
Abstract
Introduction
Findings from the Australian National Survey of Mental Health and Wellbeing (NSMHWB) show that only a minority (approximately 30%) of children and adolescents experiencing serious mental health problems attended any treatment in the preceding 6 months (Sawyer et al., 2010). Data from the 2007 NSMHWB also reveals that less than 25% of young Australians aged 16–24 years with a mental disorder of 12-month duration accessed health-care services in the preceding 12 months (Reavley et al., 2010)
For the majority of young people, the decision to seek professional help relates to the level of psychologicaldistress experienced. Students with more symptoms of distress are more likely to seek out mental health professionals than rely on informal sources of support (Sawyer et al., 2007). However, being ‘considerably distressed’ is not sufficient reason for many young people to look for any help (Boldero and Fallon, 1995). There are a number of attitudinal and practical barriers that prevent young people from seeking help and there is a need to better understand these factors to facilitate help seeking. One such source is the influence of other people to help convince the young person that help is warranted. The present study examines the relative influence of parents and others in facilitating the help seeking of young people.
Traditional adult-based models of health care use emphasize the reasoned decision-making of the individual rather than barriers to services or other environmental influences. For example, there are models that focus on the cognitive cues that determine an individual’s decision to seek help (Fisher et al., 1983). The theory of reasoned action (Ajzen and Fishbein, 1980) incorporates a person’s evaluation of the opinion of others towards help seeking into the decision-making process but it is not considered to be the primary determinant of the person’s help seeking behaviour. Sociobehavioural (Andersen, 1995; Mukolo et al., 2010) and sociocognitive model, such as the health belief model (Henshaw and Freedman-Doan, 2009), emphasize that help seeking occurs in a socioecological context. Dynamic models of health-care use recognize that help seeking is often a protracted social process involving the family, social networks and the community. Such models incorporate the social influences that may shape an individual’s decision to seek help (Logan and King, 2001; Pescosolido et al., 1998).
In a comprehensive Australian research programme into young people’s help seeking for mental health problems, Rickwood et al. (Rickwood et al., 2005; Rickwood et al., 2007) conceptualized the help-seeking process as one where the personal domain of psychological distress is translated into the interpersonal domain of seeking help. In this model, a young person must first become aware that they are experiencing mental health symptoms and then be able and willing to express their distress to others. It may be that the young person first articulates their distress to trusted friends and family who can then assist in finding appropriate help sources. The final stage of the process is the young person being able to reveal their distress to the help source (Rickwood et al., 2005; Rickwood et al., 2007).
The importance of external influences on decisions to seek formal help was demonstrated in a study of 70 adult males who had recently attended outpatient psychological services. Ninety-six per cent of respondents said they made their decision to seek help after some degree of influence by others (Cusack et al., 2004). The extent of the influence necessary for young people to access help has not yet been quantified. Conceivably, parents, relatives, friends, the school system and general practitioners play an important role in obtaining formal help for adolescents with psychological problems. Logan and King (2001) have proposed a model of a parent-mediated pathway to mental health services for young people. It incorporates the potential role of others in facilitating help for distressed young people but assumes that parents are most influential in the decision of adolescents to accept formal help. The model acknowledges that parental help seeking is not straightforward and that other factors (such as barriers) may affect a parent’s progress towards accessing services for their child. One such barrier is the parent’s perception of their child’s problem.
Many parents of children with mental health disorders do not perceive a problem (Teagle, 2002). Parental recognition of child psychological difficulties relates to the nature of the disorder, the severity of the child’s symptoms and impairment, and the consequent burden that parents experience (Angold et al., 1998; Logan and King, 2001; Teagle, 2002). The manifest symptoms of externalizing disorders are likely to be noticeable and have an impact on parents (Logan and King, 2001). In contrast, the internalized symptoms of disorders such as depression or anxiety may be more difficult for parents to recognize in their children and be less burdensome (Angold et al., 1998; Logan and King, 2002). Angold et al. (1998) found that parental burden associated with child symptoms and functional impairment predicted specialty mental health service use. However, there is no data on symptom perception and the relative influence of parents on young peoples’ help seeking.
The level of parental influence necessary to have a young person attend a clinical service is likely to be related to the extent to which parent and child agree about the nature and severity of the child’s problems. Arguably, young people who acknowledge difficulties will respond more readily to parent-initiated attempts to access help and require less coercion. To date, a common finding has been that parent and youth ratings of the social, emotional and behavioural problems in young people are discrepant (De Los Reyes and Kazdin, 2005). Indeed, there is often disagreement on whether problems even exist (Yeh and Weisz, 2001).
Parent–child agreement on problems in children is associated with problem type. There is evidence that teenagers are less likely than their parents to report externalizing behaviour (Youngstrom et al., 2000). Of concern are the findings that in comparison to externalizing behaviour, parents are poor at recognizing more internal emotional problems in their children (Sourander et al., 1999). Wu et al. (1999) interviewed 1285 parent–child (9–17 years) pairs in a community sample and found that externalizing problems were significantly related to children’s use of mental health services but depressive disorders were not. In the same study, parents reported a greater need for mental health services for young people with externalizing disorders than for those with depression. In contrast, the children saw a greater need for services for depression (Wu et al., 1999). These findings suggest that parent rather than child perceptions of the need for help, determine whether help is sought. If parents have a different view of their child’s symptoms this could potentially prove a barrier to the young person accessing professional help (Wu et al., 1999). The present study explores the relationships between parent and child perceptions of child problems and parent influence on help seeking.
Objectives
The objectives of the study were to examine the relative influence of parents and others on the decision of young people to seek formal help and to determine the relationship between the severity and types of adolescents’ psychological problems, and the degree of influence necessary to have young people access professional help.
It was hypothesized that:
Young people will endorse parents as the strongest source of influence on their decision to access clinical services;
When parents perceive the young person’s problems as more severe than the young person does, the greater the discrepancy between parent and child, the higher that parent and child will rate parental influence on help seeking;
When parents perceive the young person’s problems as less severe than the young person does, the greater the discrepancy between parent and child, the lower that parent and child will rate parental influence on help seeking;
Higher parental ratings of their child’s externalizing difficulties will be related to higher parent and child ratings of parental influence on help seeking.
Methods
Ethical considerations
The research design addressed a number of ethical considerations including the need to ensure that participation was voluntary and only undertaken after being informed of the nature of the study. Young people under the age of 14 years were excluded from the study because they were thought to be less likely to be able to give fully informed consent. It was also important for potential participants to understand that data for the study would be obtained not only from a specific research questionnaire but also from a standard assessment measure used routinely by the New South Wales State Child and Adolescent Mental Health Services (CAMHS). The parent and youth Strength and Difficulties Questionnaires (SDQs; Goodman, 1997; Goodman et al., 1998) are routinely sent to all CAMHS clients. In the same package, eligible clients of each CAMHS received parent and youth information sheets which detailed the auspice and nature of the study and stated that participation was voluntary. At the request of the Northern Sydney Area Health Service Human Research Ethics Committee (HREC), the anonymity of clients from the Sydney CAMHS was maintained. The information sheets posted to Sydney CAMHS clients informed clients that the study was anonymous but that consent to use the information supplied on the questionnaires was implied if the research questionnaire was completed. Parent and youth consent forms were sent to Illawarra CAMHS clients. Ethical approval for the research was received from the University of Wollongong HREC and the New South Wales Department of Health ethics committees responsible for overseeing clinical research in the two CAMHS involved in the study.
Participants
The sample comprised parent–child pairs that attended an initial clinical assessment interview with a CAMHS in Sydney or the CAMHS in the Illawarra region of New South Wales, Australia and agreed to participate in the research. CAMHS are part of State-wide public sector mental health services which do not require clients to pay fees. New clients to these services were eligible to participate if the young person was between 14 and 18 years of age. Consecutive, new and eligible client families of the Sydney and Illawarra CAMHS teams during the 6-month study period of December 2004–May 2005 were asked to participate in the research. In total, 244 parents and 256 young people were eligible to take part in the study. The sample of 119 parent–child pairings represents a study participation rate of 51.6% of parents and 53.7% of adolescents who were new clients presenting to the Sydney CAMHS in the research period. The overall participation rate across sites was 50% for parents and 51.2% for adolescents. Eight parents who attended for an interview chose to be involved in the study but their children declined to participate. Similarly, 10 adolescents whose parents did not participate volunteered for the study. As a result of these variations sample sizes for some descriptive statistics below vary from the 119 dyads.
An adult relative other than a parent accompanied seven participating young people and all agreed to participate in the research (for ease, these other relatives will be referred to as parents). It was considered unlikely that the accompanying adult would complete the questionnaire if not involved in the young person’s life and anecdotal reports indicated all had some awareness of the context and difficulties being experienced. The mean age of the 131 adolescent participants was 15.5 years (SD = 1.11). There were 47 (35.9%) who were male and 64.1% who were female. Of the 129 adult participants, the vast majority (n = 104; 80.6%) were mothers with the remaining being 25 fathers or other relatives. Sixty-two per cent of parents indicated that they had obtained mental health help for their child in the past. The CAMHS teams notified all newly referred clients of their initial appointment by mail. In the data collection period, the first interview was generally offered within 4–6 weeks of referral to the team. Along with the initial appointment letter, an information sheet explaining the study was provided for both parent and adolescent. Both parent and adolescent’s questionnaires were included in the package and if they agreed to participate in the research, they were asked to bring the completed measures to their first appointment.
Tools
The parent questionnaire was comprised of the Strength and Difficulties Questionnaire for parents (SDQ; Goodman, 1997) and the parental influence items. The youth questionnaire consisted of the self-report SDQ (Goodman et al., 1998) and three questions on sources of influence on the young person’s decision to attend the CAMHS assessment appointment. The SDQ (Goodman, 1997) is a brief behavioural screening questionnaire that assesses the adjustment and psychopathology of young people (11–17 years). There are near-identical parental and youth self-report versions of the SDQ (Goodman et al., 1998). The 25 core items of the parent SDQ provide scores on five scales, each comprising five items. The items depict specific behavioural, emotional or relationship-oriented attributes. The scales are Emotional Symptoms, Conduct Problems, Hyperactivity-Inattention, Peer Problems and Prosocial Behaviour. A Total Difficulties score is obtained by summing scores on the four scales of negative attributes and greater difficulties in psychological adjustment. Higher combined scores on the Conduct Problems and Hyperactivity-Inattention scales suggest externalizing problems (Goodman, 2001). Higher scores on the Emotional Symptoms scale indicate greater internalizing problems (Goodman, 2001). The internal reliability of the individual scales and Total Difficulties scale is satisfactory; concurrent validity has been established with other well-accepted child measures and both parent and youth self-report ratings on the SDQ have also discriminated between young people from community and clinic samples.
Help-seeking influences were assessed for young people using three items. Participants were asked to rate on a seven-point Likert-type scale, ‘How much do you think the decision to seek professional help was your own or influenced by others’ (1 = totally others’ decision, 4 = half my decision, half others’ decision, 7 = totally my decision), and on a five-point scale, ‘How much each of the specific people listed below influenced your decision to seek professional help on this occasion (0 = not at all; 2 = moderately; 4 = a great deal), and ‘If your decision to seek help was influenced by others, do you think you would have sought help without their influence?’ (yes or no).
Three equivalent questions on the parent questionnaire tapped the extent to which parents had been influenced to find help for their children by others. Parents were asked to rate on a seven-point Likert-type scale, ‘To what extent was your decision to seek mental health help for your child your own decision?’ (1 = totally others’ decision; 4 = half my decision, half others’ decision; 7 = totally my decision), ‘If someone else did influence your decision to seek professional mental help for your child’s problems who had the greatest influence on your decision (Please specify relationship)?’ and ‘To what extent did you influence your child’s attendance today for professional help?’ (1 = totally child’s decision; 4 = half my decision, half others’ decision; 7 = totally my decision).
Results
Data analysis was conducted using Predictive Analytics Software (PASW), version 17 (SPSS Inc., Chicago, IL) and initial screening indicated that a number of variables were not normally distributed. As a result, for most analyses, non-parametric tests were used. There were small amounts of missing data resulting in variations in samples sizes for some analyses and only valid percentages are reported. No significant differences were found between the responses of mothers (80.6% of the total adult sample), fathers and other relatives who had accompanied the young person. Consequently all adult responses were analysed together as parent responses.
Influences on youth help seeking
Ninety-four per cent (n =112) of youth respondents reported that others had influenced their decision to seek help. For 11 (9.2%) of these young people, the decision to seek help had been totally the decision of someone else, while only seven (5.9%) indicated that the decision to access help had been totally their own decision. Moreover, only two (1.7%) young people indicated that none of the nine specified sources had been influential in their decision to seek help.
Table 1 presents the mean source of influence scores and mean ranks obtained by the youth participants who completed all specified influence items. Only eight (6.5%) respondents indicated being influenced by sources of influence other than those specified (boyfriend/girlfriend, n = 5; counsellor/psychologist, n = 2; caregiver, n = 1). Since very few endorsed this item, it was not subjected to any further analyses.
Mean source of influence, standard deviation scores, mean ranks and percentage of total youth sample who endorsed specified sources of influence (n = 121).
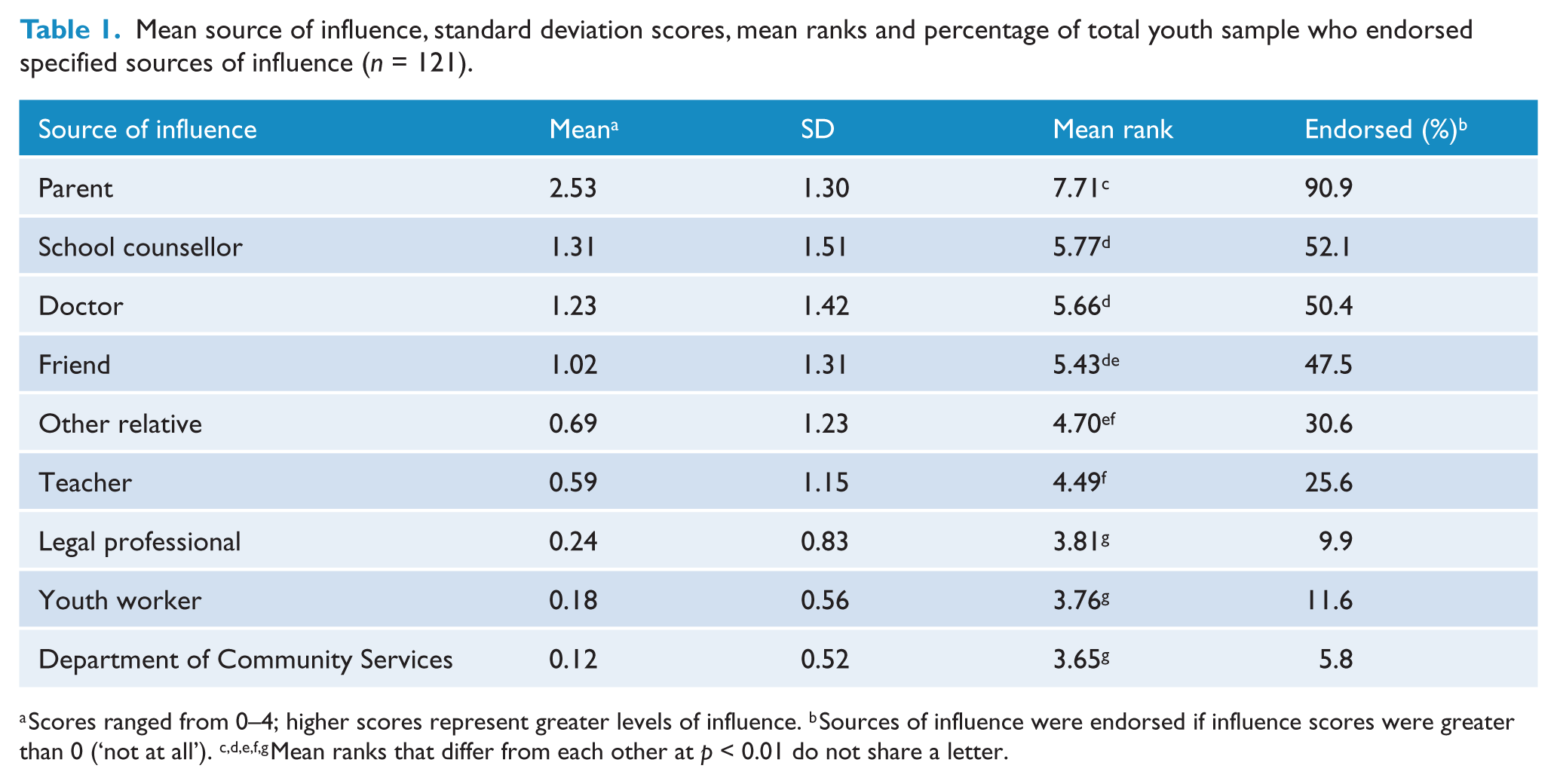
Scores ranged from 0–4; higher scores represent greater levels of influence. b Sources of influence were endorsed if influence scores were greater than 0 (‘not at all’). c,d,e,f,g Mean ranks that differ from each other at p < 0.01 do not share a letter.
A non-parametric Friedman’s test indicated that there were significant differences in the degree of influence of each influence source on the decision to seek help, χ2 (8, N =121) = 340.8, p < 0.001. Wilcoxon signed-rank tests were conducted to further explore differences between sources of influence (Table 1). Parents were significantly more influential in the decision of young people to seek help than any other influence source. Of the total youth sample, 87% (n = 105) reported that they had been influenced by more than one source to seek professional help and 36.3% indicated some degree of influence from four or more of the nine sources. On the item asking about whether help would have been sought without being influenced, 59% of the 106 young people who responded indicated that they would not have accessed help without the influence of others (Influenced group). The remaining 41% (n = 43) reported that they would have sought help independently of the influence of others (Independent group). Mann–Whitney U tests confirmed a significant difference between the Influenced and Independent groups on the extent to which young people reported that it was their own decision to seek help (Z = −4.57, p < 0.001). Notably, parents and their children were in agreement on how independent young people were in the decision to seek help. The parents of those adolescents in the Independent group rated their influence on the decision significantly lower than parents of adolescents in the Influenced group (Z = −2.63, p = 0.008).
Influences on parents seeking help for young people
The mean parental influence score was M = 4.35 (SD = 1.90). Only 12% (n = 14) of parents indicated that they had not influenced their child’s decision to access professional help to some degree while 20% (n = 23) reported that their child was not a part of the decision to seek help at all. Parent and child reports of parental influence had a significant positive relationship (r s = 0.20, p = 0.02). The mean level of influence by others reported by parents was M = 5.15 (SD = 1.78). Forty-four parents (36.7%) reported that it was their decision alone to seek help for their child while 76 parents (63.3%) indicated a degree of influence from others in deciding to access professional help. Only six (5%) parents said that the decision to seek mental health care for their child had been entirely the decision of someone else.
Youth difficulties and parent influence on youth help seeking
Table 2 presents parent and youth mean total scores on the Total Difficulties scale and the Externalizing and Internalizing subscales of the SDQ. Paired t-tests were conducted on these scores to determine if parent and youth self-rated difficulties scores differed. The only significant difference was on the Externalizing subscale where young people indicated having greater difficulties than reported by their parents, t (118) = −2.30, p < 0.05.
Mean and standard deviation total scores on the parent and self-rated youth Total Difficulties scale and the Externalizing and Internalizing subscales of the SDQ (n = 119).
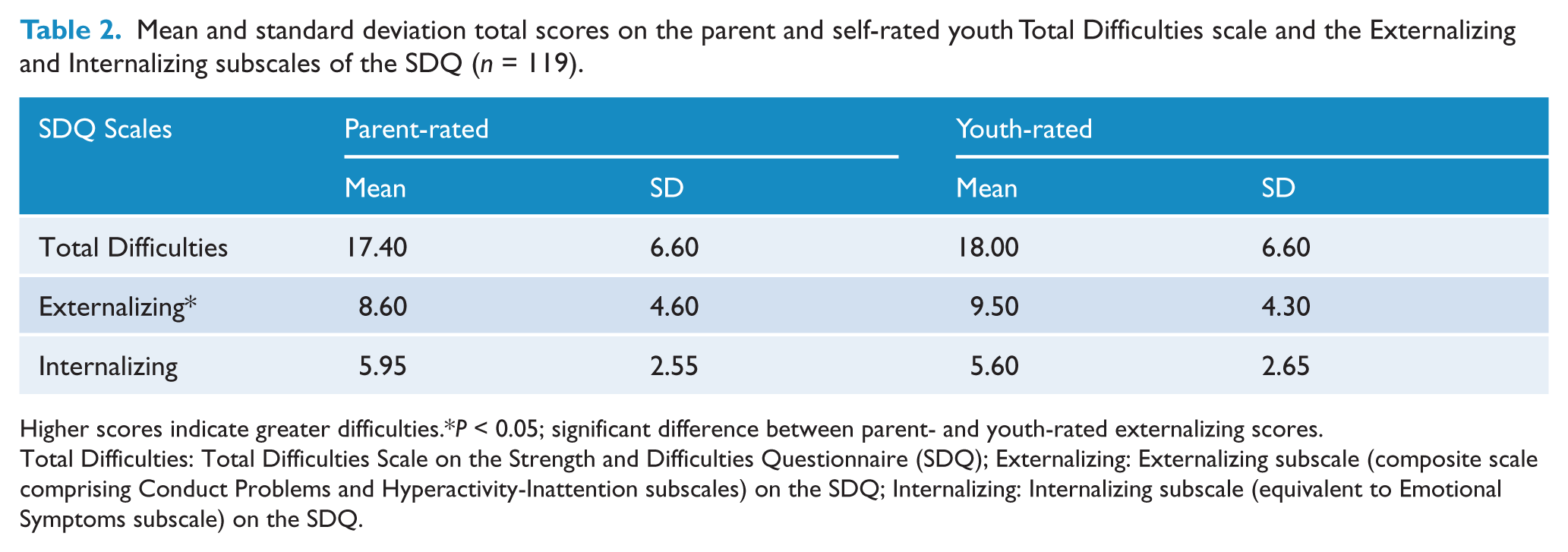
Higher scores indicate greater difficulties.*P < 0.05; significant difference between parent- and youth-rated externalizing scores.
Total Difficulties: Total Difficulties Scale on the Strength and Difficulties Questionnaire (SDQ); Externalizing: Externalizing subscale (composite scale comprising Conduct Problems and Hyperactivity-Inattention subscales) on the SDQ; Internalizing: Internalizing subscale (equivalent to Emotional Symptoms subscale) on the SDQ.
The final set of analyses explored the relationships between the level and nature of self-reported and parent-rated youth difficulties, and the influences on the decision of parents and their children to access professional help. Table 3 provides Spearman’s correlations between the various SDQ scores of parent and adolescent with parent- and adolescent-reported influence variables. Significant positive relationships emerged between the parent-rated influence variables and parent scores on the Total Difficulties and Externalizing SDQ scales. Parent-rated influence variables were not significantly related to parent scores on the Internalizing scale. Higher parental ratings of the young person’s total difficulties were significantly associated with youth respondents reporting greater parental influence on the decision to seek help. Similarly, youth-reported parent influence in the decision to seek help was significantly and positively associated with parent-rated youth internalizing difficulties. As hypothesized, the greater that the young people perceived difficulties, the more they rated independently making the decision to access help. Consistent with these findings, both youth self-reported total difficulties and externalizing difficulties were negatively correlated with youth reports of parental influence.
Spearman’s correlations between parent and youth ratings on the SDQ and influence ratings (n = 119).
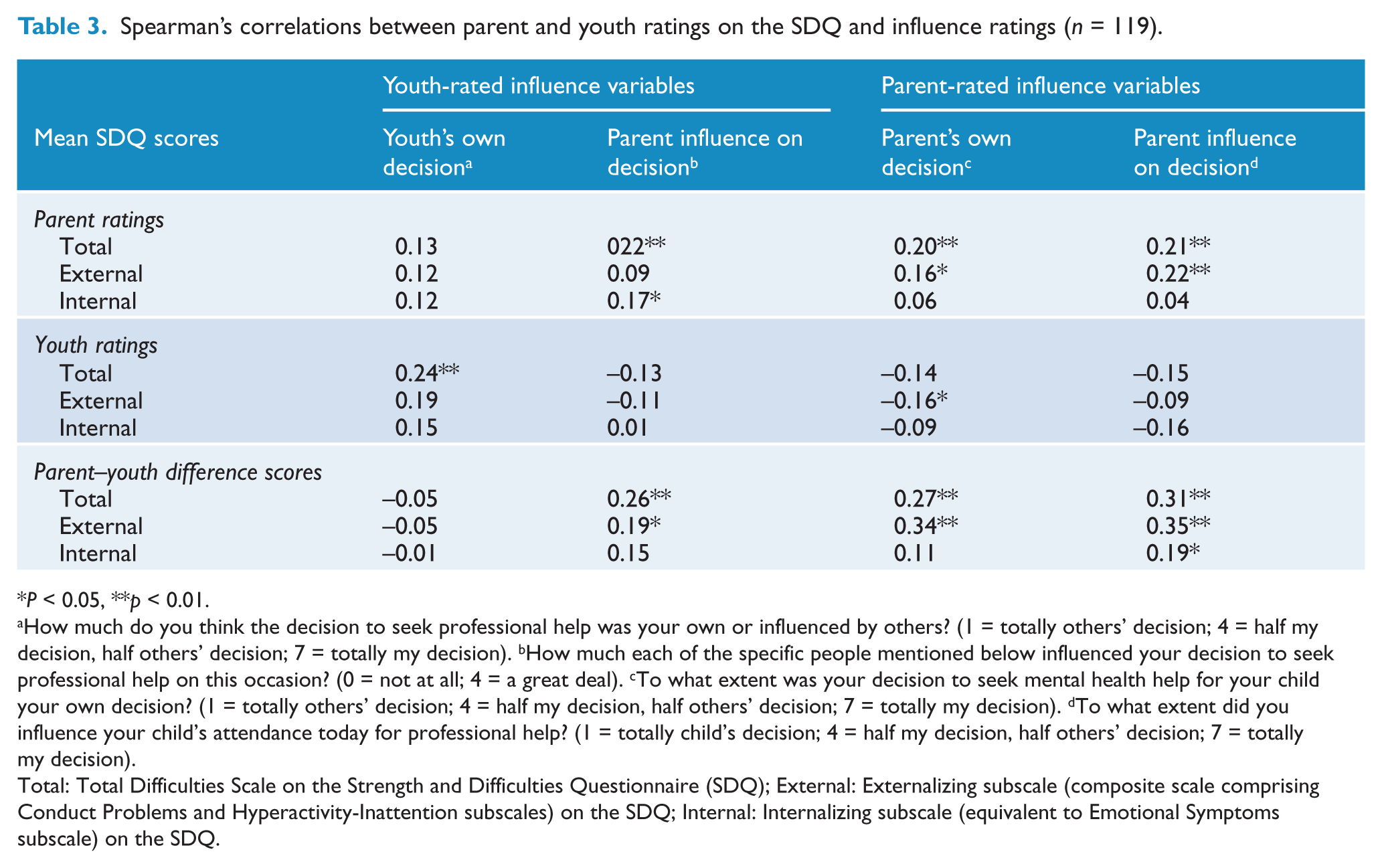
P < 0.05, **p < 0.01.
How much do you think the decision to seek professional help was your own or influenced by others? (1 = totally others’ decision; 4 = half my decision, half others’ decision; 7 = totally my decision). bHow much each of the specific people mentioned below influenced your decision to seek professional help on this occasion? (0 = not at all; 4 = a great deal). cTo what extent was your decision to seek mental health help for your child your own decision? (1 = totally others’ decision; 4 = half my decision, half others’ decision; 7 = totally my decision). dTo what extent did you influence your child’s attendance today for professional help? (1 = totally child’s decision; 4 = half my decision, half others’ decision; 7 = totally my decision).
Total: Total Difficulties Scale on the Strength and Difficulties Questionnaire (SDQ); External: Externalizing subscale (composite scale comprising Conduct Problems and Hyperactivity-Inattention subscales) on the SDQ; Internal: Internalizing subscale (equivalent to Emotional Symptoms subscale) on the SDQ.
Difference scores were calculated by subtracting mean self-rated youth scores from mean parent-rated scores (Yeh and Weisz, 2001; Youngstrom et al., 2000) on the Total Difficulties, Externalizing and Internalizing scales of the SDQ. Difference scores on the SDQ reflect the disagreement between parents and their children on the extent of problems. Difference scores above zero indicate that parent ratings of their child’s difficulties are higher than the young person’s rating of their own difficulties while difference scores below zero indicate the self-reported difficulties of the child are higher than parent-rated child difficulties. As hypothesized, young people and their parents reported more parent influence on the decision to seek help when there was greater disagreement between parent and child on the extent of the child’s difficulties.
In summary, as anticipated, the level of parent-rated involvement in the decision to seek help and the degree to which parents’ exerted influence on their children to access help were related to parent ratings of their child’s total difficulties and the young person’s externalizing behaviour. Parents reported intervening more actively to find help when their child had conduct or hyperactivity problems than when the young person had emotional problems. When there was greater parent–child disagreement on the level of the young person’s total difficulties, externalizing problems and emotional symptoms, parents also reported being more influential in the decision to seek help.
Discussion
Although almost all the young people in this study were influenced by others to access help, parents were clearly the strongest source of influence. However, parent ratings of youth internalizing difficulties were not related to how much parents rated their own influence on their child in accessing a clinical service. Consistent with past findings (Wu et al., 1999) this suggests that parents may be less concerned about or unaware of the magnitude of the emotional problems being experienced by their child. The internalized distress of emotional symptoms is likely to make problem recognition more challenging for parents (Logan and King, 2002). This may be particularly so for young people who fear being viewed as ‘not coping’ or for those who do not confide easily in their parents. Even though parents may realize that there are emotional problems, the degree of distress expressed as a function of these internal experiences may be perceived as low and therefore urgency or demands to seek help may be reduced. Another possibility is that the threshold beyond which parents intervene is higher for emotional problems than for externalizing behaviours because having emotional issues in adolescence is normalized as ‘part of growing up’ (Logan and King, 2001).
Interestingly, while parent ratings of the young person’s emotional symptoms were not related to parent reports of being influential in the decision to access help, there was a positive relationship between youth-reported parental influence to attend the initial CAMHS appointment and youth-rated emotional problems. Together these results indicate that although parents did not recognize their own influence, young people in the study with internalized problems perceived influence from their parents to attend the initial interview. Otherwise, these young people may not have accessed services.
When there was greater disagreement between parent and child reports on the young person’s overall, externalizing and emotional difficulties, parents became more involved and exerted more influence on their child to access help. Put simply, parents may react more strongly when they believe that their child is not sufficiently acknowledging their problems and need for help. This finding is unlikely to be a function of young people in this sample under-reporting their levels of externalizing problems because as a group they rated themselves higher on externalizing problems than did their parents. Further, the overall means in the current sample are similar to the top 10% found in an Australian normative sample (self-report 19+ boys and 15+ girls) (Mellor, 2005). The same normative study also found that on average young people over 14 years tended to rate externalizing problems higher than their parents (Mellor, 2005).
Wu and colleagues (1999) found in a community sample of parents that they would access services more readily for their child’s perceived externalizing problems than if the young person was experiencing depression. Similarly, in the clinical sample of the present study, parent self-report of influence was not related to parent perception of the young person having internalizing problems. However, it appears that when parents recognize that their child is experiencing internalized distress but the young person disagrees that they are suffering these emotional symptoms, parents do exert influence to have their child attend services. Previous research shows that adolescents are resistant to accessing formal help (Reavley et al., 2010; Sawyer et al., 2007), and this study suggests that it is relatively unlikely that young people will independently self-refer to mental health services. In many instances, parents break down the barriers to formal professional help for young people by locating services, providing transport to appointments and meeting the cost of services. However, when faced with a young person who is resistant to accessing help, parents may also need to involve the young person more in the decision-making process and use parental influence to support their child to use available services.
Limitations of the study
Methodological limitations should be considered when interpreting the findings from the present study. First, as the sample is drawn from a clinical population, it does not represent all young people with psychological problems and their parents. Epidemiological research shows that many young people who need psychological help do not access available services (Sawyer et al., 2007). There may also have been sampling bias in the data collection process as only around 50% of parent and adolescent clients attending for an initial assessment interview participated. Young people with greater psychological difficulties or those from families with greater chaos and disruption may have declined to participate.
A further caveat on the results is that the questions to adolescents about the influences on their decision to seek help do not fully capture the processes that led the young person to attend the initial assessment interview. The assumption in these questions is that the young person has decided to seek professional help because they turned up at the service. It is possible that some young people attended because they were influenced to attend the CAMHS interview but that they had not actually made that decision themselves. That is, they had not in their own mind ‘decided’ to access services. Reaching the decision to access mental health services involves cognitive processes such as the young person recognizing they are experiencing problems, that it may be a mental health problem, and then deciding to find professional help. A worthwhile task in future studies would be to examine where participants placed themselves in the preparatory stages of help seeking and how this related to influences on their decision to access help.
Conclusions
The potential negative impact of parental influence on the treatment process may be further exacerbated when parent and child disagree on the nature and extent of the problem and the need for therapy (Yeh and Weisz, 2001). Strategies for identifying these potential parent–child conflicts and engaging the support of other potential sources of influence to reduce some of these tensions are needed. At a practice level, referral sources and clinicians conducting triage and assessments need to be aware of the effects of discrepant views between parent and child regarding the presenting problem. The level of influence needed to get the young person to treatment should be considered in the first meeting. Questions that clarify the processes that led the family to attend the appointment and that elicit different perspectives about the nature of the problem are a first step towards reducing the potential impact of any discrepancies.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.