
Abstract
Objective:
The psychological flexibility model has been hypothesized as a transdiagnostic, process-oriented approach to understanding various clinical disorders and problems, including chronic pain, anxiety, and substance misuse. In this study we investigated the model’s applicability to the experience of hearing distressing voices.
Methods:
Fifty people experiencing persisting auditory hallucinations were administered the Kentucky Inventory of Mindfulness Skills, Acceptance and Action Questionnaire, Beliefs about Voices Questionnaire-Revised, Thought Control Questionnaire, and the Beck Anxiety and Depression Inventories. We predicted that psychological flexibility, mindful action, and nonjudgemental acceptance would be negatively associated with distress, disability, and behavioural responses to voice hearing and would have additional explanatory power when included with appraisals of voices and thought-control strategies (as predicted by cognitive models of auditory hallucinations).
Results:
The results showed differential contributions between measures of psychological flexibility and nonjudgemental acceptance. Psychological flexibility accounted for a significant proportion of the variance in regression-based models of depression and anxiety, while nonjudgemental acceptance contributed to the prediction of emotional and behavioural resistance to voices, in addition to appraisals of voices and use of thought-control strategies. However, this was not found for distress associated with voice hearing, life disruption, and engagement with voices, which were explained solely by cognitive variables.
Conclusions:
The study results suggest that psychological flexibility and nonjudgemental acceptance are related to general emotional well being and resistance response styles to voices, but not to specific dimensions of voice hearing.
Introduction
There has been increasing attention to models of human functioning that incorporate constructs such as acceptance, mindfulness, and response flexibility. These models (Hayes and Duckworth, 2006; Moses and Barlow, 2006) suggest that a person’s struggle with their internal experiences can result in greater distress and disability and that developing a flexible stance of nonjudgemental acceptance may be useful in reducing symptom impact.
The psychological flexibility model (Hayes et al., 2012) proposes that experiential avoidance is a stronger contributor to psychopathology than the content (frequency, intensity, negative valence) of private psychological and emotional experiences. Experiential avoidance is considered to be a generalized psychological vulnerability (Kashdan et al., 2006) and has been defined as “when a person is unwilling to remain in contact with particular private experiences (e.g., bodily sensations, emotions, thoughts, memories, behavioral predispositions) and takes steps to alter the form or frequency of these events and the contexts that occasion them, even when this process is unhelpful” (Hayes et al., 1999). Numerous studies have found that experiential avoidance predicts a wide range of quality of life and well-being outcomes (for a review, see Hayes and Duckworth, 2006). It also mediates the impact of acceptance-based interventions (Bond and Bunce, 2000) and moderates the effect of interventions (Masuda et al., 2007) and the impact of coping processes such as cognitive reappraisal (Kashdan et al., 2006). A consistent finding across studies is that higher levels of experiential avoidance are associated with greater impact of distressing and unwanted experiences (Feldner et al., 2003; Kashdan et al., 2006; McCracken, 1998).
One of the ways that psychological flexibility is developed is through mindfulness (Hayes and Duckworth, 2006), a set of skills that involves learning to become aware of the processes of thinking (such as taking thoughts as literal truth or “cognitive fusion”, described by Hayes et al., 1999) and relating differently to these processes by developing a nonjudgemental or decentred stance toward the content of thoughts, emotions, and other private experiences (Teasdale et al., 2002). Mindfulness and acceptance techniques both target the relationship that a person has with their internal experiences (Perez-Alvarez et al., 2008) and cultivate alternate influences over behaviour by allowing the individual to have greater capacity to respond proactively rather than reactively (by chosen value-based behaviours, as described by Hayes et al., 1999). The cultivation of nonjudgemental acceptance encompasses the relationship that a person has with their appraisals, responding to automatic evaluations from a dispassionate stance (Baer et al., 2004) and resulting in fewer efforts to engage in control of internal experiences.
There may be the potential for psychological flexibility models to inform our understanding of distress and disability with psychotic symptoms. Active acceptance of the experience of hearing voices has long been suggested as a way of increasing sense of control and life meaning (Romme and Escher, 1993), and the voices-coping literature suggests that the acceptance of voices may play a role in better functioning and less distress in voice hearers (Farhall and Gehrke, 1997). While experiential avoidance has been implicated in a clinical model of distress with psychosis (Chadwick, 2006), there has been limited empirical attention to psychological flexibility constructs within cognitive models of psychotic symptoms. Cognitive models of psychosis hold central the appraisal of unusual experiences as an important factor in influencing symptom impact (Garety et al., 2001; Morrison, 2001): consistent findings demonstrate associations between appraisals of voices and voice hearers’ affect and behaviour that are not accounted for by the presence of auditory hallucinations or their content alone (Birchwood and Chadwick, 1997; Peters et al., 2012; van der Gaag et al., 2003). There has been some overlap between cognitive and psychological flexibility models, with cognitive models suggesting that certain thought-control strategies, such as punishment and worry (perhaps forms of experiential avoidance), may have a role in increasing symptom impact (Garcia-Montes et al., 2006; Morrison, 2001; Morrison and Wells, 2000).
There is a small set of studies that has explored the relationship of psychological flexibility with dimensions of hearing voices, paranoia, and delusional ideation (Goldstone et al., 2011; Oliver et al., 2012; Shawyer et al., 2007; Udachina et al., 2009), in addition to emotional dysfunction following psychotic episodes (White et al., 2011). The findings of these studies suggest that higher levels of experiential avoidance are associated with greater delusional ideation (Goldstone et al., 2011), greater distress and disability with voice hearing, increased paranoia and poor self-esteem (Udachina et al., 2009), and greater depression and anxiety following psychosis (White et al., 2011). Finally, a recent naturalistic study comparing the influence of coping using psychological flexibility and cognitive reappraisal for those with psychosis suggests that, over time, reappraisal may have limited direct influence on symptom impact, while psychological flexibility has positive associations with quality of life and affect in the presence of psychotic symptoms (Vilardaga et al., 2013).
There is also preliminary evidence from treatment studies that suggests that developing nonjudgemental acceptance and psychological flexibility toward positive symptoms of psychosis may be useful in reducing symptom impact (Bach and Hayes, 2002; Dannahy et al., 2011; Gaudiano and Herbert, 2006; White et al., 2011).
In summary, recent transdiagnostic models consider the effects of experiential avoidance and nonacceptance as contributing to the maintenance of psychological problems; there has been limited attention to these constructs within cognitive models of psychosis, although there is preliminary evidence to suggest that developing nonjudgemental acceptance of voices can be helpful. The present study explored the relationships between acceptance, mindful action, and nonjudgemental acceptance and predictors of distress and disability in auditory hallucinations, such as appraisals of voices as malevolent, benevolent, and omnipotent (Chadwick et al., 2000), as well as the use of thought-control strategies, such as punishment and worry (Garcia-Montes et al., 2006; Morrison, 2001; Morrison and Wells, 2000). This study explored the incremental explanatory power of including acceptance constructs to cognitive models of distress with voice hearing.
Research questions and hypotheses
The two study questions were: (1) what relationships are there between psychological flexibility, nonjudgemental acceptance, appraisals of voices, coping strategies, and voice distress and disability? and (2) do psychological flexibility, mindful action, and nonjudgemental acceptance result in additional predictive power for a range of dependent variables (anxiety and depression symptoms, distress, and disability associated with voice hearing, emotions, and efforts to resist/engage with voices), when included with variables from cognitive models (such as appraisals of malevolence and benevolence, along with thought-control strategies)? It was predicted that psychological flexibility, mindful action, and nonjudgemental acceptance would be negatively correlated with appraisals of voice malevolence and power, resistance to voices, use of thought-control strategies, and voice-related distress and disruption, as well as depressive and anxiety symptoms. It was predicted that appraisals of voices, as well as use of thought-control strategies, would significantly account for the variance of the dependent variables. It was predicted that a significant amount of variance would then be additionally explained by the inclusion of psychological flexibility and nonjudgemental acceptance in models of voice hearing.
Methods
Design and ethical approval
The study used a cross-sectional design and received ethical approval from the Joint South London and Maudsley and The Institute of Psychiatry NHS Research Ethics Committee, UK (REC reference no. 066/04).
Participants and procedure
Participants met the following inclusion criteria: having a case note diagnosis of a psychotic illness according to ICD-10 criteria (F20–29; or F32.3 severe depressive episode with psychotic symptoms), experiencing persisting auditory hallucinations for at least 3 months, and on a stable medication regime (if they were taking medication). Exclusion criteria were those with a history of organic illness or primary diagnosis of substance misuse.
Voice hearers (n=50) were recruited from mental health services in an inner London borough (South London and Maudsley NHS Foundation Trust; 70% from community teams and the Psychological Interventions Clinic for Outpatients with Psychosis and 30% from inpatients wards). Consenting participants were administered the measures in one sitting.
Age was (mean±SD) 31.8±10.54 years (range 18–56 years), 66% were male. 90% had case note diagnoses of F20–F29 “schizophrenia spectrum” and 10% with F32.3; 94% were currently prescribed anti-psychotic medication and 6% were not on any form of psychotropic medication. Participants described hearing voices for an average of 9 years (range from 3 months to 33 years). Consistent with other samples of service users from UK inner city localities, the sample was ethnically diverse (36% White British or other white background, 44% Black British/African/Caribbean, 8% mixed race, 6% British Asian/Asian, and 6% from other background or unstated). The majority were unemployed (74%; student 14%; employed part-time 6%; employed full time 6%).
Measures
Acceptance and Action Questionnaire (AAQ-II)
This 7-item questionnaire (Bond et al., 2011) is designed to be a measure of experiential avoidance/psychological flexibility. Respondents rate the degree to which each statement applies to them on a Likert scale (1 never true to 7 always true; scale range 7–49). High scores on the AAQ-II suggest greater acceptance of mental experiences and persistence with life goals in the face of these experiences. The AAQ-II has good internal reliability, reported at 0.84 (Bond et al., 2011).
Beliefs about Voices Questionnaire-Revised (BAVQ-R)
This 35-item questionnaire (Chadwick et al., 2000) is designed to measure attributions, beliefs, emotional responses, and behaviour about voices. Respondents rate the degree to which each item describes the way they have been feeling in the past week on a 4-point Likert scale (“disagree” to “strongly agree”). The BAVQ-R is made up of three subscales of appraisals (malevolence, benevolence, omnipotence) and two subscales of emotional and behavioural responses (resistance and engagement), which have shown adequate internal consistency (Cronbach’s alpha for each subscale 0.74–0.88; Chadwick et al., 2000). Scales range between 0–18 for malevolence, benevolence, and omnipotence, 0–27 for resistance, and 0–24 for engagement. The behavioural and emotional responses items for resistance and engagement were examined separately, with four response items in each of the behavioural and emotional subscales for engagement and the emotional subscale for resistance (ranges 0–12) and five behavioural items in the resistance subscale (range 0–15).
Kentucky Inventory of Mindfulness Skills (KIMS)
This 39-item scale (Baer et al., 2004) is designed to measure behaviours associated with mindfulness, with subscales including skills of observing, acting with awareness (taking mindful action, with undivided attention), accepting without judgement (nonjudgemental acceptance), and describing. High KIMS scores indicate greater use of mindfulness in daily life; there is good internal consistency, with the alpha coefficients of the subscales scoring between 0.83 and 0.91.
Previous studies investigating the relationship between mindfulness and experiential avoidance (measured by the original AAQ; (Hayes et al., 2004) suggest moderate but significant (p<0.001) correlations with the describe (–0.35), acting with awareness (–0.30), and accept without judgement (–0.26) subscales of the measure (using nonpsychotic samples) (Baer et al., 2004). Scale scores range between 12–60 for observe, 8–40 for describe, 10–50 for acting with awareness, and 9–45 for accept without judgement. For the purpose of hypothesis testing in this study, we used only the acting with awareness and accept without judgement subscales.
Beck Depression Inventory-II (BDI-II)
This 21-item questionnaire (Beck et al., 1996) is designed to measure severity of depressive symptoms; BDI-II scores range between 0–63, with high scores indicating more severe depressive symptoms. It has high reported reliability (coefficient alpha 0.92). Previous correlations with the AAQ-II have been 0.71 in nonpsychosis samples (Bond et al., 2011).
Beck Anxiety Inventory
This 21-item questionnaire (Beck and Steer, 1990) is designed to measure severity of anxiety symptoms; the scale ranges between 0–63, with high scores indicating more severe anxiety symptoms. It has high reported internal consistency (Cronbach’s alpha 0.92–0.94). Previous reported correlations with the AAQ-II have been 0.61 in nonpsychosis samples (Bond et al., 2011).
Thought Control Questionnaire (TCQ)
This 30-item instrument (Wells and Davies, 1994) is designed to measure individual differences in strategies to control unwanted distressing thoughts. All items are scored 1 (never) to 4 (almost always); total scores range from 30–120; all subscales range 6–24: high scores suggest frequent use of thought strategies. The TCQ measures five factors relating to different strategies: distraction, social control, worry, punishment, and re-appraisal. The TCQ has acceptable psychometric properties, with subscale Cronbach alpha scores reported between 0.64 to .79, and adequate test–retest reliability (0.67 to 0.83). Previous subscale correlations with the AAQ have been moderate: punishment (0.37) and worry (0.36) (Hayes et al., 2004).
Psychotic Symptom Rating Scales (PSYRATS) – Auditory Hallucinations subscale
This is an interview-rated scale (Haddock et al., 1999) measuring dimensions of auditory hallucinations, with 11 subscale items for: frequency, duration, location, loudness, disruption, amount and intensity of distress, beliefs about the origin of voices, amount and degree of negative content, and controllability. The PSYRATS demonstrates high interrater reliability and was designed to be sensitive to changes following psychological intervention with psychosis (Haddock et al., 1999). Scores for each subscale range 0–4, with a total score range of 0–44. In this study, the distress amount and disruption items were used as dependent variables.
Statistical analysis
Two sets of independent variables were selected for the study to investigate the relative contributions of variables from two differing models. The first set of independent variables was based on the cognitive models of voice-hearing distress and disability: appraisals of voice omnipotence and of voice’s intentions to harm or help (malevolence and benevolence), and levels of use of thought-control strategies. The second set of independent variables was from the Psychological Flexibility Model: levels of psychological flexibility, mindful action, and nonjudgemental acceptance.
The dependent variables for the study were anxiety and depression symptoms, distress and disability associated with voice hearing, and emotional responses and behavioural efforts to resist/engage with voices.
Statistical analyses were conducted using SPSS version 18.0 for Windows. Preliminary analyses of the data distribution were performed: this showed that several variables were not normally distributed (PSYRATS distress amount and disruption and BAVQ-R malevolence, benevolence, and behavioural/emotional resistance, and engagement).
Correlations were calculated to test the hypotheses regarding relationships between variables (Pearson’s correlations for normally distributed variables; Spearman’s rho otherwise) and to clarify the independent variables to be included in hierarchical regression analyses. Hierarchical regression analyses were then conducted to test whether significant increases in explained variance resulted from including psychological flexibility, mindful action, and nonjudgemental acceptance in combination with predictors from cognitive models. For the non-normally distributed dependent variables, logistic regressions (Forward Wald) were conducted.
Results
Descriptive statistics
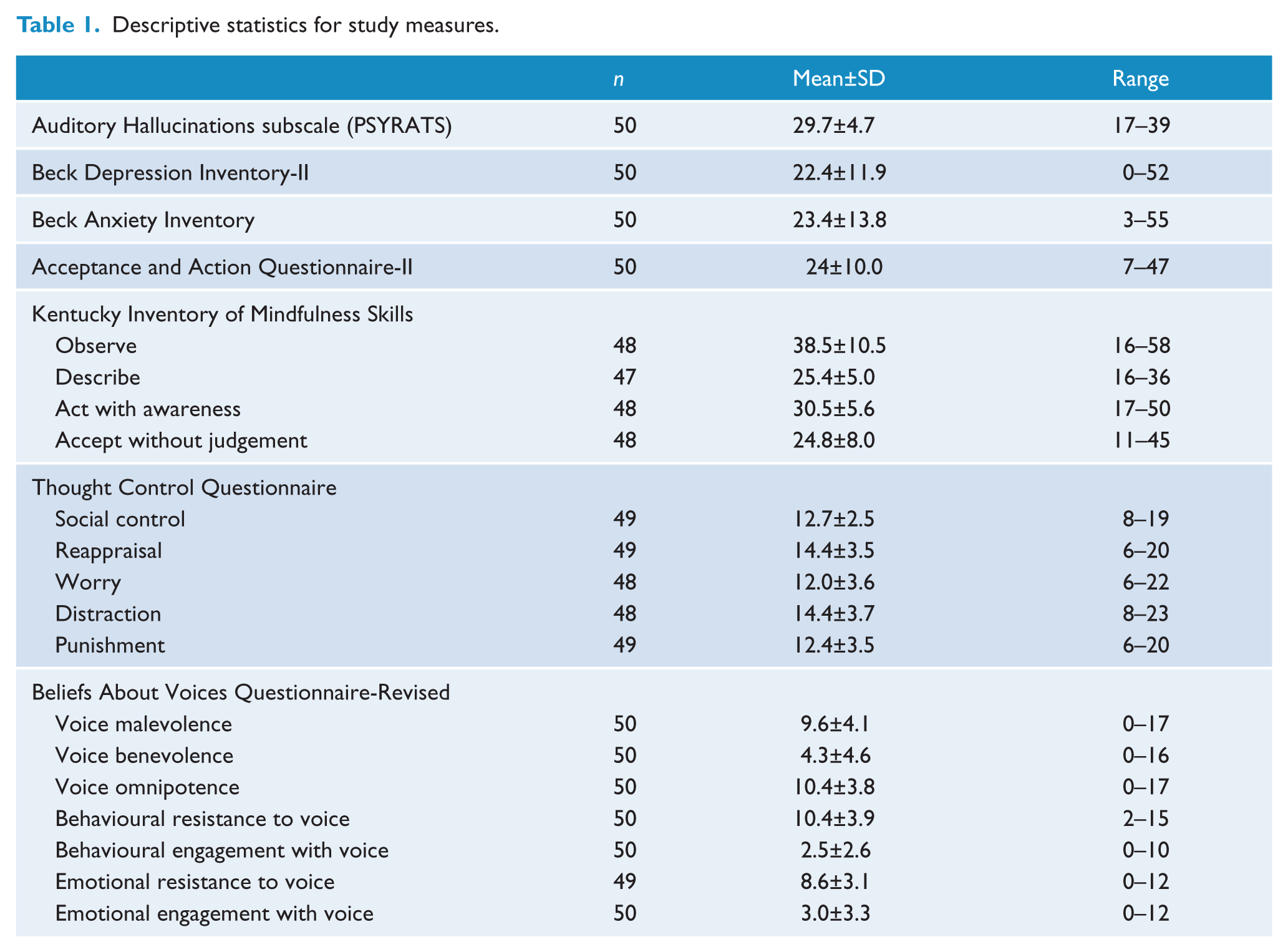
Table 1 shows the descriptive statistics for the study measures. This sample showed equivalent levels of symptomatology (depression, anxiety, voice dimensions), experiential avoidance, endorsement of voice appraisals, and thought-control strategies to previous samples of distressed voice hearers and those with psychosis (Gilbert et al., 2001; Haddock et al., 1999; Morrison and Wells, 2000; Valiente et al., 2011). Mindfulness skills of acting with awareness and nonjudgemental acceptance were of a similar level to both psychosis (White et al., 2011) and other clinical samples (Baum et al., 2010).
Descriptive statistics for study measures.
Internal consistency of the AAQ-II and the KIMS accept without judgement and acting with awareness subscales
Both the AAQ-II and the accept without judgement subscale (KIMS) demonstrated good internal consistency, with Cronbach’s alphas of 0.83 and .85 respectively. In contrast, the acting with awareness subscale (KIMS) demonstrated poor internal consistency (Cronbach’s alpha 0.59) and, as a result, was dropped from subsequent analyses.
Correlations with voice-hearing dimensions
In order to examine question 1, the relationships between psychological flexibility, mindful action, nonjudgemental acceptance, appraisals of voices, coping strategies, and voice distress and disability, and correlations (Pearson’s and Spearman’s rho) were investigated (Table 2).
Intercorrelations among study variables.
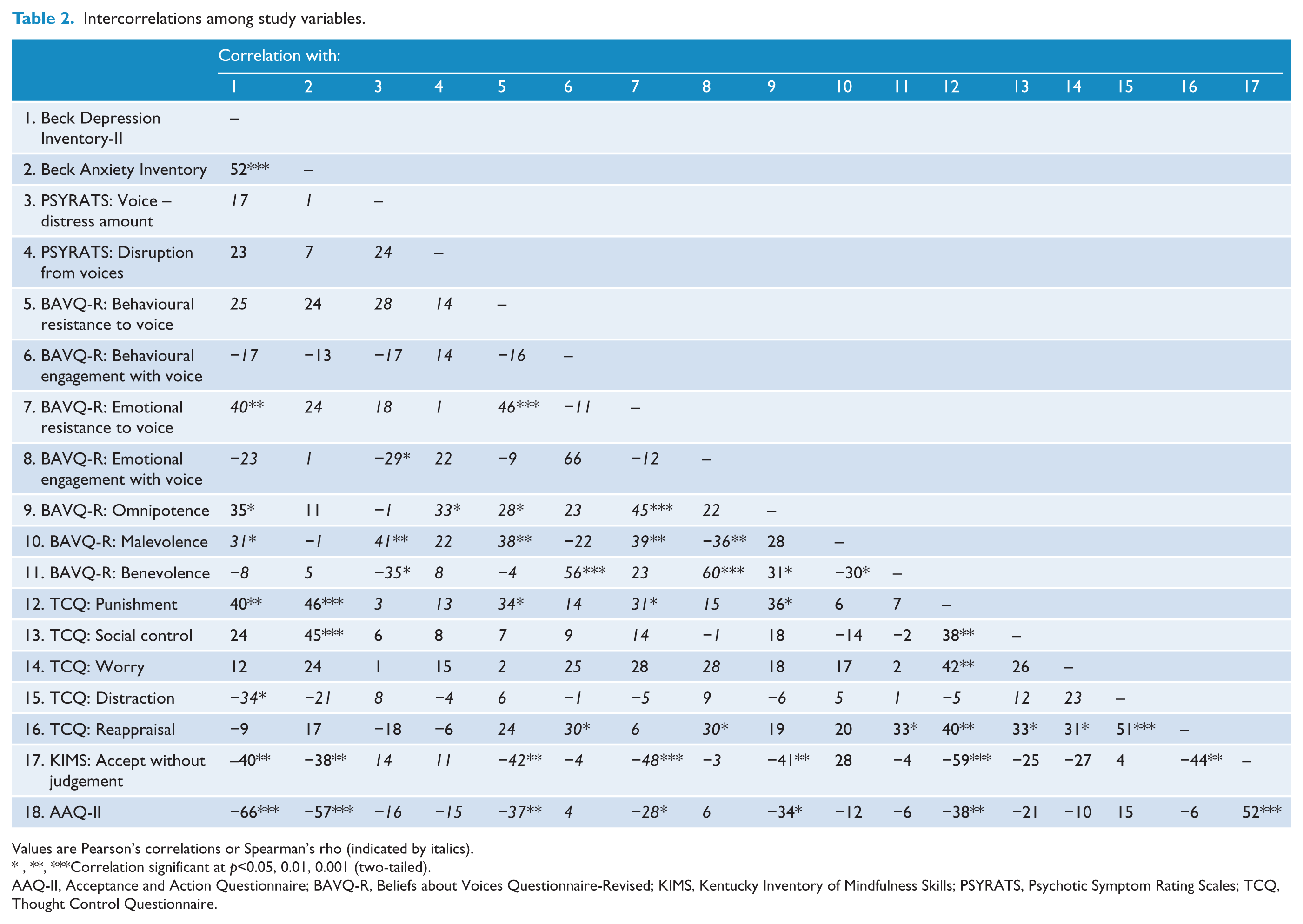
Values are Pearson’s correlations or Spearman’s rho (indicated by italics).
Correlation significant at p<0.05, 0.01, 0.001 (two-tailed).
AAQ-II, Acceptance and Action Questionnaire; BAVQ-R, Beliefs about Voices Questionnaire-Revised; KIMS, Kentucky Inventory of Mindfulness Skills; PSYRATS, Psychotic Symptom Rating Scales; TCQ, Thought Control Questionnaire.
Psychological flexibility and mindfulness with dependent/independent variables
As can be seen in Table 2, we found statistically significant, negative associations between psychological flexibility and nonjudgemental acceptance and appraisals of omnipotence, use of punishment thought control, level of depressive and anxiety symptoms, and actions and emotions focused on resisting the voices. Nonjudgemental acceptance was also found to be negatively associated with the use of reappraisal as a thought-control strategy. However, there were no relationships between psychological flexibility/nonjudgemental acceptance and distress and disruption from voices or with emotional and behavioural engagement with voices.
Dependent variables with appraisals and thought-control strategies
Table 2 also shows that there were significant positive associations for depressive symptoms (BDI-II), appraisals of voice omnipotence and malevolence (BAVQ-R), and punishment thought control (TCQ); there was also a negative relationship with the use of distraction. Anxiety symptoms (BAI) had highly significant positive associations with punishment thought control, as well as social control, but not with voice appraisals.
There were a smaller number of significant associations for the PSYRATS amount of distress caused by voices, with a positive correlation with malevolence appraisals and a negative association with appraisals of voice benevolence. The PSYRATS disruption subscale demonstrated only one significant relationship, with appraisals of voice omnipotence.
Behavioural and emotional engagement variables both had significant positive associations with appraisals of voice benevolence and use of reappraisal thought control; emotional engagement was also negatively associated with malevolence appraisals.
Finally, emotional and behavioural resistance to voices both demonstrated significant positive relationships with appraisals of voice omnipotence and malevolence, as well as use of punishment thought control.
Regression analyses
Multicollinearity of the independent variables was tested by running collinearity diagnostics within the regression analyses on SPSS; the tolerance and variance inflation factors for all variables did not suggest multi-collinearity (all scores: tolerance > 0.2; variance inflation <10).
In order to test hypothesis 2, hierarchical regression analyses were conducted to assess the variance accounted for on the dependent variables of depressive symptoms (BDI-II) and anxiety symptoms (BAI). These regressions included step-1 predictors based on cognitive models for auditory hallucinations and then added psychological flexibility and nonjudgemental acceptance. Independent variables were only selected for step 1 if they correlated significantly with the dependent variables (Table 2).
Forward Wald analyses were conducted for behavioural resistance (BAVQ-R), voice-related distress (PSYRATS), and disruption (PSYRATS); the significant cognitive independent variables were entered stepwise in step 1 and psychological flexibility and nonjudgemental acceptance in step 2. In order to conduct these analyses we created dichotomous variables using a median split for behavioural resistance, behavioural engagement, emotional resistance, emotional engagement, voice related distress, and disruption. For most variables there was an even split between high and low groups, apart from on PSYRATS distress and disruption, where scores 0–2 for PSYRATS distress amount were classed as “low distress” (28% of sample), with 3–4 “high distress” (72% of sample), and PSYRATS disruption scores 0–2 were classed as “low disruption” (68% of sample), with 3–4 “high disruption” (32% of sample).
Table 3 shows the regression analyses for the dependent variables of BDI-II and BAI, and Table 4 shows the logistic regression analyses for behavioural resistance/engagement to voices, emotional resistance/engagement, voice distress, and disruption due to voice hearing. As can be seen, models that incorporated psychological flexibility and nonjudgemental acceptance resulted in a greater proportion of the variance explained for depressive and anxiety symptoms and for behavioural and emotional resistance to voices than models including only predictors based on cognitive models of distressed voice hearing (appraisals of voices intentionality and power, thought-control strategies). As would be expected from the pattern of correlations, models of distress associated with voice hearing, life disruption, and the emotions and actions of engaging with voices did not benefit from the inclusion of psychological flexibility and nonjudgemental acceptance.
Hierarchical multiple regression analysis of study dependent variables.
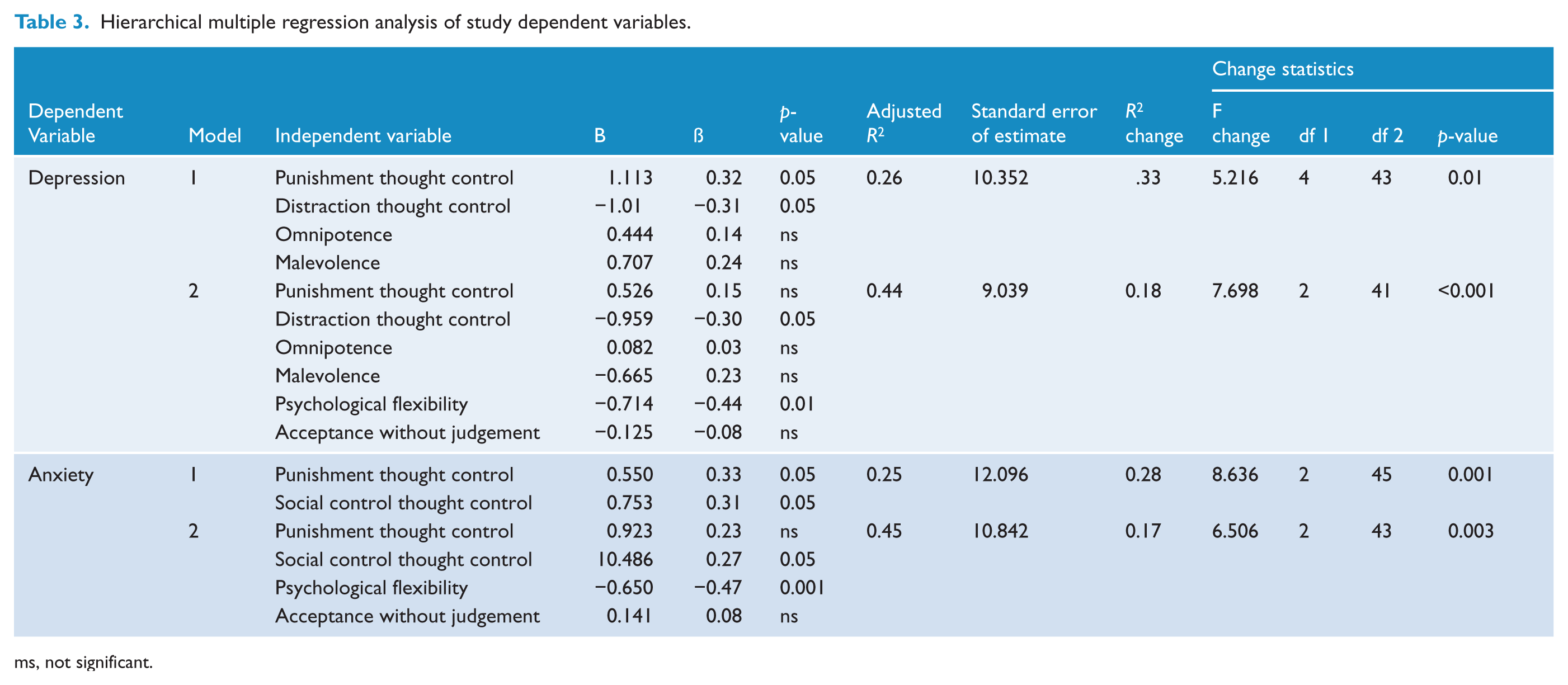
ms, not significant.
Forward Wald logistic regressions for study dependent variables.
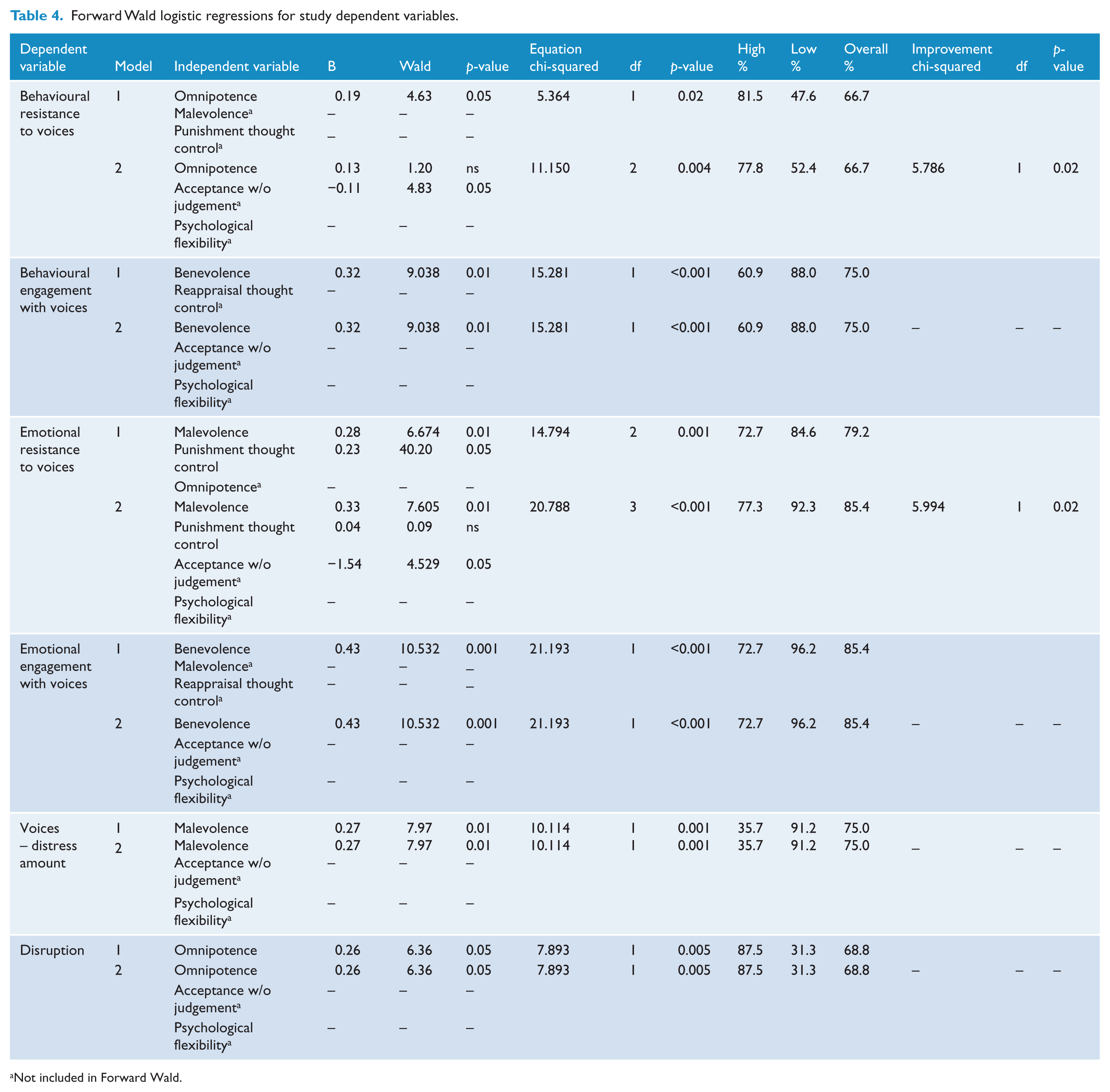
Not included in Forward Wald.
Finally, there were differential contributions between the two measures of acceptance: KIMS acceptance without judgement contributed to the prediction of behavioural and emotional resistance to voices, while AAQ-II contributed to the prediction of depressive and anxiety symptoms.
Discussion
The results of this study suggest that naturally occurring skills of psychological flexibility and nonjudgemental acceptance, as reported by voice hearers, are related to several important outcomes in voice hearing. Psychological flexibility and nonjudgemental acceptance were associated with levels of depressive and anxiety symptoms as well as emotional and behavioural responses to resist voices and they explained additional variance to variables identified in cognitive models (appraisals and thought-control methods).
However, the study predictions of significant relationships with voice-related distress and life disruption were not supported. For these outcomes, appraisals of voice intention (malevolence, in the case of voice-related distress) or power (for disruption) were found to be the only significant independent variables in the regression-based models. These results suggest that psychological flexibility (as measured by the AAQ-II) may have a role in general emotional outcomes for people who hear distressing voices but not in the specific processes that result in the amount of distress caused by voices or the disruption associated with this experience, which are better explained by variables identified in cognitive models. It is possible that a general population-based measure like the AAQ-II (Bond et al., 2011) does not have the symptom-specificity to adequately measure psychological flexibility for voice hearing; however, subsequent scales developed for auditory hallucinations, such as the Voices Acceptance and Action Scale (VAAS) have also failed to find an association between psychological flexibility and dimensions of voice hearing (Shawyer et al., 2007).
There were differential patterns of relationships for the two measures of acceptance. Consistent with studies in nonpsychosis samples, there was a strong negative association between psychological flexibility (AAQ-II) and both depression and anxiety (Bond et al., 2011). This is in line with findings of a strong relationship between experiential avoidance and depression (Hayes et al., 1996), and to behavioural models that posit a central role for avoidance in depression maintenance (e.g. Ferster, 1973). Considering that previous research has suggested that depression is associated with increased disability and morbidity for distressed voice hearers (Birchwood and Chadwick, 1997; Birchwood et al., 2005), these results provide further support for the association between experiential avoidance and depression in psychosis (White et al., 2011).
Nonjudgemental acceptance (KIMS) was found to be negatively associated to efforts to resist voices and emotions related to resistance; a similar finding to the study by Chadwick et al. (2007) that investigated mindfulness and beliefs about voices. There have been inconsistent findings on the relationship between resistance, nonjudgemental acceptance, and emotional distress: Chadwick et al. (2000) and Peters et al. (2012) found that resistance was positively associated with depression, while no such relationship was found by Shawyer et al. (2007). In this study, by dividing the emotional from the behavioural resistance BAVQ-R items, it was found that emotional resistance was significantly associated with depression severity, while behavioural resistance had no association (nor indeed with the other dependent variables anxiety, voice-related distress, or disruption). One possible explanation is that the emotional resistance items of the BAVQ-R may reflect general distress and that this may account for the previously reported high associations with depression and for the relationships with nonjudgmental acceptance and psychological flexibility in this study. For this sample, the behavioural resistance items may potentially be measuring strategic or functional actions toward voices (for instance, refusing to comply with command hallucinations) and hence are unrelated to negative outcomes, but still negatively associated with nonjudgemental acceptance/psychological flexibility: efforts to resist voices imply a judgemental stance toward these experiences.
Psychological flexibility and, more significantly, nonjudgemental acceptance, showed negative associations with appraisals of voice omnipotence, while no relationships were found with appraisals of voice intention (malevolence or benevolence). These findings are similar to the correlations reported by Shawyer et al. (2007) using the VAAS, and suggest that accepting experiences without engaging in judgement is related to a reduced chance of appraising voices as omnipotent. This association fits with the psychological flexibility model, in that believing a voice is omnipotent implies greater cognitive fusion, where experiences are responded to in a literal manner (so that a person may respond to a perceived powerful other in subordinate ways (Gilbert et al., 2001); regarding a voice as powerful is antithetical to nonjudgemental experience. Due to the cross-sectional design of this study the direction of causality is unclear: appraising voices as omnipotent may possibly also increase judgements about other experiences. A potential inconsistency with this theoretical perspective is the lack of an association found with appraisals of voice intention (which are also judgements about experience). Chadwick et al. (2007) reported a negative association between a measure of mindfulness of voices and appraisals of malevolence; it may be in the current study that a general measure of nonjudgemental acceptance did not adequately assess this relationship or that beliefs about voice intentions are unrelated to nonjudgement/ psychological flexibility. Finally it could be that the construct of mindfulness in the Chadwick et al. (2007) study is different or has an additional facet to the measures used in this study; an area for further investigation.
Also, contrary to the study predictions, thought-control strategies were not related to voice distress or disruption; however, the use of punishment as thought control was positively related to depression, anxiety, appraisals of omnipotence, emotions, and actions taken to resist voices. Psychological flexibility and nonjudgemental acceptance were related to less use of punishment as a thought-control strategy: again, as the direction of causality cannot be determined, it may be that the use of punishment to manage unwanted thoughts increases judgement and nonacceptance of a range of private experiences. Finally, the use of reappraisal to control thoughts was significantly inversely related to nonjudgemental acceptance; this could be argued to fit with the conceptualization of acceptance that reduces the necessity to reappraise experiences to live effectively. The finding that acceptance was significantly related to emotional outcomes, while the use of reappraisal was not, is in line with this potential explanation.
Limitations
As described earlier, the cross-sectional study design limits the conclusions that can be made regarding causality and directionality between the study variables.
This study utilized a sample of distressed voice hearers, and so conclusions cannot be drawn about the relationships of the study variables for people who find voice hearing a pleasant or neutral experience. The sample was skewed toward those with greater levels of life disruption (measured by the PSYRATS): only a small number of participants engaged with the voices, through action and emotion. Thus, we may not have been able to explore adequately the relationships of psychological flexibility and nonjudgemental acceptance for those who find their voices engaging and/ or benevolent but nevertheless are disabled by this experience.
There were also several limitations related to the study measures. First, analyses of the KIMS Acting with Awareness subscale were curtailed, due to the poor internal consistency of the scale. This subscale has been found to have acceptable internal consistency with other samples (Baer et al., 2004), including nonpsychosis clinical groups (Baum et al., 2010). A possibility is that the subscale items do not adequately measure this construct in psychosis samples; studies by Oliver et al. (2012) and White et al. (2011) have found that this subscale does not contribute significantly to study predictions or change significantly following intervention.
Second, measures of functioning/disruption need to be more fine-grained to capture the potential costs and benefits of coping with voices. In this study, measuring disruption associated with voice hearing was unsatisfactory, as the PSYRATS uses a 5-point scale that measures functioning by whether the participant is in supported accommodation or hospitalized. In the study sample, a minority of participants scored poorly on this item, resulting in a restricted range of scores (most participants were recruited from community settings and living in independent accommodation). Using an overall score for life disruption can obscure how voice hearing may interfere differentially in various life domains (such as concentration/attention, relating to others, self-care, pursuing personal goals). A similar challenge was found with the PSYRATS voice-related distress measure (amount of distress scale): recruiting a sample of distressed voice hearers meant that there was a restricted range of scores (basically the two highest ratings). In retrospect, it may have been better to use an alternative measure that allowed for a greater range of ratings for levels of distress associated with voices, such as the personal questionnaire approach used by Peters et al. (2012) or the alternatives to the PSYRATS reviewed by Ratcliff et al. (2011).
Clinical implications
Broadly, the results of this study provide evidence that psychological flexibility may be helpful for emotional problems in psychosis, while distress or disruption associated with voices specifically may be better explained by cognitive models. The findings suggest that the ability to “step back” from evocative private experiences is associated with voice hearers’ experiencing less depression and anxiety and engaging in fewer efforts to resist voices. It may therefore be useful to incorporate psychological flexibility and nonjudgemental awareness in clinical models of emotional distress for voice hearers as potential resilience factors. One advantage of adding these processes is that clear intervention strategies are suggested by their inclusion: mindfulness and acceptance, such as featured in the treatment approaches described by Chadwick (2006; person-based cognitive therapy) and Bach et al. (2006; acceptance and commitment therapy). Theoretically, a contextual shift is developed from a narrow repertoire of avoidance- and escape-focused actions that are negatively reinforced and maintain distress to approach behaviours that potentially result in access to a wider range of reinforcers, both directly contacted and abstractly derived, resulting in greater life meaning and vitality, even with ongoing contact with unwanted experiences (Wilson and Murrell, 2004).
Conclusions
This study provides further empirical support for the observed relationship of psychological flexibility and nonjudgemental acceptance with depression and anxiety symptoms, found in other clinical samples, and similarly in this sample of distressed voice hearers. Furthermore. this study suggests that these psychological flexibility and mindfulness variables provide an additional explanation of behavioural and emotional resistance responses to voices, beyond the role of the cognitive variables outlined in current models. However, these relationships did not extend to accounting for emotional and behavioural engagement with voices, or voice-related distress and life disruption, which were explained solely by cognitive variables, suggesting that cognitive models contribute to our understanding of these aspects of voice hearing.
Footnotes
Funding
The study was supported in part by the Trustees of the South London and Maudsley NHS Trust Health Services Research Centre (small grant; HSRC Application 06/2006-07).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.