
Abstract
Objective:
Cognitive remediation is an intervention to overcome cognitive deficits through drills and use of strategies. Previous studies have reported positive effects for cognitive remediation on neurocognition, but researchers’ allegiance effects are not always adequately controlled. Furthermore, its efficacy amongst the Asian population has not been established. Hence, this study aimed to determine if cognitive remediation would have positive effects on neurocognition and functioning within an English-speaking Asian population, when compared against the effects of a credible and balanced control provided by therapists blinded to the study hypothesis.
Method:
A total of 70 participants with schizophrenia who attended vocational training or day rehabilitation programmes were randomised to receive a 60-hour programme of either cognitive remediation or physical exercise. Neurocognition and functional outcomes were measured at baseline, upon completion of treatment, 6 months after treatment and 1 year after treatment.
Results:
Participants who received cognitive remediation had significantly greater improvement in all neurocognitive domains. Furthermore, the cognitive remediation group achieved greater attainment of vocational or independent living skills and better functional outcomes at post-intervention and at the end of the 1-year follow-up.
Conclusions:
When compared against a credible intervention such as physical exercise, cognitive remediation was able to show significant positive effects on both neurocognition and functional outcomes among the Asian population of schizophrenia patients.
Keywords
Introduction
Cognitive remediation (CR) refers to interventions designed to overcome the effects of cognitive deficits with the objective of achieving general improvement (Tomás et al., 2010; Wykes et al., 2011). Such programmes often focus on restoring cognitive functioning and/or compensating for the effects of deficits. The restorative approach seeks to improve performance in cognitive domains through exercises that challenge particular neural processes (Dirette et al., 1999; Kern et al., 2009). The compensatory approach, on the other hand, minimises the negative impact of compromised cognitive functioning through self-management strategies, task modification or the use of aids and environmental adaptations (Tawmley et al., 2008). CR can be conducted through group work, paper and pencil exercises, or via the computer modality (Delahunty and Morice, 1993; Medalia et al., 2009; Twamley et al., 2008. It may take the form of drill and practice where participants repeat the exercises until they reach proficiency, or strategy learning where participants acquire skills to accomplish the cognitive tasks successfully (Hurford et al., 2011).
Recent meta-analyses have demonstrated the efficacy of CR on both neurocognition and functional outcomes among people with a diagnosis of schizophrenia (McGurk et al., 2007; Wykes et.al., 2011). Earlier randomised controlled trials tend to use treatment-as-usual or waiting lists as controls, failing to control for the non-specific benefits of therapist contact (Hodge et al., 2010; Lopez-Luengo and Vázquez, 2005; Sartory et al., 2005). Other studies have used non-therapeutic controls such as video viewing, computer typing or computer games, although one study utilised occupational therapy as a control intervention (Albertella et al., 2008; Fisher et al., 2009; Medalia et al., 1998; Wykes et al., 1999). However, interventions that lack bona fide credentials may not achieve non-specific or placebo treatment effects (Thase, 1999).
The study reported here was designed to add to our existing knowledge of the impact of CR on functional outcomes for people with a diagnosis of schizophrenia, by implementing this treatment in an English-speaking Asian country. The CR treatment conducted in this study pulled together elements that were found to be effective in previous research, such as the combined use of restorative and compensatory approaches, as well as the emphasis on generalisation to daily functioning (Medalia et al., 2009; Twamley et al., 2008’.; Wykes et al., 2011). To provide a credible alternative placebo intervention, a physical exercise (PE) programme was utilised as the control treatment. PE not only improves activity tolerance through better cardiovascular fitness, it also improves self-esteem and reduces negative symptoms such as social withdrawal (Hutchinson et al., 2005; Richardson et al., 2005). PE may also reduce perceptions of positive symptoms, alleviate anxiety and depression, and improve social functioning (Hutchinson et al., 2005; Pelletier et al., 2005). Selecting PE as the comparison group meant that CR would need to show clear and specific advantages over this competing intervention that offered potential benefits to participants. In addition, this study also attempted to control for allegiance effects. Luborsky et al. (1999) suggested that a researcher’s allegiance may influence the outcomes of treatment studies through selection of a less effective competing treatment (or treatment-as-usual), selection of therapists who are less skilful to implement the placebo treatment, or through boosting the morale of therapists who are engaged in the experimental treatment. Therefore, appropriate blinding procedures were implemented in this study to minimise such allegiance effects. Moreover, a follow-up period of 1 year was put in place to determine the durability of treatment effects. It was hoped that this design would ensure a more rigorous test of specific and sustained efficacy of CR.
This study hypothesised that participants from the CR group would show significantly greater improvement in neurocognition than participants from the PE group at the end of the 1-year follow-up. A second hypothesis was that participants who underwent CR would achieve better overall functional outcomes (longer employment hours or greater improvement in community ability) than participants in the PE group.
Methods
Sample
All participants were recruited from the Institute of Mental Health, Singapore. Its occupational therapy department offered two types of outpatient rehabilitation programme: vocational training and day rehabilitation. Vocational training consisted of a 3-month transitional employment phase and a 1-year supported employment phase. At the transitional employment phase, participants could select from a number of transitional employment projects, ranging from food and beverage, retail, car wash, clerical and cleaning. These transitional employment programmes were conducted within the hospital campus. Through transitional employment, they acquired basic vocational skills and behaviour that were required in the competitive job market. Upon completion of the transitional employment phase, supported employment was implemented for up to 1 year. Participants were assisted in securing competitive employment and ongoing support during employment was provided. Occupational therapists would provide support weekly for the first month, fortnightly during the second month and monthly thereafter. They also performed job site visits, vocational counselling and job coaching.
The day rehabilitation programme consisted of group sessions that promoted community independence, social interaction, a healthy lifestyle and engagement in creative activities. Patients usually stayed within this programme for a few years, unless they wished to move on to vocational training or open employment. Participants in this research study stayed for at least 1 year and 3 months. Each participant had an occupational therapist who also acted as his/her case worker.
All patients with Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnoses of schizophrenia or schizoaffective disorder, as certified by a psychiatrist, who were referred to the vocational training or day rehabilitation programme between August 2007 and December 2009 were invited to participate in the study. However, patients with known neurological, cardiovascular and respiratory diseases as well as developmental disabilities were excluded. All participants also had a Global Assessment of Functioning score of above 30.
Ethics approval was obtained from the National Healthcare Group Domain-Specific Review Board, which was the institution’s ethics review board. At the same time, approval was also obtained from the University of Queensland Behavioural and Social Sciences Ethical Review Committee. Once informed consent was obtained from participants, they were randomised to receive either CR or PE.
Experimental group – cognitive remediation (CR)
CR consisted of computer-assisted cognitive exercises, as well as cognitive-based counselling.
Computer-assisted cognitive exercises
The computer-assisted cognitive exercises were conducted for up to 5 hours (three sessions) each week for 12 weeks. Two of the sessions were 2 hours each, while the third session was an hour in duration. The sessions were conducted in groups, with a maximum of six participants. Participants were given monetary incentives of S$1.50 per hour of engagement in the computer cognitive exercises. The content, frequency and duration of implementation were adapted from Bell and colleagues’ Neurocognitive Enhancement Therapy (NET) (Bell et al., 2005). Odie Bracey’s Psychological Software Services CogRehab software was used to provide the computer cognitive exercises (Bracy, 1995). A total of 52 computer exercises were selected from this software to enable repeated practice on attention, memory and executive function. A ‘PSS Cognitive Rehabilitation Software Exercise Booklet’ was devised and it contained exercises that were planned for each session, with columns for participants to chart their progress. For each computer exercise, its therapeutic objectives were clearly indicated, with goals that participants could work towards. Moreover, the parameters of most exercises could be adjusted to increase their difficulty levels. When participants were able to achieve 90% accuracy at a given difficulty level, the task was made more difficult based on a pre-set hierarchical level of difficulty.
Although the mode of computer-based exercises was repeated drills, the presence of therapist’s input ensured that participants acquired strategies that led to achievement of goals. Some of these strategies were indicated in the PSS Cognitive Rehabilitation Software Exercise Booklet, while others could be devised by the participants and their therapists. Besides teaching strategies, the role of a therapist was to provide scaffolding and positive reinforcement, so as to improve motivation to acquire these cognitive strategies.
Cognitive-based counselling
In addition to the computer exercises, participants received cognitive-based counselling fortnightly. This was conducted by therapists in charge of their rehabilitation programmes, who received information from the CR therapists about the progress of the participants’ computer exercise sessions. The therapists and participants identified any problems they encountered during vocational training or day rehabilitation as a result of cognitive difficulties. The relevance of strategies learned during the computer sessions to vocational training or day rehabilitation was then discussed. This was to enhance the transfer of cognitive skills in the computer training exercises and to minimise the effects of any persisting cognitive impairment that interfered with daily life. Based on the identified problems, participants developed goals for improvement in the computer exercise sessions and vocational training/day rehabilitation programme. This was an extension of the Vocational Cognitive Rating Scale Feedback component of NET and was similar to bridging sessions implemented in the Neuropsychological and Educational Approach to Remediation (NEAR) (Medalia et al., 2009).
Upon completion of the 12-week treatment, therapists continued to provide monthly support to participants in the use of cognitive strategies for a further 12 months. In these sessions, they identified cognitive challenges in participants’ daily lives and coached participants in cognitive strategies to overcome these challenges. Besides self-management strategies, task modifications as well as the use of external aids could also be adopted. Outcomes were reviewed and strategies modified if appropriate.
Comparison group – physical exercise (PE)
The PE programme was adapted from the Structured Exercise Programme implemented by the Centre for Psychiatric Rehabilitation at Boston University (Hutchinson et al., 2005). To match the treatment intensity and duration of CR, the PE programme was also carried out for 5 hours (three sessions) per week over 12 weeks.
The PE programme consisted of exercises in the gymnasium, as well as physical-based counselling.
Physical exercises in the gymnasium
Physical exercises in the gymnasium, involving aerobic, weight training and agility exercises, were conducted. Participants were given monetary incentives of S$1.50 per hour of engagement in the physical exercises. During aerobic training, participants could choose between using the stationery bicycle, the step-machine and the treadmill. They also engaged in brisk walking. The objectives were to increase cardiovascular capacity and improve activity tolerance.
For the weight-training component, participants received graded training using dumbbells, chest press, shoulder press and the row machine. The purpose was to build muscular strength and endurance. In addition, agility training was conducted through trampoline exercises and shuttle runs using agility rings and poles. This was to improve body control and kinaesthetic awareness.
A therapist who had experience with conducting PE devised the ‘Protocol of Physical Exercise’. This protocol was adhered to by all therapists who were trained to conduct the programme. Besides training participants in the various exercises, the role of a therapist was also to provide scaffolding and positive reinforcement, so as to improve motivation to engage in the regime. The participants recorded their own progress and therapists provided encouragement. As the sessions were conducted in a group of not more than six, the therapists used group cohesion to support and motivate participants.
Physical-based counselling
This was conducted in exactly the same format and intensity as the cognitive-based counselling, except that participants identified problems caused by physical limitations or activity intolerance. Physical strategies were then implemented to optimise functioning. This enhanced the transfer of strategies in the PE programme so as to minimise the physical difficulties experienced in daily life. In the course of counselling, participants developed goals for improvement in the PE sessions and vocational training/day rehabilitation programme.
Upon completion of the 12-week PE programme, therapists provided participants with monthly support for a further 12 months. This support focused on the use of physical strategies to optimise work and daily functioning. Difficulties in work tolerance were identified and physical strategies that could be adopted for use to overcome them were developed. The outcomes of utilising these strategies were then evaluated and modified if appropriate.
Measurements
Neurocognitive and physical fitness tests
Neurocognitive tests were selected based on previous studies that had found them to be sensitive to the effects of CR (Burda et al., 1994; McGurk et al., 2005; Vauth et al., 2005). The neurocognitive tests were administered at baseline, at the end of the 3-month treatment, 6 months after treatment, as well as 1 year after treatment.
The Comprehensive Trail Making Test (CTMT) was administered to measure immediate information processing, psychomotor speed and appreciation of sequences (Reynolds, 2002). Trail 5 of this test is a test of the mental flexibility aspect of executive function as it requires participants to connect consecutively numbered and lettered circles, thus testing flexibility in integrating numerical and alphabetical series (McGurk et al., 2005). The Rey Auditory Verbal Learning Test (RAVLT) was used as a test of verbal memory (Schmidt, 2004). Its delayed recall and word recognition component further measures memory retrieval. Alternative forms of RAVLT were used at post-intervention and follow-ups to minimise practice effects. Lastly, the Wechsler Adult Intelligence Scale (WAIS)-Digit Span Forward and Backward was administered as a test of attention and working memory, respectively (Wechsler, 1981). Improvement in WAIS Digit Span Backward was often obtained following CR in previous studies (Bell et al., 2005; McGurk et al., 2005).
The Rockport Walking Test is a widely used self-paced test to evaluate aerobic fitness (Heyward, 2006). It requires participants to walk 1 mile as fast as possible, without jogging or running. Time taken to complete the route, peak heart rate upon completion, weight and age are then used to compute the VO2 max. VO2 max is the maximum amount of oxygen one can use in 1 minute per kilogram of body weight. Hence, the higher the VO2 max, the better the fitness (Heyward, 2006). This test was carried out at baseline and upon completion of CR or PE.
Assessment of skills attainment following treatment
Different measures were required to assess skills attainment among participants within the vocational training and day rehabilitation cohorts. The Work Behaviour Inventory (WBI) was administered for the vocational training cohort by the vocational training therapists, while the Independent Living Scales (ILS) was administered within the day rehabilitation cohort by the principal investigator. WBI is a work performance assessment and consists of five subscales: work habits, work quality, personal presentation, cooperativeness, and social skills (Bell et al., 2003; Bryson et al., 1999). The ILS is a performance-based assessment of instrumental activities of daily living essential for community living (Loeb, 1996). It has five subscales: memory/orientation, managing money, managing home and transportation, health and safety and social adjustment (Loeb, 1996). The five subscale scores can be added and a Full Scale Standard score computed.
These two measurements were administered at baseline and upon completion of the 12-week treatment.
Functional outcomes measurements
Participants involved in the vocational training programme were given job placement assistance once they completed transitional employment training. Such placements were in open employment with the support of vocational specialists. The number of hours in open employment, as well as the amount of salary earned was recorded throughout the post-treatment follow-up. If participants changed jobs during the follow-up period, their total number of hours worked within each job was ascertained and the total number of hours worked at the various jobs was combined.
Community functioning outcome for the day rehabilitation cohort was delineated by changes in community ability as measured by the Multnomah Community Ability Scale (MCAS). The MCAS is a clinician-rated scale and consists of 17 items grouped into four domains: health, adaptation, social skills and behaviour (Barker et al., 2004). Total scores are computed to give an overall level of community ability. The MCAS was administered by each participant’s case worker therapist at the day rehabilitation programme at baseline, post-treatment, as well as 6 months and 1 year after treatment.
Other outcome measurements
The Positive and Negative Syndrome Scale (PANSS) was administered to determine the symptom severity of participants over the course of the research study. PANSS is a 30-item rating instrument, which evaluates the presence and severity of positive, negative and general psychopathology of schizophrenia (Brown, 2003; Kay et al., 1987). The total PANNS score, as well as the negative subscale score, were recorded at baseline, 6 months after intervention and 1 year after intervention, so as to compare symptomatology as well as the severity of negative symptoms between the two groups of participants.
The World Health Organization Quality of Life Scale-Brief (WHOQOL-Brief) is a shorter version of the WHOQOL-100, which is a World Health Organization instrument for evaluating quality of life (Kaneda, 2002). It consists of four dimensions: physical, psychological, environmental and social relations. It was administered alongside PANNS at the three time points and their changes compared between the CR and PE group.
Blinding procedures to minimise allegiance effects
During randomisation, a biostatistician independent to the study generated a random allocation of treatment using the computer. This sequence was placed in numbered sealed envelopes and given to co-investigators who recruited the participants. Eligible participants were then requested by a co-investigator to pick a sealed envelope that contained their treatment allocation. Records of participants’ treatment allocation were inaccessible to the principal investigator and she was not present during all interventions.
The recruiting therapists, vocational training/day rehabilitation therapists as well as the therapists involved in conducting CR and PE were not involved in administering the neurocognitive and Rockport Walking tests. Three therapists were involved in conducting the CR and another three therapists were involved in conducting the PE. These therapists were equal in qualifications and experience and received an equal amount of training before implementing their treatment, so as to ensure a similar quality of intervention as much as possible. The treatment protocol was also devised for both interventions for therapists to adhere to. In addition, all therapists were told that CR and PE were interventions likely to yield benefits to participants and that the efficacy of both interventions was under investigation in this study. Hence, all therapists and participants were informed that the topic of the research study was ‘The effects of CR and PE on functional outcomes among people with schizophrenia’. They were not told that the CR was the treatment that was being researched and that PE was the placebo treatment.
The principal investigator was responsible for baseline and outcome measurements. In order to reduce rater bias, the principal investigator was blinded to the group allocation and did not collect data on the participants’ functional outcomes and had no role in treatment or rehabilitation programmes.
Sample size calculation and data analyses
Based on previous related literature, it was estimated that recipients of CR would achieve job tenure three times greater than that achieved by those who did not receive CR (Bell et al., 2005; McGurk et al., 2005). Prior to the research study, the average estimated job tenure of a vocational training patient at 1 year post-transitional employment was 160 hours. Hence, it was estimated that participants at the intervention arm of this research would achieve 480 hours of job tenure. The effect size was calculated to be 0.9. Assuming a power of 80%, Type 1 error of 5%, and taking into account an attrition rate of 20%, a minimum of 50 participants were to be recruited for both arms.
The SPSS (Version 20.0) statistical package was used to present the demographic profile, calculate the descriptive statistics and analyse the data (IBM Corp., Armonk, NY, USA). The Expectation-Maximisation method was used to impute missing data due to attrition. The method capitalises on the relationship between missing data and the unknown parameters of a data model, so as to apply an iterative method to predict the missing values based on assumed values for the parameters (Schafer and Olsen, 1998). The Expectation-Maximisation method was chosen because it was an efficient, readily available approximate solution with good properties that was easy to implement (Schafer, 1999). The significance level was set at 0.05 and all tests were two-tailed.
Prior to main effects analyses, a group comparison (CR versus PE) of all baseline measures was conducted to identify covariates for post-hoc control. The General Linear Model (GLM) Repeated Measures ANOVA was used to investigate neurocognitive changes over time (baseline, post-intervention, 6 months after intervention and at 1 year post-intervention).
To analyse for differences in skills attainment, changes in WBI scores between the two arms of the vocational training cohort, as well as changes in ILS Full Scale Standard scores between the two arms within the day rehabilitation cohort were analysed using the Independent Samples Mann–Whitney U test, since these scores were not normally distributed (Vickers, 2005). Similarly, for functional outcomes, the Mann–Whitney U test was also conducted to test for differences in open employment hours and salary earned between the two groups within the vocational training cohort. Repeated Measures ANOVA was used to investigate changes in MCAS, PANNS and WHOQOL-Brief scores between the two groups over the various time points.
Results
Participants’ demographics and baseline data
A total of 70 participants were recruited between August 2007 and December 2009. These participants were followed up for a year after the 3-month intervention, hence data collection ended in March 2011. There were 36 participants randomised to CR while 34 were randomised to PE. Of the 36 participants in CR, 19 were from the vocational training cohort while 17 were from the day rehabilitation cohort. In the PE group, 17 participants were from vocational training and the remaining 17 were from the day rehabilitation cohort. Pearson’s chi-squared analysis yielded no significant differences between the distribution of participants from the two cohorts between the CR and PE groups: χ2 (1, n = 70) = 0.54, p = 0.816. There were no group differences in any of their demographic factors, cognition and physical fitness, as detailed in Table 1.
Baseline comparisons of demographic variables and cognition between cognitive remediation (CR) and physical exercise (PE) group.
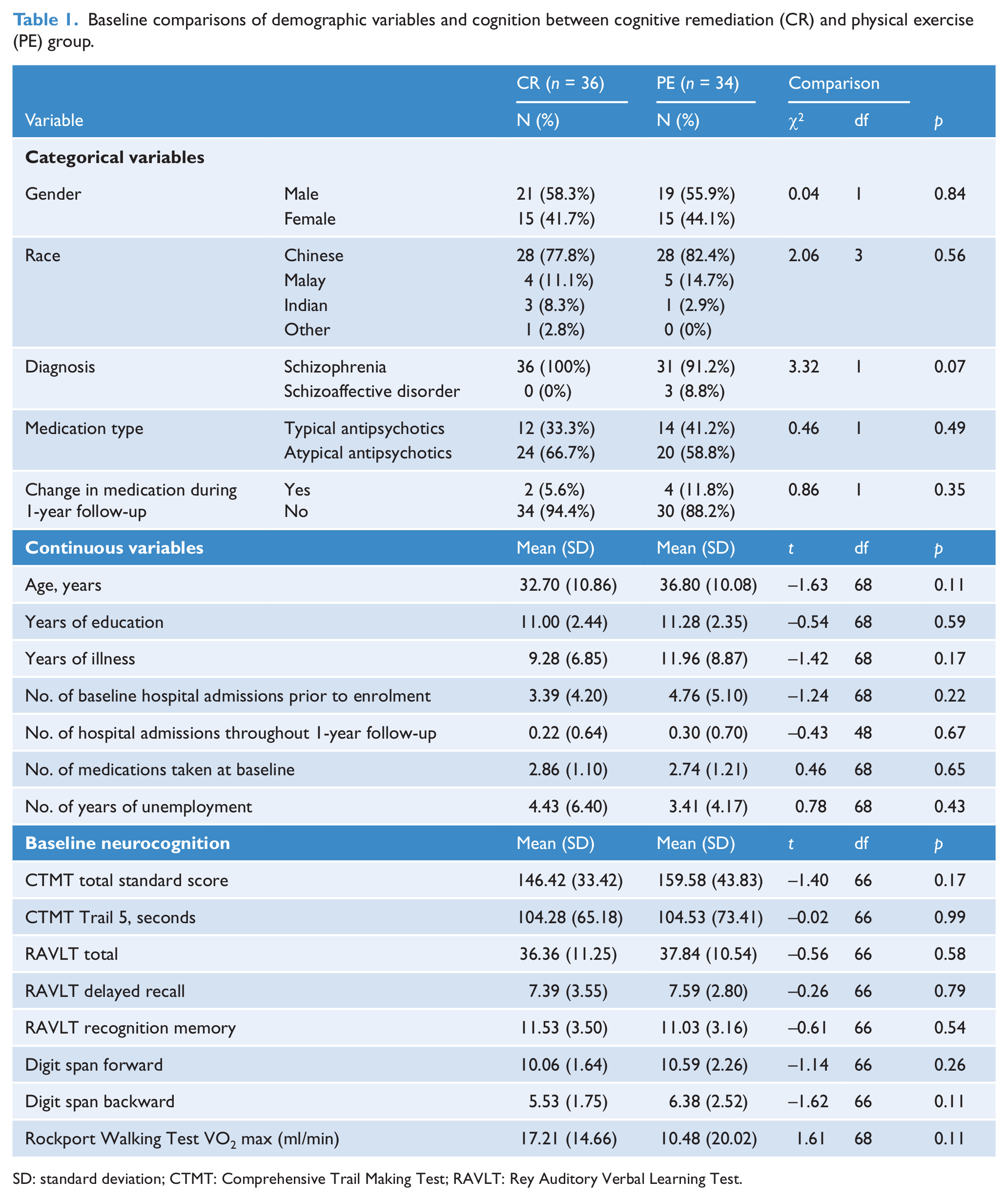
SD: standard deviation; CTMT: Comprehensive Trail Making Test; RAVLT: Rey Auditory Verbal Learning Test.
However, there were significant differences in scores in the ILS-Problem Solving subscale, U = 208.50, Z = 2.27, p = 0.02 and the MCAS, U = 207.50, Z = 2.18, p = 0.03, both favouring the PE group.
Attrition of participants
Figure 1 shows the CONSORT flow diagram of the study. A total of 20 participants dropped out without completing the 60 hours of intervention. As a result, the mean intervention hours clocked by the participants was 45.15 hours. Four participants withdrew during follow-up. There were no significant differences in drop-out rates between the two groups at both intervention and follow-up period. However, the Mann–Whitney U test found that participants who withdrew during follow-up had significantly lower scores in RAVLT Total, U = 157.50, p = 0.02, RAVLT Delayed Recall, U = 146.50, p = 0.05 and RAVLT Recognition scores, U = 161.00, p = 0.01, indicating poorer verbal learning at post-intervention.
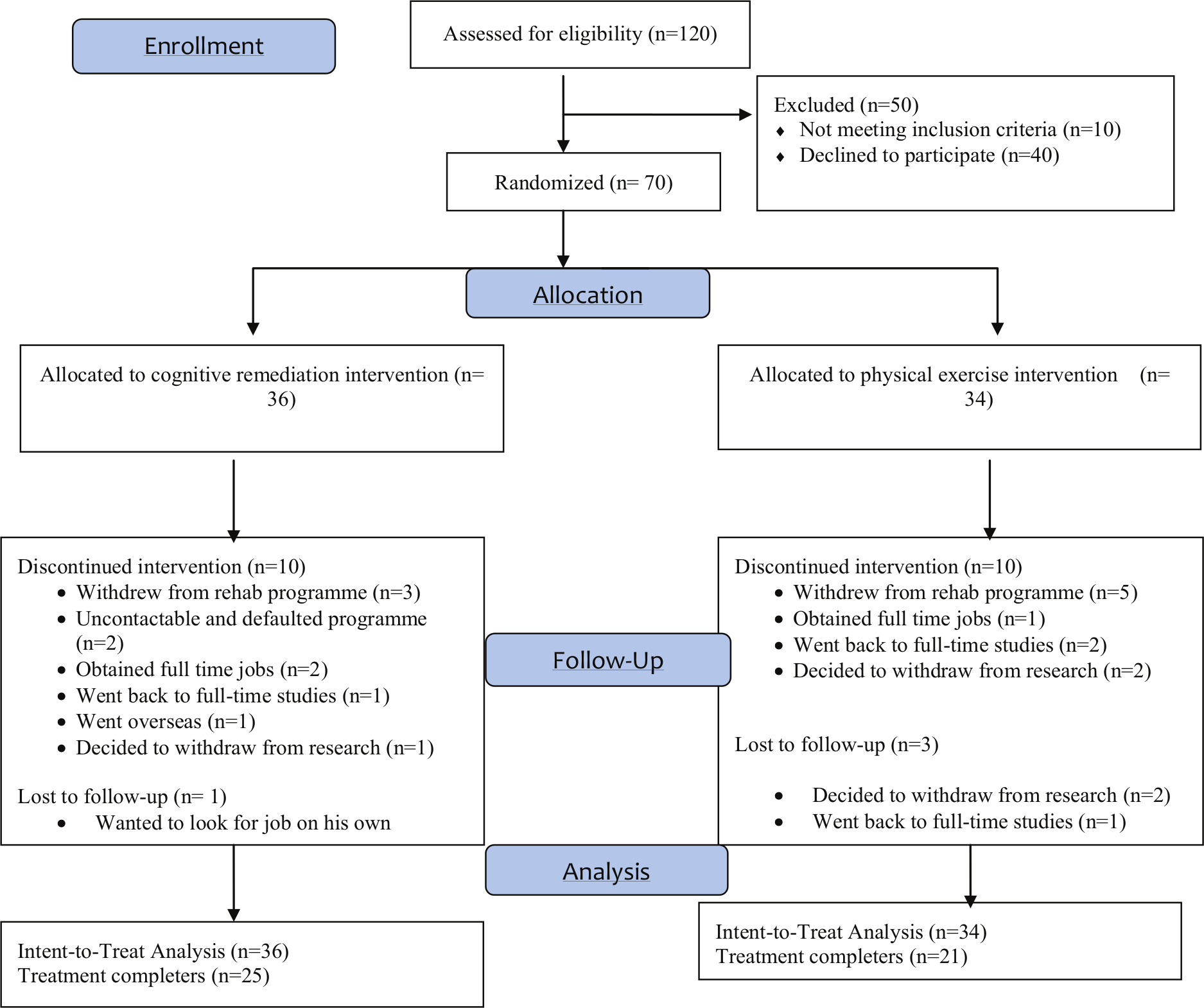
CONSORT flow diagram.
Differential effects of CR and PE on neurocognition and physical fitness
Effects on neurocognition
Repeated Measures ANOVA analyses were employed between the two groups (CR and PE) at the four time points. As multiple comparisons were done for the time factor, a post-hoc Bonferroni adjustment was made for the p value. Results showed significant improvement over time for the sample as a whole in all measures except the RAVLT Recognition score. Table 2 shows the details. There was also significantly more improvement in scores over time amongst the CR group, as shown by the significant time-by-group interaction effects and partial eta-squared scores.
Repeated measures for mean scores on cognitive performance by group (CR and PE) for baseline, post-intervention and 6-month and 1-year follow-ups.
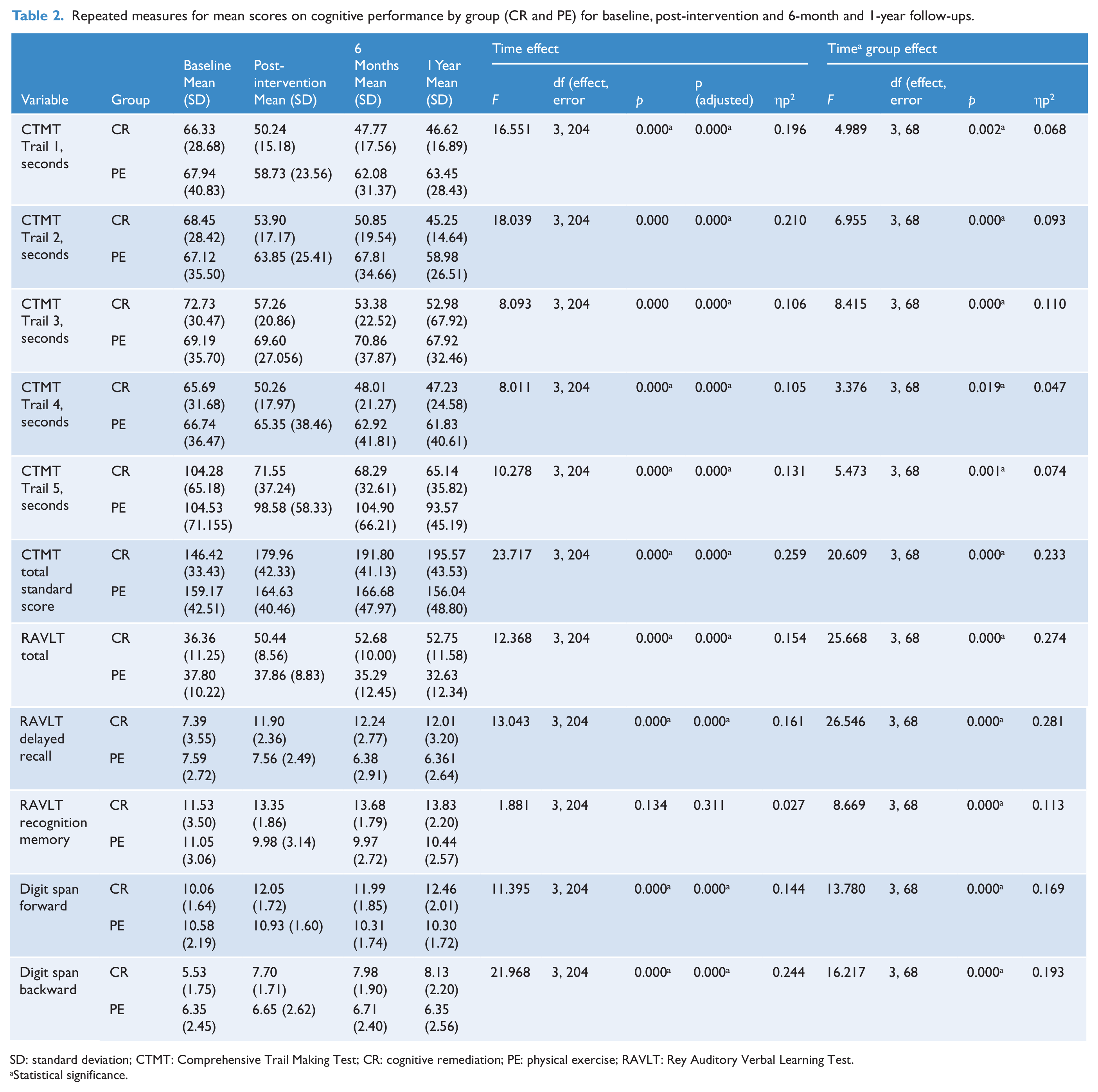
SD: standard deviation; CTMT: Comprehensive Trail Making Test; CR: cognitive remediation; PE: physical exercise; RAVLT: Rey Auditory Verbal Learning Test.
Statistical significance.
From Table 2, it was clear that the CR group showed greater improvement on all measures of neurocognition over time, thus supporting the study’s first hypothesis. In addition, time-by-group effect on verbal learning and delayed recall appeared to be strongest, as evidenced by larger partial eta-squared figures (ηp2) on the RAVLT Total and RAVLT Delayed Recall scores.
Effects on physical fitness
At post-intervention, participants from the PE group achieved a higher average VO2 max score of 26.17 ml/min as compared to 16.71 ml/min achieved by the CR group, which was significant as evaluated using the Independent Samples t-test: t(68) = −2.53, p < 0.05. There was also significantly greater improvement in Rockport Walking Test VO2 max scores for the PE group than for the CR group: t(68) = −4.78, p < 0.001. These results suggested that, as hypothesised, the PE intervention led to better physical fitness among the participants.
The Mann–Whitney U test was used to test for differences in cognitive and physical fitness performance between participants on typical and atypical antipsychotics and results showed no significant differences.
Effects of CR on skills attainment
Figures 2A and 2B show the median baseline, and final scores on WBI and ILS between the two groups of participants. As seen from the graph, participants from CR achieved more improvement in their WBI scores and this was found to be significant upon analysis using the Independent Samples Mann–Whitney U test: U = 20.50, Z = −3.27, p = 0.001. They also had a significantly higher final median score at the end of the intervention: U = 34.50, Z = −2.56, p = 0.011. This suggested that participants who underwent CR achieved significantly greater improvement and better vocational skills at the end of the intervention than those who underwent PE.
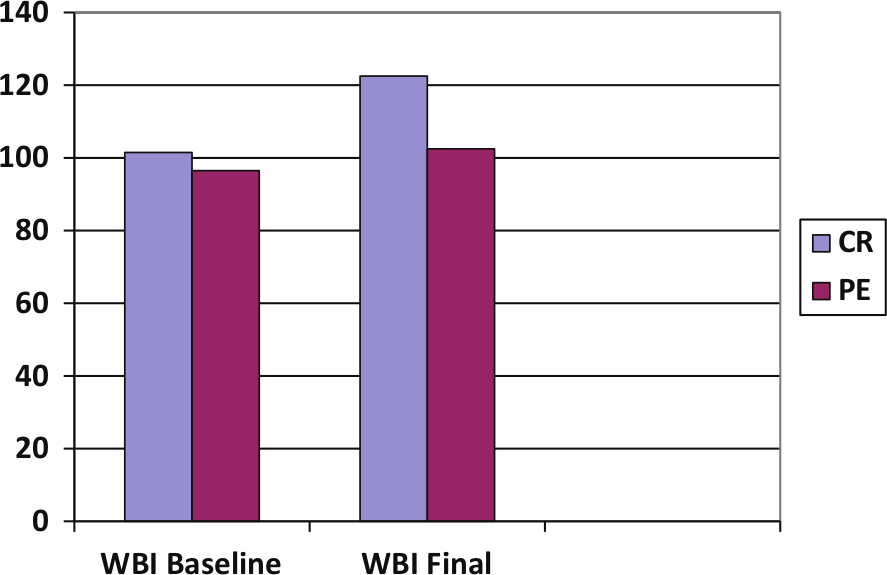
Comparison of Work Behaviour Inventory (WBI) scores (cognitive remediation (CR) and physical exercise (PE)).
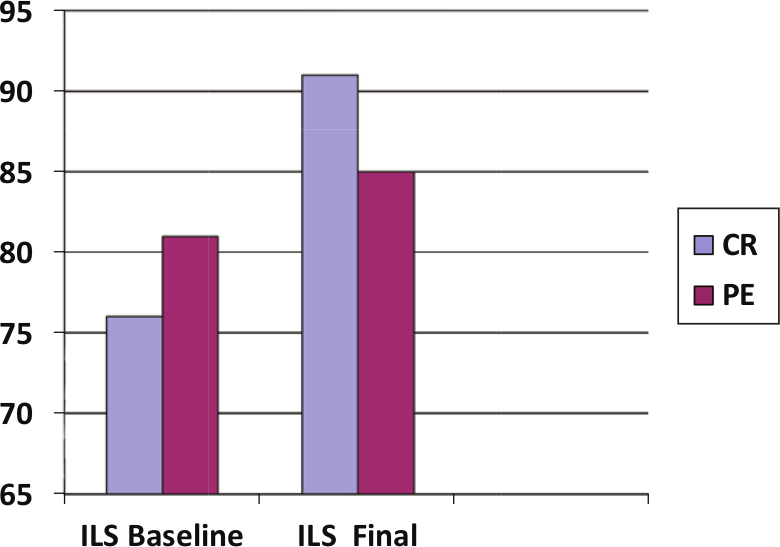
Comparison of Independent Living Scales (ILS) full-scale standard scores (cognitive remediation (CR) and physical exercise (PE)).
Although participants from the PE group had a higher baseline ILS Full Scale Standard score, their final score was lower than that of the CR group. Such a difference in the final ILS score was not found to be significant upon analysis using the Mann–Whitney U test: U = 78.50, Z = −0.88, p = 0.381. Nevertheless, the amount of improvement in ILS Full Scale Standard score among the CR participants was found to be significantly greater than that of the PE participants: U = 28.00, Z = −3.21, p = 0.001.
Effects of CR on functional outcomes
Employment outcomes
Among the CR participants, the median employment hours over the 12 months following intervention were 1225, while the PE participants achieved median employment hours of 520. The Mann–Whitney U test showed a significant difference in distribution of employment hours between the two groups: U = 6.50, Z = −3.29, p = 0.001. Participants from the CR group also earned a median salary of S$4225.50 over the year, which was significantly greater than that of the PE participants who earned S$1561.50: U = 6.00, Z = −3.33, p = 0.001.
Community ability outcomes
Figure 3 shows the mean MCAS scores of the two groups over the four time points. At baseline, the CR participants presented with significantly lower MCAS scores as evaluated by the Mann–Whitney U test: U = 207.50, p = 0.03. However, they demonstrated sizeable improvement after intervention, and further improvement in community ability was noted over the 1-year follow-up. On the other hand, the performance of PE participants on MCAS was fairly uniform from post-intervention onwards. Repeated Measures ANOVA showed significant time-by-group interaction effects, suggesting that the CR group demonstrated greater improvement in community ability than the PE group over the course of the study: F(1.59, 50.67) = 26.74, p = 0.000.
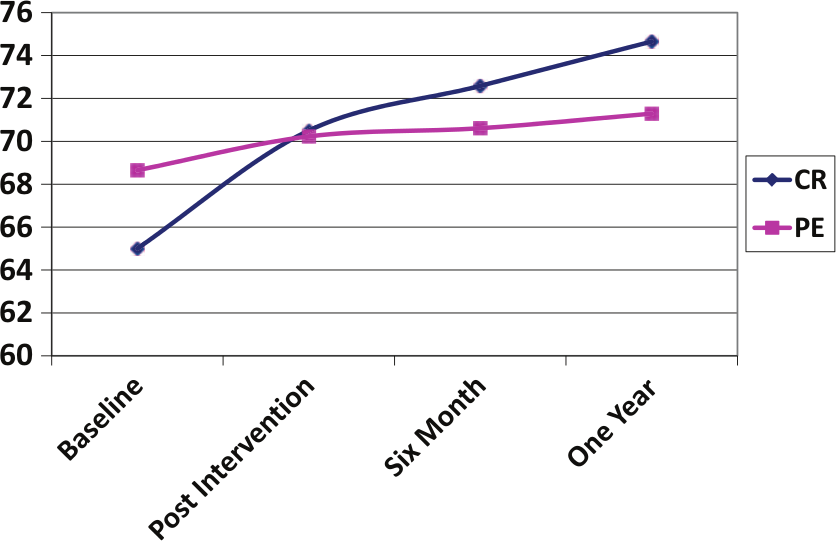
Mean MCAS scores between cognitive remediation (CR) and physical exercise (PE) groups.
Since the CR group achieved significantly better functional outcomes than the PE group, the second experimental hypothesis was supported.
Changes in symptomatology and quality of life
Repeated Measures ANOVA was also carried out for PANNS Total, PANNS Negative Subscale and WHOQOL-Brief scores at the three time points of baseline, 6-month follow-up and 1-year follow-up. Results showed significant time effects for all the measures, F(2, 130) = 3.809–36.209, p < 0.05, suggesting that the sample population experienced significant improvement in their symptoms and quality of life over the course of the research study. There were also significant time-by-group interaction effects favouring the CR group for PANSS Total, F(2, 130) = 4.683, p < 0.05, and PANSS Negative subscale scores, F(2, 130) = 4.227, p < 0.05, indicating that the CR group had significantly better symptom recovery than the PE group over the year. However, there were no significant time-by-group interaction effects for WHOQOL-Brief, suggesting that the CR group did not have more improvement in quality of life.
Discussion
This study investigated the impact of CR on both neurocognition and vocational/community functioning of a sample of participants with a diagnosis of schizophrenia. The CR programme consisted of therapeutic approaches that were believed to be effective in improving neurocognition and in translating to better functional performance. When compared against a credible alternative intervention with allegiance and placebo effects managed, CR produced differential improvement or maintenance on all the neurocognitive measures over the course of 12 months. The PE group obtained gains in physical fitness which were not achieved in the CR group. However, the functional gains evident in the CR group were not present in the PE group, suggesting that enhanced cognitive functioning was the main reason behind the improvement in vocational and community functioning.
The CR intervention in this study utilised both rehearsal and strategy approaches. Although meta-analyses suggested that the strategy approach was usually more effective (Wykes et al., 2011), the design of this study did not enable investigation of the effects of specific therapeutic components that led to cognitive and functional improvements. The rationale for the intervention was that rehearsal was needed to build competency of cognitive skills, while strategies were taught to aid in the execution of vocational or community living tasks. However, it was noticed that improvement was less marked during the follow-up phase, even though participants were continually reminded of the strategies. This might be due to either ceiling effects reached during the intensive computer-assisted phase, or it might be that any further gains would require more prolonged intensive remediation. It was unclear as to the optimal dose of CR needed, as very few studies had investigated dose effects. One study which compared neurocognitive gains for participants receiving 50 hours versus 100 hours of computer-based training showed that verbal learning and memory were amenable to change after 50 hours of training, while processing speed and global cognition were only significantly improved upon 100 hours of training (Fisher et al., 2010). However, the findings of the study reported here showed that improvement in CTMT scores was possible through a shorter duration of treatment.
Participants from the CR group achieved greater improvements in skills attainment and this was subsequently reflected by differences in functional outcomes between the two groups at the end of the 1-year follow-up. The CR group achieved greater employment hours and higher salaries than the PE group. Two meta-analyses of 26 and 39 studies, respectively, had showed that CR, when provided in the context of a psychiatric rehabilitation programme, could create significant positive impact on functioning (McGurk et al., 2007; Wykes et al., 2011). In the study reported here, CR was offered as an adjunct to vocational training or day rehabilitation. The goals of the rehabilitation programmes were thus clearly defined as open employment or improvement in community ability. Such clearly defined functional goals could have led to more targeted bridging and implementation of cognitive strategies amongst staff and participants.
The CR group displayed significantly more improvement in overall symptoms and negative symptoms throughout the duration of the study. Since negative symptoms and neurocognition were shown to be intricately linked (Ventura et al., 2009), improvement in cognitive function amongst the CR participants would have consequently reduced their intensity of negative symptoms. For example, when one is able to pay attention and remember things better, one is more likely to feel satisfied in activity engagement, thereby increasing one’s motivation to assume vocational or community living roles. However, perceived quality of life amongst the CR participants was not significantly better than the PE group. It might take beyond the 1-year follow-up period before the CR participants could experience the effects of better cognitive and functional performance on their quality of life.
A number of limitations in this research study should be noted. Although double blinding measures as well as steps to minimise allegiance effects were in place, the relative larger number of studies on CR compared to PE could have caused therapists to presume that CR was the more effective treatment. In addition, the attrition rate of 29%, though within the range found in a recent meta-analysis (Wykes et al., 2011), was substantial. This resulted in a much smaller sample size of fewer than 30 in each arm who had the full data. It would be difficult to extend the duration of recruitment as data collection already took 3 years. The Expectation-Maximisation method of imputing missing data, while efficient, might not be as ideal as the Multiple Imputation method, which might offer a closer approximation to the missing values due to dropouts during treatment. Most participants who dropped out cited loss of interest in continuing with the rehabilitation programme. The requirement to attend almost daily for both the rehabilitation and CR/PE interventions was a major challenge for these participants, as many of them presented with avolition and other negative symptoms. This may have implications for the implementation of CR in routine clinical practice. There is evidence that, while higher regularity of treatment leads to greater gains in neurocognition (Medalia and Richardson, 2005), a relatively small number of treatment sessions may be sufficient to produce some positive neurocognitive changes (McGurk et al., 2007). Flexibility in the intensity and duration of treatment may be useful in improving treatment adherence and still yield worthwhile outcomes.
Although CR was shown to produce beneficial effects on functional outcomes, the exact mechanism behind this was difficult to determine. The small sample size was insufficient to investigate the extent to which each neurocognitive domain singularly or compositely affected skills attainment and functional outcomes. In addition, a small sample had also resulted in unequal distribution of potentially confounding variables such as diagnosis and medication. The three participants diagnosed with schizoaffective disorder were randomised to the PE group. Given the small number of people with schizoaffective disorder in this study and the very clear pattern of results, it was unlikely that this was a serious confound. With respect to medication, a higher proportion of CR participants were taking atypical antipsychotics than the PE group. Again, there was no evidence in this study of interaction between medication type and neurocognitive changes or functional outcomes. However, a larger sample size of participants on typical antipsychotics could possibly eliminate any Type II error.
This research study used an active treatment as a comparison group but no treatment-as-usual group. Owing to difficulties in recruiting and retaining an adequate number of participants, a third control arm was not included. Having another control arm might allow for accurate evaluation of the neurocognitive gains of CR versus vocational training or day rehabilitation alone.
Lastly, it will be useful to extend the follow-up period beyond 1 year, since schizophrenia follows an enduring course with periods of relapses. If CR can be shown to have longer sustainable effects on function, it may dramatically enhance the recovery process of schizophrenia.
In conclusion, CR produced significant differential improvement in neurocognition, which was maintained for at least 1 year when compared with a credible alternative intervention. Moreover, the CR group achieved better employment and community ability outcomes, as well as more improvement in symptoms, compared with the PE group. The findings provided support for the use of CR in the psychiatric rehabilitation of people with a diagnosis of schizophrenia within the Asian population.
Footnotes
Acknowledgements
We thank all psychiatrists and occupational therapy staff who were involved in the diagnosis and recruitment of research participants, as well as in the implementation of the interventions.
Funding
This research was partially funded by a grant of S$10,000 from the Institute of Mental Health Research Department. Study number: 175/2006.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.