
Abstract
Objective:
Self-harm is common in adolescence, but most young people who self-harm do not seek professional help. The aim of this literature review was to determine (a) the sources of support adolescents who self-harm access if they seek help, and (b) the barriers and facilitators to help-seeking for adolescents who self-harm.
Method:
Using a pre-defined search strategy we searched databases for terms related to self-harm, adolescents and help-seeking. Studies were included in the review if participants were aged 11–19 years.
Results:
Twenty articles met criteria for inclusion. Between a third and one half of adolescents who self-harm do not seek help for this behaviour. Of those who seek help, results showed adolescents primarily turned to friends and family for support. The Internet may be more commonly used as a tool for self-disclosure rather than asking for help. Barriers to help-seeking included fear of negative reactions from others including stigmatisation, fear of confidentiality being breached and fear of being seen as ‘attention-seeking’. Few facilitators of help-seeking were identified.
Conclusions:
Of the small proportion of adolescents who seek help for their self-harm, informal sources are the most likely support systems accessed. Interpersonal barriers and a lack of knowledge about where to go for help may impede help-seeking. Future research should address the lack of knowledge regarding the facilitators of help-seeking behaviour in order to improve the ability of services to engage with this vulnerable group of young people.
Introduction
Self-harm is an act in which an individual deliberately initiates behaviour (such as self-cutting or ingesting a toxic substance or object), with the intention of causing harm to themselves with a non-fatal outcome (Madge et al., 2008). It is prevalent among adolescents with the peak incidence of self-harm coinciding with the onset of puberty (Hawton et al., 2012; Moran et al., 2012; Morey et al., 2008; O’Connor et al., 2009). There are few good comparative studies that exist, and it is unclear whether rates of self-harm are stable or have increased over recent years (Hawton et al., 2003; Muehlenkamp et al., 2012). Over half of adolescents who have self-harmed report engaging in more than one episode in their lifetime (Madge et al., 2008), showing the repetitious nature of this behaviour. Moreover, a previous history of self-harm is a key risk factor for suicide (Owens et al., 2002) and so self-harm has become a growing public health concern (Cooper et al., 2005; Hawton et al., 1997; Whitlock and Knox, 2007).
There are few definitions of ‘help-seeking’ agreed upon, although the World Health Organization has proposed that it is:
Any action or activity carried out by an adolescent who perceives herself/himself as needing personal, psychological, affective assistance or health or social services, with the purpose of meeting this need in a positive way. This includes seeking help from formal services – for example, clinic services, counsellors, psychologists, medical staff, traditional healers, religious leaders or youth programmes – as well as informal sources, which includes peer groups and friends, family members or kinship groups and/or other adults in the community. (Barker, 2007: 2)
Three sub-categories of help-seeking have been identified: help-seeking for specific health needs, help-seeking for normative developmental needs and help-seeking for personal stress or problems (Barker, 2007). Help-seeking for self-harm would fall into the latter category.
Early interventions and prevention programs may reduce the number of serious physical injuries resulting from self-harm and lower the risk of future suicide in young people (Aseltine et al., 2007). However, in order to engage young people in such programs, we need to better understand the barriers that impede help-seeking behaviour. For this reason, researchers have recently started to examine help-seeking behaviour in adolescents who self-harm. To our knowledge, only one review of this literature has been published and that review included adult participants and studies predominantly related to suicidal ideation. With this in mind, we set out to conduct a systematic review to focus on help-seeking related to self-harming behaviours in adolescents. We addressed two questions:
Review question 1 (Sources): ‘For those who do seek help, what sources of support do they use before or after an episode of self-harm?’
Review question 2 (Influences): ‘What are the barriers and facilitators to formal and informal help-seeking in adolescents who self-harm?’
The majority of young people who self-harm do so for a variety of reasons that do not always relate to suicidal intent (Scoliers et al., 2009). Therefore, in this review, when referring to ‘self-harm’, we are referring to the broad definition used in the UK and Europe which includes both non-suicidal self-injury (NSSI) and suicide attempts (Kapur et al., 2013).
The Internet may act as a resource for information and communication on sensitive topics such as self-harm (Suzuki and Calzo, 2004). Indeed, the influence of the Internet on self-harm in adolescents is increasingly attracting attention (Daine et al., 2013). Online discussion forums, videos and social media are widely accessed by young people predominantly for social reasons (Gross et al., 2002). Adolescents may also prefer to discuss their self-harm on the Internet because it can provide them with a sense of anonymity, acceptance, validation and support at a ‘safe’ distance (McKenna et al., 2002). In light of some high-profile cases of teenage suicide, concern has also been expressed about use of the Internet by young self-harmers, as it may maintain or normalise their behaviour (Lewis et al., 2012). Nevertheless, given its increasing use as a form of help-seeking by adolescents, we felt it was important to incorporate studies that had looked at Internet use into our review.
Methods
Search strategy
We searched MEDLINE, EMBASE, PsycINFO, PubMed, Cochrane Collaboration and Google Scholar using the following search terms: ‘self-harm or self-injury or self-mutilation or non-suicidal self-injury or suicide or deliberate self-harm or DSH or suicidal behavio$ or NSSI or non-fatal deliberate self-harm or self-poisoning or self-injurious behavio$ or parasuicide’ and ‘helpseek$ or seek$ help or seek$ treatment or help seeking behave$ or disclosure’ and ‘young people or teenager$ or youth$ or adolscen$ or young adult$ or children’. Additionally, the reference lists of all included articles were scanned for potentially relevant articles.
Inclusion/exclusion criteria
Studies were included if they examined help-seeking behaviour in adolescents that self-harm. Behavioural intent (i.e. planned help-seeking) and behaviour (actual help-seeking) were both included. To maximise the sensitivity of detection of relevant literature, no limits were placed on study design. Articles were limited to those published in English, and in indexed journals. Duplicate records that appeared in more than one database (e.g. both MEDLINE and EMBASE) were excluded.
Studies were excluded if all participants were under the age of 11 years or over the age of 19 years or if they primarily focused on suicide rather than self-harm.
Data extraction and validity assessment
Titles and abstracts were checked by one reviewer (SR) against the eligibility criteria, and the full text of articles meeting the criteria were obtained and reviewed. Reasons for exclusion were recorded, and data from included articles were also extracted by RF. All screened articles were cross-checked and any disagreements were resolved by a discussion with a third reviewer (PM). The PRISMA checklist was used to ensure transparent reporting of the systematic review.
Synthesis
Owing to the diverse nature of the literature included in this review, we were unable to conduct a formal meta-analysis but instead used a narrative synthesis approach in order to summarise the findings. Quantitative data are presented as reported (e.g. proportions), and themes identified from qualitative data are summarised.
Results
Search results
After excluding duplicate articles, 579 articles were considered, of which 20 articles were included in the narrative synthesis (Figure 1).
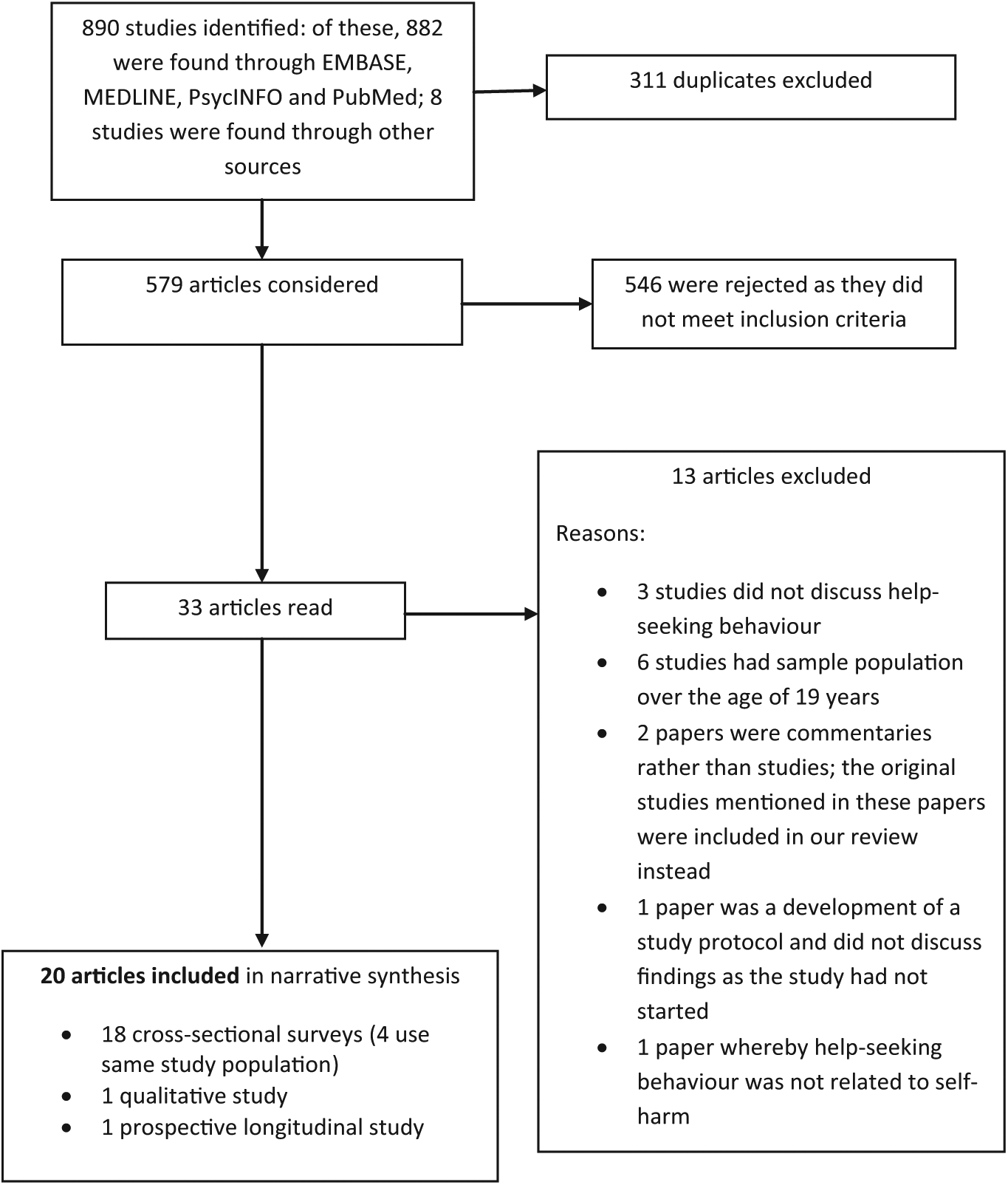
Flow diagram of identified articles.
Study characteristics
Identified articles consisted of one qualitative study (Klineberg et al., 2013), one prospective longitudinal study (Stallard et al., 2013) and 18 cross-sectional studies (Baetens et al., 2011; Berger et al., 2013; De Leo and Heller, 2004; Evans et al., 2005; Fortune et al., 2008a, 2008b; Hawton et al., 2009; Heath et al., 2010; Morey et al., 2008; Muehlenkamp et al., 2010; Rossow and Wichstrom, 2010; Watanabe et al., 2012; Ystgaard et al., 2009). Of these, four articles reported data from the same study (Evans et al., 2005; Fortune et al., 2008a, 2008b; Hawton et al., 2009).
The studies derived from the United Kingdom, United States, Canada, Europe, Australia and Japan and the majority were conducted within a school setting. The study characteristics, along with their main findings, are shown in Table 1.
Summary of help-seeking sources and influences.

Papers derived from the same study population.
The lifetime prevalence of self-harm ranged from 9% to 26% (De Leo and Heller, 2004; Fortune et al., 2008a, 2008b; Morey et al., 2008; Muehlenkamp et al., 2010) and past year prevalence ranged from 3% to 8% (De Leo and Heller, 2004; Evans et al., 2005; Hawton et al., 2009; Watanabe et al., 2012). Females were more likely to report self-harm than males (Evans et al., 2005; Morey et al., 2008; Ystgaard et al., 2009).
Review question 1 (Sources of support)
Thirteen of the 20 articles reported the prevalence of any help-seeking behaviour related to self-harm, of which four distinguished between help-seeking before or after an episode of self-harm (De Leo and Heller, 2004; Evans et al., 2005; Fortune et al., 2008b; Morey et al., 2008). Between a third and one half of adolescents did not seek help for their self-harm. Similar rates of help-seeking were found before or after an episode of self-harm, although adolescents were more likely to contact health services after harming themselves (Morey et al., 2008).
Sources of help were most commonly informal sources, such as friends and family (De Leo and Heller, 2004; Fortune et al., 2008b; Watanabe et al., 2012). Formal sources approached in smaller numbers were psychologists or psychiatrists, school nurses, teachers, social workers and general practitioners. Fewer than 13% of those self-harming presented for hospital treatment (De Leo et al., 2004; Hawton et al., 2009). Rates of contact with child and adolescent psychiatric services were increased in adolescents that reported both NSSI and suicide attempts compared to adolescents that did not self-harm and adolescents who reported either suicide attempts or NSSI (Tørmoen et al., 2014). Telephone helplines and ‘other’ were also mentioned as sources of help in the studies reviewed; however, no descriptions or examples were given for the ‘other’ sources. A study of Internet use showed that comments related to videos of NSSI on YouTube were most frequently used as a forum for self-disclosure (38%) rather than asking for help (<3%) or offering help (<3%) (Lewis et al., 2012). Participants using an online discussion forum said that found it easier to use online methods of support rather than face-to-face because they valued the anonymity, were more open about their self-harm and felt less judged (Jones et al., 2011).
Review question 2 (Influences)
Several correlates of help-seeking emerged in the literature. These were: sex, age, frequency and method of self-harm and suicidal intent. Three of the studies reported that females were more likely to receive help after an episode of self-harm than males, a factor not explained by sampling strategy (Evans et al., 2005; Rossow and Wichstrom, 2010; Ystgaard et al., 2009). However, no sex differences were found among participants who sought help before an episode of self-harm in the study by De Leo and Heller (2004). The type of help received was also affected by sex, with females more likely to receive informal help from friends and family (Rossow and Wichstrom, 2010) and males more likely to present to hospital (Ystgaard et al., 2009). The only study to address age in this review reported that younger students were more willing to access school-based support than older students (Heath et al., 2010). Few studies commented on the role of mental health problems on help-seeking behaviour; of those that did, there were mixed findings. Tørmoen and colleagues (2014) found that symptoms of depression, eating problems and the use of illicit drugs were associated with an increased use of child and adolescent psychiatric services; however, other studies found that symptoms of depression and anxiety did not significantly affect young people’s help-seeking for self-harm (Hawton et al., 2009; Ystgaard et al., 2009).
The method of self-harm (e.g. overdose) and previous attempts to seek help were the only variables that differentiated between adolescents who presented to hospital after self-harm compared to those that did not go to hospital (Hawton et al., 2008). Of the four studies in this review that looked at NSSI (Baetens et al., 2011; Berger et al., 2013; Heath et al., 2010; Muehlenkamp et al., 2010), only one study made comparisons of help-seeking status between NSSI and suicidal self-injury (SSI) groups (Baetens et al., 2011). This study reported that adolescents in the SSI group were more likely to disclose their self-harm and to have received psychological and medical help than those in the NSSI groups (Baetens et al., 2011).
Barriers to help-seeking
Nine of the 20 articles identified barriers to help-seeking (Figure 2). Barriers fell into two main thematic categories: interpersonal and intrapsychic.
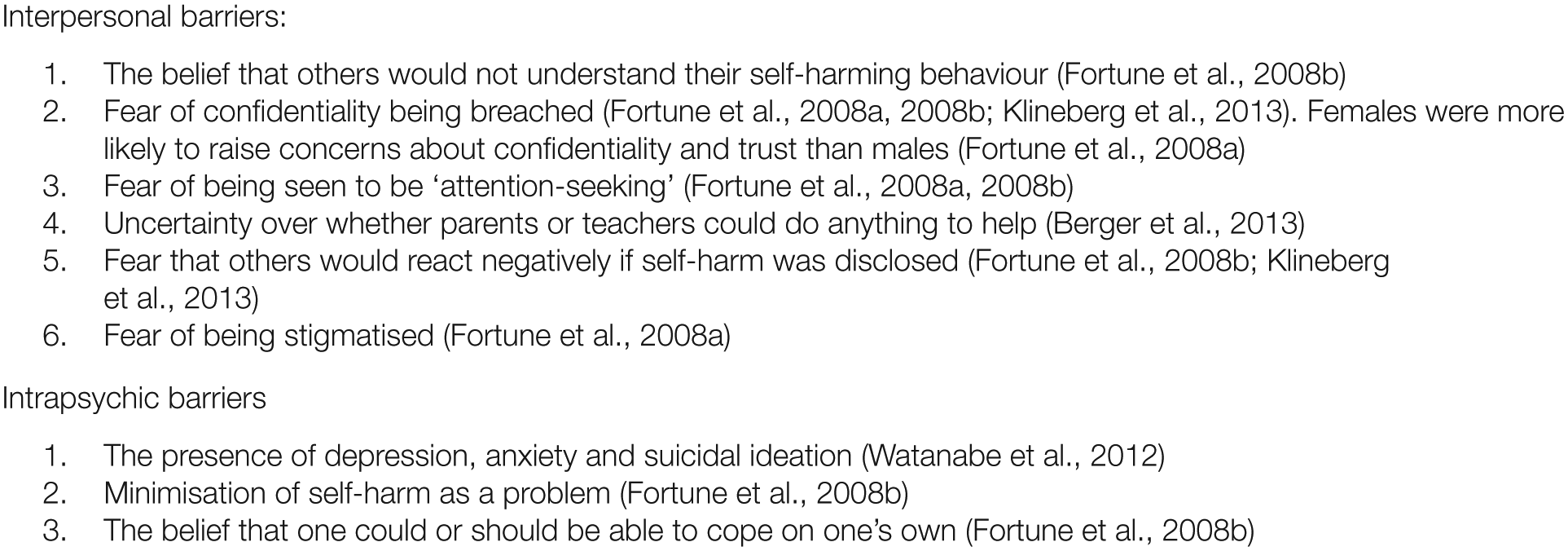
Barriers to help-seeking.
Once the decision was made to seek help, other barriers could impede the process of actually getting help. In the only published qualitative study that was identified, the adolescent participants revealed that many of them simply did not know where to turn for help or what to expect from the help they might receive (Klineberg et al., 2013). Geographical factors determined help-utilisation in another study, with adolescents living in suburban and rural areas being less likely to use services compared to their counterparts living in urban areas (Fadum et al., 2013). Adolescents who turn to the Internet for help with their self-harm may be actively discouraged from seeking treatment by other online users (Lewis et al., 2012).
Facilitators to help-seeking
Two studies identified facilitators to help-seeking behaviour (Berger et al., 2013; Klineberg et al., 2013). In Klineberg and colleague’s qualitative study, adolescents suggested the following as factors which might encourage help-seeking behaviour related to self-harm: assurances of confidentiality, being treated respectfully, having a trustworthy person to talk to and the option of talking to someone of a similar age and background. Facilitators suggested by Berger and colleagues were: parents and teachers helping young people to resolve their problems, parents and teachers referring the young person to formal sources such as psychologists and psychiatrists, reducing stigma, improving the family context (e.g. reducing conflict, increasing activities, creating a closer bond), and reducing academic stress (Berger et al., 2013).
Discussion
Facilitating help-seeking behaviour in young people who self-harm may reduce their distress and increase the likelihood of them accessing effective treatment for underlying emotional difficulties (Wilson and Deane, 2001). Approximately half of adolescent participants in the studies included in this review did not seek help for their self-harming behaviour. This was particularly true of clinical services, which were accessed minimally by adolescents who self-harm, supporting the premise that self-harm goes largely unnoticed by mental health services (Hawton et al., 1996).
A recent review of the literature on help-seeking behaviour among young people for suicidal thoughts and self-harm concluded that the phenomenon of help-seeking amongst self-harmers was not sufficiently different between those with and without suicidal ideation (Michelmore and Hindley, 2012). However, our review identified too few studies to enable us to reach a definitive conclusion about this issue The Internet may exert both positive and negative influences on help-seeking in adolescents that self-harm. Self-disclosure and informal support were the most common themes identified on message boards and discussion forums associated with self-harm (Jones et al., 2011; Lewis et al., 2012). Clearly the Internet may encourage disclosure of self-harm in adolescents because it provides anonymity and a forum where young people may feel less likely to be judged by others (Jones et al., 2011; Whitlock et al., 2006). However, use of the Internet also has unpredictable, dangerous side effects. Recovery-oriented content is sparse and responses to messages may be hostile or help to maintain self-harming behaviour (by sharing personal experiences) (Lewis et al., 2012; Whitlock et al., 2006). Furthermore, the Internet may act as a substitute for offline skills and hinder healthy social development (Daine et al., 2013; Whitlock et al., 2006, 2007). The majority of the barriers to help-seeking were interpersonal (relating to relationships and communications with others) rather than intrapsychic (internal psychological processes of the individual). The strongest finding relating to interpersonal barriers was the beliefs and fears that adolescents had about the possible negative consequences of disclosing their self-harm status. It is also worth noting that one study shed important light on the fact that adolescents may be prevented from seeking help because they simply may not know where or who to turn to for support (Klineberg et al., 2013). Adolescents who did seek help primarily turned to friends and family (De Leo and Heller, 2004; Fortune et al., 2008b; Morey et al., 2008).
We identified a paucity of research into the facilitators of help-seeking behaviour among young people who self-harm and this finding is consistent with a general lack of research into facilitators of help-seeking behaviour among young people (Gulliver et al., 2010). More broadly, facilitators of help-seeking in young people include positive past experiences, emotional competence (the ability to identify and describe emotions), and mental health literacy (recognising symptoms/knowledge of their own symptoms) (Gulliver et al., 2010; Rickwood et al., 2005). Whether these same facilitators apply to young people who self-harm, who may have specific psychological deficits, (McAuliffe et al., 2006) is less clear.
Interventions promoting help-seeking
To date, no intervention has been shown to increase help-seeking behaviour in young people who self-harm. For example, a school-based program aimed at preventing NSSI in adolescents, found that the program improved help-seeking attitudes and intentions amongst students but this did not translate into any significant changes in help-seeking behaviour (Muehlenkamp et al., 2010). Similarly, a randomised controlled trial using an intervention that consisted of sending regular postcards to young people who presented to a service following suicide-related behaviour was well received, yet failed to have any significant effect on self-harm or help-seeking behaviour (Robinson et al., 2012). Interventions that show an increase in treatment adherence do exist. A randomised controlled trial using an enhanced emergency department intervention to improve follow-up rates in suicidal youths was effective in increasing rates of outpatient treatment and psychotherapy (Asarnow et al., 2011). In another study, treatment engagement was higher in adolescents who received therapeutic assessment compared to usual assessments; however, the frequency of hospital presentations for self-harm was not affected by the intervention (Ougrin et al., 2013).
Our review suggests that adolescents are more likely to go to informal sources when asking for help. Rickwood and colleagues suggest that young people turn to friends and family first and foremost because they are trusted and secure relationships. Therefore, interventions may be more effectively targeted at friends and family members who might then be able to influence formal help-seeking in a young person (Rickwood et al., 2005). Clearly, this will be inappropriate in situations where family and friends are contributing to an adolescent’s self-harming behaviour (Hawton et al., 2012). Interventions that focus on improving mental health literacy have been shown to reduce stigma, improve knowledge and attitudes about mental health issues and increase help-seeking behaviours (Kelly et al., 2007) and so this may be another avenue to investigate. Exploring the ways of harnessing social media (i.e. the Internet) to enhance knowledge of young people who self-harm is the subject of an on-going investigation by our research group.
Limitations and methodological factors
Our review needs to be considered in the light of certain limitations. We used a broad definition of self-harm which encompassed behaviours with and without suicidal intention. There has been some suggestion that non-suicidal self-harm and suicidal behaviour may be aetiologically and functionally distinct from one another and, increasingly, researchers in the field are emphasising the need to disentangle these constructs (Butler and Malone, 2013; Wichstrom, 2009). We used a broad definition because there is a substantial overlap between suicidal and non-suicidal self-harm (Kapur et al., 2013), and behavioural intention with respect to suicide is changeable (Salter and Platt, 1990). Furthermore, there is some question over the validity and usefulness of categorising this phenomenon (Kapur et al., 2013). Given the paucity of articles in this area, it is unfeasible to separate these two concepts within the scope of this review.
The number of papers included in this review is relatively small and heterogeneous; for example, the samples in the studies ranged from 30 to 30,532. The search strategy used may not have captured all relevant articles, and restricting articles to English language limits the generalisability of our findings.
Methodological issues across the papers should also be taken into account. Definitions of self-harm differed somewhat across the studies, which may impact the responses provided by participants and subsequently the samples identified as ‘self-harmers’. Furthermore, a consequence of merging non-suicidal self-harm and suicidal behaviour into a single category of self-harm overlooks potentially important confounding issues such as method of self-harm, medical severity, visibility and associated morbidity – all of which will potentially influence whether or not a young person goes on to seek help. For example, non-suicidal self-harm resulting in minor skin damage (as a result of scratching the skin) is unlikely to require medical attention, whereas an overdose is more likely to result in service utilisation. Measures of help-seeking also differed across studies, from questions asking ‘Are you currently consulting anyone to discuss your psychological stress or problems?’ (Watanabe et al., 2012) to a nine-item list of helping sources accessed after an episode of self-harm (Ystgaard et al., 2009). The absence of a consensus definition of help-seeking is also unhelpful in this regard. It is unclear where adolescents engaged with services were internally motivated or were doing so at the direction of an adult. Information on help-seeking behaviours was based on self-report across studies, which may lead to potential bias in the recording of help-seeking behaviour. Selection bias was noted in several of the school-based studies. Those that were truant on the day of the survey may be at greater risk of self-harm; this may also lead to an underestimate of prevalence rates in adolescents that self-harm (De Leo and Heller, 2004; Evans et al., 2005; Watanabe et al., 2012).
Although we identified a range of sources of support, no study has examined the relative effectiveness of these sources. Finally, help-seeking behaviour is a complex construct; the phenomenon and motivating factors behind help-seeking prior to an act of self-harm are likely to differ from those driving help-seeking after an act of self-harm. Yet, only four of the 20 studies distinguished the chronology of help-seeking behaviour.
Conclusion
Four key findings emerged from this review. First, few adolescents seek help for self-harm and, of those who do, informal sources such as friends and family are the most likely support systems accessed. This has implications for public health campaigns and school personal and social education courses. Second, interpersonal barriers, including the fear of others’ reactions, disrupt the help-seeking process. Increasing mental health literacy may play an important part in encouraging adolescents to seek help when they are experiencing emotional difficulties. Moreover, fears relating to the stigma of self-harm might diminish as a result of anti-stigma campaigns. Third, basic lack of knowledge about where to go for help further impedes help-seeking. Young people are prolific users of the Internet and whilst they may be reluctant to seek help from health care professionals when distressed, many turn to the Internet as a way of coping with psychological distress (Baker and Fortune, 2008; Jones et al., 2011). Responsible and accessible web-based information about sources of support for those who self-harm could therefore be of benefit to large numbers of young people. Finally, our review identified a key knowledge gap relating to positive enablers of help-seeking. If the ability of services to engage with this vulnerable group of young people is to improve, then research on facilitators to help-seeking behaviour should be considered a high priority.
Footnotes
Funding
This review was funded by a grant from Guy’s & St Thomas’ Charity (MAJ120701). PM is part-funded by the NIHR Specialist Biomedical Research Centre for Mental Health at the South London and Maudsley NHS Foundation Trust and Kings College London. The views expressed in this paper are those of the authors and not necessarily those of Guys & St Thomas’ Charity, the NHS, NIHR or the Department of Health.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.