
Abstract
Objective:
Antisocial personality disorder (ASPD) and schizophrenia, as well as childhood abuse, are associated with violent behaviour and show marked volumetric reduction in the anterior cingulate (AC), a brain region implicated in regulation of violence through its involvement in decision making, empathy, impulse control, and emotion regulation. The present study examined, for the first time to the authors’ knowledge, the grey matter volume of the AC in relation to seriously violent behaviour and childhood psychosocial deprivation (including physical and sexual abuse) in the context of a mental disorder (schizophrenia or ASPD).
Methods:
Fifty-seven men [14 with ASPD and a history of serious violence; 13 with schizophrenia and a history of serious violence (VSZ); 15 with schizophrenia without a violence history (SZ); 15 nonviolent healthy participants] underwent whole-brain magnetic resonance imaging and were rated on the presence of physical abuse, sexual abuse, neglect, extreme poverty, foster home placement, criminal parent, severe family conflict, and broken home (collectively ‘psychosocial deprivation’). Stereological volumetric ratings of the AC were examined for group differences and their association with childhood psychosocial deprivation.
Results:
A higher proportion of ASPD and VSZ patients had suffered psychosocial deprivation as children, in particular severe physical abuse, relative to SZ patients and healthy participants. ASPD and VSZ, but not SZ, patients had significantly lower AC volume relative to healthy participants. AC volumes correlated negatively with (total) psychosocial deprivation as well as physical and sexual abuse ratings. Group differences in AC volume became nonsignificant when psychosocial deprivation ratings were covaried for.
Conclusions:
Violent mentally disordered individuals with ASPD or schizophrenia suffer from a significant AC volume loss and this deficit, at least in part, is explained by their histories of stressful childhood experiences. Current and future therapies aiming to reduce violence in such populations would benefit by attending to biological (and other) correlates of childhood abuse.
Introduction
There is robust epidemiological evidence of an increased risk of violent offending, relative to the general population, in men with antisocial personality disorder (ASPD; Eronen et al., 1998) and schizophrenia (Arseneault et al., 2000). Individuals who as children suffered adversity, in particular sexual or physical abuse, have a heightened risk of developing mental disorders (Bebbington et al., 2011; Janssen et al., 2004; Maniglio, 2009), and, although the majority of these do not commit any violent offences as an adult, they are, on average, more likely to commit violent crimes than those who were not abused (Perepletchikova and Kaufman, 2010). Morphological variation in multiple brain structures, particularly the frontal and temporal lobes, have been linked in individual studies with violence (Dolan et al., 2010), ASPD (Bassarath, 2001; Yang and Raine, 2009) and schizophrenia (Honea et al., 2005; Leung et al., 2011; Shenton et al., 2001) as well as a history of childhood abuse (examined mainly in the context of post-traumatic stress disorder, depression or borderline personality disorder; McCrory et al., 2010).
So far, only two published studies (Kumari et al., 2013; Raine et al., 1998) have examined the role of childhood abuse in brain properties of forensic psychiatric populations. The first study, by Raine et al. (1998), showed that within the group of individuals who had been charged with murder, only those (12/41) who did not have marked psychosocial deprivation (i.e. no severe physical or sexual abuse) showed a lower prefrontal glucose metabolism compared with nonviolent control participants. This observation led Raine et al. (1998) to propose that psychosocially deprived individuals learn to be violent due to experiencing a maladaptive environment rather than due to prefrontal deficits that normally affect social and emotional learning. In the second study (Kumari et al., 2013), we observed that childhood abuse, as conceptualized by Raine et al. (1998), was associated with volumetric loss of stress-responsive regions (De Bellis et al., 1999), namely the hippocampus and the frontal cortex, in nonviolent individuals with or without schizophrenia. However, in those individuals with schizophrenia and ASPD who also had a history of serious violence, childhood abuse was associated with volume loss of the thalamus, an area that is considered important for normal sensory information processing (Steriade and Llinas, 1988) and corticocortical communication (Sherman, 2007). Our findings (Kumari et al., 2013) suggested that childhood abuse may be associated with different patterns of brain deficits in individuals who go on to commit violent offences and those who do not engage in violent or antisocial behaviour in adulthood (and perhaps are prone to other conditions such as depression or post-traumatic stress disorder; McCrory et al., 2010).
The present study examined, for the first time to our knowledge, the grey matter volume of the anterior cingulate (AC) in relation to the presence of a mental disorder (schizophrenia or ASPD), as well as of seriously violent behaviour and childhood psychosocial deprivation, including physical and sexual abuse, in the same sample. The AC is considered an important part of the neural circuit regulating violence and antisocial behaviour (Davidson et al., 2000), because of its known involvement in functions such decision making, empathy, impulse control, and emotion regulation (Devinsky et al., 1995; Shackman et al., 2011). A number of studies have reported AC volume loss in association with ASPD (Yang and Raine, 2009), schizophrenia (Baiano et al., 2007; Fornito et al., 2009; Shepherd et al., 2012) as well as childhood abuse (Thomaes et al., 2010). The present study aimed to test the following two hypotheses: (i) patients with ASPD or schizophrenia and a history of serious violence would have lower AC grey matter volume, whereas those with schizophrenia but without a history of violence would not differ or have only a subtle AC volume reduction, relative to nonviolent healthy participants; and (ii) a history of childhood psychosocial deprivation, in particular severe physical or sexual abuse, would be associated negatively with AC volumes. Additionally, the study explored whether the relationship between AC volume and psychosocial deprivation/abuse, if found, is present across all groups or specific to either violent or nonviolent groups.
Methods
Participants
This study included 57 men who were recruited as part of a larger project (Barkataki et al., 2006; Kumari et al., 2006, 2009a, b, 2013). Of these 57 men, 14 men had a diagnosis of ASPD and a history of serious violence (ASPD group), 13 were diagnosed with schizophrenia and had a history, similar to the ASPD group, of serious violence (VSZ group), 15 had schizophrenia without a history of serious violence (SZ group), and a control group of 15 men had no history of a mental disorder or violence (healthy participants; HP group).
All included participants met the following criteria: (i) aged between 18–55 years; (ii) free of substance abuse as confirmed by urine analysis; (iii) no history of neurological conditions or head injury; and (iv) fluent in English and able to provide written informed consent. The included ASPD patients were required to have a diagnosis of ASPD (cluster B, DSM-IV) and a history of significant violence (criteria for significant violence provided under Assessment of Violence) but no comorbid diagnosis of schizophrenia. The VSZ patients were required to meet the criteria for a schizophrenia diagnosis and not to have a comorbid diagnosis of ASPD.
All ASPD and VSZ patients were recruited from specialist high- and medium-security UK hospitals where security and treatment is provided, for mentally ill patients who require compulsory detention under the Mental Health Act, 1983 (England and Wales; www.legislation.gov.uk/ukpga/1983/20/contents) because of their dangerous, violent or criminal tendencies and the risk of violence. Nonviolent SZ patients were recruited from local hospitals and outpatient clinics. Healthy participants were recruited through local advertisements.
The study was approved by the research ethics committee of the Institute of Psychiatry, London. All participants provided written informed consent.
Diagnosis and clinical assessments
The diagnosis of ASPD was established using the Structured Clinical Interview for DSM IV personality disorders (First et al., 1997) and of schizophrenia using the Structured Clinical Interview for DSM IV Axis I disorder (First et al., 1995). Healthy participants were screened to ensure a negative history of mental illness using the Structured Clinical Interview for DSM-III-R – Non-Patient Edition (Spitzer et al., 1990). All participants were assessed on National Adult Reading Test (Nelson and Willison, 1991) to obtain an estimate of predicted IQ. Additionally, all patients with schizophrenia were rated on symptoms using the Positive and Negative Syndrome Scale (Kay et al., 1987) and their antipsychotic treatment was noted for sample characterization purposes.
Assessment of violence
The history of violence in VSZ and ASPD groups was established from their clinical and forensic records. The Gunn and Robertson criminal profile (score range 0–8; Gunn and Robertson, 1976) was used to rate violence in all participants, with serious violence defined as score 4 or above for the seriousness of the most recent violence act, indicating a fatal or near fatal act of violence against a victim.
Assessment of psychosocial deprivation
Psychosocial deprivation ratings were collected using the same method as used by Raine et al. (1998) on all participants using interview, case history, clinical records, and forensic records (where applicable) by one of investigators (MD). The ratings were based on the presence of: (i) physical abuse; (ii) sexual abuse; (iii) neglect; (iv) extreme poverty; (v) foster home placement; (vi) having a criminal parent; (vii) severe family conflict; and (viii) a broken home. Each of these items was rated (by MD) on a 5-point scale (0=none, 1=minimal, 2=partial, 3=substantial, 4=extreme). A total psychosocial deprivation score was created by summing up ratings on the eight individual items. In addition, two raters (GHG, VK) independently coded the ratings on each participant for the degree to which evidence was present for childhood psychosocial deprivation, following the procedure described by Raine et al. (1998). A score of 4 was given to participants with clear evidence of repeated physical or sexual abuse as a child; score 3 to those for whom there was clear evidence of severe family conflict and placement into a foster home; score 2 to those who came from a broken home and who had other clear evidence of extreme poverty or having a criminal parent; score 1 to those from broken homes who lacked deprivation on other indices; and finally score 0 to those with no convincing objective evidence of deprivation. Participants who received a score of 2–4 were identified as having significant psychosocial deprivation and those with a score of 1 or 0 as having no or minimal psychosocial deprivation.
MRI acquisition
MRI scans were acquired using a 1.5 Tesla GE NV/i Signa system (General Electric, Milwaukee WI, USA) at the Maudsley Hospital, London. Initially, a series of sagittal fast gradient echo scout images were acquired. A 3-D inversion-recovery-prepared fast-spoiled GRASS sequence was applied to the whole brain to obtain T1-weighted images in the axial plane with 1.5-mm contiguous sections with the following specifications: TR=13.8 ms, TI=450 ms, TE=2.8 ms, flip angle=20 degrees, FoV=24 cm.
Stereological volumetric ratings
Stereological volumetric assessment of the AC grey matter volume was conducted using the MEASURE program and Cavalieri method (Barta et al., 1997), adopting the identification procedure described by Takahashi et al. (2002) (Figure 1). All AC grey matter volumes ratings, separately for the left and right hemispheres, were performed by a single trained rater (SU), who had high intra- and inter-rater (against PP, an experienced MEASURE rater) reliabilities and was kept blind to participant group membership to avoid any observer bias in rating results. Our previous work (Kumari et al., 2013) examined, using the region of interest approach, the whole brain, cerebellum, temporal lobe, lateral ventricles, caudate nucleus, putamen, thalamus, hippocampus, amygdala, and prefrontal and occipito-parietal regions in relation to a history of violence and childhood abuse in this sample. The AC grey matter volumes of this sample are being examined and reported for the first time.

Illustration of anterior cingulate boundaries.
Statistical analysis
All statistical analyses were carried out using SPSS version 20. The level of significance was set at p=0.05 unless stated otherwise.
Group differences in age, predicted IQ, and the severity of violence were examined by a one-way analysis of variance (ANOVA) with Group (ASPD, VSZ, SZ, HP) as the between-subjects factor. Psychosocial deprivation (absent, present) was not entered as an additional between-subjects factor in ANOVAs because there were no deprived people in the healthy participant group and there were only three nondeprived patients in the ASPD group.
Group differences in AC grey matter volume were analysed using a 2 × 4 (Hemisphere × Group) analysis of variance (ANOVA) with Hemisphere (left, right) as a within-subjects factor and Group (ASPD, VSZ, SZ, HP) as a between-subjects factor. Significant effects were followed up using lower-order ANOVAs and post-hoc mean comparisons as appropriate. Effects sizes, where reported, are partial eta-squared (i.e. the proportion of variance associated with a factor). Following the observations of a higher proportion of deprived/abused individuals in the ASPD and VSZ groups relative to the SZ and HP groups and a negative association between childhood psychosocial deprivation ratings and AC volume across the whole sample (see Results), group differences in AC volume were re-evaluated using 2 × 4 analysis of covariance (ANCOVA) with Hemisphere (left, right) as a within-subjects factor, Group (ASPD, VSZ, SZ, HP) as a between-subjects factor, and childhood psychosocial deprivation ratings as the covariate.
The associations between total psychosocial deprivation ratings and AC volumes (total, right, and left) were examined by Pearson correlations. The associations between ratings (obtained on a 5-point scale) on individual items of sexual abuse and physical abuse (in separate analyses) and AC volumes were examined using Spearman rank order correlations; ratings on other psychosocial deprivation items were not analysed individually because they were present mostly in the same individuals who had physical and sexual abuse histories. These analyses were first carried out across the whole sample (n=57), and then separately for nonviolent (SZ + HP, n=30) and violent subgroups (ASPD + VSZ, n=27). The negative relationship between the AC volumes and psychosocial deprivation ratings across the whole sample was further evaluated after controlling for the whole-brain volume, given the earlier reported group differences in whole-brain volume (Kumari et al., 2013).
The relationships of the violence score (Gunn and Robertson, 1976) with psychosocial deprivation/abuse ratings and AC volumes were also examined using Spearman rank order correlations to try to understand inter-relationships amongst these variables.
Results
Demographic and clinical measures
As shown in Table 1, the four groups (ASPD, VSZ, SZ, and HP) had similar age and predicted IQ (p>0.10). As expected, there was a main effect of Group for violence ratings (F=52.09, df=3,50, p<0.001), confirming that the two violent groups (ASPD, VSZ) had higher violence ratings than the two nonviolent groups (SZ, HP).
Demographic and clinical characteristics of participant groups, classified by presence or absence of significant psychosocial deprivation.
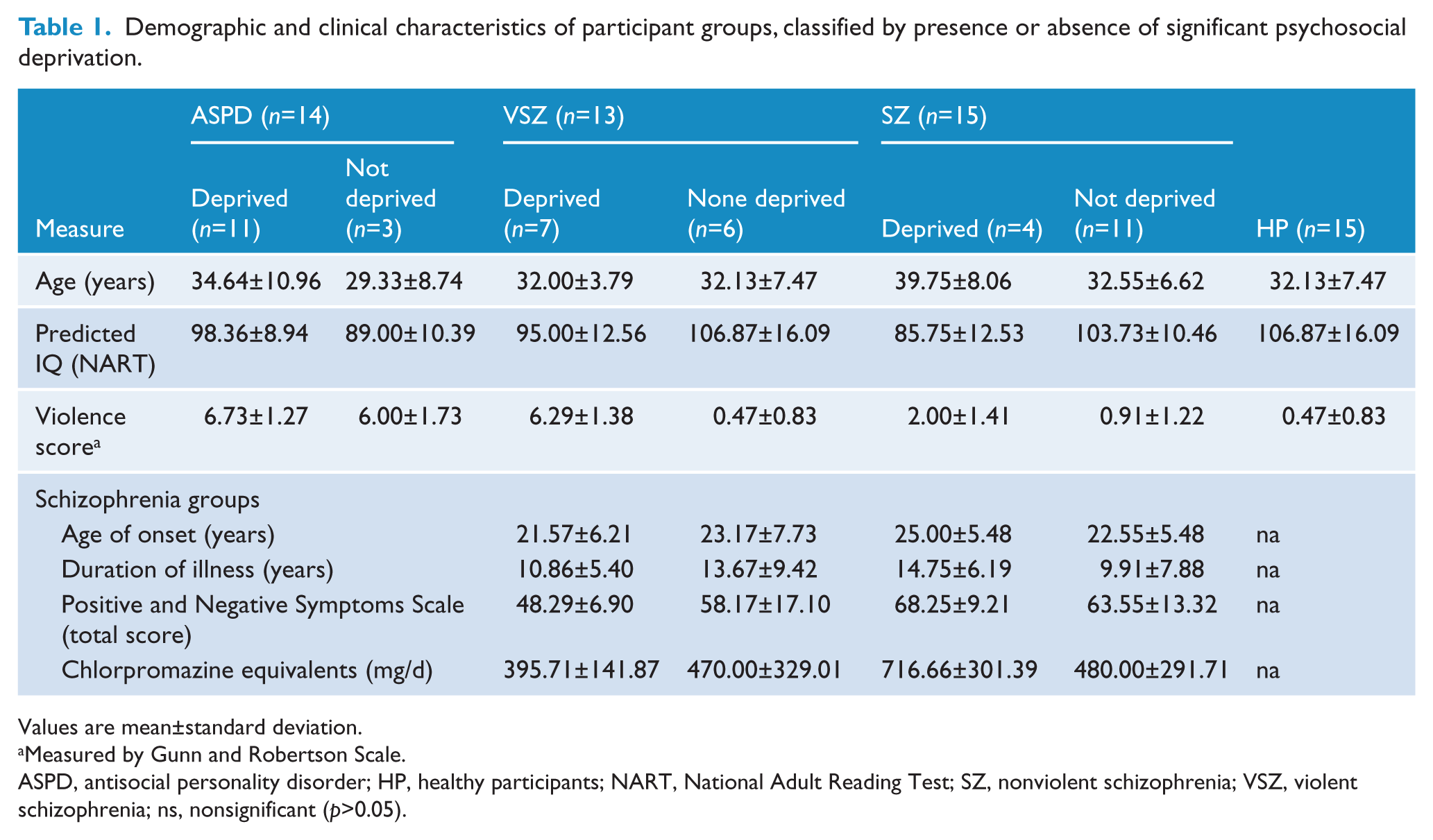
Values are mean±standard deviation.
Measured by Gunn and Robertson Scale.
ASPD, antisocial personality disorder; HP, healthy participants; NART, National Adult Reading Test; SZ, nonviolent schizophrenia; VSZ, violent schizophrenia; ns, nonsignificant (p>0.05).
As shown in Table 2, a higher proportion of the violent groups (ASPD, 79%; VSZ, 54%), relative to the nonviolent groups (SZ, 27%; HP, 0%), had suffered significant psychosocial deprivation (Table 2). There was a high frequency of severe physical (present in 9/14 cases; 3/14 extreme) and sexual abuse (7/14; 5/14 extreme) in the ASPD group. Severe physical abuse was also common (4/13; 2/13 extreme), but sexual abuse was relatively less common (1/13; none extreme) in the VSZ group.
Psychosocial deprivation ratings classified by study groups.
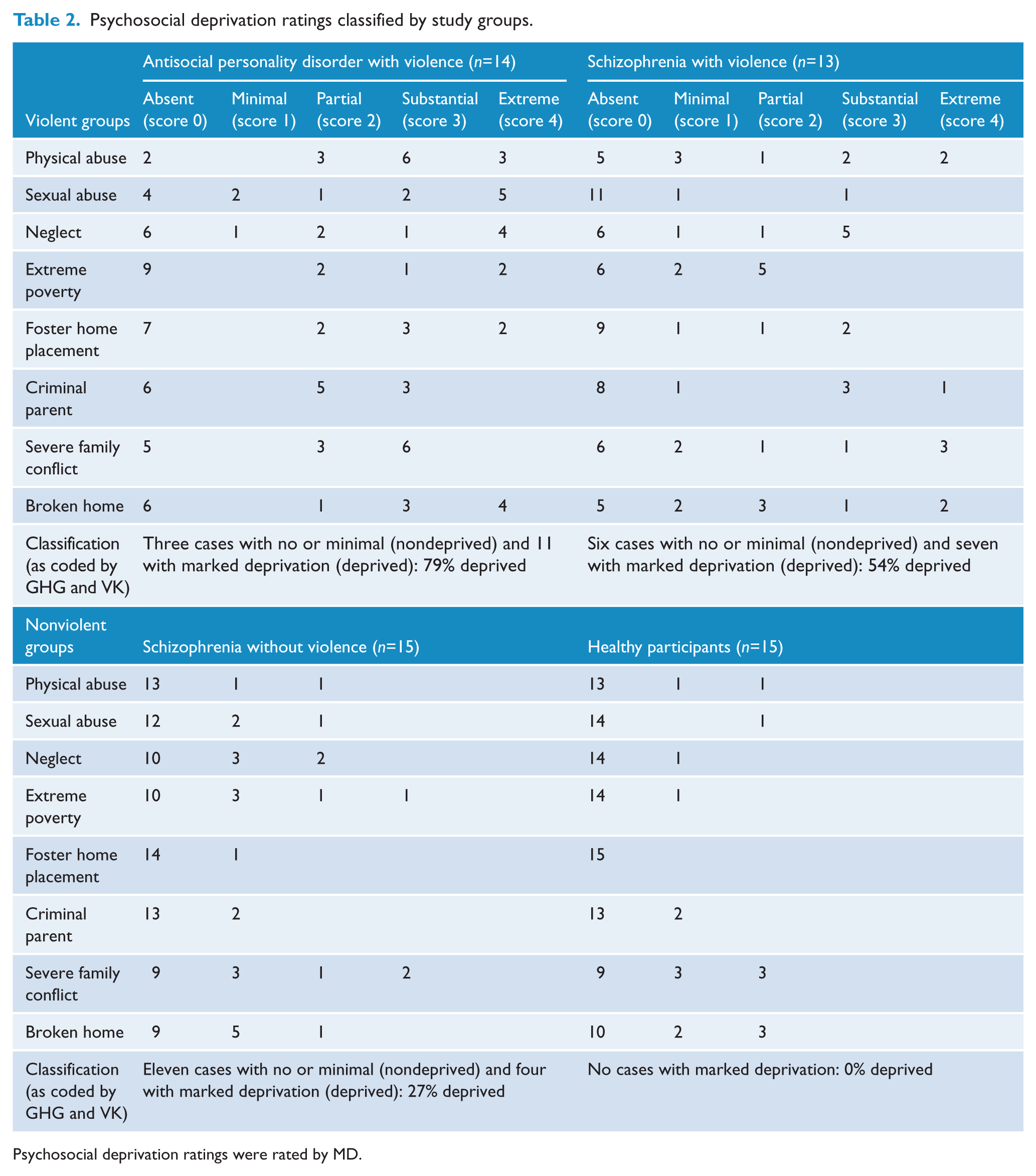
Psychosocial deprivation ratings were rated by MD.
Although all ASPD and VSZ patients were free of alcohol and substance misuse for a minimum of 2 years (confirmed by regular random urine screens in secure hospitals) at the time of their participation, past alcohol and substance misuse/dependence were relatively more common in these patients than SZ patients. Specifically, 12 of 14 ASPD patients had a history of past alcohol and substance misuse/dependence (one with a history of alcohol dependence; one with alcohol dependence and benzodiazepines misuse; one with alcohol dependence and cannabis dependence; four with alcohol and polysubstance misuse, five with alcohol dependence and polysubstance misuse) and all of these except one were rated as having significant psychosocial deprivation. All 11 ASPD patients identified as having significant psychosocial deprivation (Table 2) had a history of alcohol and substance misuse.
Six of 13 VSZ patients had a history of past alcohol and substance misuse/dependence (two with a history of alcohol dependence; one with solvent misuse; one with cannabis dependence; one with alcohol and polysubstance misuse; one with alcohol dependence and polysubstance misuse), and five were found to have significant psychosocial deprivation.
In the SZ group, one patient had a past history of using cannabis and one of using cannabis and lysergic acid diethylamide. None of these were rated as having significant psychosocial deprivation.
Within the schizophrenia groups, the deprived VSZ group had less severe symptoms than nondeprived VSZ group (F=6.27, df=1,24, p=0.02; Table 1). This, as discussed in our previous reports involving highly overlapping samples (Kumari et al., 2009b, 2013), may reflect VSZ group living in a safer environment (i.e. a high-security hospital) as well as better medication compliance than the community-based SZ group.
AC volume
There was a significant main effect of Group (F=3.65, df=3,53, p=0.018; eta2=0.17). Follow-up analysis indicated that, on average, both the ASPD (F=11.82, df=1,27, p=0.002; eta2=0.30) and VSZ patients (F=6.84, df=1,26; p=0.015; eta2=0.21) had significantly lower AC volume than healthy participants (Figure 2). There was a trend for the SZ group to have lower AC volume than healthy participants (F=3.56, df=1,28, p=0.07; eta2=0.11). Other Group comparisons were not significant (p>0.20).
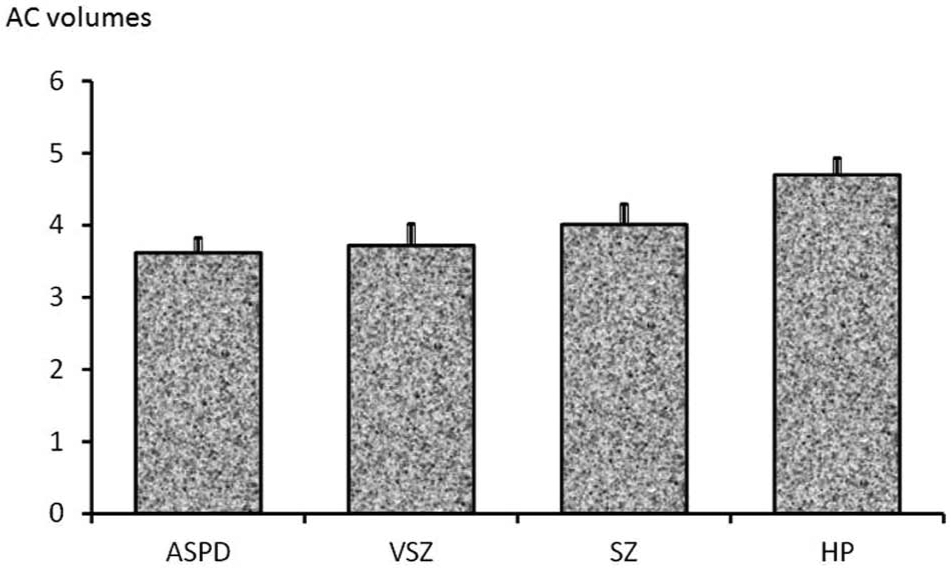
Mean anterior cingulate (AC) volumes classified by study groups.
There was also a significant main effect of Hemisphere (F=10.81, df=1,53, p=0.002; eta2=0.17), indicating larger AC volume on the right than on the left across all participants (t=3.38, df=56, p=0.001), but no interaction between Hemisphere and Group (F<1).
The effect of Group became nonsignificant (F=1.57, df=3.52, p=0.21; eta2=0.08) when total psychosocial deprivation ratings were entered as a covariate.
Relationship between AC volume and childhood psychosocial deprivation/abuse ratings
AC volumes correlated significantly negatively with total psychosocial deprivation ratings as well as with ratings of sexual and physical abuse; and both violent and nonviolent participants appeared to contribute to these relationships (Table 3). The negative relationship between the AC volumes and psychosocial deprivation ratings across the whole sample remained significant even after controlling for the whole-brain volume (partial r=−0.323, df=54, p=0.015); whole-brain volume on its own was not significantly correlated with psychosocial deprivation ratings (r=−0.228, df=57, p=0.09).
Relationships of anterior cingulate (AC) grey matter volumes with total and individual ratings of psychosocial deprivation/abuse and violence.
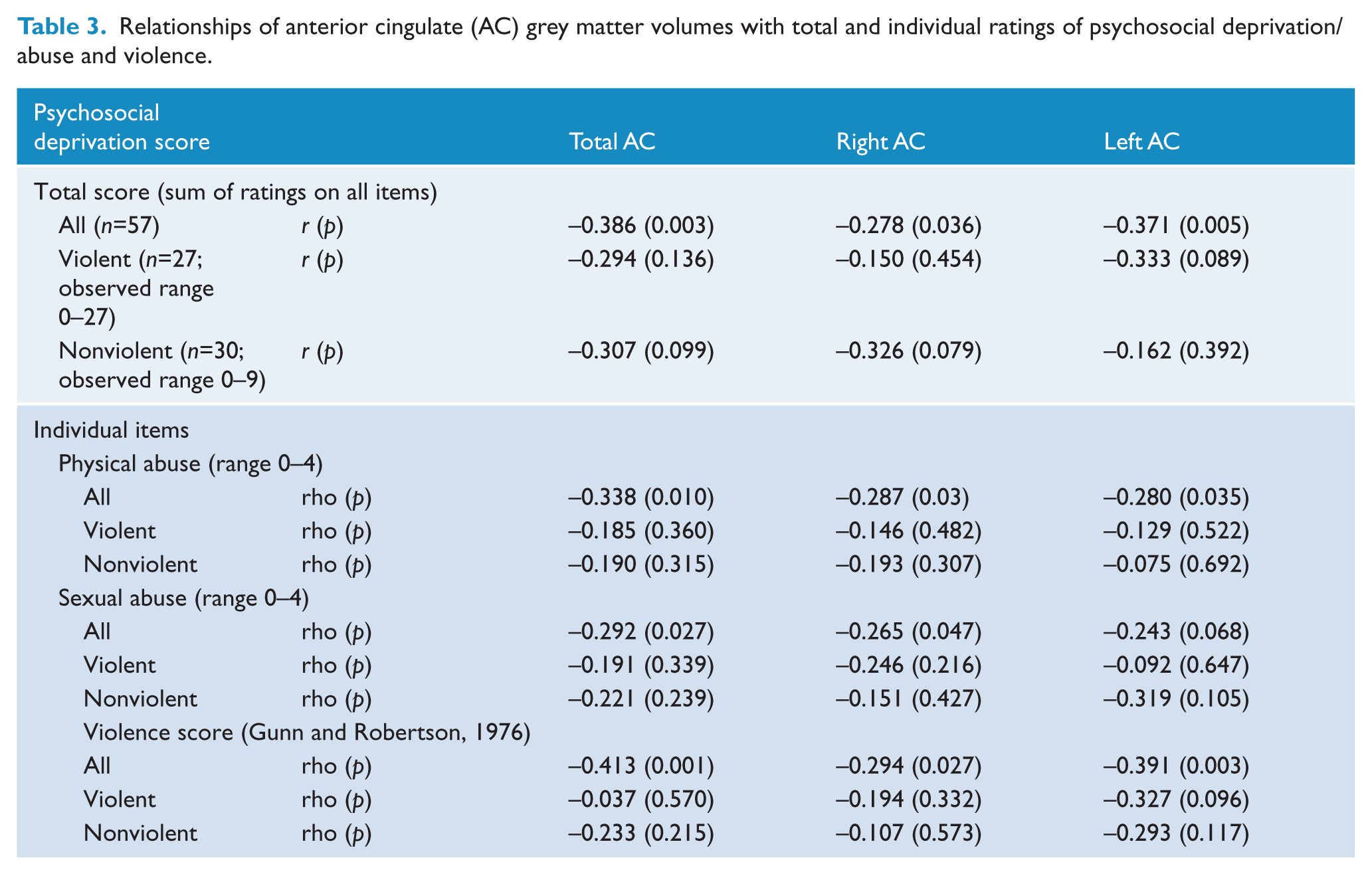
The violence score correlated positively with psychosocial deprivation ratings (rho=0.572, df=57, p<0.001), and negatively with AC volumes across the whole sample (Table 3).
Discussion
This study examined AC volume in relation to the presence of a mental disorder (schizophrenia or ASPD), as well as histories of seriously violent behaviour and childhood abuse in the same sample. The main findings were: (i) the two violent groups (ASPD, VSZ), on average, had significantly lower AC volume relative to the healthy participant group while there was only a trend for lower AC volume in the nonviolent schizophrenia (SZ) group; and (ii) AC volumes correlated significantly negatively, even after controlling for whole-brain volume, with psychosocial deprivation (total) as well as physical and sexual abuse ratings across the whole sample, with both violent and nonviolent participants contributing to these relationships.
Our finding of a lower AC grey matter volume in the ASPD and VSZ groups is consistent with our hypothesis and previous data on this topic (Yang and Raine, 2009). However, since group differences in AC volume became nonsignificant when psychosocial deprivation ratings were covaried for, the observed group differences in AC volumes were most likely due to the higher rate of psychosocial deprivation in the two violent groups. As reported here (Table 2) and in an earlier report involving 56 patients of this cohort (Kumari et al., 2013), a higher proportion of ASPD and VSZ patients had suffered significant psychosocial deprivation, in particular severe physical and/or sexual abuse as children, and there was a direct negative correlation between the AC volume bilaterally and psychosocial deprivation (total) as well as physical and sexual abuse ratings across the whole sample. The AC is highly vulnerable to stress-related changes in noradrenergic activity (Hermans et al., 2011) and, like the hippocampus, shows grey matter loss following a variety of stressful conditions, including childhood adversity, in individuals with or without a PTSD diagnosis (Ansell et al., 2012; Dannlowski et al., 2012; Karl et al., 2006). Although the current study is unable to conclusively inform about the direction of causality in the observed relationship between AC volume and psychosocial deprivation/abuse, a number of studies have clearly shown AC grey matter loss in people experiencing stressful life events and cumulative life adversities with no psychiatric diagnosis (Ansell et al., 2012; Ganzel et al., 2008; Papagni et al., 2011), as well as in animals following exposure to stress (Cerqueira et al., 2005; Kassem et al., 2013).
It should be noted that all ASPD and 5/7 violent schizophrenia patients who were identified as having significant psychosocial deprivation also had substance and alcohol misuse/abuse histories. While this is not surprising, given previous evidence of a link between childhood maltreatment and the risk of psychiatric disorders including drug addiction (Bebbington et al., 2011; Green et al., 2010; Janssen et al., 2004; Maniglio, 2009), it opens up the possibility that childhood psychosocial deprivation/abuse may contribute to drug addiction (which in turn is commonly associated with violence and criminal behaviour; Miller et al., 2006) via an AC deficit. Intact AC function is required for cognitive and behavioural control (Devinsky et al., 1995; Shackman et al., 2011), and poor cognitive control is strongly implicated in drug addiction (Bari and Robbins, 2013) as well as antisocial/violent behaviour (Swann et al., 2009). Future functional neuroimaging research should consider how AC-related functions of emotional decision making, empathy, and impulse control mediate the association between experiencing childhood psychosocial deprivation and the likelihood of inflicting violence on others and/or drug addiction in relevant clinical groups.
Unlike our previous finding of an association between lower thalamic volume and childhood psychosocial deprivation/abuse that was present only in violent (i.e. ASPD and VSZ) participants (Kumari et al., 2013), AC volume was negatively correlated with childhood psychosocial deprivation/abuse across all participants in this study. This suggests that some brain damage (e.g. AC deficit) following stressful events/childhood abuse may be present across individuals, regardless of a presence/absence of violent behaviour or a mental disorder, while additional deficits may occur in those who go on to commit violent offences. However, even if AC deficit alone, at least at the structural level, may not be sufficient to predispose deprived/abused individuals with schizophrenia or ASPD to violence, it might still impede the effectiveness of relevant cognitive behavioural therapies that make use of AC-modulated cognitive processes (Kumari et al., 2009c) to prevent the occurrence of future violence in these populations.
The limitations of this study, which was opportunistic and carried out using an existing data set, include the relatively small sample size. A further limitation concerns the fact that this study is unable to disentangle the effects of drug abuse in AC deficit separate from those of childhood psychosocial deprivation/abuse. A larger sample size might have allowed investigation of other contributing factors (e.g. through mediation analysis to understand the contribution of alcohol and substance abuse history to the observed AC deficit). Other sample characteristics (i.e. alcohol and substance abuse history present in all 11 ASPD and 5/7 violent schizophrenia patients with marked psychosocial deprivation) also precluded such analyses. Furthermore, as this study was limited to men, the findings may not be applicable to women.
In conclusion, violent mentally disordered individuals are more likely to have suffered significant childhood psychosocial deprivation and in turn to display a marked AC grey matter volume loss. Current and future therapies aiming to reduce violence in mentally disordered populations would benefit by attending to biological (and other) consequences of childhood abuse, while policy makers must consider means to prevent or minimize childhood abuse, especially in populations at risk of ASPD or SZ, to reduce violence in society on the whole.
Footnotes
Funding
This investigation was supported by the British Academy, UK (grant no. SCHK03) and funds from the Biomedical Research Centre for Mental Health at the Institute of Psychiatry, King’s College London, and by the South London and Maudsley NHS Foundation Trust for some of VK’s time.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.