
Abstract
Background:
Internet-delivered cognitive behaviour therapy may increase access by young adults to evidence-based treatments for anxiety and depression.
Objective:
The aim of this study was to compare the efficacy of an Internet-delivered cognitive behaviour therapy intervention designed for adults aged 18–24 years, when delivered in clinician-guided versus self-guided formats.
Design:
The intervention, the Mood Mechanic Course, is a transdiagnostic treatment that simultaneously targets symptoms of anxiety and depression using cognitive and behavioural skills. The brief intervention comprised four lessons, delivered over 5 weeks. Following a brief telephone interview, young adults (n = 191) with symptoms of anxiety and depression were randomly allocated to either (1) clinician-guided treatment (n = 96) or (2) self-guided treatment (n = 95).
Results:
At post treatment, large reductions (average improvement; clinician guided vs self-guided) were observed in symptoms of anxiety (44% vs 35%) and depression (40% vs 31%) in both groups. Significant improvements were also observed in general psychological distress (33% vs 29%), satisfaction with life (18% vs 15%) and disability (36% vs 29%). No marked or consistent differences in clinical outcomes emerged between conditions at post-treatment, at 3-month or 12-month follow-up. Satisfaction was high with both treatment formats, but slightly higher for clinician-guided treatment.
Conclusion:
These results indicate the potential of carefully developed Internet-delivered cognitive behaviour therapy interventions for young adults with anxiety and depression provided in either self or therapist-guided format. Further large-scale research is required to determine the short- and long-term advantages and disadvantages of different models of support.
Keywords
Introduction
Anxiety and depression are common in young adults and often have their onset in adolescence and early adulthood (Patel et al., 2007). However, research indicates that young adults are less likely to seek treatment compared to older adults (McDermott, 2010; Merikangas et al., 2011). This is problematic given the well-known associations between anxiety and depression in youth and chronic mental health difficulties, poorer workforce participation and lower living standards in later life (Gibb et al., 2010; Shankman et al., 2009). Barriers to treatment include the costs of treatment, the limited number of services and geographic distance from services, stigma and the well-documented belief among youth that they do not require professional help (Collins et al., 2004; Corrigan and Rusch, 2002; Rickwood et al., 2007). These barriers have led to calls for ‘youth friendly’ mental health services (McDermott, 2010; Patel et al., 2007) and significant interest in the potential of e-mental health services (Reyes-Portillo et al., 2014).
There is substantial evidence for Internet-delivered treatment for anxiety and depression in adults, particularly treatments based on the principles of cognitive behaviour therapy (Internet-delivered cognitive behaviour therapy [iCBT]; Andersson and Hedman, 2013; Andersson and Titov, 2014; Andrews et al., 2010; Hedman et al., 2012). Reflecting this, online mental health services that provide iCBT as a routine service for anxiety and depressive disorders are emerging in several countries (Hadjistavropoulos et al., 2016; Hedman et al., 2013; Mewton et al., 2012; Ruwaard et al., 2012; Titov et al., 2015b, 2016a). However, comparatively few studies have examined iCBT for younger adults and adolescents. For example, a recent systematic review of interventions for youth found 17 clinical trials (14 randomised controlled trials [RCTs] and 3 open trials) reporting on 9 different interventions (Reyes-Portillo et al., 2014). This systematic review provides encouraging evidence with most trials reporting significant reductions in symptoms of depression and anxiety. However, the review noted significant variability in the quality of available trials and that many were limited by small sample sizes. It also highlighted the need for further research to explore a broad range of issues, including adherence, satisfaction and the role of clinician support.
iCBT treatments are designed to teach the same information and cognitive and behavioural skills as face-to-face treatments (Andersson et al., 2014). However, where these skills are taught by clinicians in face-to-face treatment, iCBT uses online modules which patients work through themselves. iCBT can be provided with different levels of clinician guidance varying from regular weekly contact, clinical contact as-needed and self-guided formats with little or no contact. Available meta-analyses have found both clinician-guided and self-guided iCBT to be efficacious, but have consistently reported that clinician-guided interventions are associated with superior adherence and clinical outcomes (Andersson and Hedman, 2013; Andersson et al., 2014; Andrews et al., 2010). For example, a systematic review of trials directly comparing clinician-guided and self-guided interventions (eight trials; combined n = 737) found evidence that clinician guidance was associated with slightly better outcomes for depression (standard mean difference = –0.15) and social anxiety (standard mean difference = –0.27; Baumeister et al., 2014). However, several trials have recently emerged of newly developed self-guided interventions that have produced similar outcomes to clinician-guided interventions (Dear et al., 2015a, 2015b, 2016; Fogliati et al., 2016; Titov et al., 2015a, 2016b). This new generation of self-guided interventions is specifically designed to facilitate engagement and adherence (e.g. automated emails, initial preparatory discussions with a therapist, symptom and safety monitoring) to enhance their potential to provide sufficient exposure to therapeutic materials. To date, however, the potential of these second-generation self-guided iCBT interventions has not been evaluated with young adults.
This study compared the efficacy and acceptability of an iCBT intervention for anxiety and depression among young adults aged 18–24 years, when delivered in either a clinician-guided or self-guided format. Following a brief telephone assessment and preparatory discussion, participants were randomised to receive a transdiagnostic iCBT intervention with regular contact with a clinician via email and telephone or via a self-guided format without contact. It was hypothesised that at post-treatment, both groups would report significant improvements on measures of anxiety and depression, but that the clinician-guided group (CG) would obtain superior outcomes, higher levels of satisfaction and higher levels of treatment adherence than the self-guided group (SG). It was hypothesised that the clinical outcomes would be maintained at 3- and 12-month follow-up.
Method
Design and measures
The study employed a two-arm randomised controlled trial (RCT) comparing Internet-delivered treatment for young adults when provided with or without clinician support. The researchers sought to recruit at least 300 participants, which, with a two-tailed alpha set at 0.05 and a power of 0.80, would enable the detection of small effect size differences (i.e. Cohen’s d ⩾ 0.33) between the two groups. All outcome measures were collected via online questionnaires. The primary measures of anxiety and depression were administered weekly to monitor participants’ progress and safety throughout treatment. The secondary and tertiary measures were administered at pre-treatment, post-treatment and at 3- and 12-month follow-up. The acceptability and satisfaction questions were administered at post-treatment. Participants were informed they would have the opportunity to win a tablet device by completing the questionnaire measures at the follow-up time points.
Primary measures
The Patient Health Questionnaire 9-Item (PHQ-9) was used to assess the severity of depression symptoms (Kroenke et al., 2001). The PHQ-9 comprises 9 items and total scores ⩾10 are indicative of a Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) diagnosis of depression (Titov et al., 2011). The PHQ-9 has a score range of 0–27. Total scores can be classified as 0–4 (none), 5–9 (mild), 10–14 (moderate), 15–19 (moderately severe) and 20–27 (severe). Cronbach’s α = 0.75.
The Generalised Anxiety Disorder 7-Item Scale (GAD-7) was used to assess the severity of anxiety symptoms (Spitzer et al., 2006). The GAD-7 comprises 7 items and total scores ⩾8 are indicative of a DSM-IV diagnosis of an anxiety disorder (Dear et al., 2011). The GAD-7 has a score range of 0–21 and total scores can be classified as 0–4 (minimal), 5–9 (mild), 10–14 (moderate), and 15–21 (severe). Cronbach’s α = 0.87.
Secondary measures
The Kessler Psychological Distress Scale 10-Item (K10) was used to measure general psychological distress. The K10 is sensitive to symptoms and diagnoses of anxiety and depressive disorders (Kessler et al., 2002). The K10 has a score range of 10–50 and total scores can be classified as 10–19 (likely to be well), 20–24 (likely to have a mild mental disorder), 25–29 (likely to have a moderate mental disorder) and 30–50 (likely to have a severe mental disorder). Cronbach’s α = 0.87.
Tertiary measures
The Sheehan Disability Scale (SDS) is a 3-item measure of disability and functional impairment in work, study, social life and family life, and household responsibilities (Sheehan, 1983). The Satisfaction with Life Scale (SWLS) is a 5-item measure of general satisfaction with one’s life (Diener et al., 1985). Cronbach’s α = 0.83.
Acceptability and satisfaction
Treatment satisfaction and acceptability were assessed at post-treatment using three questions taken from other studies (Dear et al., 2015b, 2016; Fogliati et al., 2016; Titov et al., 2015a): (1) ‘Overall how satisfied were you with the course?’; (2) ‘Would you recommend the course to others?’ and (3) ‘Was it worth your time doing the course?’. Participants responded to the first question using a 5-point Likert scale, which ranged from ‘Very Satisfied’ to ‘Very Dissatisfied’, and the latter two questions with a ‘Yes’ or ‘No’ response.
Participants
The study was approved by the Human Research Ethics Committee (HREC) of Macquarie University, Sydney, Australia, and the trial was registered on the Australian and New Zealand Clinical Trials Registry (ANZCTR) as ACTRN12613000915752. Participants read about the study and applied to participate via the website of the eCentreClinic (www.ecentreclinic.org), which is a research unit specialising in developing and evaluating virtual treatments. The study was promoted via online advertising and social media. Interested individuals were invited to submit an online application to participate in the trial, which involved completing several symptom questionnaires and providing basic demographic information and contact details.
The inclusion criteria for the study were (1) resident of Australia aged 18–24 years, (2) a self-reported principal complaint of depression or anxiety symptoms and (3) having reliable Internet access. No cut-offs or threshold of minimal symptoms were employed as a criterion for participation in this study. The exclusion criteria were (1) experiencing very severe symptoms of depression (i.e. defined as a total score >23 or endorsing a score >2 to item 9 of the PHQ-9, (2) having a history of self-harm or suicide attempts within the last 12 months or (3) currently participating in cognitive behaviour therapy (CBT). The CONSORT flowchart for the trial is displayed in Figure 1. Questions pertaining to the inclusion and exclusion criteria were assessed via an online application form and confirmed during a telephone assessment. As shown in Figure 1, a large proportion of participants were excluded for not completing their online application (21%), not being willing to speak on the telephone (24%), being outside of the target age ranges (14%) and not living in Australia (5%). A proportion were also excluded for having very severe symptoms of depression (8%), significant suicidal ideation (6%), being actively suicidal (6%) and having a recent history of self-harm (4%).
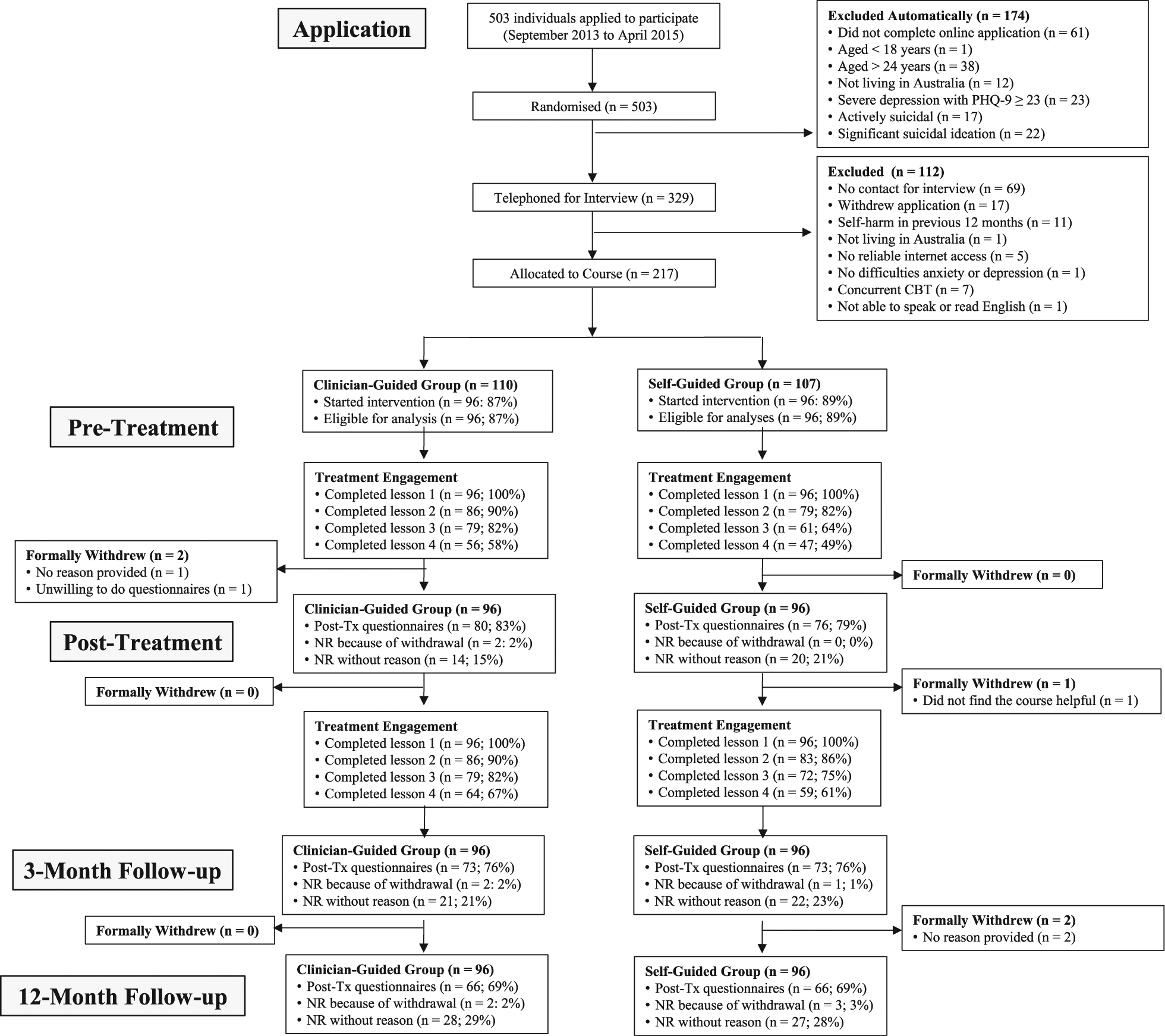
Participant flow from application to 12-month follow-up (NR = no response).
Participants were recruited between September 2013 and April 2015. All applicants were randomly allocated at the point of application by the eCentreClinic software system before participants had any contact with the researchers or the researchers had the opportunity to review the details of participants’ applications. Participants were randomised to one of two treatment groups, using a permuted block randomisation sequence generated by B.F.D.: a CG Group (n = 110) or a SG Group (n = 107). No blinding was employed. A total of 192 participants in the CG (n = 96) and SG (n = 96) groups started the intervention and were included in subsequent analyses.
Treatment intervention
This study employed the Mood Mechanic Course (Johnston et al., 2014), which is a brief 5-week intervention that teaches core transdiagnostic psychological principles and cognitive and behavioural skills (Andersen et al., 2016; Barlow et al., 2004; McHugh et al., 2009; Newby et al., 2015) for managing symptoms of depression and anxiety. The Mood Mechanic Course has been developed alongside several similar courses (Dear et al., 2015b, 2016; Fogliati et al., 2016; Titov et al., 2015a), but has been designed specifically for younger adults. It consists of four online lessons, homework assignments and detailed examples and case stories, which describe the experiences of young adults recovering from symptoms of depression and anxiety. An overview of the structure, content and skills taught within the course is provided in Table 1.
Timetable and content of the Mood Mechanic Course.
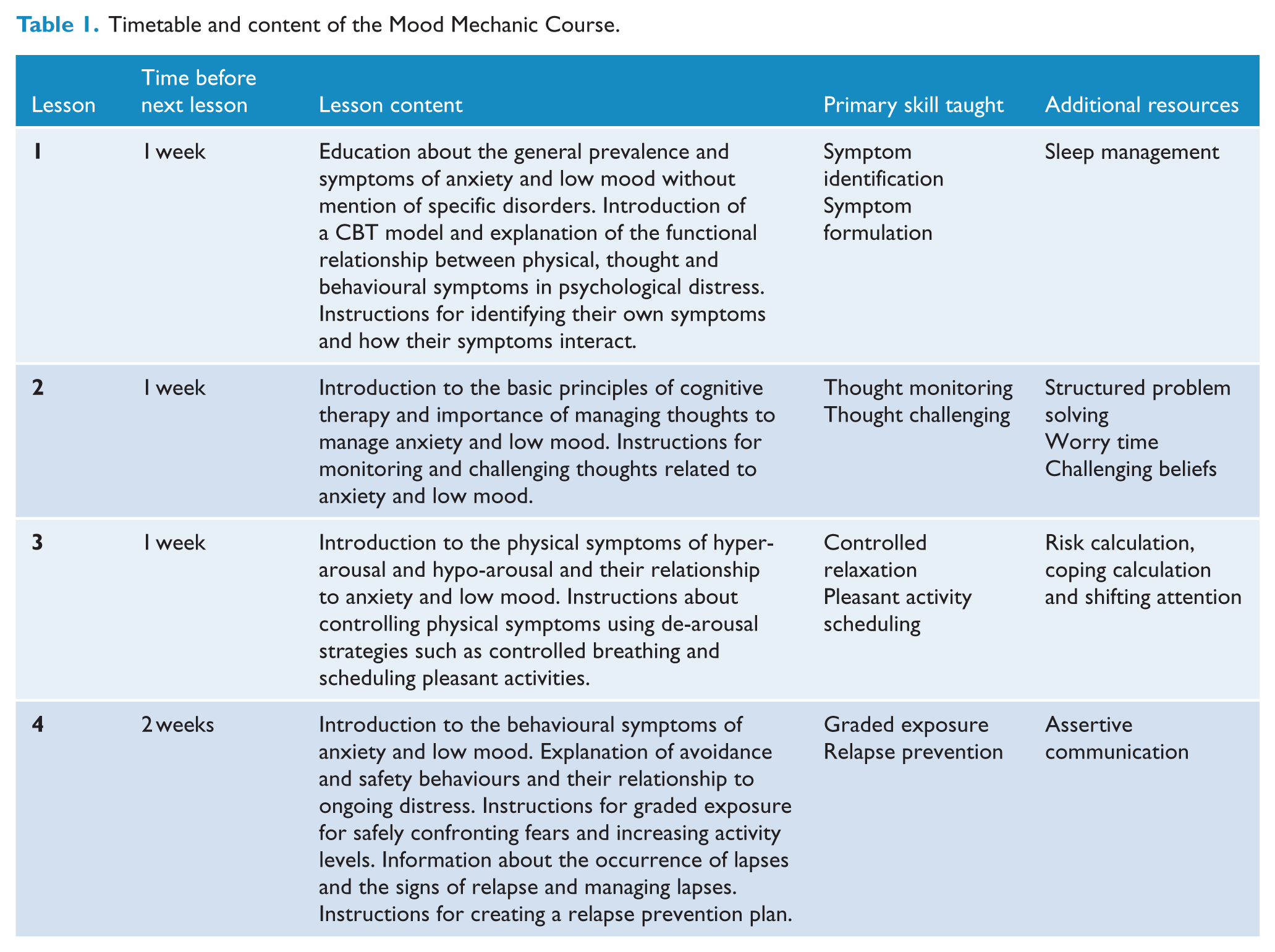
Each lesson is presented in a slide show format that combines didactic material (i.e. text based instructions and information) as well as real-world examples and case stories from young adults with anxiety and depression. These examples and case stories assist in showing how the information and skills can be used as well as to normalise the challenges in learning and applying the skills. Participants are instructed to read the lessons over 5 weeks according to a timetable. Each lesson takes between 10 and 20 minutes to read. Access to later lessons was dependent on participants first completing preceding lessons. Participants also receive regular automatic emails, which notify them of new course materials, and reinforce completion of materials and practice of skills. Participants are encouraged to complete one lesson every 7–10 days and to attempt to regularly practise the skills covered.
Clinician contact
Participants in the CG and SG groups received a brief telephone interview from an eCentreClinic clinician. This call was scripted and aimed to (1) discuss the aims of treatment; (2) convey hope by describing the results of previous participants; (3) emphasise the importance of consistent practice of the skills over time; and (4) answer questions about the treatment. Participants in the CG group also received weekly contact from a clinician during treatment. Two registered and experienced psychologists provided all clinical contact with participants via telephone or a secure email system. In accordance with previous research (Dear et al., 2015b, 2016; Fogliati et al., 2016; Titov et al., 2015a), clinicians were instructed to (1) answer participants’ questions, (2) summarise content, (3) encourage skills practice, (4) resolve difficulties applying skills and (5) reinforce progress. Clinicians were instructed not to introduce therapeutic skills not covered within the course and to limit their contact with participants to approximately 10–15 minutes per week.
Participants in the SG Group were informed that they would not receive clinical contact throughout treatment unless their symptoms deteriorated. The symptom questionnaire responses of participants in both groups were monitored daily by the clinicians and contact was initiated if a deterioration in their mental health (i.e. defined as an increase in PHQ-9 total score of ⩾5 with a total score ⩾15 or a PHQ-9 question 9 score = 3) was observed.
Statistical analysis
All analyses were conducted using SPSS version 22. Participants who never started the intervention (n = 25) were not included in the main analyses reported here (resultant n = 192). However, the primary and secondary outcomes for the complete intention-to-treat sample (i.e. including participants that never started treatment) are provided in Supplement 1 and Supplementary Table 1. To address missing values and consistent with intention-to-treat principles, replacement values were generated for all dependent variables under the missing values assumption of missing at random (MAR; Little and Rubin, 2014). To determine the suitability of the MAR assumption, an exploration of variables predicting the likelihood of cases to become missing was conducted. Variables that predicted both missing-cases and treatment outcomes indicate non-ignorable mechanisms of missing cases (Little and Rubin, 2014). In a stepwise manner, non-predictive variables were removed. These models identified two dominant predictors for missing post-treatment cases. Specifically, the presentation of increased baseline depressive symptoms and decreased degree of treatment adherence together was identified to account for 25.2% of the missing-cases probability variance. Reflecting these findings, and consistent with expert recommendations (Hollis and Campbell, 1999; Little et al., 2012), the outcomes of missing cases were simulated and replaced via weighted longitudinal models that were adjusted for an individual’s degree of lesson completion, respective baseline symptoms and time by covariate interactions.
To examine the average trend of change following treatment, a generalised estimation equation (GEE) longitudinal modelling technique was employed. GEE emphasises the modelling of change in an average group effect over time while accounting for within-subject variance with the specification of a working correlation structure. All GEE models specified a gamma distribution with a log link response scale to address positive skewness in the dependent variable distributions and an unstructured working correlation matrix to account for the possibility of unique symptom change periods between time points. These models enable the measurement of patient change over time and produce change coefficients that reflect the average percentage change from baseline. Initial assessment was employed as baseline for the primary and secondary outcomes. For the tertiary outcomes, which were not assessed at initial assessment, pre-treatment was employed as baseline for all analyses. SPSS pairwise comparisons were used to explore and understand any significant main and interaction effects observed in the GEE analyses. No adjustments were made for multiple statistical comparisons in the current trial.
Several different statistics were calculated for comparison and benchmarking purposes. First, the average percentage change across time was calculated from the GEE analyses for each of the outcome variables with 95% confidence intervals (CIs). Importantly, to accurately reflect percentage change, a constant of 10 was subtracted from K10 scores when calculating percentage change scores to result in a minimum score of 0. Second, Cohen’s d effect sizes and 95% CIs were also calculated for the within-group and between-group effects based on the estimated marginal means derived from the GEE models. Third, consistent with recommendations (Rozental et al., 2014), the Reliable Change Index was employed to identify both deterioration and improvement in symptoms at post-treatment. Specifically, participants reporting increases in their total scores of ⩾5 and ⩾6 points on the PHQ-9 and GAD-7, respectively, and reporting at least mild symptoms at post-treatment (i.e. total scores ⩾5) were classified as having Reliably Deteriorated.
Participants reporting reductions in their total scores ⩾5 and ⩾6 points on the PHQ-9 and GAD-7, respectively, and symptoms below the clinical range (total scores ⩾10 and ⩾8 points on the PHQ-9 and GAD-7, respectively) were classified as Reliably Recovered.
Results
Baseline data, adherence and attrition
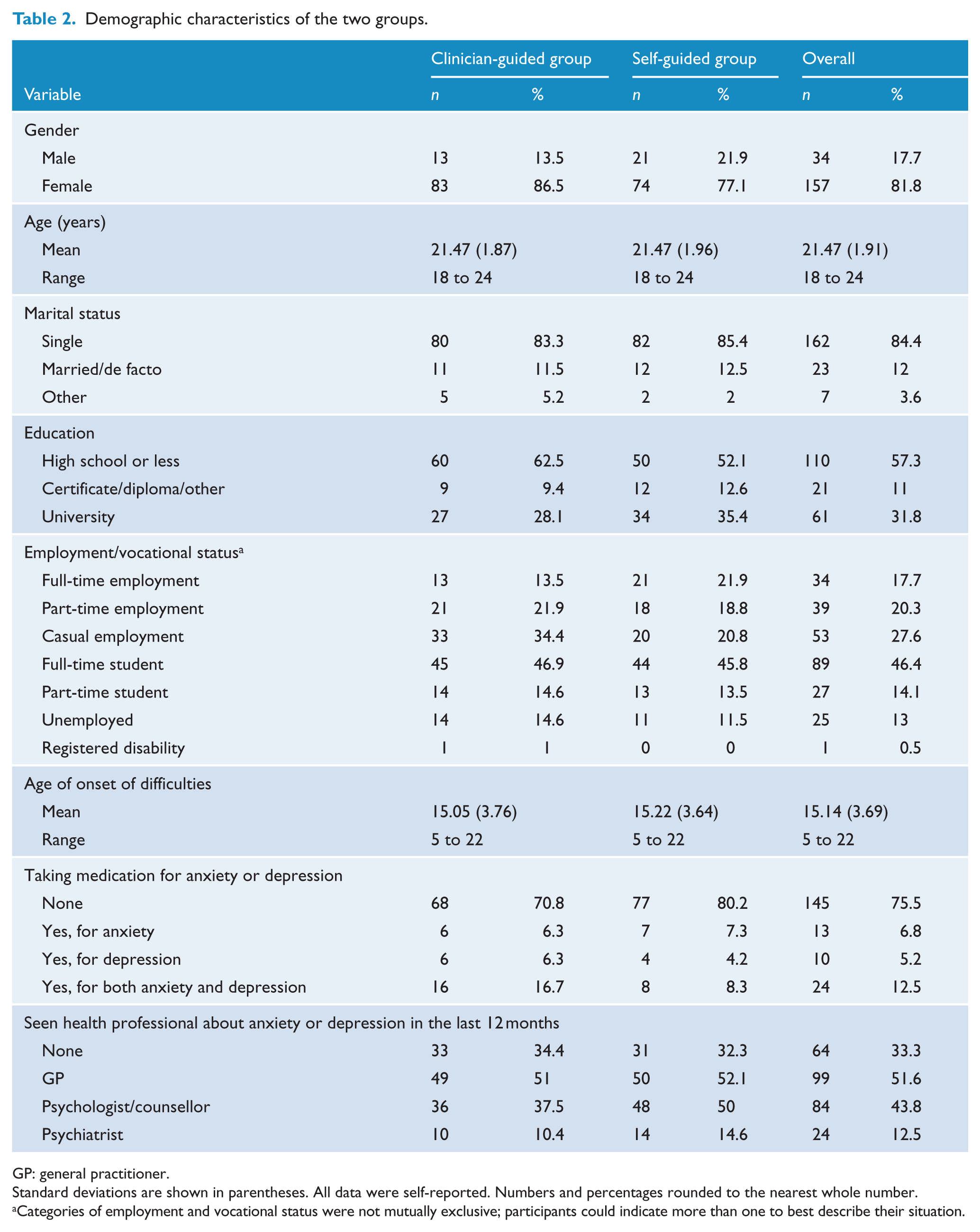
The demographic and clinical characteristics of the sample are shown in Table 2. Specific details of participant flow, treatment attrition, lesson completion and questionnaire response are shown in Figure 1. Randomisation appeared to result in largely comparable groups. Of note, the sample was mostly female (81.8%) and many had seen a health professional (general practitioner (GP) = 51.6%; psychologist or counsellor = 43.8%; psychiatrist = 12.5%) about their mental health in the previous 12 months.
Demographic characteristics of the two groups.
GP: general practitioner.
Standard deviations are shown in parentheses. All data were self-reported. Numbers and percentages rounded to the nearest whole number.
Categories of employment and vocational status were not mutually exclusive; participants could indicate more than one to best describe their situation.
Achieved statistical power
Difficulties were experienced in recruiting the target number of participants (n = 300) and the resultant sample size was consequently smaller than planned (n = 192). With a two-tailed alpha set at 0.05 and a power of 0.80, the current analyses were powered to detect between-group effect (Cohen’s d) sizes ⩾0.41 between the two groups compared with the ⩾0.33 originally planned.
Clinician time
There were significant differences between the CG and SG Groups in the amount of overall clinician time required (Wald’s χ2 = 164.54, p < 0.001), with participants in the CG Group receiving an average of 34.20 minutes (SD = 23.89 minutes) contact with a therapist and participants in the SG Group receiving an average of 1.77 minutes (SD = 6.99 minutes) contact. The initial telephone assessment required an average of 11.69 minutes (SD = 3.99 minutes) contact with participants.
Clinicians made an average of 5.52 calls (SD = 1.88; average total call time = 21.78 minutes) to participants in the CG Group and sent an average of 4.59 messages (SD = 1.85; average total message time = 12.42 minutes). The clinicians made a total of 14 calls (average call time = 0.84 minutes; SD call time = 5.76 minutes) to participants in the SG Group and sent a total of 39 emails (average call time = 0.92 minutes; SD call time = 2.10 minutes). No participants required referral to emergency or crisis mental health services, and no participants attributed their deteriorations to the course.
Primary outcomes
The means, standard deviations and clinical statistics are shown in Table 3. The GEE analyses indicated a significant Time effect for both of the primary outcomes (PHQ-9; Wald’s χ2 = 312.02, p < 0.001; GAD-7: Wald’s χ2 = 342.24, p < 0.001). A significant Time-by-Group interaction was found for anxiety (GAD-7; Wald’s χ2 = 22.69, p < 0.001), but not depression (PHQ-9; Wald’s χ2 = 8.13, p = 0.087). Pairwise comparisons indicated that there were no significant differences between the CG and SG Groups at any time point for anxiety (ps > 0.183) and depression (ps > 0.076), with the exception of 3-month follow-up (p = 0.002) where the SG group reported significantly more anxiety symptoms than the CG Group.
Means, standard deviations and average percentage change from baseline.
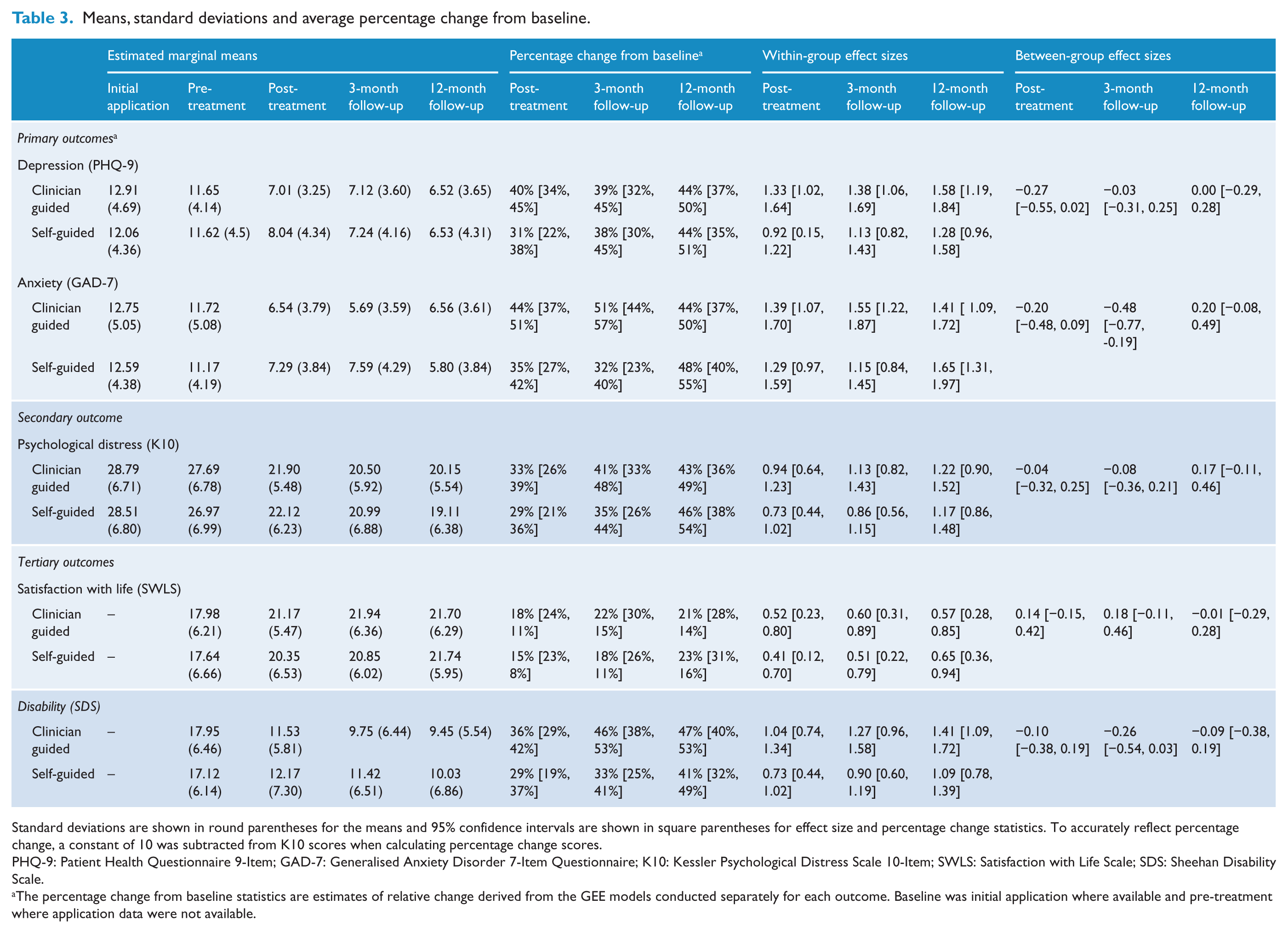
Standard deviations are shown in round parentheses for the means and 95% confidence intervals are shown in square parentheses for effect size and percentage change statistics. To accurately reflect percentage change, a constant of 10 was subtracted from K10 scores when calculating percentage change scores.
PHQ-9: Patient Health Questionnaire 9-Item; GAD-7: Generalised Anxiety Disorder 7-Item Questionnaire; K10: Kessler Psychological Distress Scale 10-Item; SWLS: Satisfaction with Life Scale; SDS: Sheehan Disability Scale.
The percentage change from baseline statistics are estimates of relative change derived from the GEE models conducted separately for each outcome. Baseline was initial application where available and pre-treatment where application data were not available.
Pairwise comparisons revealed that both groups improved from pre-treatment to post-treatment in depression symptoms (p < 0.001) and that these improvements were maintained from post-treatment to 3-month (p > 0.107) and 12-month follow-up (p > 0.153). These comparisons also revealed that both groups improved from pre-treatment to post-treatment in anxiety symptoms (p < 0.001), but that the SG Group also improved slightly from 3-month to 12-month follow-up (p < 0.001). In contrast, anxiety symptoms in the CG Group reduced slightly from post-treatment to 3-month follow-up (p = 0.023) but then slightly increased from 3-month follow-up to 12-month follow-up (p = 0.020).
Fifty-eight percent [CI: 48% to 68%] and fifty-one percent [CI: 40% to 61%] of participants in the CG and SG Groups, respectively, were classified as cases with Reliable Recovery from their depressive symptoms at post-treatment; a difference that was not significant between groups (Wald’s = 1.083, p = .298). Fifty-eight percent [CI: 48% to 68%] and forty-eight percent [CI: 38% to 58%] of participants in the CG and SG Groups, respectively, were classified as cases with Reliable Recovery from their anxiety symptoms at post-treatment (Wald’s = 2.336, p = .126).
Secondary outcomes
The secondary outcome was general psychological distress, which was assessed with the K10. The GEE analyses indicated a significant effect for Time (K10: Wald’s χ2 = 297.10, p < 0.001) but no significant Time-by-Group interactions (K10: Wald’s χ2 = 3.58, p = 0.465). Pairwise comparisons indicated no significant differences in psychological distress between the groups at any time point (ps > 0.250).
Tertiary outcomes
The tertiary outcomes were disability and satisfaction with life, which were assessed with the SDS and SWLS, respectively. Analyses indicated a significant time effect for both groups (SDS: Wald’s χ2 = 222.56, p < 0.001; SWLS: Wald’s χ2 = 79.30, p < 0.001) for both of the tertiary outcomes, but no significant Time-by-Group interactions (SDS: Wald’s χ2 = 5.08, p = 0.166; SWLS: Wald’s χ2 = 2.28, p = 0.516).
Negative outcomes
Six percent [CI: 3% to 15%] and 1% [CI: 0% to 9%] of participants in the CG and SG Groups, respectively, were classified as deteriorating in depression symptoms at post-treatment. Seven percent [CI: 3% to 16%] and 8% [CI: 4% to 17%] of participants in the CG and SG Groups, respectively, were classified as deteriorating in anxiety symptoms at post-treatment. No between-group differences were found in the proportions of participants deteriorating in symptoms of depression (Wald’s = 2.036, p = .154) or anxiety (Wald’s = 0.058, p = .810). No participants reported their deteriorations as being due to the treatment.
Treatment completion and satisfaction rates
There was a significant difference between groups in the number of lessons completed immediately post-treatment (Wald’s χ2 = 4.48, p = 0.034) with the CG Group completing more of the lessons compared with the SG Group (% completing all lessons: 58% vs 49%; M lessons completed = 3.28 vs 2.95). However, there was no significant difference (Wald’s χ2 = 0.77, p = .378) at 3-month follow-up (% completing all lessons: 67% vs 61%; M lessons completed = 3.36 vs 3.23), indicating that a significant proportion continued to access the materials post-treatment. Of the participants who completed the evaluation questions at post-treatment, 100% (78/78) and 94% (70/74) of participants in the CG and SG Groups, respectively, indicated they would recommend the course to others. Similarly, 97% (76/78) and 93% (69/74) of participants in the CG and SG Groups respectively, responded that the course was worth their time. There were no differences between groups in the proportions reporting they would recommend the course (Wald’s χ2 = 0.00, p = 0.998) or that it was worth their time (Wald’s χ2 = 1.41, p = 0.235). A greater proportion of participants in the CG reported being very satisfied with the course compared with the SG Group (Wald’s χ2 = 1.8, p = 0.001; 46% vs 27%). However, there was no difference in the percentage of participants in the CG group reporting being either satisfied (Wald’s χ2 = 1.84, p = 0.174; 37% vs 51%) or neutral (Wald’s χ2 = 1.33, p = 0.248; 17% vs 28%). Only one participant in the SG Group reported being dissatisfied.
Discussion
This study evaluated a transdiagnostic Internet-delivered intervention, the Mood Mechanic Course, for young adults when provided in clinician-guided and self-guided formats. It was hypothesised that both formats would be acceptable and associated with symptom improvements, but that the clinician-guided format would be superior. These hypotheses were partially supported. Both treatment groups achieved significant reductions in symptoms immediately post-treatment. Despite a trend favouring the clinician-guided treatment, no significant differences were found between the two treatment formats. Importantly, clinical improvements were maintained at 3- and 12-month follow-up, and rates of satisfaction were high across formats. Significant improvements were also observed on measures of satisfaction with life, psychological distress and disability, indicating improvements generalised to other important domains. Both groups continued to use the course after the post-treatment time point, and no differences in treatment completion were present at 3-month follow-up. Low levels of deterioration were also observed and no participants reported deteriorations as resulting from the treatment provided.
The reductions seen in the current trial were large and consistent with those reported in Internet-delivered treatments for adults (Andersson et al., 2014; Andersson and Hedman, 2013; Andrews et al., 2010; Hedman et al., 2012). These findings contribute to the growing literature (Berger et al., 2011a, 2011b; Dear et al., 2015a, 2015b, 2016; Fogliati et al., 2016; Titov et al., 2015a, 2016b) indicating that second-generation self-guided treatments, which include features designed to improve engagement, can produce clinical benefits similar to clinician-guided treatments. This is an important outcome given the significant public health potential of self-guided treatments, especially as a first step for young adults who are otherwise unwilling to engage with mental health services. A relatively recent development which may further help realise the public health potential of Internet-delivered treatments is to combine aspects of clinician and self-guided treatment models. For example, emerging evidence suggests so-called ‘patient-centred’ treatment models, in which clinician support is only provided when requested or clinically indicated, may provide an optimum balance of patient independence and clinical care, while achieving outcomes comparable to clinician-guided models (Berger et al., 2011a, 2011b; Dear et al., 2015a; Hadjistavropoulos et al., 2016a). Future research could explore the potential of this patient-centred model in young adults, who may be less inclined to want regular clinician contact. Such research should also explore the cost-effectiveness of the different models.
The results of this study should be interpreted with consideration of two important caveats. First, the intervention employed in this study has been carefully developed over several years with the aim of optimising its efficacy in a self-guided format. Specifically, it was informed by the relevant evidence-base and co-designed with large numbers of patients and numerous clinicians who have had first-hand experience with the intervention. Reflecting this, the structure and content of the current course was heavily modified for the current trial based on feasibility testing of an earlier version of the Mood Mechanic Course (Johnston et al., 2014) and other similar courses for university students (Mullin et al., 2015). Second, all participants had an initial, albeit brief, telephone discussion with a clinician that was designed to prepare and encourage the participant to engage with the course. Moreover, participants were informed that a clinician would be monitoring their progress throughout the course and would get in touch if they had concerns about their progress or safety. This is important in light of the proportion of young adults interested in this trial who had severe symptoms, suicidal ideation and histories of self-harm. This approach to self-guided treatment differs from fully automated self-guided interventions, where a participant’s only experience is with a standalone website which may not provide monitoring or support.
This study has several limitations. First, the absence of a control group means it is not possible to conclude that the clinical effects observed were a result of the treatment provided. However, the magnitude of clinical effects observed was large and would seem unlikely to be explained entirely by time or natural remission. Second, difficulties were experienced in the recruitment of the target number of participants. A non-trivial proportion of interested participants (21%) were also excluded for not completing their online applications and, after completing an application, not being willing to speak on the telephone (24%). Consequently, this study was only powered to detect between-group differences of a magnitude greater than 0.41 compared with 0.33 as originally designed. This difficulty in recruitment occurred despite considerable marketing and in the face of relatively limited demands for participation. This raises the possibility that the true demand for treatment among young adults may be lower than thought and that the difficulties engaging young adults in face-to-face services may also extend to online services. It may also reflect the possibility that having to engage directly with a clinician, even via telephone and secure email, is a barrier to mental health services for young adults. Third, the present trial was designed as a superiority trial and caution is needed in concluding the two treatment formats are truly equivalent. Fourth, the results are based on self-reported symptom scores and no formal diagnostic interviews were undertaken. Fifth, this study employed a convenience sample of treatment seeking young adults, which may not be representative of the broader population or the cohorts presenting to other mental health services. Consequently, some caution is required in generalising the current findings.
In conclusion, these results augment and extend available evidence indicating that carefully developed iCBT interventions may be both acceptable and effective at reducing symptoms in young adults, when administered in both clinician-guided and self-guided formats. Outstanding questions include the relative benefits of clinician and self-guided interventions when the latter is delivered without an initial telephone discussion. Another important question is whether these results will be replicated if the Mood Mechanic intervention were administered in routine clinical care. The Mood Mechanic course has recently been deployed for use at a national virtual mental health service in Australia, the MindSpot Clinic (www.mindspot.org.au; Titov et al., 2015b, 2016a), and reports of this intervention when provided as routine care will be forthcoming.
Footnotes
Acknowledgements
The authors gratefully acknowledge the participants for their involvement and helpful feedback during the course of this research.
Declaration of Conflicting Interests
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was enabled by a National Priority-Driven Research Program Grant from beyondblue. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication. BFD was supported by a National Health and Medical Research Council (NHMRC) Australian Public Health Fellowship during this research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.