
Abstract
Aims:
There is very little empirical evidence about the relationship between severe mental illness and the physical health of Indigenous peoples. This paper aims to compare the physical health of Māori and non-Māori with a diagnosis of bipolar disorder in contact with NZ mental health services.
Methods:
A cohort of Māori and non-Māori with a current bipolar disorder diagnosis at 1 January 2010 were identified from routine mental health services data and followed up for non-psychiatric hospital admissions and deaths over the subsequent 5 years.
Results:
Māori with bipolar disorder had a higher level of morbidity and a higher risk of death from natural causes compared to non-Māori with the same diagnosis, indicating higher levels of physical health need. The rate of medical and surgical hospitalisation was not higher among Māori compared to non-Māori (as might be expected given increased health needs) which suggests under-treatment of physical health conditions in this group may be a factor in the observed higher risk of mortality from natural causes for Māori.
Conclusion:
This study provides the first indication that systemic factors which cause health inequities between Māori and non-Māori are compounded for Māori living with severe mental illness. Further exploration of other diagnostic groups and subgroups is needed to understand the best approach to reducing these inequalities.
Background
Premature mortality is increased among those with severe mental illness, including schizophrenia and bipolar disorder, mainly due to premature deaths from chronic physical health conditions (Cunningham et al., 2014; Druss et al., 2011; Firth et al., 2019). Cardiovascular disease has been identified as the main potentially avoidable contributor to premature deaths in people with bipolar disorder or schizophrenia (Correll et al., 2017). Systemic factors including discrimination relating to disadvantaged status are important in understanding health inequities, and multiple disadvantage (such as experience of mental illness and non-dominant ethnicity) can lead to cumulative impacts on health (Grollman, 2014). However, the relationship between severe mental illness and physical health in non-dominant ethnic groups is not well understood (Das-Munshi et al., 2016).
Studies examining differences by ethnicity in the mortality gap between people with severe mental illness and the general population have generally reported higher SMRs (standardised mortality ratios) for natural and external causes among dominant compared to non-dominant ethnic groups (Das-Munshi et al., 2017; Daumit et al., 2010; Musuuza et al., 2013; Olfson et al., 2015). This lower effect of severe mental illness among non-dominant ethnic groups appears surprising but may relate to higher baseline rates of mortality among the general population in non-dominant ethnic groups.
It is less clear how rates of premature mortality and other markers of physical health vary between ethnic groups with severe mental illness. The few studies which report differences by ethnicity or race report conflicting findings, with some evidence of a lower risk of mortality for non-dominant ethnic groups compared to dominant ethnic groups (Das-Munshi et al., 2017, 2020), while other studies point to a similar or higher risk of mortality among non-dominant compared to dominant groups with severe mental illness (Daumit et al., 2010; Piatt, 2011). There is some evidence of higher rates of comorbid physical health conditions among non-dominant compared to dominant ethnic groups with severe mental illness (Carliner et al., 2014; Mangurian et al., 2017).
In New Zealand, the Indigenous Māori population have a higher incidence of severe mental illness than other ethnic groups, as well as a reduced life expectancy (Baxter et al., 2006; Kake et al., 2008; Ministry of Health, 2019). There is also clear evidence of reduced life expectancy among those with severe mental illness in New Zealand (Cunningham et al., 2014). However, the cumulative systemic impacts of living with severe mental illness on physical health morbidity and mortality within Māori communities has not been explored. This study investigates the physical health of Māori with a diagnosis of bipolar disorder and seeks to understand whether Māori with bipolar disorder are exposed to systemic factors that impact their physical health compared to non-Māori New Zealanders with the same diagnosis. Three indicators of physical health were considered: level of physical condition multimorbidity, the risk of non-psychiatric (medical or surgical) hospital admission and the risk of death due to natural causes, the latter enabling us to build on previous international research which has focused on mortality.
Methods
The Programme for the Integration of Mental Health Data (PRIMHD) is a national data set including all contacts with secondary mental health services in New Zealand since July 2007. PRIMHD was used to identify a prevalent cohort of Māori and non-Māori patients with a recorded diagnosis (principal, other relevant or provisional) of Bipolar Disorder (ICD10 F31.0 - F31.9 or DSMIV 296.0 - 296.89) open at 1 January 2010. The cohort was limited to age 18 to 64 at the cohort inception date because of incomplete data on mental health service use over the age of 65 (Cunningham et al., 2019).
This cohort was followed (via their unique identifier) for a 5-year period in the PRIMHD data (to the 31 December 2014). PRIMHD data were also linked by encrypted National Health Index (NHI) identifier to the National Minimum Data Set (NMDS) and mortality collections to identify hospitalisation and mortality during follow-up. Follow-up time was calculated from the index date (1 January 2010) to the end of the study period (31 December 2014). Individuals who died during this follow-up period contributed time-at-risk from the index date to their date of death.
Variables
Ethnic group, as recorded on health service data, was used to identify Māori service users. Individuals are given the opportunity to self-identify ethnic affiliation at each health service contact, and up to three ethnicities can be recorded in the master NHI data source. The analyses presented here compare those with any reported Māori ethnicity (irrespective of any other recorded ethnicities) with all other (non-Māori) service users (Ministry of Health, 2017).
Outcomes
The M3 multimorbidity index quantifies the level of morbidity, or the degree to which an individual is experiencing multiple chronic conditions, using diagnoses recorded in hospitalisation data (ICD10 codes), with 55 conditions weighted by contribution to risk of mortality (more fatal conditions being weighted higher) (Stanley and Sarfati, 2017). An adapted version of the M3 score was used, excluding psychiatric conditions from the weight calculation. M3 score was categorised for descriptive analyses (categories 0, 0 to <1, 1 to <2, 2 to <3 and 3+) and used as a continuous variable to adjust for multimorbidity as a confounder in regression analyses. Where a patient has an M3 score of 0, none of the 55 chronic conditions have been recorded by hospital services. A score of 0 to <1 represents a small number of recorded conditions not highly predictive of mortality (e.g. uncomplicated diabetes and hypertension). A score of 2 or 3 could represent having a large number of chronic conditions or a small number of conditions which are highly likely to be fatal (e.g. a diagnosis of lung cancer gives a score of 1.97, while a combination of diabetes, obesity, liver disease, peripheral vascular disease and chronic kidney disease would give a similar score).
Hospitalisations during follow-up were identified from the NMDS data set, which records all publicly funded hospital stays with a duration of 3 or more hours. Hospitalisations were categorised into medical (including rehabilitation), surgical, psychiatric and other types (maternity, emergency department) using the Health Specialty Code in the NMDS. Maternity admissions were excluded since these do not represent an adverse physical health event. For regression analyses, medical and surgical admissions were combined into a single category to increase the power of the analysis.
Cause-specific mortality was identified from the national mortality collection. Mortality was categorised into external causes (ICD codes starting with an X, including accidental and self-inflicted injury) and medical or natural causes (all other ICD codes).
Covariates
Gender and date of birth were identified from the master NHI data set. Social deprivation was assessed using NZDep 2013 quintiles, an area-based measure of deprivation based on information from the 2013 NZ census, where 1 represents the least deprived areas and 5 the most deprived areas (Atkinson, 2014).
Psychiatric diagnoses were identified from the PRIMHD data set for diagnoses recorded as open at the baseline date. In New Zealand, for inpatient admissions, coding of diagnosis is carried out by trained coders who code the diagnoses based on a set of rules applied to the clinical file. For outpatient specialist care, at discharge or after 3 months of care, a diagnosis must be entered by clinicians based on a clinical diagnosis. Bipolar affective disorder diagnoses were categorised into BPAD 1 (ICD F31.0-F31.7; DSMIV 2960, 2964-67), BPAD II (ICD10 F31.81; DSMIV 29689) and BPAD not otherwise specified (NOS) (ICD10 F31.9; DSMIV 29680). Where multiple BPAD diagnoses had been recorded, diagnoses were prioritised in the order BPAD I, BPAD II, BPAD NOS in order to identify the most severe and specific diagnosis for each individual. Comorbid psychiatric diagnoses were also identified from PRIMHD and categorised into functional psychoses, alcohol use disorders, other substance use disorders, depression, anxiety, personality disorders (see Supplementary Material for codes).
Analysis
Descriptive analyses, stratified by ethnicity, compare sociodemographic factors and clinical characteristics between Māori and non-Māori patients. Chi-square tests of difference were performed.
Cox proportional hazards regression was used to compare risk of hospitalisation for physical health conditions (medical and surgical admissions) by ethnicity, adjusted for demographic confounders (age, sex, deprivation) and multimorbidity profile at baseline (M3 index score). The proportional hazards assumption was confirmed as reasonable through visualisation of survival curves. Analysis followed individuals until first hospitalisation, with follow-up time censored at the study end date (31 December 2014) or date of death (for patients who died prior to 31 December 2014).
Cox regression was also used to compare risk of death from external causes and natural causes (separate cause-specific analyses) by ethnicity, adjusted for demographic confounders (age, sex, ethnicity) and multimorbidity (for natural causes only). For each cause-specific mortality analyses, follow-up time was censored at the study end date or date of death from another cause (for patients who died prior to 31 December 2014: e.g. patients dying from external causes were censored in the natural causes analysis).
Data cleaning and analysis was performed using SAS 9.4.
Results
A total of 3938 people were identified from PRIMHD mental health service records as being alive with an open diagnosis of bipolar disorder (at index date of 1 January 2010), of whom 828 (21%) were Māori. For all analyses, the cohort was limited to those aged 18–64 at 1 January 2010 (n = 3428; n = 777 Māori, 23%).
Table 1 shows the distribution of demographic and clinical factors by patient ethnicity. Māori using services for bipolar disorder were younger and living in much more deprived circumstances, with nearly half living in areas in the most deprived quintile. Māori were more likely to have a Bipolar 1 diagnosis, and more commonly had a comorbid diagnosis recorded for another psychotic, alcohol or substance use disorder. Physical morbidity scores were higher among Māori than non-Māori (mean score 0.55 Māori, 0.33 non-Māori).
Cohort demographic and clinical characteristics by ethnicity.
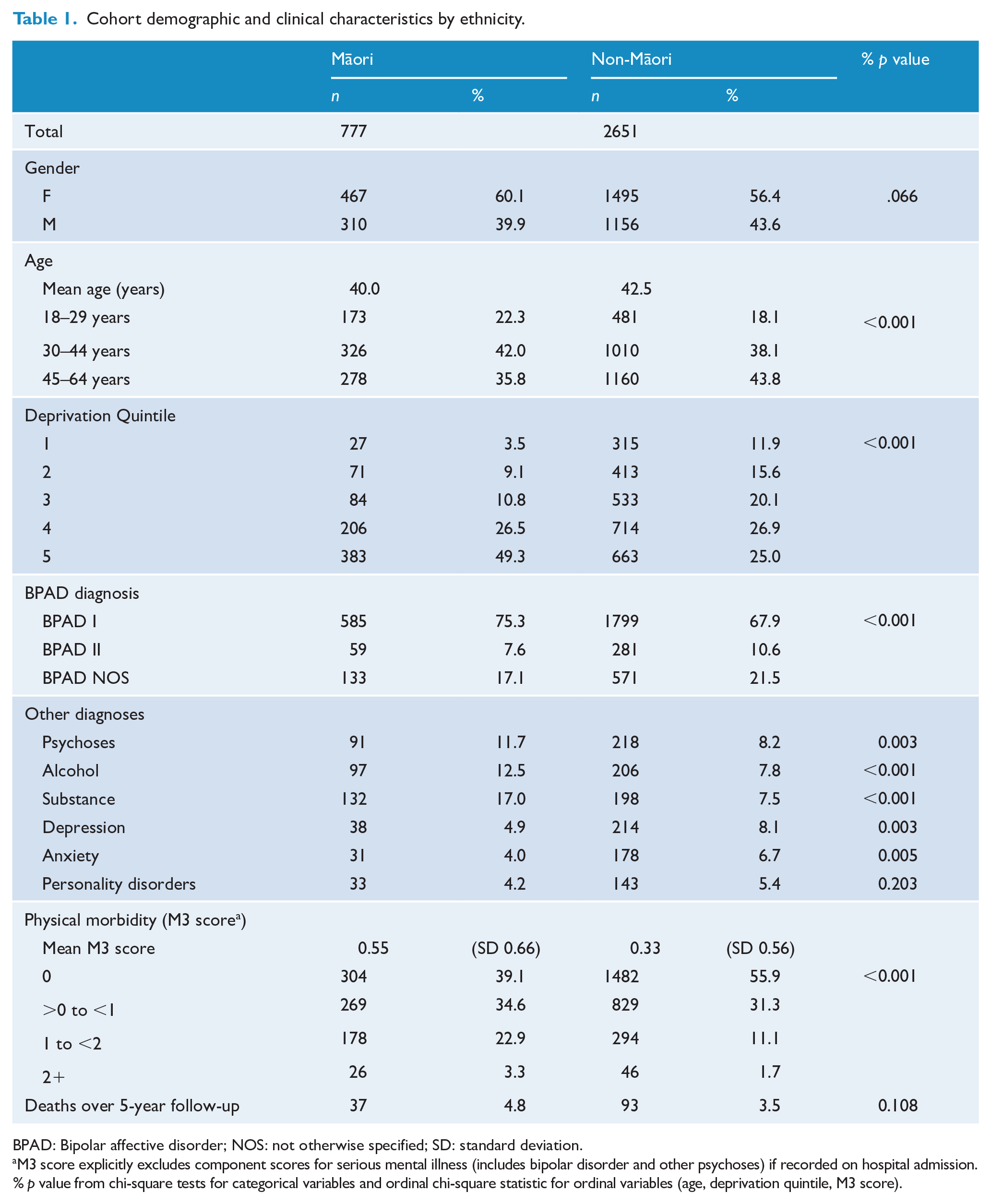
BPAD: Bipolar affective disorder; NOS: not otherwise specified; SD: standard deviation.
M3 score explicitly excludes component scores for serious mental illness (includes bipolar disorder and other psychoses) if recorded on hospital admission. % p value from chi-square tests for categorical variables and ordinal chi-square statistic for ordinal variables (age, deprivation quintile, M3 score).
Over the follow-up period, 51% of the cohort (417 Māori, 1326 non-Māori) were admitted to non-psychiatric inpatient services. Table 2 shows differences in risk of medical or surgical admissions over the follow-up period by ethnicity. The crude risk of admission was marginally higher for Māori compared to non-Māori (hazard ratio [HR]: 1.12; 95% confidence interval [CI] = [1.01, 1.26]), but after adjustment for confounders, there was no difference in risk of admission between Māori and non-Māori (HR: 1.00; 95% CI = [0.89, 1.3]).
Risk of admissions (combined medical and surgical admissions) during follow-up for Māori compared to non-Māori people with bipolar disorder.
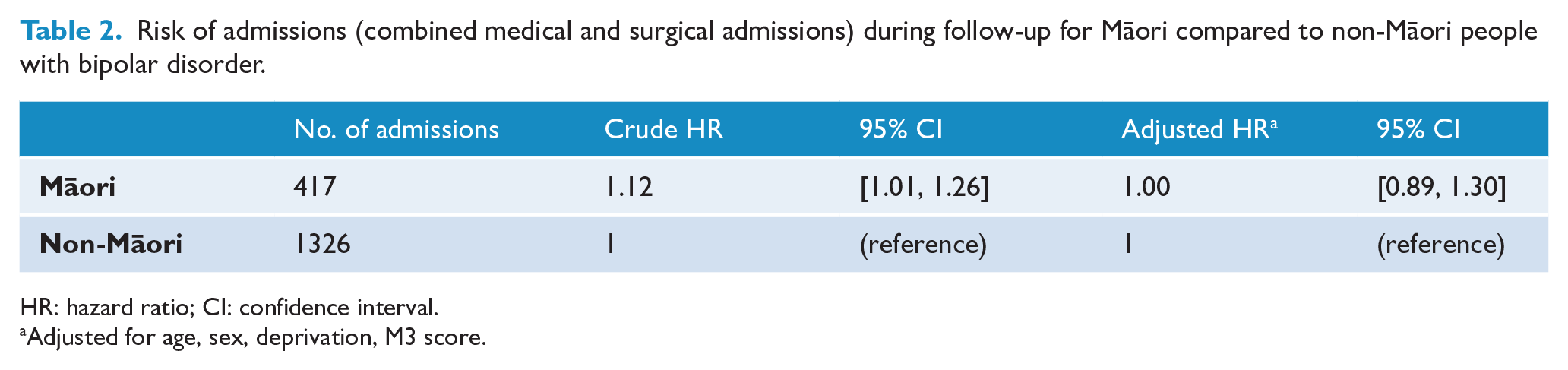
HR: hazard ratio; CI: confidence interval.
Adjusted for age, sex, deprivation, M3 score.
A total of 130 people died over the follow-up period (37 Māori: 21 men, 16 women; 93 non-Māori: 54 men, 39 women). Most of these deaths were from natural causes: 90 deaths were recorded as due to physical health conditions including cancer (27), cardiovascular disease (29) and other natural causes (primarily diabetes, respiratory disease and neurological conditions). The remaining 40 deaths were from external causes, including 25 recorded as suicide.
Table 3 shows the differences in risk of death over follow-up by ethnicity, split into natural causes and external causes. The risk of death from natural causes was higher among Māori compared to non-Māori with bipolar disorder. This difference was stronger after adjustment for demographic confounders (HR: 2.14, 95% CI = [1.36, 3.39]). When further adjusted for level of physical multimorbidity, the risk of death remained 52% higher, although the CI no longer excluded the null (HR: 1.52, 95% CI = [0.96, 2.41]).
Risk of death during follow-up from natural causes and external causes for Māori compared to non-Māori people with bipolar disorder.
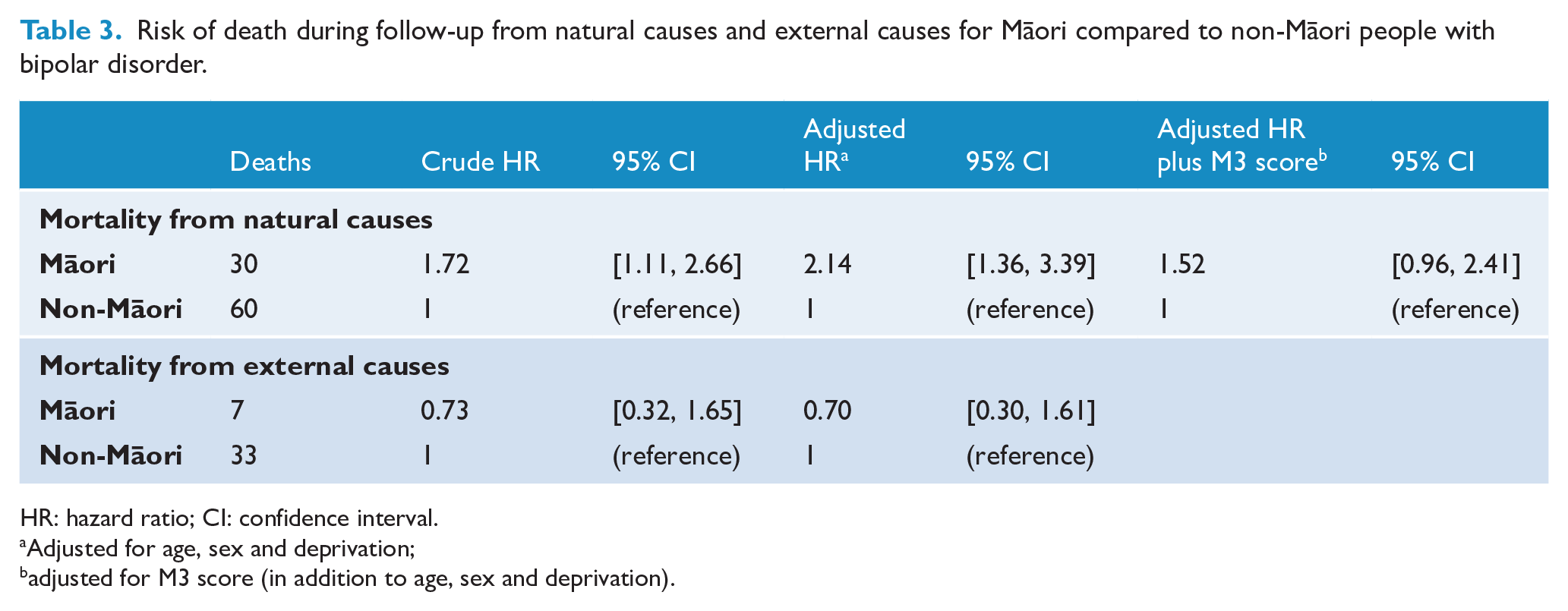
HR: hazard ratio; CI: confidence interval.
Adjusted for age, sex and deprivation;
adjusted for M3 score (in addition to age, sex and deprivation).
Risk of death from external causes was not significantly different between Māori and non-Māori (HR: 0.73, 95% CI = [0.32, 1.65]) and did not change with adjustment for demographic confounders (HR: 0.7, 95% CI = [0.3, 1.61]). However, the CIs for these estimates were wide and included substantively important differences between groups.
Discussion
This paper is the first to examine the relationship between severe mental illness and physical health for the Indigenous peoples of New Zealand. We found a higher level of physical morbidity and a higher risk of death from natural causes among Māori with bipolar disorder compared to non-Māori with the same diagnosis. However, the rate of medical and surgical hospitalisation was not higher among Māori compared to non-Māori (as might be expected given increased health needs) which suggests under-treatment of physical health conditions in this group may be a factor in the observed higher risk of mortality from natural causes for Māori with severe mental illness.
The high degree of physical morbidity (as assessed by the M3 index) is in keeping with previous research showing high levels of cardiovascular risk factors among those from non-dominant ethnic populations who experience severe mental illness (Carliner et al., 2014; De Caluwé et al., 2019). The higher M3 scores seen for Māori relative to non-Māori with bipolar disorder were consistent with differences found between ethnic groups in other populations defined by specific diseases. For example, among those with a cancer diagnosis, non-Māori have lower rates of comorbidity compared to Māori, and this partly explains differences in mortality (Brewer et al., 2011; Hill et al., 2010). However, adjusting risk of mortality from natural causes for physical morbidity (M3 index score) only partially explained ethnic disparities among this population of people with bipolar disorder. Systemic factors including racism are likely to be important in understanding the remaining differences in mortality.
The findings of increased risk of mortality from natural causes for Māori with bipolar disorder compared to non-Māori are inconsistent with a recent London-based study, which found that among those with severe mental illness, people of Black non-dominant ethnicity had lower all-cause mortality than those in dominant White ethnic groups (Das-Munshi et al., 2017). This discrepancy may relate to the different contexts of the two studies, including the different non-dominant ethnic groups in the population. The small urban geographic setting for the UK study (with a more uniform distribution of other determinants of survival, including level of socioeconomic deprivation and health service access) compared to the broad national setting of this study may also be important.
Moreover, while the overall finding was of higher premature mortality rates of Māori compared to non-Māori with bipolar disorder, there will also be variation in the risk of premature mortality among Māori with bipolar disorder. Further analysis of the London cohort described above revealed that risk of mortality varied by ethnic density, with people from non-dominant ethnic populations living in the most ethnically dense areas having the lowest all-cause mortality compared to the British White population rate (Das-Munshi et al., 2019). This raises the possibility of a protective effect among non-dominant populations that may be associated with neighbourhood context and social connection (Susser and Kirkbride, 2019).
A recent New Zealand study found that speaking Te Reo Māori (the Indigenous language) was associated with a reduced risk of progression from pre-diabetes to diabetes (Teng et al., 2019), similarly suggesting a protective effect on health arising from strength of social connection and connection with culture. High Māori ethnic density has also been found to be associated with high self-rated health and lower experience of discrimination, although this protective effect is masked by the strong negative effect of area-level deprivation (Bécares et al., 2013), suggesting that system-level factors may diminish any benefit of living in ethnically dense communities. It will therefore be important to explore the relationship between mental health and physical health among Māori further in the NZ context. For example, such research could consider whether the impact of severe mental illness on physical health is reduced in areas where connection to culture is stronger and/or in more ethnically dense areas, and to understand the system-level factors by which ethnic density impacts on health.
Persistent unequal health system access and outcomes for the Indigenous peoples of New Zealand are widely acknowledged (Goodyear-Smith and Ashton, 2019). In particular, the role of ongoing colonisation, including racism within the health system, as a risk factor that contributes to health inequities is increasingly recognised as a driver of health outcomes (Harris et al., 2012, 2019; Reid et al., 2019). The current results are in keeping with past studies, particularly the finding that Māori with bipolar disorder did not have higher rates of hospital admission despite having indicators suggesting higher need including higher rates of substance use and physical comorbidity. This is similar to other studies; for example, a large cohort study found that the Māori rate of hospitalisation for cardiovascular disease was lower than expected given the high rates of cardiovascular mortality (Grey et al., 2018).
Strengths and limitations
This study uses data from a complete national cohort of people in contact with public specialist mental health services for bipolar disorder. There is very little private psychiatric treatment in New Zealand and so public data provide a relatively complete picture. The use of linkage to national routine data sets enables almost complete ascertainment of outcomes (publicly funded hospital admissions and deaths). The collection of high-quality ethnicity data by health services in New Zealand (Cormack and McLeod, 2010) allows for valid comparisons by ethnic group.
There is some potential for missing outcomes in these kinds of data. Privately funded hospital admissions for physical treatment are not fully captured in the national data collections, and hospital admissions or deaths overseas would also not be recorded. However, these are relatively rare, particularly among people utilising secondary mental health services for bipolar disorder, for economic reasons. Moreover, any expected differences in these outcomes would be anticipated as producing a greater extent of missing outcome data among non-Māori compared to Māori, driven by socioeconomic factors. This might lead to underestimation of non-Māori rates of hospitalisation (as the most plausibly affected outcome), which strengthens our finding of lower than expected hospitalisations among Māori.
The prevalence estimates for psychiatric comorbidities in this study may represent underestimates, as diagnoses are not always completely recorded in the PRIMHD system. Diagnosis and coding of mental disorders may be subject to observer bias, including bias by ethnicity (Arnold et al., 2004), and so recording of comorbid diagnoses may vary by ethnicity. This means differences in psychiatric comorbidity by ethnicity (such as alcohol and substance use) should be interpreted with caution. However, the M3 index includes physical conditions caused by alcohol and substance use disorders and will be less subject to observer bias, and so adjustment of mortality analyses will largely control for any impact of differences in alcohol and substance use on physical health.
We used a prevalent cohort design – that is, individuals in the study were at different stages of mental illness at the study index date. This is the only pragmatic course for a large-scale study interested in physical outcomes (rather than focussed on early-stage outcomes for people recently diagnosed with serious mental illness), but this does mean that the results are a blend of outcomes for people across the range from recently diagnosed individuals through to people with considerable years of living with severe mental illness.
The M3 index relies on hospital discharge data to identify diagnoses of physical health conditions (collated in a 5-year period prior to the index date) and is therefore likely to underestimate the overall level of morbidity in populations with reduced access to health services, and potentially miss conditions prone to diagnostic overshadowing. These might both apply among those with severe mental illness (Jones et al., 2008; Knaak et al., 2017), potentially resulting in overall underestimation of M3 scores but not necessarily biasing the comparisons between these two groups with severe mental illness.
Most people with bipolar disorder access public secondary mental health services; however, data from primary care were not included in this study. Similar analyses of primary care services would assist in identification of possible under-recognition and under-treatment of physical comorbidities.
Data on individual measures of deprivation such as income were not available in the routine data used for this study. Individual-level deprivation may play a stronger role in explaining ethnic differences in outcomes than area-level deprivation, and thus the presented results may be subject to residual confounding by deprivation.
Implications
This study provides the first indication that Māori with severe mental illness are disadvantaged with respect to their physical health due to the cumulative impact of greater lifelong exposure to risk factors that affect health coupled with inequitable access to and through health services. This finding is in contrast to studies from the United Kingdom, which suggest that non-dominant populations with severe mental illness have lower mortality rates than dominant White groups with severe mental illness (Das-Munshi et al., 2017, 2020). Further work is needed to explore the physical health of Māori with other mental health diagnoses and also to examine other measures of physical health such as cardiovascular disease incidence and survival in order to better understand the factors contributing to higher mortality. Exploration of the relationship between measures of access to cultural resources such as ethnic density and the physical health of people experiencing mental illness will also be important in understanding how best to address the inequities found.
Supplemental Material
Supplementary_material – Supplemental material for The physical health of Māori with bipolar disorder
Supplemental material, Supplementary_material for The physical health of Māori with bipolar disorder by Ruth Cunningham, James Stanley, Tracy Haitana, Suzanne Pitama, Marie Crowe, Roger Mulder, Richard Porter and Cameron Lacey in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was funded by the Health Research Council of New Zealand, Rangahau Hauora Māori (ref ID: 16/338).
Ethical and Data Availability
This study was approved by the New Zealand Health and Disability Ethics Committee (ref:16/STH/137). The data used in this study are held by the New Zealand Ministry of Health and are available on request to researchers with appropriate ethical clearance.
Supplemental Material
Supplemental material for this article is available online.