
Abstract
Background:
The highest prevalence of mental health problems is amongst people aged 18–24, with anxiety disorders and depression the most common disorders in this age group. Few young adults seek and receive effective care, prompting calls for the development of ‘youth friendly’ services. The Internet is a modality that has the potential to facilitate engagement with, and delivery of psychological treatments to, young adults. To date, however, no therapist-guided Internet-delivered treatments have been developed specifically for young adults experiencing depression and anxiety.
Aims:
To examine the efficacy and acceptability of a new therapist-guided Internet-delivered treatment for young adults aged 18–24 with symptoms of depression and anxiety.
Method:
Participants accessed the Mood Mechanic Course, which consisted of four lessons delivered over 5 weeks. Measures of depression, anxiety, distress and disability were gathered before and after treatment, and at 3-month follow-up. Results were provided by 78% and 83% of participants at post-treatment and 3-month follow-up, respectively. Data were analysed using mixed linear model analyses. The trial was registered as: ACTRN12612001099819.
Results:
Treatment significantly reduced depression and anxiety symptom severity, disability and distress at post-treatment and 3-month follow-up. Large within-group effect sizes were found at post-treatment and 3-month follow-up on all measures using both completer and estimated marginal means (Cohen’s d = 1.02 to 1.41 and 0.94 to 1.45, respectively). The therapist spent an average of 37 minutes (SD = 18 minutes) in contact with participants during treatment. Participants rated the treatment as acceptable.
Conclusions:
Treatment gains recorded at post-treatment were sustained at 3-month follow-up, and were consistent with those reported in meta-analyses of Internet-delivered treatments developed for the broader adult population with depression and anxiety. These results provide encouraging preliminary evidence for the efficacy of therapist-guided Internet-delivered treatments for anxiety and depression tailored for young adults.
Introduction
The 12-month prevalence rates of disorders of depression and anxiety in Australian adults aged 18–24 years are 6% and 15%, respectively (Australian Bureau of Statistics, 2009). If left untreated, symptoms of anxiety and depression during young adulthood increase the likelihood of chronic mental health difficulties in later life and are associated with poorer workforce participation, income and living standards by age 30 (Gibb et al., 2010; Shankman et al., 2009). Unfortunately, treatment seeking amongst young adults is considerably lower than for other adult age groups (McDermott et al., 2010). Young adults experience similar barriers to treatment as those experienced by older adults, including the direct and indirect costs of treatment, geographic distance to appropriate services, and public and self-stigma surrounding mental health (Collins et al., 2004; Corrigan and Rüsch, 2002; Olfson et al., 2000). However, additional barriers characteristic of young adults include lack of trust in service providers, negative previous experiences, and a lack of health professionals trained in working with young adults (Rickwood et al., 2007; Silk, 2005). This has led to calls for the development of ‘youth friendly’ services (McDermott et al., 2010; Silk, 2005).
Internet- and computer-delivered information services and treatments are increasingly used to facilitate access by young adults to effective care (Rickwood et al., 2007). Internet-delivered cognitive behavioural therapy (iCBT) programs use the same principles and components of traditional face-to-face treatment, but are administered via a computer and the Internet. Meta-analytic studies indicate that these treatments are effective for adults with anxiety and depression, are acceptable to consumers, and result in similar outcomes to face-to-face delivered treatment (Andersson et al., 2005; Andrews et al., 2010; Cuijpers et al., 2009; Spek et al., 2006). Researchers have begun to explore the efficacy of such interventions with younger adults. For example, one randomized controlled trial (RCT) examined a 32-week purely self-guided iCBT intervention for 160 adults aged 18–24 with depression and found significant, but small (e.g. Cohen’s d = 0.20), improvements in depression symptoms when compared with treatment as usual (Clarke et al., 2009). Another RCT examined a therapist-guided iCBT program, provided with and without group face-to-face exposure sessions, amongst 38 university students with social anxiety and found that treatment reduced the severity of social phobia symptoms (Cohen’s d = 0.82 to 1.31) (Tillfors et al., 2008).
The present study examined the preliminary efficacy, acceptability and feasibility of a new transdiagnostic iCBT intervention, the Mood Mechanic Course, for younger adults aged between 18 and 24 with symptoms of depression and anxiety. Transdiagnostic treatments target core symptoms of both anxiety and depression simultaneously (Andersson et al., 2011; Carlbring et al., 2011; Dear et al., 2011a; Johnston et al., 2011, 2013; Titov et al., 2011) and thus offer numerous advantages to both patients and therapists, including addressing the high levels of comorbidity between and within anxiety and depressive disorders. The Mood Mechanic Course is a brief four-lesson course delivered over 5 weeks with weekly contact from a psychologist via email and telephone. In order to gain preliminary data about the likely magnitude of clinical benefit which would inform the design of a subsequent RCT, the current study employed a single-group open-trial design. It was hypothesized that: (1) participants would show statistically significant improvements on measures of anxiety, depression and disability; (2) these changes would be reflected in clinically significant improvements on measures of depression and anxiety; and (3) participants would rate the treatment as acceptable.
Method
Participants
Interested people applied to participate in the study through a clinical research website, www.ecentreclinic.org, which provides information about common mental health difficulties and the opportunity to participate in research evaluating new online treatments. The inclusion criteria for the current study were that all participants: (i) were aged 18–24 years; (ii) were residing in Australia; (iii) had access to the Internet; (iv) were not currently experiencing a psychotic illness or severe symptoms of depression (defined as a total score ≥23 or responding with a score ≥3 to item 9 of the Patient Health Questionnaire 9-item) (Kroenke et al., 2001); (v) were not currently completing CBT treatment elsewhere; and (vi) were experiencing at least mild symptoms of depression or anxiety (i.e. defined as a total score ≥5 on either the Patient Health Questionnaire 9-item (Kroenke et al., 2001) or Generalized Anxiety Disorder 7-item scale) (Spitzer et al., 2006).
Fifty-six people applied for the study, 30 of whom were contacted via telephone to confirm they met the inclusion criteria – at which time they were administered the Mini Neuropsychiatric Interview, Version 5 (MINI) (Sheehan et al., 1998). Twenty participants met all inclusion criteria and were allocated to the Treatment Group. Two participants withdrew their participation before treatment began, resulting in a sample of 18 participants. Details of the participant flow are shown in Figure 1.
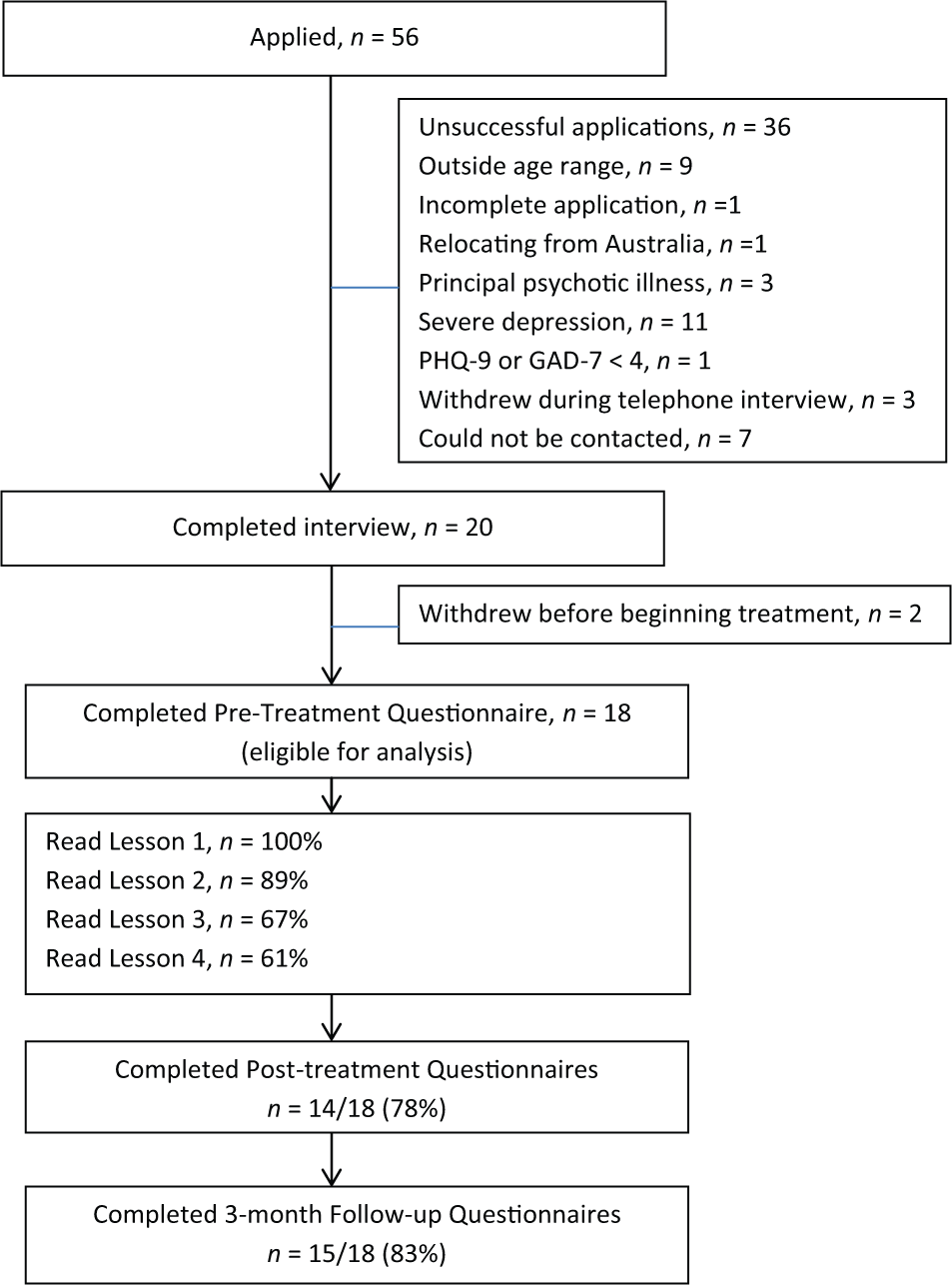
Participant flow.
The resulting sample had a mean age of 20.61 years (SD = 1.98; range = 18 to 24) and 14/18 (78%) were female. Three of 18 (17%) were married or were in a de facto relationship, while the remaining 15/18 were single or had never been married. Two of 18 (11%) were in full-time work, 3/18 (17%) part-time employment, 11/18 (61%) were full-time students, 1/18 (6%) was a part-time student and 1/18 (6%) was unemployed. Four of 18 (22%) reported that their highest level of educational attainment was Year 10, 8/18 (45%) reported it was Year 12, 2/18 reported having completed a trade or technical certificate, and 4/18 (22%) had completed a university level diploma or degree. Eleven of 18 (61%) reported some form of previous mental health treatment and 3/18 (17%) reported taking medication for their mental health. In addition, 5/18 (28%) met diagnostic criteria for a principal diagnosis of a major depressive episode, 4/18 (22%) met criteria for social phobia, 1/18 (5%) met criteria for panic disorder with agoraphobia, 5/18 (28%) met criteria for generalized anxiety disorder, while 3/18 (17%) did not meet criteria for depression or an anxiety disorder. Twelve of the 13 (92%) participants meeting criteria for one mental disorder also met criteria for a comorbid major depressive episode or anxiety disorder.
The study was approved by the Human Research Ethics Committee of Macquarie University (Sydney, Australia) and the trial was registered as ACTRN12612001099819.
Design and measures
A single-group open trial design was employed for the present study. Participants completed questionnaires immediately prior to beginning the course (i.e. pre-treatment), immediately after finishing the 5-week course (i.e. post-treatment) and again 3 months after the course finished (i.e. 3-month follow-up). The following questionnaires were administered online using secure login via the research website.
Mini International Neuropsychiatric Interview, Version 5.0.0 (MINI) (Sheehan et al., 1998)
The MINI is a brief diagnostic interview developed to determine the presence of current and life-time Axis-I disorders using Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) diagnostic criteria. Psychometric evaluations of the MINI indicate it has excellent inter-rater reliability (k = 0.88 to 1.00) (Lecrubier et al., 1997) and adequate concurrent validity with the Composite International Diagnostic Interview (World Health Organization, 1990).
Patient Health Questionnaire 9-item (PHQ-9) (Kroenke et al., 2001)
The PHQ-9 is a nine-item measure of the symptoms and severity of depression. It is based on DSM-IV criteria and provides a total score ranging from 0 to 27, with higher scores indicating greater symptoms of severity and a total score of 10 identified as predicting a DSM-IV diagnosis of depression (Kroenke et al., 2001). Psychometric studies indicate the internal consistency is high (α range: 0.74 to 0.89) and the measure is sensitive to change (Kroenke et al., 2010). In the present study, Cronbach’s α = 0.79.
Generalized Anxiety Disorder 7-item (GAD-7) (Spitzer et al., 2006)
The GAD-7 measures the symptoms and severity of generalized anxiety disorder (GAD) and is comprised of seven items. The GAD-7 is increasingly used in research and in large-scale dissemination studies as a generic measure of anxiety symptoms (Clark et al., 2009; Richards and Suckling, 2009). Evidence suggests that the GAD-7 is sensitive to DSM-IV congruent GAD, social phobia and panic disorder, and the measure provides scores ranging from 0 to 21, with increasing scores indicating greater severity of symptoms (Löwe et al., 2008). The GAD-7 has good internal consistency (α = 0.79 to 0.91) and good convergent and divergent validity with other anxiety and disability scales (Dear et al., 2011b). In the present study Cronbach’s α = 0.92.
Sheehan Disability Scale (SDS) (Sheehan, 1983)
The SDS is a three-item measure that assesses impairment in psychosocial functioning, with total scores ranging from 0 to 10, whereby higher scores indicate a greater level of disability. The SDS has been used widely in studies examining the efficacy of Internet-delivered treatments (Dear et al., 2011a; Johnston et al., 2011, 2013; Titov et al., 2010a, 2011; Zou et al., 2012), and has high internal consistency (α = 0.89) (Leon et al., 1997). The internal consistency of the measure in the current study, however, was moderate (α = 0.57).
Kessler 10-item (K-10) (Kessler et al., 2002)
The K-10 is a 10-item, non-specific measure of psychological distress, with total scores ranging from 10 to 50, whereby higher scores indicate greater distress. The measure has been used in large epidemiological studies as a measure of psychological distress (Andrews and Slade, 2001) and evidence suggests that it discriminates between community cases and non-cases of anxiety, mood and non-affective psychotic disorders (Kessler et al., 2002). The K-10 has excellent internal consistency (α = 0.92 to 0.93) (Cornelius et al., 2013; Kessler et al., 2002). In the present study Cronbach’s α = 0.88.
Treatment acceptability
Four questions were used to assess treatment acceptability at post-treatment: (1) ‘Overall, how satisfied were you with the course?’; (2) ‘How satisfied were you with the lessons and lesson summaries?’; (3) ‘Would you feel confident in recommending this treatment to a friend?’; and (4) ‘Was it worth your time doing the course?’. Participants responded to the first two questions using a five-point Likert scale, ranging from ‘very satisfied’ to ‘very dissatisfied’. The second two questions required a simple ‘yes’ or ‘no’ response. These questions were included in the present research as they have been used in previous studies examining the acceptability of iCBT treatments amongst consumers of different age groups and with a range of different conditions (Dear et al., 2013; Kirkpatrick et al., 2013; Titov et al., 2013).
Intervention
The intervention, the Mood Mechanic Course, is a new iCBT intervention based on the Wellbeing Course (Dear et al., 2011a), a brief transdiagnostic treatment course developed to treat symptoms of depression and anxiety disorders in adults. Transdiagnostic iCBT interventions have been found to be clinically efficacious and acceptable to people with anxiety and depressive disorders (Johnston et al., 2011; Titov et al., 2010a, 2011). The Mood Mechanic Course comprises four lessons and is delivered over 5 weeks. The number of lessons and the duration of the course was informed by a review of the available literature about computer- and Internet-delivered treatments for adolescents and young adults, which although limited to a small number of studies, indicated that brief interventions were likely to result in higher adherence rates (O’Kearney et al., 2006; Sethi, 2013).
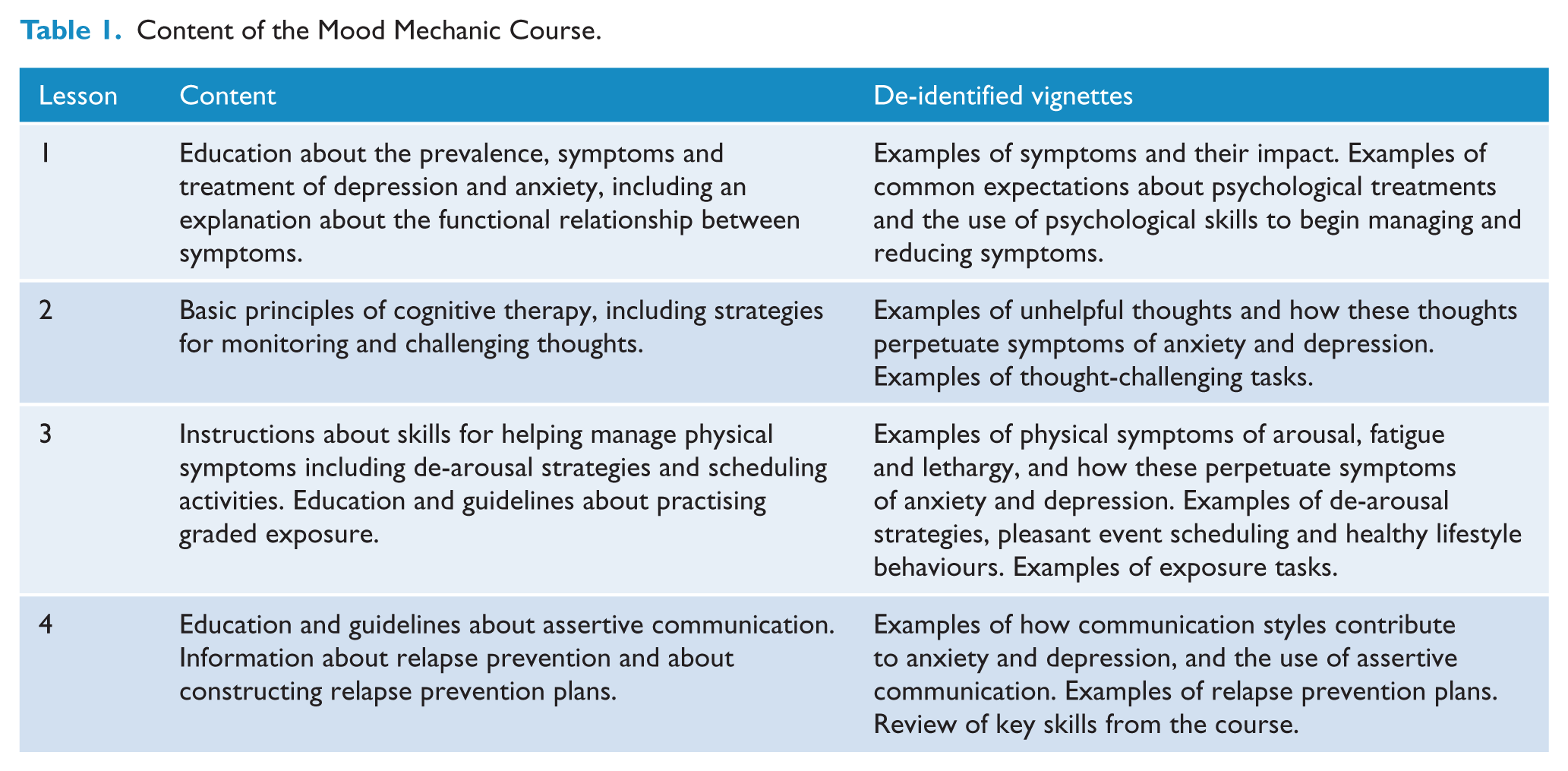
A description of the content of each lesson is provided in Table 1. Each lesson was supplemented with written homework tasks to help participants apply the skills taught in the lesson, and two clinical vignettes which provided further examples of managing symptoms. Participants had access to additional resources about topics that included structured problem-solving, challenging unhelpful beliefs, examples of behavioural activation and graded exposure tasks, techniques for challenging overestimation of risk and underestimation of ability to cope, establishing an effective sleep routine, a list of crisis and emergency services, and answers to frequently asked questions. Treatment materials were tailored for the study population by providing clinical vignettes of adults aged 18–24, using age-appropriate language, and by providing examples of CBT techniques used to manage some difficulties commonly faced by young adults (e.g. managing the demands of tertiary education, leaving the family home, limiting alcohol consumption to manage emotional wellbeing, and balancing workplace and other demands).
Content of the Mood Mechanic Course.
Contact with participants occurred via telephone calls, automatic emails and short message service (SMS). Telephone calls were offered on a once-weekly basis and missed calls were followed up with an email. Automatic emails were authored by the researchers before the treatment began, and were automatically sent to participants to reinforce reading lessons, to remind them of the availability of treatment materials, and to notify them of the release of new materials. All participants were offered the option of receiving SMS reminders three times a week during the course plus once-monthly reminders between post-treatment and the 3-month follow-up. SMS reminders encouraged participants to access the site or to practise skills taught in previous lessons.
One registered psychologist (LJ), experienced in the online treatment of anxiety and depression, provided all clinical contact with participants before, during and after the treatment. All clinical contact was recorded and the therapist was advised to limit weekly contact to approximately 10 minutes, unless otherwise clinically indicated. The therapist aimed to provide the following four components in each interaction with participants: (1) reinforcement of progress; (2) a summary of the key skills in the course; (3) normalizing of difficulties commonly experienced in applying the skills and managing symptoms; and (4) encouragement to continue with the course. The therapist was supervised by BFD with scheduled meetings once a week and on an as-needed basis.
Statistical methods
Mixed linear models analyses with a compound symmetry covariance structure and using maximum likelihood estimation was identified as the best way to handle missing data at post-treatment and follow-up. Within-group effect sizes (Cohen’s d) were calculated based on the pooled standard deviation for the entire sample using both the data of those participants who provided data (i.e. completers) and the estimated marginal means derived from the mixed linear models analyses. As described in recent dissemination studies (Richards and Suckling, 2009), pre-treatment, post-treatment and follow-up PHQ-9 and GAD-7 scores were compared with clinical cut-offs to provide an index of clinically significant remission. This was defined as the proportion of participants who initially scored at or above the clinical cut-offs of 10 on the PHQ-9 and 8 on the GAD-7, and then subsequently below these clinical cut-offs. The first available data (i.e. baseline-observation-carried-forward; BOCF) were carried forward for participants who did not complete post-treatment or follow-up questionnaires to provide a conservative estimate of remission. As described in a recent RCT examining the efficacy of iCBT for depression and anxiety (Titov et al., 2013), deterioration was defined as an increase of five or more points on the PHQ-9 or GAD-7 at post-treatment or follow-up, relative to pre-treatment.
Results
Adherence and attrition
Eleven of 18 participants (61%) completed all lessons during the 5 weeks of the course. Four additional participants logged on to the site and completed all of the lessons after the course had finished, resulting in 15/18 (83%) participants completing all lessons by the 3-month follow-up. Fourteen of 18 (78%) and 15/18 (83%) participants provided post-treatment and 3-month follow-up data, respectively. Details of participant adherence and attrition are presented in Figure 1.
Outcomes and effect sizes
Means and standard deviations are presented in Table 2. The mixed linear models analyses revealed significant main effects for time on all measures: PHQ-9 (F2, 28.56 = 8.02, p < 0.005); GAD-7 (F2, 31.32 = 8.62, p < 0.005); SDS (F2, 34.96 = 9.22, p < 0.005); and K-10 (F2, 27.98 = 16.30, p < 0.005). PHQ-9, GAD-7, SDS and K-10 scores had significantly improved at post-treatment and the 3-month follow-up compared with pre-treatment (all p < 0.005). There were no significant differences, however, on any measures between post-treatment and 3-month follow-up (p > 0.05).
Results of outcome measures for the overall sample: observed and estimated means, standard deviations, confidence intervals and effect sizes (Cohen’s d).
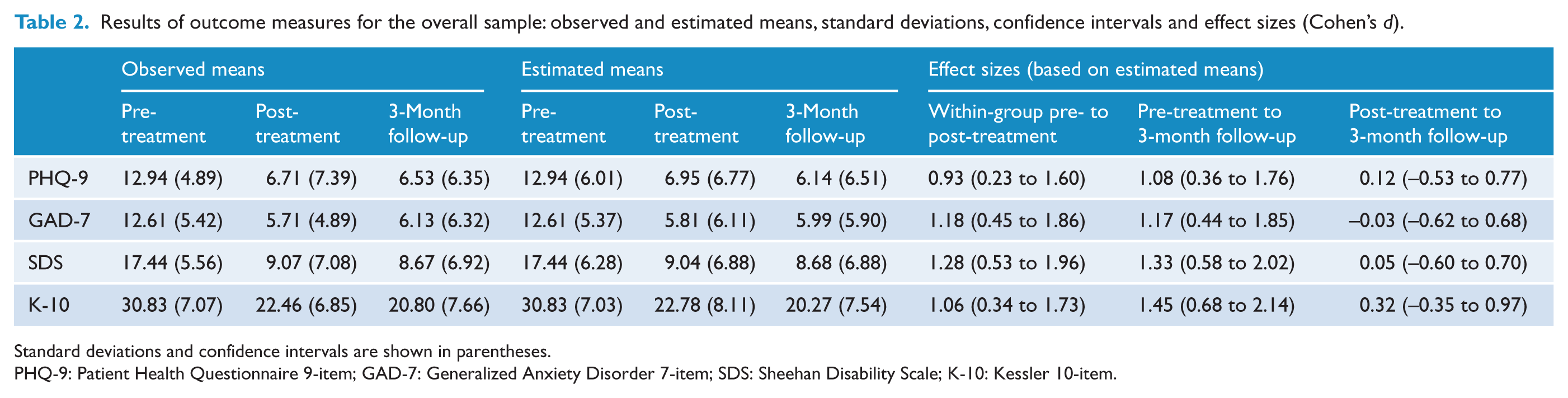
Standard deviations and confidence intervals are shown in parentheses.
PHQ-9: Patient Health Questionnaire 9-item; GAD-7: Generalized Anxiety Disorder 7-item; SDS: Sheehan Disability Scale; K-10: Kessler 10-item.
Within-group effect sizes for the outcome measures are included in Table 2. Large pre-treatment to post-treatment and pre-treatment to 3-month follow-up effect sizes were found on all measures, using both completer and estimated marginal means (completers: d = 1.02 to 1.41; estimated marginal means: d = 0.94 to 1.45).
Clinical significance
Rates of clinically significant remission and recovery on the PHQ-9 and GAD-7 are reported in Table 3. For the PHQ-9, 5/14 (35.71%) and 3/14 (21.43%) participants who scored above the cut-off at pre-treatment remained above this cut-off at post-treatment and the 3-month follow-up. Eleven of 18 (61.11%) participants made a 50% or greater improvement on the PHQ-9 at post-treatment and 3-month follow-up. For the GAD-7, 7/13 (53.85%) and 4/13 (30.77%) participants who scored above the cut-off at pre-treatment remained above this cut-off at post-treatment and 3-month follow-up. Nine of 18 (50.00%) and 10/18 (55.56%) participants made a 50% or greater improvement on the GAD-7 at post-treatment and 3-month follow-up, respectively.
Proportion of participants above cut-off scores of clinical significance (remission) and proportion demonstrating at least a 50% reduction in pre-treatment scores (recovery).
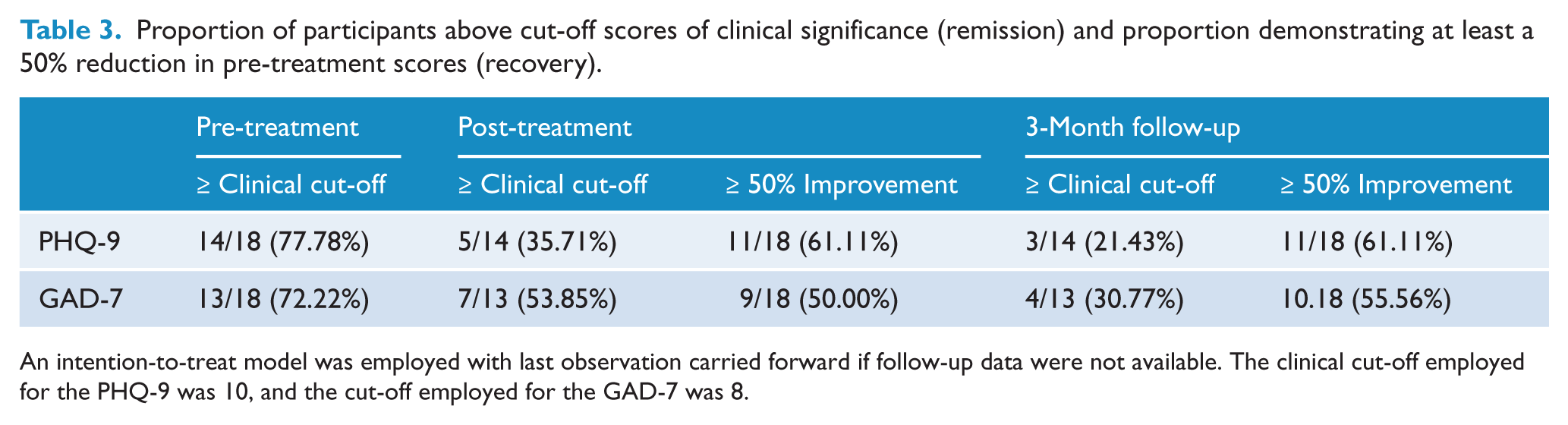
An intention-to-treat model was employed with last observation carried forward if follow-up data were not available. The clinical cut-off employed for the PHQ-9 was 10, and the cut-off employed for the GAD-7 was 8.
Deterioration
One of 18 participants (5.5%) deteriorated ≥5 on both the PHQ-9 and GAD-7 at post-treatment. No participants deteriorated by ≥5 on either measure at the 3-month follow-up.
Contact
The mean total time of therapist contact per participant was 18.50 minutes (SD = 18.07; range = 15 to 90), including sending and reading emails, and telephoning participants. An additional average 22.4 minutes (SD = 8.5; range = 13 to 37) per participant was required for administrative purposes, including time required to conduct the diagnostic telephone interviews. Participants were sent an average of 3.34 emails (SD = 1.25; range = 2 to 6) during the course. The therapist also made an average of 5.2 telephone calls (SD = 0.43; range = 5 to 6) per participant.
Acceptability
Thirteen of 18 (72%) participants provided treatment satisfaction data. Of these participants, 11/13 (85%) reported they were either very satisfied or mostly satisfied with the course, while two participants (15%) reported a neutral level of satisfaction. Twelve of 13 (92%) reported that they were either very satisfied or mostly satisfied with the quality of the lessons and DIY guides, while one participant (8%) reported a neutral level of satisfaction. All 13 (100%) participants who provided treatment satisfaction data reported ‘it was worth their time doing the course’ and that they ‘would recommend the course to a friend’.
Discussion
The primary aims of the present study were to examine the preliminary efficacy, acceptability and feasibility of the Mood Mechanic Course, a brief and therapist-guided iCBT intervention for symptoms of anxiety and depression amongst younger adults aged 18–24. The three hypotheses, that (1) participants would show statistically significant improvements on measures of anxiety, depression and disability; (2) these changes would be reflected in clinically significant improvements on measures of depression and anxiety; and (3) participants would rate the treatment as acceptable, were supported. Large within-group effect sizes were found on the PHQ-9 and GAD-7, which corresponded to statistically and clinically significant reductions in symptoms. These results were maintained at the 3-month follow-up and participant satisfaction with the course was also high.
The results are consistent with meta-analytic studies evaluating Internet-delivered treatments for adults generally (Andersson and Cuijpers, 2009; Andrews et al., 2010) and specific reports of Internet-delivered transdiagnostic treatments for adults with anxiety and depression (Dear et al., 2011a; Johnston et al., 2011, 2013; Titov et al., 2010a, 2011). These results are also consistent with the few existing studies examining Internet-delivered treatments specifically developed for younger adults; that is, adults less than 25 years of age (Clarke et al., 2009; Tillfors et al., 2008). Lastly, the results are consistent with studies concerning the efficacy of traditional face-to-face treatments for young adults (Lindgren et al., 2010; Piet et al., 2010). However, the improvements in symptoms observed in the current study were obtained with an average of 37 minutes (SD = 18 minutes) of contact time per participant, considerably less than usually required in face-to-face treatment. Reduced therapist demands is a common feature of Internet treatments (Spek et al., 2006) and is achieved by designing the interventions to automatically and systematically teach the core information and skills, thus saving therapist time, which allows the therapist to focus on supporting the patient to apply the content of the intervention to their own circumstances (Dear et al., 2011a).
While consistent with the findings of the broader research, the present study extends the existing literature in several important ways. First, it is one of a few studies to examine the efficacy, acceptability and feasibility of Internet treatments with younger adults, who are at ages when many mental health difficulties are known to have their onset (McDermott et al., 2010) and yet are less likely to engage with traditional treatment services (Reavley et al., 2010). Second, the present study indicates that younger adults may also respond to transdiagnostic approaches to treatment, which aim to simultaneously target related clusters of symptoms (Johnston et al., 2011), but which have not been evaluated with younger adults. This is encouraging given the high levels of comorbidity between the anxiety and depressive disorders (Australian Bureau of Statistics, 2009) and the challenges of administering disorder-specific treatments (Clark, 2009). Finally, the present study managed to achieve statistically and clinically significant improvements in symptoms, despite using a brief treatment with relatively little therapist time per participant.
Despite these strengths, there are a number of important limitations that need to be considered when interpreting the findings of the present study. First, the present study employed a single-group open trial design, which does not control for spontaneous remission of symptoms or allow comparison with other treatments. Thus, although the results of the present study are encouraging, future studies involving comparison groups are needed to establish the clinical efficacy of this treatment for younger adults. Second, the present study only examined general symptoms of anxiety and depression, rather than specific symptoms (e.g. panic symptoms, social anxiety symptoms), and no formal diagnostic interviews were conducted at follow-up. Consequently, the efficacy of the treatment for specific symptom clusters is less clear. In addition, while appropriate for a proof-of-concept study, the sample in the current study was small and only a short-term follow-up was conducted. Third, it is unclear what might have led to the lower than expected completion rates at the end of treatment (i.e. 67%), as the acceptability of the course was endorsed by most participants. It is noteworthy that, despite this completion rate, the post-treatment gains were consistent with those reported in the literature for iCBT programs for a broader adult population (Andersson et al., 2011; Johnston et al., 2011; Titov et al., 2011), as were completion rates at the 3-month follow-up (i.e. 83%). This pattern raises potential questions about the optimal length of treatment and support required for young adults and about how young adults engage with online services compared with older adults. However, being a small feasibility study, it is also important to be cautious in over-interpreting these findings until further, larger, trials are conducted. Finally, the present study employed therapist-guidance, which limits the potential implementation of the Mood Mechanic Course, particularly for young people who do not wish to speak to a health professional. Several recent studies of self-guided iCBT interventions for anxiety disorders and depression have generated outcomes similar to those from therapist-guided interventions (Titov et al., 2009, 2010b, 2013). Thus, future RCTs exploring the relative benefits of therapist and self-guided interventions as well as younger adults’ usage patterns and engagement with online interventions, with larger sample sizes and longer-term follow-up, would be of considerable value.
In summary, the present study provides preliminary evidence indicating the Mood Mechanic Course for younger adults with anxiety and depression is efficacious and acceptable to young adults. Large within-group effect sizes were found on standard measures of anxiety and depression, which were maintained at the 3-month follow-up. Overall, the findings of the present study are encouraging and highlight the value of continued research concerning the Internet-delivery of treatment to younger adults as a way of increasing access to effective, acceptable and evidence-based care.
Footnotes
Funding
This project was funded by a National Priority Driven Research Program Grant from beyondblue. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. BFD is supported by a National Health and Medical Research Council (NHMRC) Australian Public Health Fellowship.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.