
Abstract
Objective:
Frequent callers present a challenge for crisis helplines, which strive to achieve optimal outcomes for all callers within finite resources. This study aimed to describe frequent callers to Lifeline (the largest crisis helpline in Australia) and compare them with non-frequent callers, with a view to furthering knowledge about models of service delivery that might meet the needs of frequent callers.
Method:
Lifeline provided an anonymous dataset on calls made between December 2011 and May 2013. We assumed calls from the same (encrypted) phone number were made by the same person, and aggregated call level data up to the person level. Individuals who made 0.667 calls per day in any period from 1 week to the full 549 days for which we had data (i.e. 4.7 calls in 7 days, 20 calls in 30 days, 40 calls in 60 days, etc.) were regarded as frequent callers.
Results:
Our analysis dataset included 411,725 calls made by 98,174 individuals, 2594 (2.6%) of whom met our definition of frequent callers. We identified a number of predictors of being a frequent caller, including being male or transgender, and never having been married. The odds increased with age until 55–64 years, and then declined. Suicidality, self-harm, mental health issues, crime, child protection and domestic violence issues all predicted being a frequent caller.
Conclusions:
Collectively, frequent callers have a significant impact on crisis lines, and solutions need to be found for responding to them that are in everybody’s best interests (i.e. the frequent callers themselves, other callers, telephone crisis supporters who staff crisis lines, and those who manage crisis lines). In striking this balance, the complex and multiple needs of frequent callers must be taken into account.
Introduction
Crisis helplines have provided support to individuals in the community who are experiencing personal crisis (including risk of suicide) since they were introduced in the 1950s and 1960s (Lester, 2002). Helplines are generally staffed by trained volunteers or para-professionals, allow callers to remain anonymous, and only cost the caller the price of a standard telephone call (Coman et al., 2001; Hall and Schlosar, 1995; Kalafat et al., 2007; Lester, 2002; Sawyer and Jameton, 1979). Many, though not all, are available on a 24-hour basis.
In Australia, Lifeline is the largest national crisis helpline. Lifeline was established in Sydney in 1963 and is a not-for-profit organisation which offers a free 24-hour access to telephone crisis support, suicide prevention, and a referral service. It operates from call centres across Australia and is staffed by more than 3000 volunteers and some paid staff who have received specific training in interacting with callers. Lifeline uses the term ‘telephone crisis supporters’ to describe these individuals. Other services use different terms – such as counsellors (or crisis counsellors, telephone counsellors) (Apsler, 1976; Barmann, 1980; Burgess et al., 2008; Haycock, 1997; Leuthe and O’Connor, 1980; Watson et al., 2006), helpers (Mishara et al., 2007), volunteers (Brunet et al., 1994; Daigle and Mishara, 1995; Hall and Schlosar, 1995; Kinzel and Nanson, 2000; MacKinnon, 1998; Pollock et al., 2010), and staff (Greer, 1976; Torop and Torop, 1972) – but we use Lifeline’s terminology throughout this paper.
As their name suggests, crisis helplines are designed to assist callers who are experiencing a crisis. A crisis is defined as a transient state of psychological disequilibrium during which a person’s usual coping mechanisms are disrupted (Kalafat et al., 2007; Sawyer and Jameton, 1979). Crisis helplines aim to help callers to develop a plan to manage the situation that has precipitated the crisis, and/or recommend services that can provide specialist support. A common characteristic of crisis helplines is a strong emphasis on developing a rapport with callers through listening to the presenting problems with respect, concern and a non-judgmental attitude (Hall and Schlosar, 1995; Kalafat et al., 2007).
Assistance from crisis helplines is intended as a one-off or time-limited intervention (Kalafat et al., 2007). Some people, however, make numerous calls to crisis helplines over defined periods. These callers have been termed ‘frequent’ (Haycock, 1997; Leuthe and O’Connor, 1980), ‘chronic’ (Barmann, 1980; Bartholomew and Olijnyk, 1973; Bassuk and Gerson, 1980; Brockopp, 1970; Greer, 1976; Imboden, 1980; Lester and Brockopp, 1970; Sawyer and Jameton, 1979; Speer, 1971), and ‘repeat’ (Hall and Schlosar, 1995; Houry et al., 2004) callers. In this paper, we use the nomenclature ‘frequent callers’ to describe them. Frequent callers present a challenge for these services; they strive to achieve optimal outcomes for all callers but have finite resources available. Although there are variations between services in their capacity to respond to incoming calls, frequent use of crisis helplines by the same individuals reduces the availability of counsellors to other callers for immediate intervention, and may mean that some calls are left unanswered (Watson et al., 2006). Services also grapple with the question of how best to respond to people calling frequently, recognising that inadvertently encouraging dependency in these callers may not be in their best interests.
Understanding who makes multiple calls to crisis helplines and what drives them to call could inform interventions better suited to the needs of this caller group. Anecdotally, there is sometimes a perception that frequent callers are isolated individuals who are not necessarily experiencing any form of crisis but who contact services like Lifeline for general support (Lester and Brockopp, 1970; Speer, 1971; Watson et al., 2006). Several studies have tried to characterise frequent callers, and we recently reviewed these (Middleton et al., 2014). These studies suggest that individuals who make frequent calls to crisis helplines tend to be male and unmarried, but their findings are more equivocal in terms of other demographic details (Bartholomew and Olijnyk, 1973; Burgess et al., 2008; Greer, 1976; Ingram et al., 2008; Lester and Brockopp, 1970; Sawyer and Jameton, 1979). They also suggest that frequent callers contact crisis helplines because they are seeking social support, have mental health issues or are experiencing physical illness (Bartholomew and Olijnyk, 1973; Burgess et al., 2008; Coveney et al., 2012; Ingram et al., 2008; Simon et al., 2006). In addition, they indicate that a high proportion of these callers have a history of suicidal behaviour (Bartholomew and Olijnyk, 1973; Greer, 1976; Lester, 2002; Murphy et al., 1969; Sawyer and Jameton, 1979).
Although these studies offer valuable insights about this caller population, four limitations make it difficult to draw conclusions from the existing findings. First, frequent callers have either not been defined (Sawyer and Jameton, 1979) or have been defined in different ways (e.g. classified as those who have made more than one call to a crisis helpline, made a specific number of calls over a single defined time period, and/or made extensive numbers of calls about the same problem) (Apsler, 1976; Bartholomew and Olijnyk, 1973; Burgess et al., 2008; Coveney et al., 2012; Greer, 1976; Ingram et al., 2008; Johnson and Barry, 1978; Lester and Brockopp, 1970). Second, with one exception (Ingram et al., 2008), the samples of callers and calls in these studies have tended to be fairly small and/or not representative. Third, apart from a handful of studies (Burgess et al., 2008; Coveney et al., 2012; Ingram et al., 2008), these studies present data which is now at least 10 years old. Finally, the majority of studies have been descriptive only, and only a relatively small number have made comparisons between frequent callers and those who call less often (Apsler, 1976; Burgess et al., 2008; Coveney et al., 2012; Greer, 1976; Ingram et al., 2008; Johnson and Barry, 1978; Lester and Brockopp, 1970; Mishara and Daigle, 1997; Sawyer and Jameton, 1979). These study weaknesses have limited collective understanding about who frequent callers are and what their needs might be. Our review concluded that future work in this area required greater consistency in classifying frequent callers, larger and more representative samples, and improved study designs (Middleton et al., 2014).
The current study aimed to describe frequent callers to Lifeline and compare them with non-frequent callers, with a view to furthering knowledge about the models of service delivery that might meet the needs of frequent callers, other callers, counsellors and service managers. Our ultimate goal was to inform current thinking about how to approach the issue of frequent callers in a manner that meets both their needs and the needs of Lifeline and other crisis helplines. We deliberately set out to overcome the limitations that have beset previous studies. We addressed the definitional issue by proposing a clear, scalable definition of the term ‘frequent caller’ on the basis of analysis of current patterns of calls made to Lifeline. We overcame the issues of sample size/representativeness and contemporariness by including data on all calls to Lifeline over an 18-month period; this made our study larger and more current than all other studies that have been conducted to date, including previous studies that have used Lifeline data (Burgess et al., 2008; Watson et al., 2006). We made explicit comparisons between frequent and non-frequent callers, examining whether the former differed from the latter on the basis of their socio-demographic characteristics, their clinical histories, and the reasons for and durations of their calls.
Method
Lifeline provided us with data on calls made between 1 December 2011 and 31 May 2013. Although callers contacting Lifeline remain anonymous, certain data are routinely captured for each call, either automatically through the service’s computerised telephony system or by the telephone crisis supporter entering information into an operational database. These data include: phone number; call date and time; region of call origin; call process (e.g. queuing time, duration of the call); caller demographics (age, sex, marital status); presenting issues (e.g. safety issues, such as suicidality); and call type (crisis vs non-crisis). Approval for this study was granted by The University of Melbourne’s Human Research Ethics Committee.
Before releasing the data to us, Lifeline encrypted the phone numbers associated with each call using a system of unique, randomly generated codes. We made the assumption that calls from the same (encrypted) phone number were made by the same person.
As a rule of thumb, Lifeline regards people who make 20 or more calls per month as frequent callers. We used this as our starting point for defining and identifying frequent callers, expanding the definition to cater for different time periods. In practical terms, we converted 20 calls in 30 days to a rate (i.e. 0.667 calls per day). After converting our person-call dataset to a person-day dataset, we applied this rate to periods that began at 1 week and incremented daily up to the full 549 days for which we had calls data to determine the number of calls within each period that would qualify an individual as being a frequent caller (4.7 calls in 7 days, 5.3 calls in 8 days, 6.0 calls in 9 days and so on). We treated each of these periods as ‘windows’ and iteratively ran them across each individual’s daily-level data. We classified an individual as a frequent caller (yes or no) if during any window he or she had a number of calls that met or exceeded the qualifying number of calls.
In the process of aggregating data up to the person level, we also defined a number of other variables. Sex was coded into three categories (female, male, transgender or intersex), and age was coded into six categories (≤24, 25–34, 35–44, 45–54, 55–64, ≥65). Marital status was coded into four categories (never married, married/de facto, separated/divorced, widowed). Because sex, age and marital status were not recorded for every call, we used each individual’s most common (mode) value to define these variables from the available information.
We used call duration, defined as the time a telephone crisis supporter spent on an individual call with a given caller, to compute an average call duration for each person, and then classified this into five categories (≤5 minutes, 5–10 minutes, 10–20 minutes, 20–30 minutes, ≥30 minutes).
We coded individuals who were identified for suicide safety assessment by Lifeline’s telephone crisis supporters during each call. If, during any given call, one or more of the following events were recorded, then we classified them as being suicidal at the time of that call: a telephone crisis supporter identified suicide as a safety issue during the call; the caller indicated he/she was considering suicide; or the caller indicated he/she had engaged in self-harm or was about to do so. Using Lifeline’s safety assessment tool, we also constructed measures of self-harm, domestic violence, crime, child protection and mental health issues. That is, if a telephone crisis supporter had activated the safety assessment tool, a caller was flagged against those issues. When converting the dataset to the person-level, we considered a person identified through the safety assessments (e.g. suicide, self-harm) if they were ever flagged as such during their call history.
We computed descriptive statistics for calls (using call-level data) and callers (using person-level data). In our primary analysis, we used multivariate logistic regression to identify the characteristics of frequent callers. The predictors were age, sex, marital status and average length of call, and history of suicide, self-harm, domestic violence, crime, child protection and mental health issues (from the safety assessments). A large amount of missing data for age and marital status (i.e. ‘unknown’ checked in these fields) meant that 55% of observations were excluded from the primary analysis. We therefore undertook two sensitivity analyses to determine whether the findings for the other variables were affected by the missing data. In the first sensitivity analysis, we excluded age and relationship status from the model; in our second sensitivity analysis, we used multiple imputation methods to impute age and relationship data. Specifically, we estimated M = 20 values for each missing observation on these two variables and re-estimated our primary model, combining the estimates from the 20 imputation datasets using standard methods. Both sensitivity analyses substantially increased the sample size (just 6.3% of observations were excluded). Because both sets of results were similar for all predictors except one (average length of call), we focus on reporting the results of the primary analysis for the remaining variables. We report results for both the primary analysis and the two sensitivity analyses for the average length of call variable.
Results
Profile of calls
In the study period, there were 850,344 calls to Lifeline. Since a phone number was used as a proxy for a caller, 345,553 (40.6%) contacts from blocked numbers were excluded from the dataset, as were 80,021 (9.4%) calls of less than 60 seconds’ duration, 219 calls with no end time and four duplicate calls from the same caller at the same moment in time. We also excluded several categories of non-crisis calls: hang-up calls (2967 calls or 0.7%), unwelcome calls (7634 or 1.8%), shop or donation enquiries (956 or 0.2%) and feedback calls (1265 or 0.3%). We retained non-crisis calls for referrals and requesting information (9665 calls) and for other reasons (9539 calls). This left 411,725 calls for analysis (48.4% of all calls). The average duration of these calls was 20.7 minutes (SD = 11.1 minutes; range: 1 minute to 2.8 hours). Individuals contacted Lifeline with a range of issues (see Figure 1). The most common presenting issues were problems with family and relationships (42.5%), mental health problems (33.1%), and issues related to self-identity and self-esteem (e.g. sense of purpose, loneliness, self-confidence or self-esteem, sexuality) (28.5%). Suicide and suicidal thoughts were the focus of 7.9% of all calls.
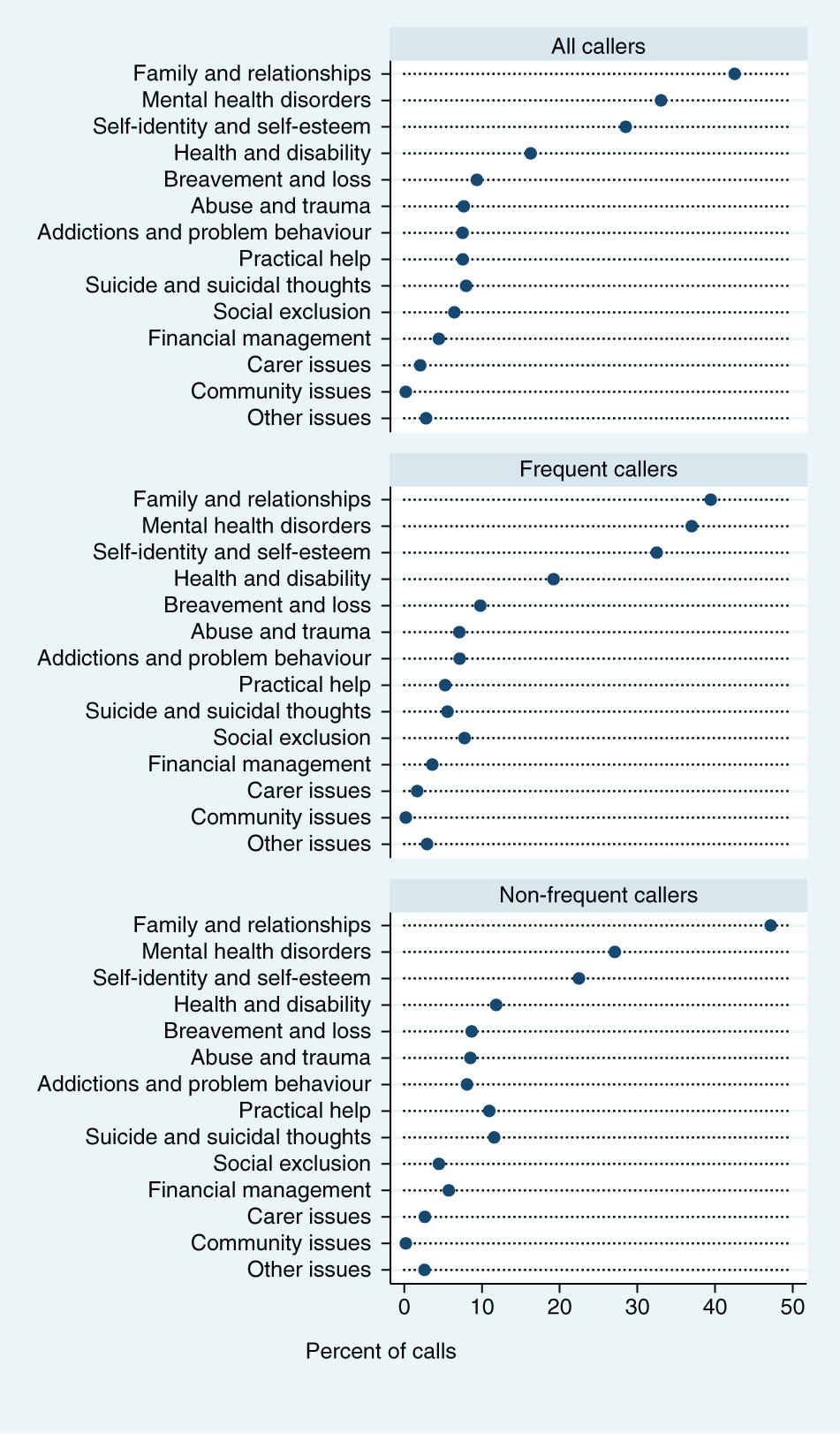
Presenting problems as a percentage of all calls (n=411,725 calls): calls by frequent callers (n=247,547) and calls by non-frequent callers (n=164,178). (Note: categories do not sum to 100% because multiple presenting problems can be recorded for each call.)
Characteristics of callers
The above 411,725 calls were made by 98,174 individuals. Of the people contacting Lifeline, 75,362 (76.8%) made a single call during the study period and 22,812 (23.2%) rang more than once. The mean number of calls was 4.2 calls per person (SD = 37.6), ranging from one to 3259 calls. The characteristics of these callers are presented in Table 1 (‘All individuals’ column). There were almost twice as many female callers as male callers (60,561 or 61.7% vs 31,273 or 31.9%). A further 88 callers (0.1%) identified themselves as transgender or intersex, and sex was not recorded for 6252 (6.4%). Most individuals contacting Lifeline and whose age was recorded were in the age groups 25–34 years (13,018 or 13.3%), 35–44 years (12,480 or 12.7%), and 45–54 years (10,443 or 10.6%). Adolescents and young adults (15–24 year olds) represented 9.3% (9091) of Lifeline callers, those aged 55–64 years accounted for 6.6% (6443), and a further 4.7% (4661) of the callers were 65 years old and older. Age was unknown for the remaining 42,038 callers (42.8%). Over one-quarter of callers were married or in de facto relationships (28,154, or 28.7%), 15,441 (15.7%) were separated/divorced, 15,220 (15.5%) had never been married, and 2696 (2.7%) were widowed. Relationship status was unknown for 36,663 individuals (37.3%).
Descriptive characteristics of Lifeline callers: all callers (n=98,174), frequent callers (n=2594) and non-frequent callers (n=95,580).
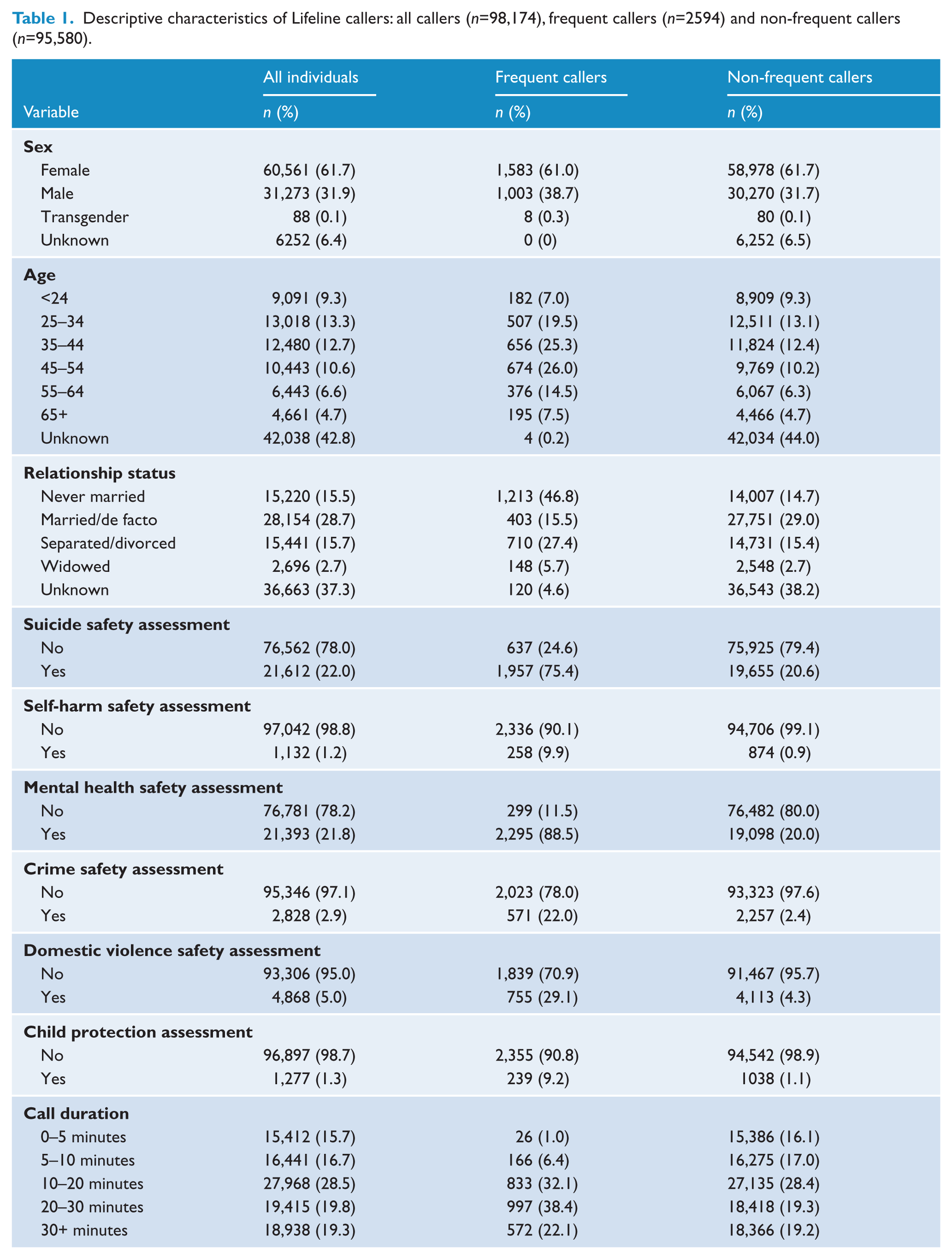
The assessments by Lifeline telephone crisis supporters indicated that suicide was identified as a safety issue for 22.0% of the 98,174 callers and self-harm was identified for 1.2% of them. Mental health issues were identified as a safety issue for 21.8% of callers. Crime was identified by telephone crisis supporters as a safety issue for 2.9% of all callers and domestic violence was identified as an issue for 5.0% of all callers. Child protection featured as a safety issue for only 1.3% of all callers.
For the majority of callers, an average call lasted less than 20 minutes. However, about 40% of individuals (38,353 callers) had average call durations that exceeded 20 minutes.
Characteristics of frequent callers
Individuals who met the definition of being a frequent caller represented 2.6% (2594) of callers and 60.1% (247,547) of calls during the period. Among frequent callers, the mean number of calls during the period was 95.4 calls per person (SD = 211.6), ranging from five to 3259 calls. The characteristics of frequent callers are shown in Table 1 (‘Frequent callers’ and ‘Non-frequent callers’ columns). Frequent callers were predominately female (1583 or 61.0% vs 1003 or 38.7%). Just 0.3% or eight individuals identified as transgender and there were no missing data. The age profile for frequent callers was similar to that of all callers – most were aged between 25 and 54 years (1837 individuals or 70.8%). The remainder were aged 15–24 years (182 or 7.0%), 55–64 years (376 or 14.5%) or 65 and older (195 or 7.5%). Age was unknown for four frequent callers (0.2%). In total, 1213 frequent callers (46.8%) were never married, 403 (15.5%) were married or in de facto relationships, 710 (27.4%) were separated or divorced and 148 (5.7%) were widowed. Relationship status was unknown for 120 (4.6%) frequent callers. Suicide was identified as a safety issue by telephone crisis supporters for 75.4% of frequent callers and self-harm for 9.9%. Mental health issues were identified for 88.5% of frequent callers and crime for 22.0%. Domestic violence was identified by telephone crisis supporters for 29.1% of frequent callers and child protection for 9.2% of frequent callers. Among frequent callers, the average call duration was typically greater than 20 minutes (60.5% or 1569 frequent callers).
We identified a number of predictors of being a frequent caller (Table 2). Males were at slightly greater risk of being a frequent caller than females (odds ratio (OR) = 1.2) and transgender individuals had 2.8 times the odds of females (although it should be noted that this estimate is based on only a small number of individuals). Increased age was associated with being a frequent caller. Compared to those aged under 24 years (the reference category), the odds of being a frequent caller increased with each age band until a peak of 55–64 years, after which there was a slight decline. At 55–64 years the odds of being a frequent caller were 5.9 times the odds of someone aged under 24 years; for those aged 65 years or older the odds were 5.5 times that of the reference category. Those who were never married had the highest odds of being a frequent caller – all other groups had between 0.2 and 0.6 times the odds of being a frequent caller.
Primary analysis – multivariate logistic regression models predicting frequent callers to Lifeline, n=44,587.
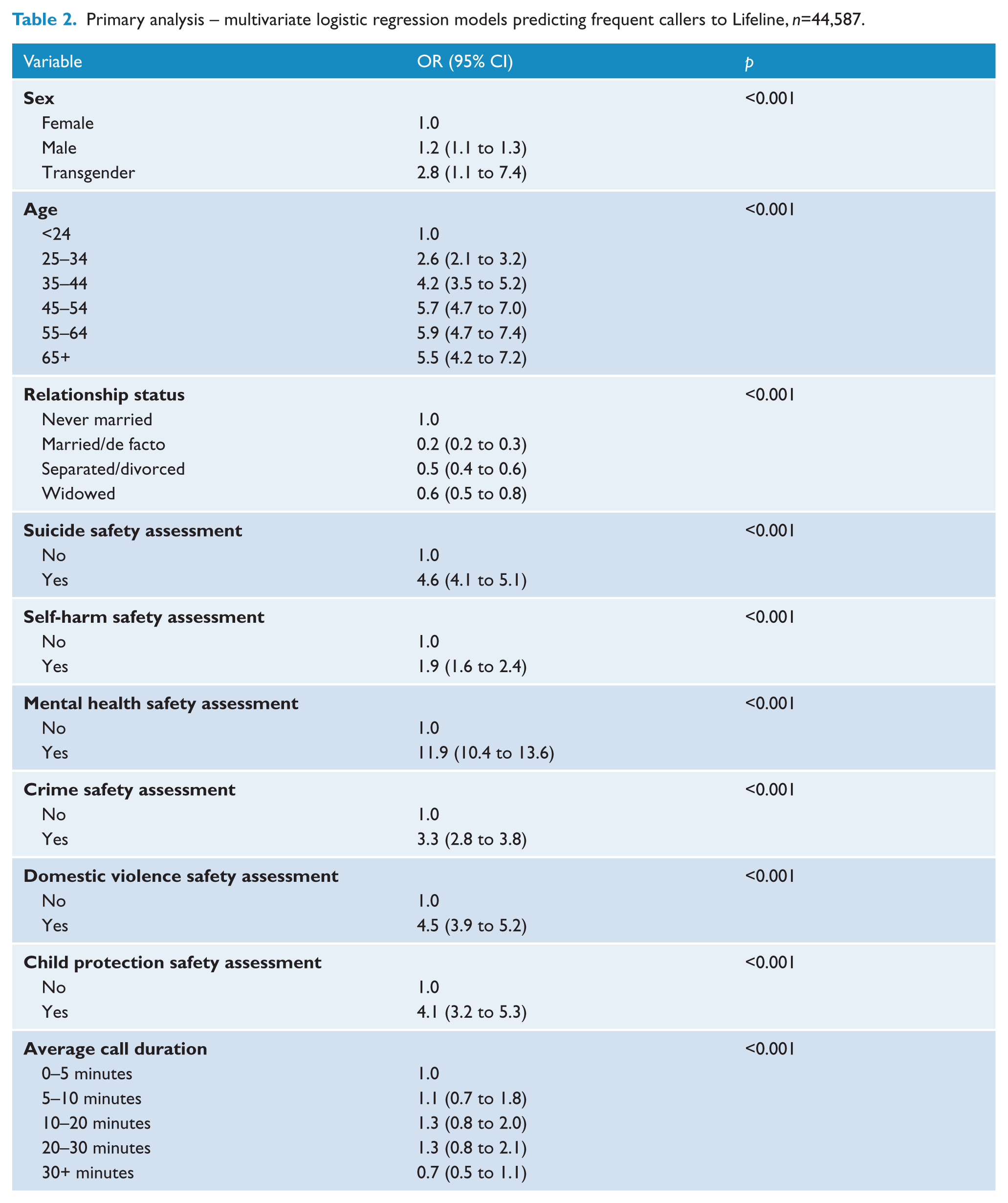
Individuals for whom suicide was identified as a safety issue by telephone crisis supporters had 4.6 times the odds of being a frequent caller compared with those for whom suicide was not identified as an issue. Safety assessments for self-harm were also associated with being a frequent caller (OR = 1.9). Those for whom mental health issues were identified by telephone crisis supporters had 11.9 times the odds of being a frequent caller compared with those for whom no such issues were identified. Safety assessments for crime were associated with the odds of being a frequent caller (OR = 3.3) and individuals for whom domestic violence or child protection were identified as safety issues had 4.5 and 4.1 times the odds, respectively, of being a frequent caller.
With regards to average call duration, in the primary analysis, compared to those who spoke on average between 1 and 5 minutes with a telephone crisis supporter (the reference category), those who spoke for an average of between 5 and 30 minutes had a slight increase in the odds of being a frequent caller (OR range 1.1 to 1.3); those who spoke with telephone crisis supporters for 30 minutes or more had lower odds than the reference category of being a frequent caller (OR = 0.7). But in both sensitivity analyses (Table 3), there was evidence that longer call duration was associated with increased odds of being a frequent caller. In comparison to the reference category, the odds of being a frequent caller increased as average call duration increased, reaching a peak for calls between 20 and 30 minutes (OR = 4.5 for complete case analysis; OR = 4.0 for multiple imputation analysis); for calls greater than 30 minutes, the odds of being a frequent caller were 2.6 times (complete case analysis) and 2.2 times (multiple imputation analysis) that of the odds in the reference category.
Sensitivity analyses – multivariate logistic regression models predicting frequent callers to Lifeline, n=91,922.
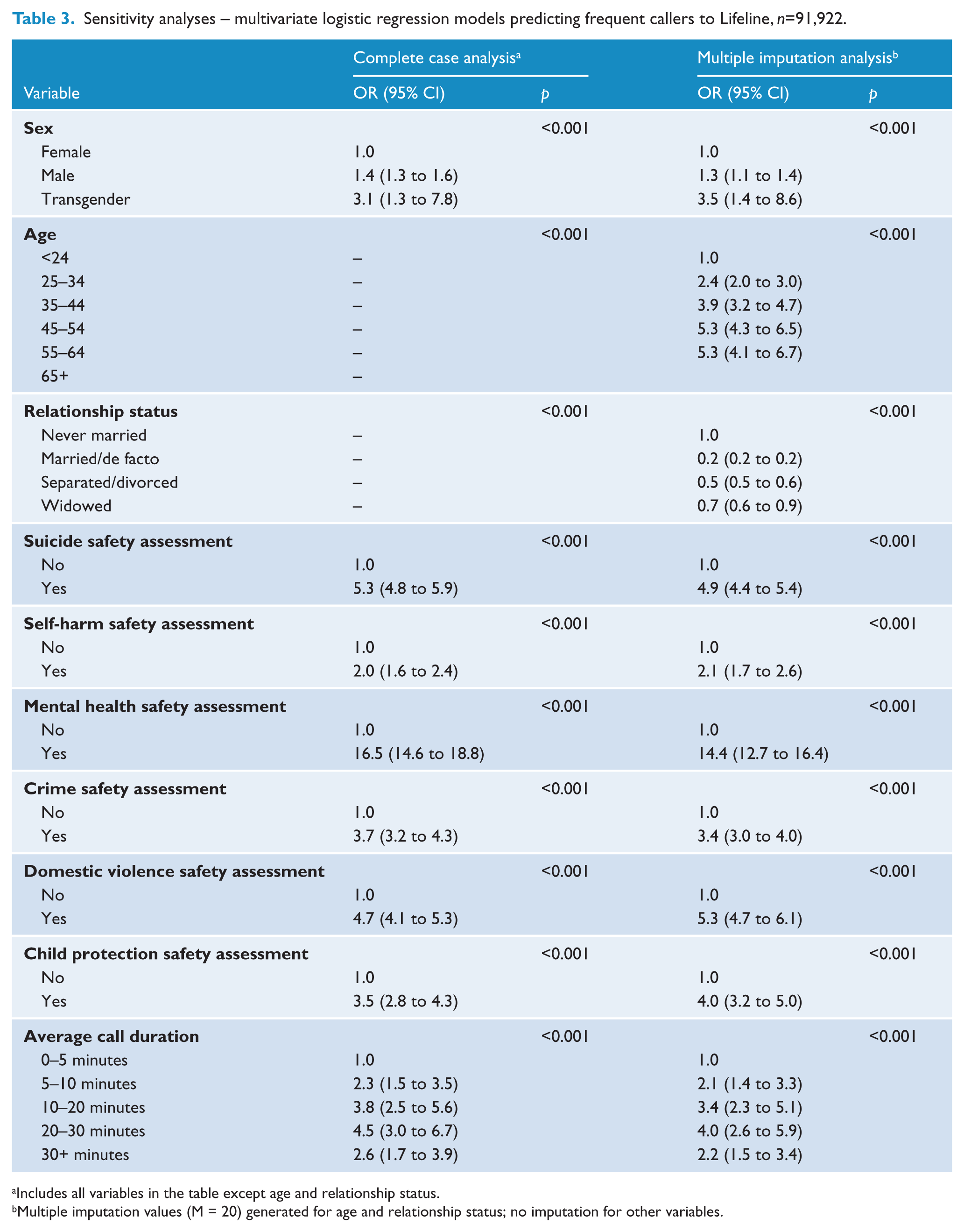
Includes all variables in the table except age and relationship status.
Multiple imputation values (M = 20) generated for age and relationship status; no imputation for other variables.
Discussion
In this study of over 411,000 calls over an 18-month period to Lifeline, we found that frequent callers represented approximately 3% of all callers but 60% of calls. Our definition of a frequent caller was based on a moving window whereby individuals whose number of calls during the window exceeded 0.667 calls per day (e.g. 4.7 calls in 7 days, 20 calls in 30 days, and so on). As such, our definition does not distinguish between those patterns of frequent calling that are fluctuating in nature from those patterns that are continuing in nature. Some make a high number of calls over a relatively short period, and others do so over much longer periods. Some only just reach the threshold for being considered a frequent caller, and others would be regarded as extremely frequent callers. Further work is needed to tease out the differences between these groups in terms of their socio-demographic and clinical characteristics, the reasons for their calls, and the benefits they feel they get from calling.
Our data suggest that the perception that frequent callers are lonely and contacting services such as Lifeline for general support underestimates their needs. There is some evidence that they may have fewer social supports than other callers, if never having been married is regarded as a proxy for this, but, as a group, they don’t call without good reason. Compared with non-frequent callers, they are more likely to present with significant mental health problems and high levels of risk, including for suicide. They are also more likely to experience issues associated with child protection and domestic violence.
This suggests that frequent callers cannot be ignored and should not be dismissed; their issues are many and complex. Nonetheless, careful consideration needs to be given to how best to manage their needs within the resourcing constraints of crisis lines. Their calls consume a considerable amount of time, although it should be noted that frequent callers are less likely to make very long calls (i.e., calls which last for half an hour or more) than non-frequent callers.
There is a dearth of literature on models of service delivery for frequent callers, but our recent review (Middleton et al., 2014) identified a few small studies. These tested interventions which used a combination of approaches, including limiting the number of calls an individual could make over a given period unless there were extenuating circumstances, and assigning a specific telephone crisis supporter to frequent callers who would initiate contact with them at designated times or engage in written correspondence with them (Barmann, 1980; Brunet et al., 1994; Hall and Schlosar, 1995). These interventions all showed promise, as evidenced by a reduction in the number of calls and/or the amount of call time, but all were tested on small samples of frequent callers (Barmann, 1980; Brunet et al., 1994; Hall and Schlosar, 1995). Our study suggests that these sorts of interventions might be helpful in managing frequent callers, providing that they are tailored and take into account their profile. As noted, frequent callers have complex problems and high levels of need, so any system that involves restrictions on calls requires a safety net which allows crisis calls. In addition, a model that involves alternative forms of communication with telephone crisis supporters should reflect the communication preferences of typical frequent callers, noting that these may be influenced by sex and age.
Other models that have been proposed but not tested include more intensive interventions like developing comprehensive management plans and offering short-term treatment programs for depression and anxiety (Burgess et al., 2008; Sawyer and Jameton, 1979). These sorts of interventions are probably beyond the capacity of most crisis helplines and are not within their remit, so they might require relationships with and referrals to other services. This sort of approach makes intuitive sense, particularly given our finding that frequent callers may have a range of clinical issues and face extreme situational circumstances. We would caution, however, that a parallel study that we are conducting has shown that frequent callers to crisis helplines are likely to already be using other services, particularly primary mental health-care services (Bassilios et al., Forthcoming).
Finally, interventions such as internet-based cognitive behavioural therapy (CBT) may be a useful referral route for addressing underlying mental health issues. For instance, a recent randomised controlled trial found that depression was lower among telephone helpline callers who received an web-based CBT intervention than those who received treatment as usual (Farrer et al., 2011). Interestingly, the study found no differences between those in the treatment arm who received internet CBT only and those who received internet CBT plus telephone support.
It is worth returning to the finding about the average length of frequent callers’ calls here. We found conflicting results between the primary analysis and the sensitivity analyses. In the primary analysis, which included adjustment for age and marital status (but also a large amount of missing data), the results indicated that frequent callers are less likely to make very long calls than non-frequent callers. In both sensitivity analyses, we found that frequent callers were more likely to make longer calls. There are plausible explanations for both these findings. With regard to the first finding – that frequent callers are less likely to make long calls – one interpretation is that Lifelines’ telephone crisis supporters are managing these callers themselves, containing their calls as far as possible and/or suggesting that they make use of alternative services (e.g. Lifeline’s own online chat service or other, external mental health services). Another interpretation is that the callers themselves are finding that if they call often they do not feel the need to stay on the line for extended periods. Explanations for the second finding – that frequent callers are more likely to make longer calls – suggest that the opposite explanations may explain the frequent callers’ behaviour (i.e. frequent callers are difficult to manage, or they have difficultly managing themselves). Further research is needed to better understand this issue. We are conducting a complementary study which will further explore the nature and outcome of frequent callers’ calls in more depth through a combination of cross-sectional surveys with Lifeline callers, qualitative interviews and linking these data to routinely collected calls data.
Our study had a number of strengths, most notably its sample size and its sophisticated approach to defining frequent callers. It also has some limitations, including the use of administrative data, which whilst contributing to the size of the sample, meant that we had less control over data quality than we might otherwise have had. The majority of data fields were completed by Lifeline’s own telephone crisis supporters, and although they are extensively trained they may have interpreted some coding categories in different ways, thus impacting on inter-rater reliability. Missing data were also something of a problem, although we made every attempt to minimise this. Finally, we relied on an encrypted phone number to identify individuals. There are two limitations with this. First, individuals who call from several different phone numbers will be misclassified as unique individuals; second, where two or more individuals are calling from the same number, they will be misclassified as the same individual.
Notwithstanding these limitations, our study provides important information to further understanding of the phenomenon of frequent callers. Collectively, frequent callers have a significant impact on crisis lines, and solutions need to be found for responding to them that are in everybody’s best interests (i.e. those of frequent callers themselves, those of other callers, those of the telephone crisis supporters who staff crisis lines on a voluntary or paid basis, and those of the management of crisis lines). In striking this balance, the complex and multiple needs of frequent callers must be taken into account.
Footnotes
Acknowledgements
We are grateful to the staff at Lifeline Australia for assistance with data management and the interpretation of the results, in particular Mr Sajid Hassan.
Funding
The research was supported by the Lifeline Research Foundation with funding from Servier Australia.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.