
Abstract

Keywords
Introduction
Clarification is needed around the use of cannabis in chronic pain. In Australia and New Zealand, general practitioners are routinely faced with patients who smoke cannabis for ‘so called’ medicinal reasons.
Criminal drug laws in all Australian States continue to prohibit the possession, cultivation and supply of cannabis – even for medical purposes. In Australia, a parliamentary committee is recommending that the New South Wales Government amend legislation to allow the medical use of cannabis by patients with a terminal illness and those who have moved from HIV infection to AIDS (Legislative Council, 2013). The recommendation, if adopted by the Government, will allow patients with specific medical conditions certified by their specialist treating medical practitioner to possess and use up to 15 grams of dry cannabis or the equivalent amount of other cannabis products and equipment (Legislative Council, 2013). The inquiry by the Legislative Council’s General Purpose Standing Committee No. 4 was established in November 2012 to examine the efficacy and safety of cannabis for medical purposes. The Committee believed that people who are at the end of their life and take measures to either relieve their severe pain or stimulate their appetite should not be criminalised (Legislative Council, 2013).
The medicinal use of cannabis has been much debated in New Zealand. It has been estimated that 13.4% of those between the ages of 16 and 64 years in New Zealand use cannabis (United Nations Office on Drugs and Crime, 2006). In New Zealand, the use of cannabis is governed by the Misuse of Drugs Act 1975. Unauthorised possession of any amount of cannabis is illegal. In 2006, Metiria Turei from the New Zealand Green Party proposed the ‘Misuse of Drugs (Medicinal Cannabis) Amendment Bill’, whereby cannabis would be allowed for medicinal use (New Zealand Parliament, 2009). The bill was defeated.
Calls are being made for the legalisation of cannabis, citing its compassionate use for alleviation of a number of ailments. The Law Commission’s Issues Paper on ‘Controlling and Regulating Drugs’ recommends those suffering from chronic or debilitating illnesses be able to use cannabis under medical supervision, particularly where conventional treatment options have proven ineffective (Law Commission, 2010).
Pressure is being placed on the judicial system to condone its medicinal use. In March 2012, Victoria Davis was discharged without conviction by Judge Tony Zohrab on charges of cultivating cannabis. She grew the plants to help her husband cope with phantom pain. The New Zealand Medical Association does not oppose partial decriminalisation of the use of small amounts for medical purposes, provided it can be shown that no harm would result.
In New Zealand, all injured patients are covered by accident compensation insurance. The Accident Compensation Corporation in New Zealand has been requested to fund synthetic cannabis (nabiximols or Sativex®) for chronic pain, where conventional treatments have failed or are not tolerated. At present, Sativex® is approved for use as an add-on treatment for symptom improvement in unresponsive patients with spasticity due to multiple sclerosis under strict medical supervision after ministerial approval has been granted.
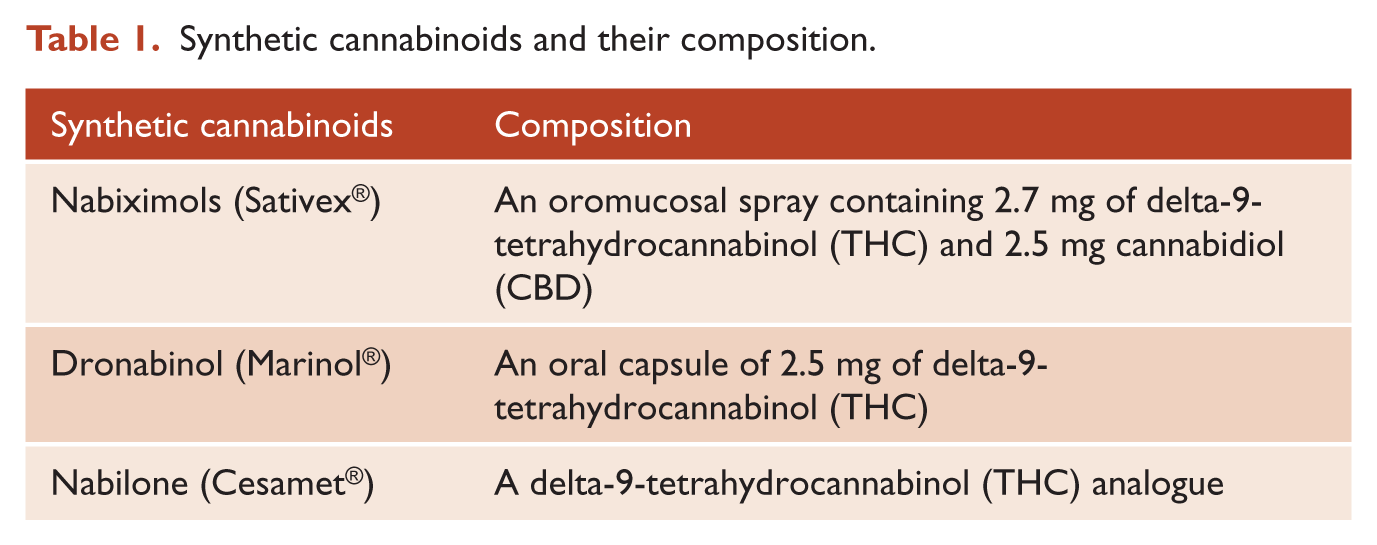
The types of synthetic cannabinoids used are shown in Table 1.
Synthetic cannabinoids and their composition.
Is there evidence that cannabinoids are effective in pain?
There is a paucity of well-designed studies evaluating medical cannabis for pain (Borgelt et al., 2013). Limitations of these studies include widely varying doses and dosage forms of medical cannabis, lack of validated criteria or assessment for some types of pain, lack of comparative trials for various formulations and routes of administration, and small study populations (Borgelt et al., 2013). Hence, a cautious approach is needed. One systematic review has suggested cannabis to be moderately efficacious for chronic pain; its beneficial effects may, however, be offset by potentially serious harms (Martin-Sanchez et al., 2009). Another systematic review suggested that overall cannabinoids were safe and modestly effective in neuropathic pain (Lynch and Campbell, 2011).
Neuropathic pain
Trials indicate that smoked cannabis or cannabis extract tetrahydrocannabinol (THC) / cannabidiol (CBD) can be effective for several different types of pain, primarily neuropathic pain (Borgelt et al., 2013). Seven short-term, placebo-controlled trials have suggested a slight to moderate reduction of neuropathic pain with nabiximols in patients with multiple sclerosis, advanced cancer, rheumatoid arthritis and mixed neuropathies with improved sleep (Podda and Constantinescum, 2012).
In a double-blinded, placebo-controlled, crossover study, Wilsey et al. (2008) demonstrated an analgesic response to smoking cannabis (p = 0.016) in neuropathic pain. In chemotherapy-induced neuropathic pain, a recent pilot study supports the notion that it is worthwhile to study nabiximols in a full randomised, placebo-controlled trial (Lynch et al., 2013).
Ware et al. (2010) studied patients with post-traumatic neuropathic pain. The daily pain intensity was significantly lower for those smoking 9.4% THC compared to placebo. Small limited studies have examined the efficacy of smoked cannabis for neuropathic pain (Wilsey et al., 2008). A recent systematic review found that despite some jurisdictions making allowances for the ‘medical’ use of marijuana by patients with HIV/AIDS, evidence for the efficacy and safety of cannabis and cannabinoids in this setting is lacking (Lutge et al., 2013).
Other painful conditions
Nabilone may be effective for pain related to fibromyalgia but also has not been widely studied (Borgelt et al., 2013). Oral THC (dronabinol) does not appear to be as effective as nabiximols for pain, but has not been widely studied in different pain conditions (Borgelt et al., 2013).
Adverse effects (Table 2)
Cannabinoids present no risk for lethal overdose or end-organ failure. Reported adverse effects are typically not serious. In a systematic review of the use of cannabinoids in pain (Lynch and Campbell, 2011), the most common adverse events were sedation, dizziness, dry mouth, nausea, and disturbances in concentration. However, the psychoactive adverse effects poor co-ordination, ataxia, paranoid thinking, agitation, dissociation, euphoria and dysphoria were noted as well (Lynch and Campbell, 2011). In general, impairments in memory and cognition occur (Borgelt et al., 2013).
Adverse effects of cannabinoids (Borgelt et al., 2013; Lynch and Campbell, 2011; Wang et al., 2008).
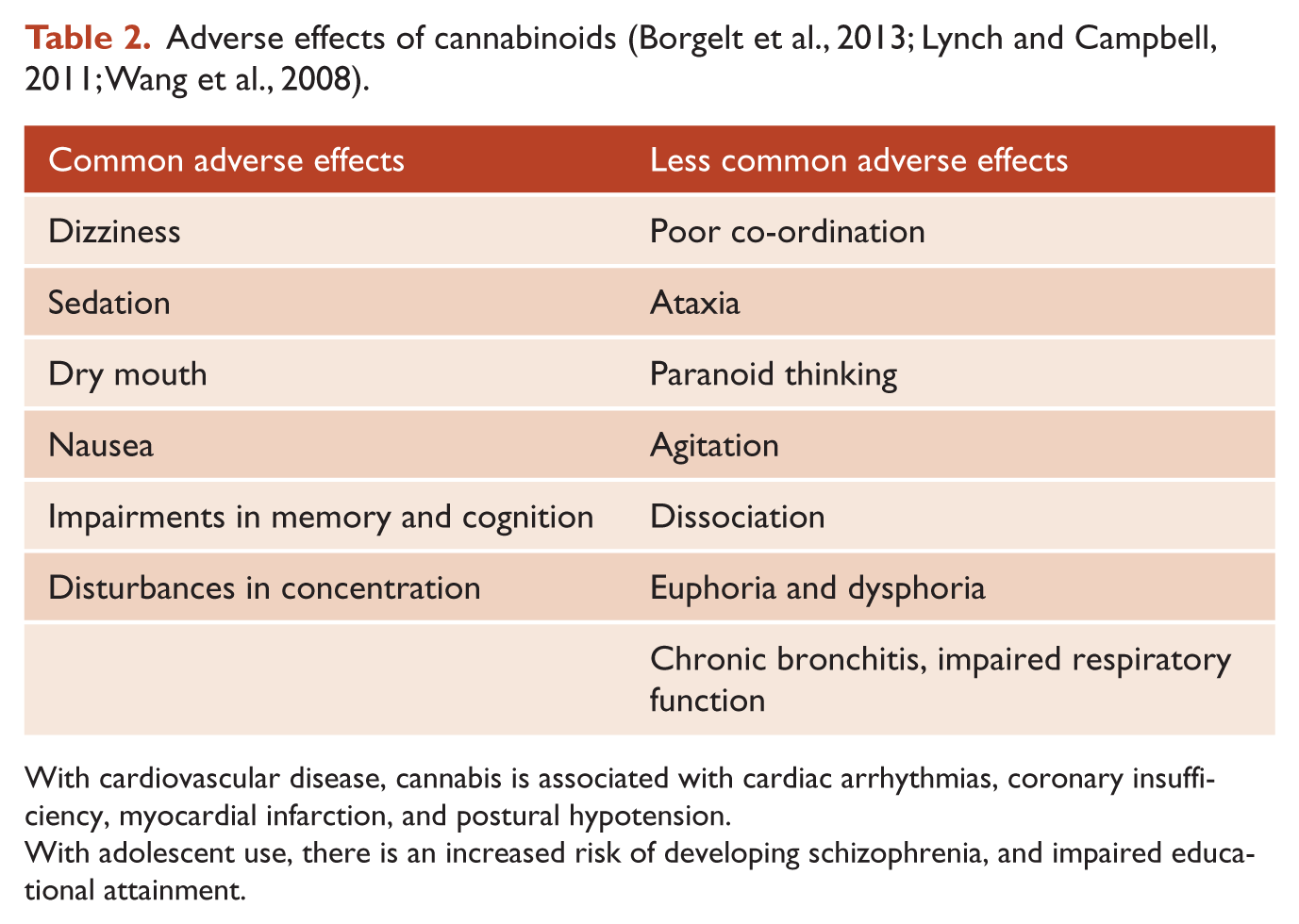
With cardiovascular disease, cannabis is associated with cardiac arrhythmias, coronary insufficiency, myocardial infarction, and postural hypotension.
With adolescent use, there is an increased risk of developing schizophrenia, and impaired educational attainment.
Psychiatric adverse effects
Available data show that heavy cannabis use in adolescence increases the risk of developing psychiatric disorders. In Australia, the use of cannabis is common in young people seeking mental healthcare. In a 10-year Australian follow-up, adolescents who used cannabis occasionally were found to be at higher risk of later drug abuse and educational problems (Degenhardt et al., 2010). There is an increased risk of developing schizophrenia with adolescent use (Borgelt et al., 2013). A recent meta-analysis has provided evidence for a relationship between cannabis use and earlier onset of psychotic illness (Large et al., 2011). Chronic regular cannabis use can produce a dependence syndrome in one in 10 users (Hall and Degenhardt, 2013).
Cognitive functioning
Acute exposure to cannabinoids produces modest transient declines in cognitive performance. Heavy prolonged cannabis exposure may be associated with deficits in memory, sustained attention and executive functioning (D’Souza et al., 2009). Care is needed when prescribing medical cannabis for chronic pain, especially when learning and memory are integral to a patient’s work. Driving and the operation of dangerous equipment would need to be limited. There is a near doubling of risk of a driver being involved in a vehicle collision resulting in serious injury or death after ingestion of cannabis in the previous 3 hours (Asbridge et al., 2012).
Cardiovascular adverse effects
Various reports have associated cannabis with cardiac arrhythmias, coronary insufficiency, myocardial infarction, and postural hypotension; caution is warranted for its use in patients with cardiovascular disease (Leung, 2011).
Other adverse effects
A large Australian study of over 24,000 birthing women showed the use of cannabis in pregnancy to be associated with an increased risk of adverse birth outcomes (Hayatbakhsh et al., 2012). Smoking cannabis is associated with decreasing pulmonary function, and may increase the risk of lung cancer in young adults. Other safety concerns in other countries are accidental paediatric ingestions and lack of safety packaging for medical cannabis formulations (Borgelt et al., 2013).
Is there evidence of efficacy over other medications or where these have failed?
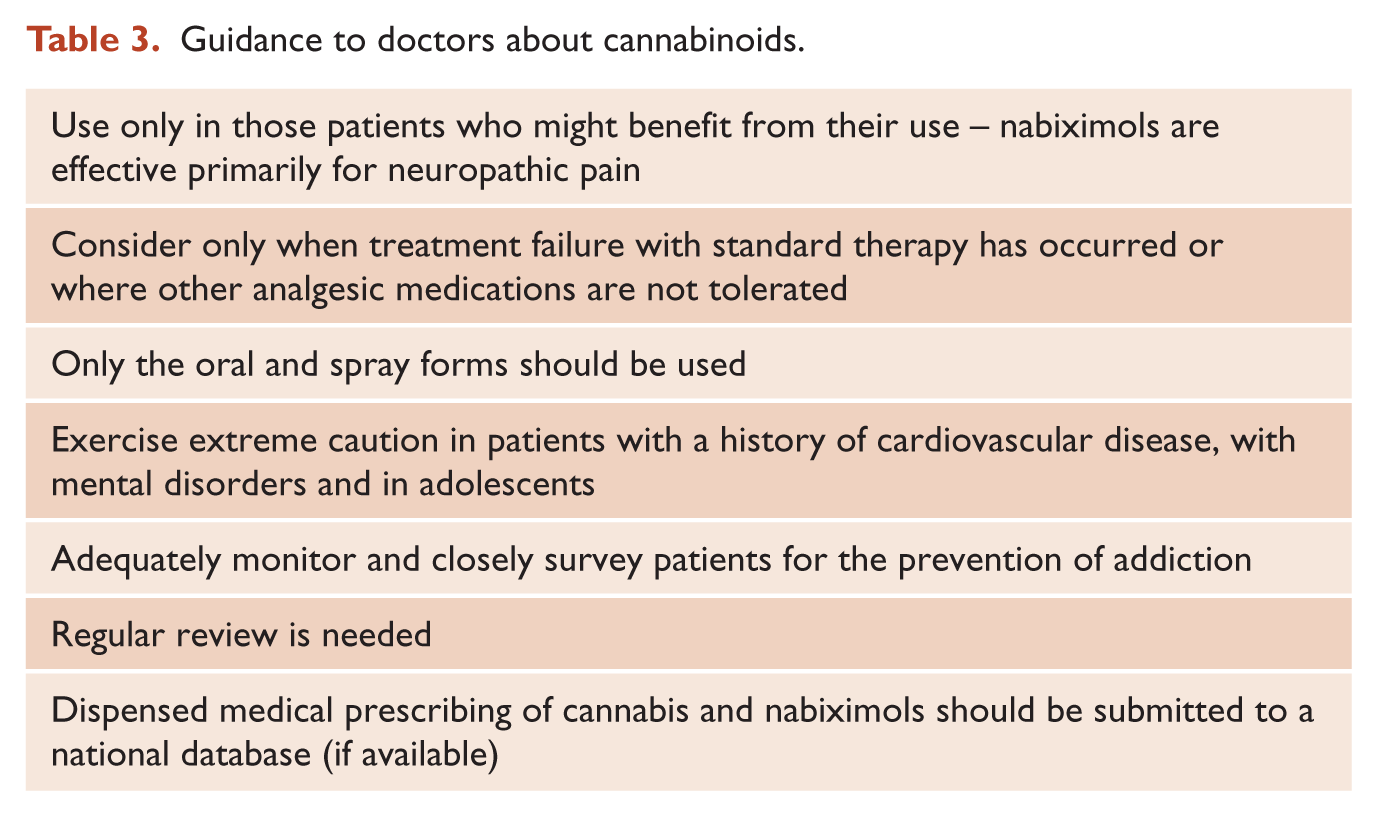
Cannabinoids in general do not offer advantages over current analgesics. Should medical cannabinoids be used at all (Table 3)? Medical cannabinoids appear to have some limited benefits for patients with certain painful conditions, such as those with neuropathic pain from different causes (such as multiple sclerosis).
Guidance to doctors about cannabinoids.
Opioid addiction is a common adverse effect of extended opioid use by chronic pain sufferers. Research suggests that the biological actions of the cannabinoids might prove useful in reducing this opioid dependence. Patients in a palliative care setting who are currently on long-term opioids could potentially be treated with a combination using a lower dose of opioids.
Valid concerns
However, there are a number of valid concerns. One is the unfavourable and somewhat variable adverse effect profile when used in different formulations as a medicinal product (such as inhalation from smoking) (Borgelt et al., 2013). To avoid the risks of smoking cannabis, an oral preparation of THC (dronabinol, a partial agonist at the CB1 receptors, marketed as Marinol®), an oral synthetic analogue of THC (nabilone, marketed as Cesamet®), and an oromucosal spray combining THC and CBD in a 1:1 mixture (nabiximols, marketed as Sativex®) have been developed (Table 1).
The method of delivery and patient individuality cause great variability in its effect. There remains a lack of quality control of formulations used (Borgelt et al., 2013). Only the oral and spray forms should be used. There is a mandatory need for adequate monitoring and close surveillance of patients for the prevention of addiction (Borgelt et al., 2013). In addition, training and education should be made available to prescribers.
Extreme caution should be exercised in the use of cannabinoids in patients with a history of cardiovascular disease or mental disorders and in adolescents (Borgelt et al., 2013). A national database should be set up in future to monitor information about the dispensed medical prescribing of cannabis and nabiximols, similar to data sources that collect information about the dispensed prescribing of opioid medications.
Conclusion
The use of cannabinoids is highly topical in the medical world at present; it is particularly relevant to psychiatrists, with the debate being on the vulnerability of the adolescent brain towards cannabinoid exposure. There is renewed public interest and increased political pressure in Australia and New Zealand to allow the medicinal use of either smoked cannabis and/or cannabis extracts such as nabiximols (Sativex®).
Given its legal status, the need for more efficacy data, and its unknown safety and tolerability profile, medical cannabis should be considered only for painful conditions when treatment failure with standard therapy has occurred or where other analgesic medications are not tolerated (Borgelt et al., 2013). Cannabinoids should only be used in those patients who might benefit from their use, such as those with neuropathic pain from various causes (including multiple sclerosis).
Subject to all these provisos, there is a case to be made for medical cannabinoids to be legally available on a limited basis to patients with specific pain conditions. This must be carried out under strict qualified medical supervision. In New Zealand, this would entail a change in legislation.
Future cannabinoid research should focus on formulations without the THC component resulting in analgesia and without psychiatric adverse effects. These new formulations would not further the cause of those desiring legislation change for street cannabis. High-quality studies (with large study populations and long-term exposure) are needed to determine the appropriate uses of medical cannabinoids. Formulations and dosages require standardisation. Given the prevalence of chronic pain, more research into the cannabinoids should be funded.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no financial disclosures, grant support, or conflicts of interest. The authors alone are responsible for the content and writing of the paper.