
Abstract
Objective:
In September 2010 Christchurch, New Zealand, was struck by a 7.1 magnitude earthquake, followed by a prolonged sequence of significant aftershocks including a fatal aftershock in February 2011. Christchurch City has experienced widespread damage, ongoing disruption and building demolitions resulting in many difficulties for the residents of the Christchurch area. We explore what impact the earthquakes have had on the mental and physical health of a random sample of 50-year-olds who live in the Christchurch area.
Methods:
The 295 participants were selected from the electoral rolls for participation in the CHALICE study, a longitudinal study of ageing. Self-reported health status was assessed using the standardised Short Form 36 version 2 health survey (SF-36v2), a 36-item questionnaire, and results from the eight subscales compared to a national health survey. Mood disorders were assessed and the results were compared to other local and national studies.
Results:
Since the onset of the earthquakes and throughout the study period, participating middle-aged Christchurch residents have mean SF-36v2 scores significantly lower than population norms in the mental health, vitality, social functioning and role-emotional subscales (Cohen’s d ranged from −0.270 to −0.357, all p < 0.001), while there was no evidence of reduced physical health. Rates of current major depressive disorder were 7.5% in the earthquake survivors compared to 5.1% and 3.7% in other historical, local and national surveys. Similarly, bipolar disorder prevalence was 2.8% in the earthquake survivors compared to 2.2% and 1.4% in other studies.
Conclusion:
Eighteen months after the first earthquake the significant adverse impact on mental health clearly continues. The ongoing provision of additional mental health services and consideration of these adverse mental health effects in relation to other social policies remains necessary and fundamental.
Keywords
Introduction
At 04:35 on 4 September 2010 a 7.1 magnitude earthquake was centred 38 km west of Christchurch, New Zealand at a depth of 11 km. Despite the strength and shallowness of the earthquake, there were no fatalities but there was widespread damage to buildings in the Christchurch area. In the 2 years since the initial earthquake there have been over 4000 aftershocks of magnitude 3 and over in and around the Christchurch area. The aftershock sequence includes the 22 February 2011 earthquake that resulted in 185 fatalities, a magnitude 6.3 tremor on 13 June 2011 and a 6.2 magnitude earthquake on 23 December 2011. The initial health-system response to this earthquake has been described previously (Ardagh et al., 2012). The widespread damage has resulted in a multitude of stressors for the residents of the Christchurch area – 100,000 homes are damaged and 10,000 are to be demolished, including the abandonment of whole suburbs. The estimated cost of the rebuild is NZ$40 billion (TV3 New Zealand, 2013). Residents have had to negotiate their way through a process of insurance claims and government buy-outs of their land.
Exposure to earthquakes and disasters has been shown to affect the mental well-being of survivors (Chou et al., 2004a, 2004b; Wang et al., 2000b). Survivors are at increased risk of developing post-traumatic stress disorder (Chou et al., 2004b; Wang et al., 2000a), and depression and anxiety (Chou et al., 2004b; Zhang et al., 2012). These adverse impacts can continue for years after the event (Tempesta et al., 2013; Wu et al., 2006). The Short Form 36 health survey (SF-36) (Ware and Sherbourne, 1992; Ware et al., 2000), is a widely used measure of self-reported health-related quality of life (Garratt et al., 2002). One earthquake study in South West China (Ke et al., 2010), which resulted in massive loss of life and destruction, has used the SF-36 to measure self-reported health across eight domains of physical and mental health. To our knowledge this is the only earthquake study to compare SF-36 results with national population norms. The study population were survivors living in earthquake shelters with a mean age 32.28 years and 40% were full-time students. Survivors reported significantly lower scores on all eight scales than the general population and the researchers found that being older and female were risk factors for poorer SF-36 scores. Other factors influencing the SF-36 scores in this study were marital status, occupation and residential zone (Ke et al., 2010).
Ke et al. (2010) describe an earthquake that caused 70,000 deaths and approximately 5 million survivors to become homeless. What is not known is how earthquake survivors respond physically and mentally when earthquakes hit their region which, though devastating in many ways, do not cause massive fatalities, homelessness and injuries. A review of stressors in extreme events (Lock et al., 2012) has identified primary stressors that cause obvious and immediate distress such as injuries or watching someone die. The review also describes secondary stressors (e.g. economic, family, continued lack of infrastructure), the effects of which can be more prolonged and may contribute to ongoing stress and mental disorder.
Using data from a longitudinal population study, we present findings on how a sample of 50-year-olds self-report on eight measures of health assessed by the SF-36 version 2 (SF-36v2) (Ware and Sherbourne, 1992; Ware et al., 2000), and on the prevalence of current mood disorders, as assessed by interviewers. These results are compared with recent historical data from regional and national populations. We expect that earthquake survivors will self-report poorer mental and physical health and that the prevalence of current mood disorders will be higher than prevalence rates previously recorded for a similar geographical area.
Methods
Study population
The participants were from a random sample chosen from the New Zealand electoral rolls to take part in a prospective longitudinal study of health and well-being called the Canterbury Health, Ageing and Lifecourse (CHALICE) study (For more details see Schluter et al., 2013). Potential participants had to be aged 49–51 years, intend to reside within the greater Christchurch district area for at least 6 of the next 12 months, live in the community (i.e. not in a prison or a rest home) and be able to complete the assessment (e.g. speak English proficiently). Recruitment began immediately prior to the onset of the earthquake sequence.
Māori are the indigenous people of New Zealand and about 20% of the population are descended from Māori. In Canterbury Māori constitute only 8%. To ensure a sufficient sample for meaningful ethnic comparisons, Māori were over-sampled with an objective of being 20% of the CHALICE study sample. The New Zealand government has two electoral rolls, a general roll and a Māori roll. Registration on one of the rolls is compulsory. Enrolment statistics estimate that in 2012 97.1% of 50–54-year-olds were registered to vote in the Christchurch City Council area (Electoral Commission Te Kaitiaki Taki Kowhiri, 2013).
Christchurch is in the South Island of New Zealand and is in the region of Canterbury. In June 2012 the estimated population of urban Christchurch was 363,000 (Statistics New Zealand, 2012), and the population of the combined urban and rural area of the Canterbury District Health Board (CDHB) was 510,000 (Ministry of Health, 2012/3). Relative to the rest of New Zealand, the CDHB area has a slightly higher proportion of people aged 40 years and above and a higher proportion of people living in the least economically deprived national quintile (Ministry of Health, 2012/3).
A subsample (N = 212) of the CHALICE participants were asked additional earthquake questions after the destructive aftershock in February 2012 had occurred. The additional questions included whether they had lost family or a close friend as a result of the earthquakes, the personal impact of the earthquakes and the extent of earthquake damage to their home.
Assessment
CHALICE participants took part in a 4–5 hour assessment which had seven modules: physical health, health history, family and social health, heart health, mental health, cognitive aspects and lifestyle. Participants completed questionnaires in the 7 days before their assessment, including the SF-36v2 (Ware and Sherbourne, 1992; Ware et al., 2000). Standard of living was assessed using the Economic Living Standard Index Short Form (ELSISF) (Jensen et al., 2005). The ELSISF correlates moderately with other measures associated with standard of living and has excellent internal consistency (coefficient alpha of 0.88) (Jensen et al., 2005). For some of the analyses participants were divided into two groups of lower and higher SES by their ELSISF score. The range of scores for the ELSISF is 0 to 31; with those who score 0 to 24 described as being in severe hardship to comfortable (lower) and scores of 25 or above are considered to be socio-economically good or very good (higher) (Jensen et al., 2005).
During the assessment trained interviewers used the Mini-International Neuropsychiatric Interview (MINI) (Sheehan et al., 1998) for diagnosis of current and past depressive episodes and for identifying episodes of mania, hypomania and recurrent brief hypomanic episodes. Those participants that reported any type of manic episode, including recurrent brief hypomanic episodes, were classified as having bipolar disorder. Recurrent brief hypomanic episode was defined as a hypomanic episode that lasted for less than 4 days and there was no impairment.
SF-36v2
The SF-36v2 (Ware and Sherbourne, 1992; Ware et al., 2000) is a 36-item questionnaire that measures eight multi-item subscales of health: physical functioning, role limitations due to physical problems (role-physical), bodily pain, general health perception, vitality, social functioning, role limitations due to emotional problems (role-emotional) and mental health. The first scale, physical functioning, has primarily a physical health focus and the eighth scale, mental health, has a mental health focus. For each subscale item scores are coded, summed and transformed on to a scale from 0 (worst possible health state measured by the questionnaire) to 100 (best possible health state). The questionnaire has high internal consistency with Cronbach’s alpha coefficients ranging from 0.83 (general health) to 0.95 (role-physical) and good test–retest reliability (intra-class correlation coefficient ranging from 0.42 to 0.96) (Ware et al., 2007). The concurrent validity estimates for the eight subscales are between 0.76 (role-emotional) and 0.93 (general health and mental health). The SF-36 has eight of the most commonly used health concepts (Ware et al., 2007), but does not measure other concepts such as sleep and cognitive function. The most recent 2006/7 New Zealand Health Survey has published scores for the SF-36v2 by age group (Ministry of Health, 2008), thereby providing scores for the general population.
Statistical methods
Data from the study was entered into the study database (Progeny Software, Needham, South Norfolk, UK) and transferred to Stata version 12.0 for statistical analyses and graphing (StataCorp, 2011). A two-sided α = 5% defined significance for all tests. Missing data points of the scored instruments (i.e. ELSISF and SF-36v2) were estimated using the guidelines from the appropriate user manual (Jensen et al., 2005; Ware et al., 2007). There was one item of missing data for the ELSISF and eight missing data points for the SF-36v2. There were no other missing data points. Reporting of method and results were informed by the STROBE guideline (Vandenbroucke et al., 2007). Analyses included frequencies, means, confidence intervals and t-tests. The comparison of SF-36v2 means between the CHALICE and New Zealand Health Survey (NZHS) data used Student’s t-test, with degrees of freedom derived from the Welch–Satterthwaite equation to account for any difference between the variances. The data has been analysed with estimates weighted inversely to the sampling fractions in the selection strata. The studies used for comparison with the CHALICE study were the 2006/7 New Zealand Health Survey (NZHS) (Ministry of Health, 2008), the 2004 New Zealand Mental Health Survey (NZMHS) (Oakley Browne et al., 2006), the Christchurch Psychiatric Epidemiology Survey (CPES) (Oakley-Browne et al., 1989; Wells et al., 1989), and the findings of a prevalence and comorbidity study by the Canterbury Suicide Project (CSP) (Beautrais et al., 1996).
Ethics
All participants gave informed written consent for the study. Ethical approval for the CHALICE study was obtained from the Upper South A Regional Ethics Committee on 14 June 2010 (reference: URA/10/03/021) and progress reporting is completed every 12 months.
Results
Participants
For this paper the cross-sectional data is for 295 of the first 300 participants enrolled into the study. The first five participants have been excluded because they were assessed before any of the earthquakes had happened. For the first 300 participants the participation rate was 63.7%. Table 1 shows the demographic characteristics of the CHALICE study participants at baseline compared to New Zealand 2006 census data (Statistics New Zealand, 2013) for the Canterbury region (where possible). In the CHALICE study there is a slightly higher percentage of females, home-owners and the percentage of people with a post-secondary qualification or university degree is higher in the CHALICE sample. Māori are over-represented in the CHALICE study and this reflects the sampling strategy. Further details of CHALICE study participants are described elsewhere (Schluter et al., 2013).
Baseline demographic characteristics of CHALICE study participants compared to New Zealand census 2006 data for the Canterbury region.
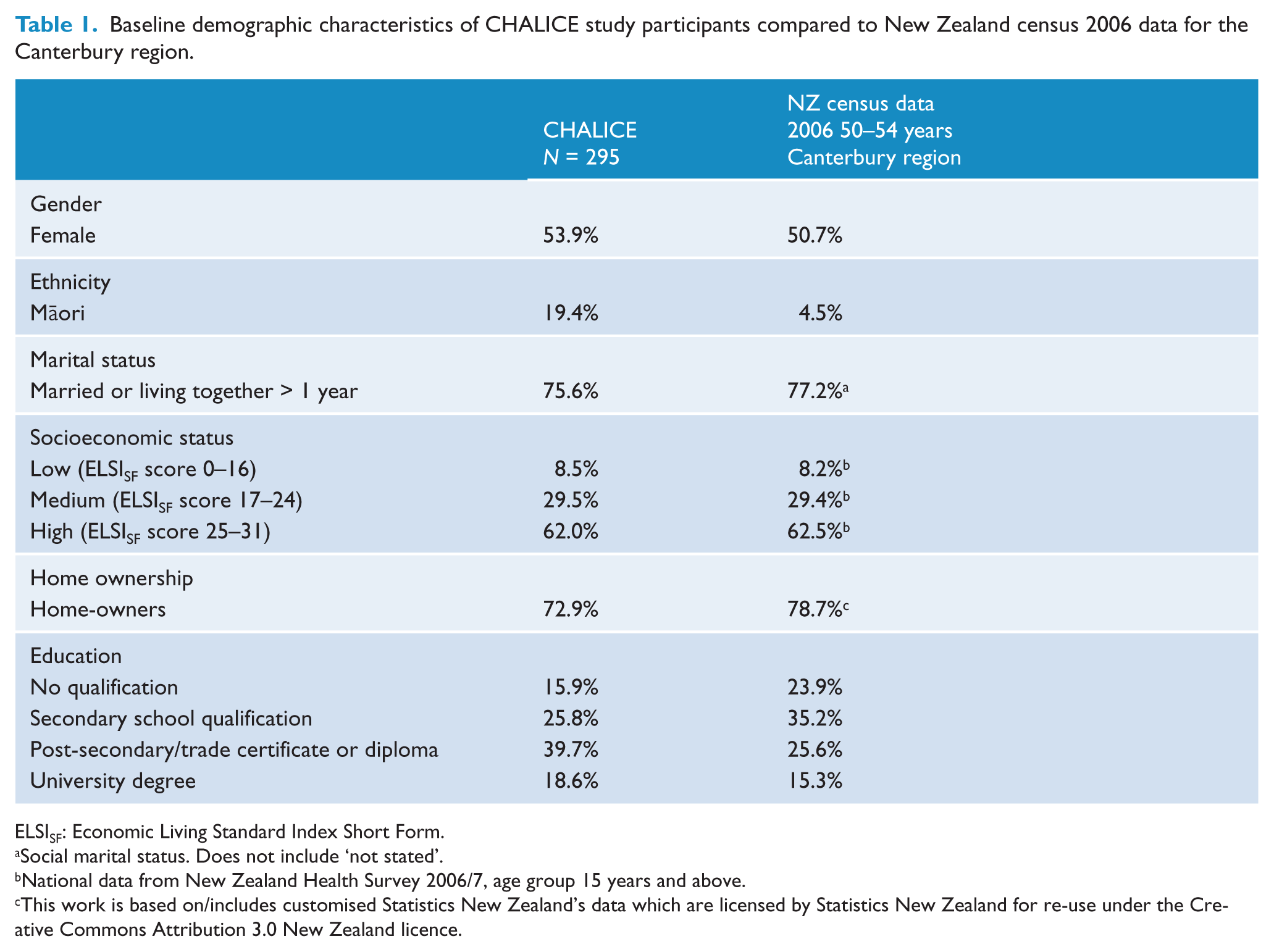
ELSISF: Economic Living Standard Index Short Form.
Social marital status. Does not include ‘not stated’.
National data from New Zealand Health Survey 2006/7, age group 15 years and above.
This work is based on/includes customised Statistics New Zealand’s data which are licensed by Statistics New Zealand for re-use under the Creative Commons Attribution 3.0 New Zealand licence.
SF-36v2 scores CHALICE vs. NZHS
Table 2 shows that the CHALICE study participants have significantly lower scores on the mental health aspects of the SF-36v2 subscales than the New Zealand average for a similar age group. The mean scores for physical functioning (PF), role-physical and bodily pain subscales are similar for both groups. The largest estimated absolute difference between the two groups is seen in the subscale mental health (MH), where post-earthquake Cantabrians have a score that is 7.3 points lower than the national average (p < 0.001); 5.1% of the sample scored two standard deviations below the New Zealand Health Survey mean on the MH subscale. There are also significant differences in mean scores between the two groups for vitality, social functioning and role-emotional (Table 2). Cohen’s d shows a small effect size (−0.357) for changes in MH subscale.
The baseline SF-36v2 subscale scores of CHALICE study participants compared to national figures. The range for all subscales is 0 to 100.
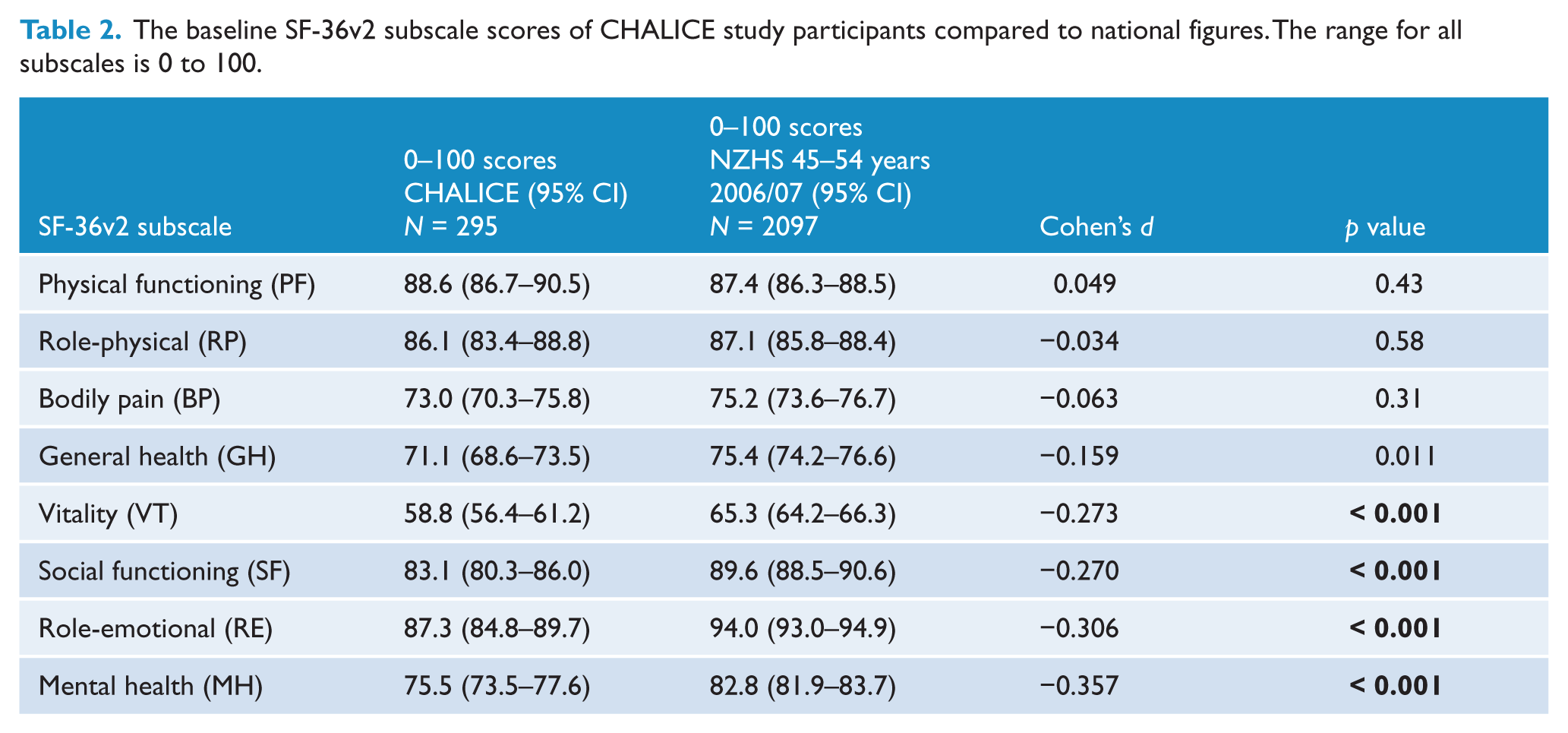
While PF was not different in CHALICE to the national sample, the MH score of the CHALICE sample has been consistently below the mean national score since the onset of earthquakes. Simple linear regression analysis showed that there is no significant change in mean physical functioning (p = 0.16) or mental health (p = 0.22) over time.
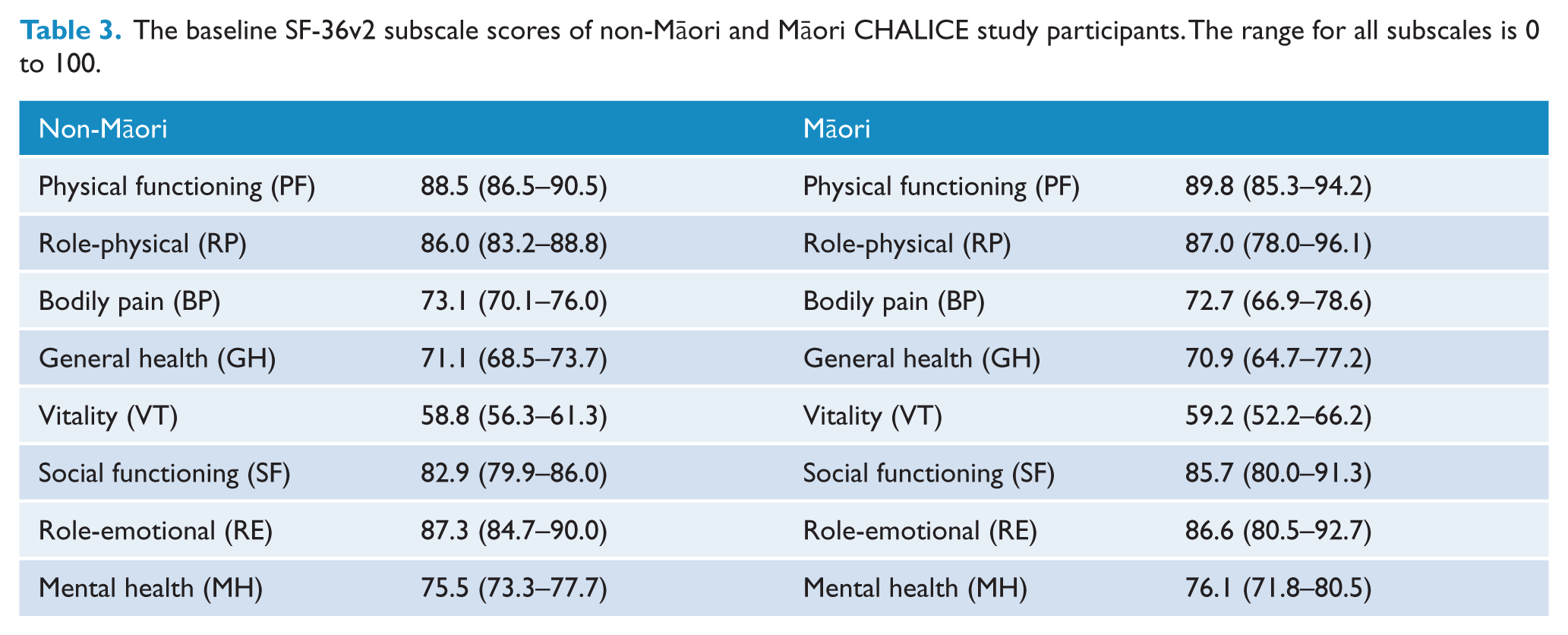
Moreover, there were no significant differences in mean SF-36v2 scores between males and females, except for physical functioning (p = 0.002). Further analysis on a subset of the sample (N = 212) showed that there were no significant differences between those who lost a close friend or relative because of the earthquakes (n = 22) and those who did not, or those people who reported more damage to their home (n = 19) compared to those reporting less damage. Table 3 presents the SF-36v2 scores for Māori and non-Māori. There were no significant differences between these two groups.
The baseline SF-36v2 subscale scores of non-Māori and Māori CHALICE study participants. The range for all subscales is 0 to 100.
Prevalence of current major depressive disorder compared to local and national surveys
Table 4 shows that the percentage of earthquake-exposed CHALICE participants being assessed as having current major depressive disorder (MDD) was 7.5% (2 week prevalence period) compared to 5.2% in a similar age group who were part of the NZMHS (12 month prevalence). The CPES, a study carried out in a similar geographical area to the CHALICE study, reported a 2 week prevalence in participants aged 16 years or over of 3.7%, almost half that of the percentage for the CHALICE study. Additionally, the 6 month prevalence for 45–64-year-olds in CPES was 5.1%, which is 2% lower than the shorter 2 week prevalence of 7.5% reported by CHALICE participants. Results published by CSP are similar in that they report MDD prevalence of 5.6% in people 18 years old and over who live in Canterbury, a comparable geographical area to the CHALICE study. The difference between the CHALICE study and historical prevalence rates mentioned above were found not to be significant.
Prevalence of current major depression and bipolar disorder for CHALICE study participants compared with local and national studies.
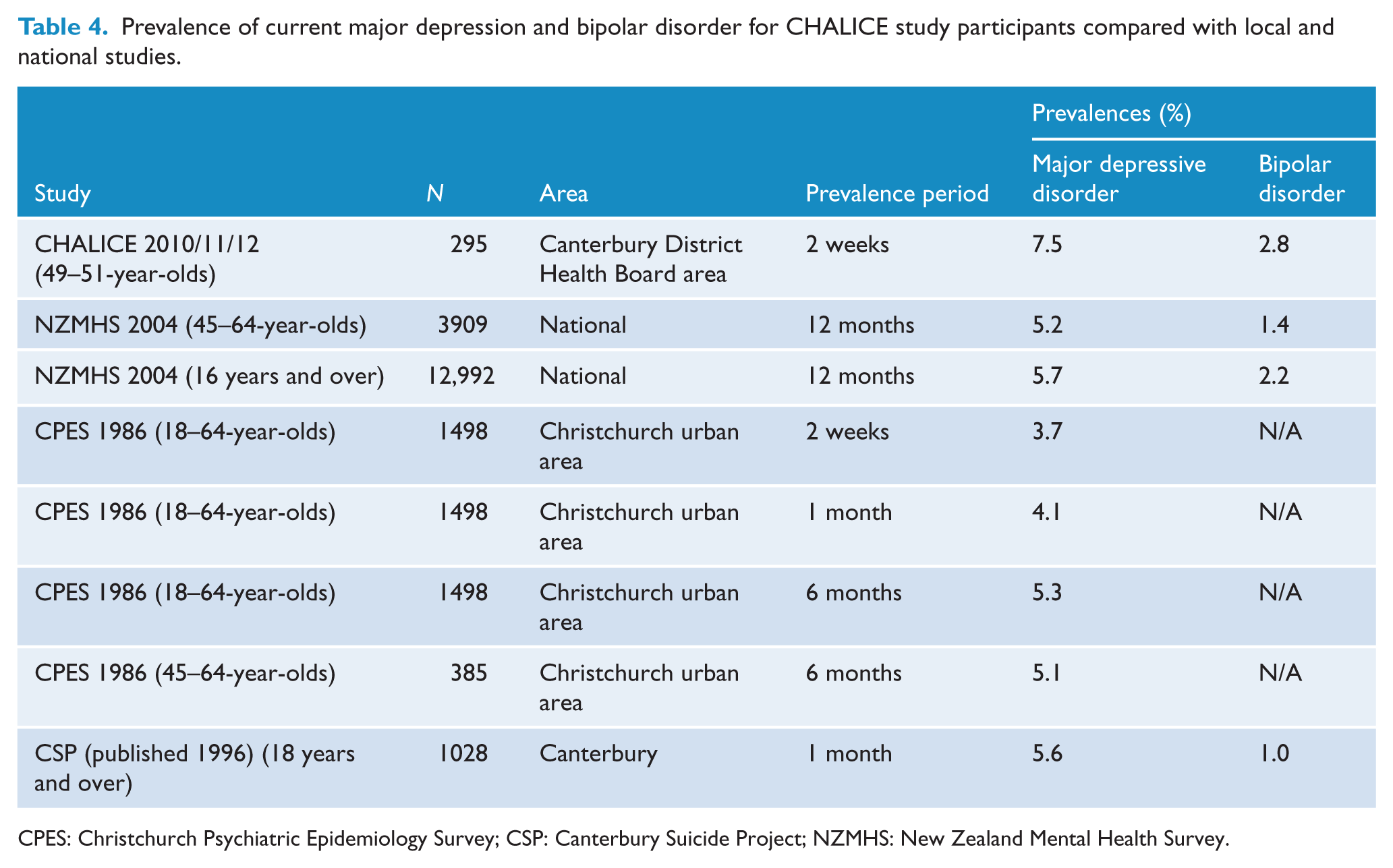
CPES: Christchurch Psychiatric Epidemiology Survey; CSP: Canterbury Suicide Project; NZMHS: New Zealand Mental Health Survey.
The results for bipolar disorder show a similar pattern. The 2 week prevalence for the CHALICE study is 2.8% compared with that of the NZMHS 12 month prevalence which is 2.2% for 16 years and over and 1.4% for 45–64-year-olds. In the CHALICE sample 89% of those with current bipolar were classified as bipolar I. We compared the current prevalence of bipolar disorder with the most comparable prevalence previously reported for this area, i.e. NZMHS in 45–64-year-olds and the difference between the rates was not significant.
Discussion
We have demonstrated that mental but not physical health was significantly worse than pre-earthquake population norms for the earthquake-affected Canterbury population. We have reported that 50-year-olds living in post-earthquake Christchurch have significantly lower scores on the mental health, role-emotional, social functioning and vitality scales of the SF-36v2 compared to national data; but not on physical functioning, role-physical, bodily pain or general health. In addition this sample of 50-year-olds was assessed as having 7.5% prevalence of current major depressive disorder and a bipolar disorder prevalence of 2.8% over the past 2 weeks. The prevalence rates were not significantly higher than historical studies of similar geographical populations.
This study did not replicate the findings of a study conducted after the 2008 Wenchuan earthquake, which found significant differences between all eight subscale scores of the SF-36 for earthquake survivors as compared to previously derived population norms (Ke et al., 2010). In Christchurch only the mental health subscales were significantly different and we suggest that this may be because of differences in actual or perceived threat of physical danger. It may be that Christchurch residents are experiencing more secondary stressors, which affect their mental but not their physical health, as opposed to primary stressors such as fearing for one’s life or being injured (Lock et al., 2012). Many secondary stressors, for example economic challenges, stress arising from repairs to the home or rebuild, or the continued lack of infrastructure, are avoidable or modifiable (Lock et al., 2012). In order to alleviate the burden of survivors local authorities and health professionals need to be aware of the role of secondary stressors and develop plans to address these potential problems in the aftermath of a disaster.
For people who live in Christchurch these significant mental health impacts are not unexpected, and are consistent with other studies on post-earthquake effects (Ke et al., 2010; Wu et al., 2006). However, contrary to many studies (Chou et al., 2004b; Ke et al., 2010; Wu et al., 2006; Zhang et al., 2012), the mental health impacts were not more marked in women than men. This finding may reflect cultural differences in accepting psychological stresses or may be because of differences in the age of the participants. CHALICE study participants are 49–51 years old, an older age group compared to the samples used by the other studies. It’s possible that the more mature age of the CHALICE sample mean they are a group that are more willing to disclose their feelings in a study of this type or that, in this age group, gender differences are not evident.
An interesting aspect to the results is the age of the CHALICE group in relation to previous SF-36 research. The 2006/7 New Zealand Health Survey shows that the means for the physical subscales of the SF-36 decrease with age while the mean mental health subscale scores rise with age, peak in middle age and decline again in old age (Ministry of Health, 2008). The results presented here are for a middle-aged cohort and, if the change in scores holds true for older or younger age groups, then their mental health related quality of life scores may be even lower. However, many previous studies on the effects of earthquakes on quality of life show that the effects are more marked with age (Chou et al., 2004b; Ke et al., 2010). One study found that the psychological impact of earthquakes was strongest in the 54–70-year-old age group and that people above that age seemed to be more resilient (Chou et al., 2004a). Further research into the effects for specific age groups is warranted.
We have also reported that, for a subset of the CHALICE sample, the adverse mental health impacts are not related to death of a family member or close friend or to the extent of damage to the house. These findings are consistent with mental health impacts being more related to secondary effects from the earthquakes such as dealing with insurance companies, problems with recovery and rebuilding of homes and ongoing disruptions.
While having salient strengths, the reported findings also have limitations, including that the comparison groups are historical rather than current. However, when recruiting to this longitudinal study, which began only days before the first earthquake, a comparison was never planned or available. To negate this limitation, the most recent valid and reliable datasets available for a similar geographical area were selected for the comparison group. While completion of the SF-36 should be comparable across different studies, diverse methods were used for collecting the data for major depressive disorder and bipolar disorder, i.e. the MINI (Sheehan et al., 1998), used in CHALICE as opposed to Composite International Diagnostic Interview 3.0 (Kessler et al., 2004) used in the NZMHS. The CHALICE study used recurrent brief hypomanic episodes as inclusion criteria for bipolar which the comparison studies did not. Also, all of the studies used for comparison had different prevalence periods and age groups, making strictly meaningful comparisons difficult.
The limited age range of the CHALICE study cohort is a strength, as it essentially removes age as a confounding variable. Additionally, at 50 years of age, this group is neither a young nor old sample and they may be more stable and financially secure than a younger sample. Furthermore, the study cohort was a random sample selected to take part in a study unrelated to earthquake research and the response rate was 64%. In the face of this good recruitment rate, despite the ongoing disruption to the population of Canterbury, and that the CHALICE cohort SF-36v2 physical functioning subscale mean was largely no different from the age-matched national figures, any recruitment bias is likely to be modest.
There have been adverse mental health impacts on both middle-aged men and women in Christchurch following the earthquakes. Even 18 months after the first earthquake the significant adverse impact on mental health clearly continues. Future emergency management planning for earthquakes and possibly other disasters may expect that, even in the absence of massive casualties and homelessness, there will be enduring mental health effects for the local population. Of this sample, 5.1% scored below two standard deviations of the national mean and this group of people may be particularly vulnerable and need access to specialist mental health services. Authorities may be able to reduce stress and burden of survivors by faster resolution of secondary stressors such as earthquake-related insurance claims and by effective planning of mental health services in the long term.
The major implications of these findings relate to the need for ongoing provision of additional mental health services, whether via primary care or specialist mental health services, to the people of Canterbury. Further, an understanding of the ongoing adverse mental health effects in relation to other social policies, including faster resolution of insurance-related earthquake claims and a faster rebuild of the city remains necessary and fundamental.
Footnotes
Acknowledgements
We thank all the CHALICE study participants who gave their time so readily during a difficult period. We thank Bridget Kimber and Robyn Abbott for participant care, Monica Johnstone for data management and to Anna Thorpe and Julia Martin for their contribution to data collection.
Funding
The CHALICE study is supported by grants awarded from the Department of Internal Affairs’ Lotteries Health (grant number: AP265022), Canterbury Community Trust, Otago Thyroid Research Foundation and University of Otago Foundation Trust (grant number: TL1060).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.