Os and colleagues (2006) reported that patients with an enduring remission status as compared with patients who moved out of remission at follow-up had fewer unmet needs (around 1.5 fewer). Their findings on QoL appraisal, however, were less substantial than ours (Van Os et al., 2006).
Last, in the current study patients in all change-in-remission categories showed an average increase in QoL, an increase in GAF scores, and a decrease in unmet needs (with the exception for a small increase in unmet needs in the RN group). It must be noted that although substantial functional improvement took place, an average GAF score of 51 in the NN category at follow-up still indicates the presence of symptoms and poor daily life functioning at a moderate to severe level. The improvement in QoL and unmet needs (see Figures 1(a–d)) may partly be an adaptation effect to one’s situation. Ongoing attempts, however, to ameliorate residual symptoms, functional difficulties, and altered life goals remain desirable to achieve further improvement (Bellack, 2006).
Limitations
A first limitation of our study is the fact that we were not able to include the time criterion of remission at baseline assessment; it is possible that patients have moved in or out remission just before baseline assessment. Our findings nevertheless suggest that the symptomatic criterion without the time criterion is valid in terms of its association with functional outcome, as differences between the groups that did and did not meet the symptomatic remission criteria were similar at baseline and follow-up assessment. Another limitation is lack of information on symptom severity during the interval with exception of 6 months prior to follow-up assessment (the time criterion). Perhaps patients in the RR and NR category did experience a relapse prior to this time frame, so that the ‘enduring’ state of being without symptoms represents a misclassification. A third limitation is that follow-up assessment was not possible for all patients assessed at baseline and that the attrition group was characterized by more severe symptomatology at baseline. Had these patients been included at follow-up assessment, results for overall improvement (aim IV) would perhaps have been different. However, bias would only have arisen if attrition would have been contingent not only on baseline psychopathology, but on differential associations between psychopathology and QoL and functioning, which is unlikely.
Conclusion
We have replicated and extended earlier evidence in support of the validity of the concept of RSWG remission. We found associations between various functional and clinical variables and the RSWG remission criteria, providing support for the RSWG remission criteria to be used as a valid outcome measure in research and clinical settings. Our findings highlight furthermore that achieving and maintaining RSWG remission occurs in only a small percentage of patients with schizophrenia or a related disorder. Nevertheless, improvement in (patient-reported) functional measures over time, regardless of remission status, suggests growing adaptation and self-management, and the possibility of improving satisfaction with life despite ongoing difficulties.
Footnotes
Acknowledgements
Genetic Risk and OUtcome of Psychosis (GROUP) Investigators: Richard Bruggeman, Wypke Cahn, Lieuwe de Haan, René S Kahn, Carin J Meijer, Inez Myin-Germeys, Jim van Os and Durk Wiersma.
Funding
This work was supported by the Geestkracht program of the Dutch Health Research Council (ZON-MW, grant number 10-000-1002) and matching funds from participating universities and mental health care organizations (Site Amsterdam: Academic Psychiatric Centre AMC, Ingeest, Arkin, Dijk en Duin, Rivierduinen, Erasmus MC, GGZ Noord Holland Noord; Site Utrecht: University Medical Centre Utrecht, Altrecht, Symfora, Meerkanten, Riagg Amersfoort, Delta; Site Groningen: University Medical Centre Groningen, Lentis, GGZ Friesland,GGZ Drenthe, Dimence, Mediant, GGNet Warnsveld, Yulius Dordrecht and Parnassia psycho-medical centre; Site Maastricht: Maastricht University Medical Centre, GGZ Eindhoven, GGZ Midden-Brabant, GGZ Oost-Brabant, GGZ Noord- Midden Limburg, Mondriaan Zorggroep, Prins Clauscentrum Sittard, RIAGG Roermond, Universitair Centrum Sint-Jozef Kortenberg, CAPRI University of Antwerp, PC Ziekeren Sint-Truiden, PZ Sancta Maria Sint-Truiden, GGZ Overpelt, OPZ Rekem). The analyses were supported by unrestricted grants from Jansen-Cilag, Eli Lilly and Company, Astra-Zeneca and Lundbeck. The research leading to these results has received funding from the European Community’s Seventh Framework Program under grant agreement No. HEALTH-F2-2009-241909 (Project EU-GEI).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.