
Abstract
Objective:
To describe and compare individuals with any DSM-IV mental disorder from three different birth cohorts – young (16–34 years), middle age (35–59 years) and older age (60–85 years) – on a range of clinically relevant factors.
Method:
Data were derived from the 2007 Australian National Survey of Mental Health and Wellbeing. Individuals from three birth cohorts with a range of mental health and substance use disorders were identified using DSM-IV criteria and compared using regression analysis. The specific factors that were compared include: (1) type of disorder/disorders present; (2) suicidality; (3) number of co-occurring disorders; (4) levels of distress and impairment; (5) self-assessed physical and mental health; (6) presence of physical conditions; (7) size and quality of social support/network; and (8) treatment-seeking behaviour.
Results:
The birth cohorts differed dramatically in terms of the specific disorders that were present. The older cohort were significantly more likely to experience internalising disorders and significantly less likely to experience externalising disorders in comparison to the young cohort. The older cohort were significantly more likely to experience co-morbid physical conditions as well as lower life satisfaction, poorer self-rated physical health, increased functional impairment, and more days out of role. The younger cohort had a significantly larger peer group that they could confide in and rely on in comparison to the older cohort.
Conclusions:
Clinicians and researchers need to be cognisant that mental disorders manifest as highly heterogeneous constructs. The presentation of a disorder in a younger individual could be vastly different from the presentation of the same disorder in an older individual. The additional burden associated with these factors and how they apply to different birth cohorts must be taken into consideration when planning mental health services and effective treatment for the general population.
Introduction
Epidemiological studies from around the world have consistently indicated that the prevalence of common mental disorders is lower amongst older cohorts compared to younger cohorts (Kessler et al., 2010a, 2010b; McEvoy et al., 2011; Trollor et al., 2007). This finding has led some researchers to conclude that numerous protective factors lead to a reduced prevalence of disorders in older age (Jorm, 2000a). Such protective factors include improved resilience, coping skills and emotional control as well as a decrease in emotional responsiveness and neuroticism levels (Blazer and Hybels, 2005; Ernst and Angst, 1995; Mroczek and Spiro, 2003; Williams et al., 2006). Alternatively, researchers have questioned these findings and claim that the prevalence of mental disorders in older cohorts may be underestimated due to poor validity of the diagnostic instruments and the complexity of epidemiological surveys (O’Connor and Parslow, 2010). These findings have often provided the image that disorders amongst the older population are rare in comparison to younger cohorts regardless of whether it is a true decline or artefact of assessment. Indeed, across younger age groups there is a steady increase in the prevalence and onset of most mental disorders before reaching a peak in middle age (Kessler et al., 2007).
This rise and fall trajectory of mental illness across age cohorts has encouraged clinicians and researchers to focus research and health service expenditure on younger cohorts in the population. Indeed, improving the quality and size of treatment services as well as utilisation of these services amongst the whole population is a key aim of the Australian government mental health policy reforms (Council of Australian Governments, 2012). However, the population boom in the 1940s and 1950s has resulted in a large-scale demographic shift that poses a significant challenge to mental health services, which may struggle to keep up with the greater demands of an aging population (Jeste et al., 1999; Karel et al., 2012). Therefore, further examination of mental health disorders amongst older cohorts may result in significant improvements in mental health services and the development of treatment and prevention programs that reduce the incidence of mental disorders in old age by targeting known risk factors (Draper et al., 2006).
Examination of the prevalence rates across the age cohorts might distort the picture of mental health experienced by various birth cohorts. Mental disorders are heterogeneous constructs, meaning that the use of polythetic diagnostic criteria and the possibility of receiving multiple related diagnoses can often result in large variations in the type of disorders, symptoms and criteria that are experienced by individuals (Hyman, 2010; Krueger and Bezdjian, 2009). Moreover, mental disorders co-occur more often than expected by chance and a number of external but related factors influence course, severity, distress level and treatment outcome. For example, the presence of suicidality, regardless of the diagnosis, is often used by clinicians as a marker of severity and requires special consideration when planning effective treatment (Claassen et al., 2007; Kim et al., 2011). Co-morbid physical and mental disorders also pose a growing problem that can result in higher degrees of severity and distress and increased levels of mortality, particularly in relation to mental disorders that co-occur with cardiovascular and heart disease (Barth et al., 2004; Baumeister et al., 2011; Penninx et al., 2001). Finally, the level of social support and treatment utilisation are important factors associated with a reduction in the burden of mental disorders faced by individuals (Thoits, 2011).
Therefore, whilst the prevalence of mental disorders provides a picture of improved mental health across age, it is unclear whether the disorder profile and associated clinical factors remain constant across birth cohorts. It is possible that disorders, whilst comparatively rare in older age, might be accompanied by additional, complicating factors that may not be present in younger cohorts and therefore require greater clinical attention, more nuanced treatment planning, and exert additional pressure on health services and government budgets. Providing additional evidence that better describes the profiles of disorder across different age groups is a key step towards improving interventions and alleviating pressure on health services, clinicians and government budgets.
Previous research provides support for a changing disorder profile with age, particularly research demonstrating higher rates of co-morbid physical and mental disorders in older age (Kessler et al., 2010b). Moreover, many physical disorders are often observed as a result of advanced aging, such as chronic pain due to arthritis or reduced bone and cartilage density. The increased symptom overlap between mental and physical disorders may also further contribute to poor recognition and diagnosis of mental disorders amongst older individuals (Mitchell, 2011). Research also indicates that psychosocial factors such as loneliness and social isolation are more common with increasing age and can contribute to increased severity of mental disorders (Jylhä, 2004). Finally, in one of the few studies to directly compare the prevalence and determinants of mental disorders across middle age and older age cohorts, Trollor et al. (2007) demonstrated that socio-demographic characteristics related to the diagnosis of any mental disorder (mood, anxiety and substance use disorders) differ dramatically across the two age cohorts, particularly in regard to marital status, sex and employment status. In sum, previous evidence indicates a nuanced picture of mental disorders across age cohorts. However, there is a paucity of research examining whether the specific profiles of mental disorder (i.e. the types of disorders and pattern of co-morbidities that are present) and various clinical correlates of interest significantly differ across the birth cohorts in the general population.
The current study aims to address this gap by comparing individuals who receive a diagnosis of any mental disorder across three birth cohorts – young (16–34 years), middle age (35–59 years) and older age (60–85 years) – on a range of clinically relevant factors. The specific factors under examination include: (1) type of disorder/disorders present; (2) suicidality; (3) number of co-occurring disorders; (4) levels of distress and impairment; (5) self-assessed physical and mental health; (6) presence of physical conditions; (7) size and quality of social support/network; and (8) treatment-seeking behaviour. It is hypothesised that the birth cohorts will differ dramatically with respect to the profile of individuals with a mental disorder, thereby providing clinicians and researchers with a greater understanding about what to expect when diagnosing and treating mental disorders amongst community members from different birth cohorts. Ultimately, this research will benefit patients through the implementation of interventions that are tailored to different age groups/birth cohorts as well as providing a greater focus on more problematic and specific issues that are related to mental disorders experienced across birth cohorts.
Method
Sample
Data for the current study were derived from the 2007 Australian National Survey of Mental Health and Wellbeing (NSMHWB), a cross-sectional household survey of the Australian general population (excluding very remote areas). The survey employed a randomly selected, stratified, multistate area design of private non-institutionalised dwellings. The survey was administered to a total of 8841 households representing a response rate of 60%. One member of each selected household within the designated age bracket (aged 16–85 years) was randomly selected to participate in the survey. Over-sampling of the older (aged 65–85 years) and young (aged 16–21 years) age brackets was utilised to ensure the reliability of estimates from these traditionally under-represented age groups. Further information on the administration and sample design of the survey is provided elsewhere (Slade et al., 2009). Respondents were classified into three age brackets for the purpose of the current study: young (aged 16–34 years, n = 2761), middle age (aged 35–59 years, n = 3565) and older age (aged 60–85 years, n = 2515) Australians.
Assessment
The survey was administered by trained lay interviewers from the Australian Bureau of Statistics (ABS) between August and December of 2007. The survey assessed a range of socio-demographic factors, the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and the 10th revision of the International Classification of Diseases (ICD-10) diagnostic information for common mental health and substance use disorders, measures of psychological distress, physical impairment, chronic physical conditions, social networks, self-assessed health, suicidality, and treatment seeking.
Mental health measures
The World Mental Health version of the Composite International Diagnostic Interview (WMH-CIDI; Kessler and Ustun, 2004) was utilised as the base instrument to derive the lifetime presence of DSM-IV and ICD-10 diagnostic criteria of the common mental health and substance use disorders. Diagnostic modules of WMH-CIDI possess sound psychometric properties that have been described in detail elsewhere, including a clinical re-appraisal study using the clinical-administered Structured Clinical Interview for DSM-IV (SCID-IV) as the gold standard (Kessler et al., 2004).
Diagnostic criteria were assessed for several common mental disorders, including: depression, dysthymia, bipolar disorder (manic episode), panic disorder, agoraphobia, social phobia, generalised anxiety disorder (GAD), substance abuse, substance dependence, obsessive-compulsive disorder and post-traumatic stress disorder (PTSD). We further classified disorders into categorical groupings representing internalising disorders (i.e. depression, dysthymia, bipolar disorder, panic disorder, agoraphobia, social phobia, GAD, obsessive compulsive disorder and PTSD) and externalising disorders (i.e. substance abuse, substance dependence) based on evidence regarding the underlying structure of DSM-IV disorders (Slade and Watson, 2006). Questions used to assess diagnostic criteria were worded using a lifetime timeframe and the presence of symptoms in the past 12 months and 30 days was determined using additional recency questions. Respondents were coded as having a diagnosis in the past 12 months if they met criteria for the disorder across their lifetime and indicated that they had experienced symptoms of the disorder in the past 12 months.
Non-specific psychological distress experienced in the past 30 days was measured using the self-report Kessler 10 psychological distress scale (K10; Kessler et al., 2002). The K10 has excellent psychometric properties and has previously demonstrated strong predictive validity for DSM-IV-defined serious mental illness in a variety of populations and settings (Andrews and Slade, 2001; Kessler et al., 2010c; Slade et al., 2011; Sunderland et al., 2011). The K10 consists of 10 items on a five-point scale with scores ranging from 10 to 50; higher scores signify higher levels of psychological distress. Previous guidelines have suggested that scores above 20 are indicative of moderate to very high levels of distress and increase the probability of experiencing a DSM-IV diagnosis (Andrews and Slade, 2001; Australian Bureau of Statistics, 2001). The K10 has also proven suitable as a measure of psychological distress in older aged populations (Anderson et al., 2013).
To measure suicidality, screening questions were included in a stand-alone module of the WMH-CIDI. Three questions were asked to determine the presence of suicide ideation, suicidal plans and suicide attempts in the past 12 months on a binary yes/no scale. The current study utilised these three questions as measures of self-reported suicidality. Self-assessed overall mental health was measured using a single question that rated each respondent’s mental health on a five-point scale, ranging from poor through to excellent. Finally, an additional question was utilised to determine how happy each respondent was with their overall health on a seven-point scale ranging from ‘delighted’ to ‘terrible’.
Physical health measures
The World Health Organization Disability Assessment Schedule 2.0 (WHODAS; Üstün et al., 2010) was utilised to measure physical impairment or activity limitation. This 12-item scale assesses how difficult it would be for each respondent to complete a range of activities in the past 30 days, such as standing for long periods, learning a new task, joining in community activities, concentrating, getting dressed, day-to-day work, etc. Each activity is rated on a five-point scale that ranges from no difficulty to extreme difficulty or cannot do activity. The WHODAS has sound psychometric properties including a stable factor structure and has established normative data (Andrews et al., 2009). The WHODAS was scored so that each individual received a score from 0 to 100, with higher scores indicating greater levels of impairment. Physical disability was also measured using the number of days out of role due to physical or mental poor health. Self-assessed overall physical health was rated using a single question that determined a respondent’s physical health on a five-point scale ranging from ‘poor’ to ‘excellent’. Finally, self-reported chronic physical health conditions were determined by enquiring whether the respondent previously experienced or received a diagnosis of any one of 21 chronic physical conditions in the past 12 months.
Social networks
To assess the degree and nature of social networks available to each respondent, four questions were included in the survey. Two questions required the respondents to provide information regarding (1) the number of family members they could confide in if they had a serious problem and (2) the number of family members they could rely on if they had a serious problem. The remaining two questions required respondents to provide information regarding the number of friends they could confide in and rely on if they had a serious problem. The response categories for all four questions were: (1) zero friends/family; (2) one to two friends/family members; (3) three to four friends/family members; (4) five or more friends/family members; (5) no contact with friends/family; and (6) no friends/family. A final binary (yes/no) question was included to determine the caregiver status of each individual.
Treatment seeking
Treatment seeking was assessed in the survey through a sequence of questions that sought to determine whether each individual had seen a health professional for a mental health problem across their lifetime and in the past 12 months. Health professionals included: alternative therapists, general practitioners (GPs), mental health nurses, specialist doctors or surgeons, psychiatrists, and clinical psychologists. For the purposes of the current study, a final category was created that merged all health professionals together into a general treatment-seeking variable for mental health concerns.
Data analysis
The data were weighted for sex and age according to the most recent Australian national census. Replicate weights and the jackknife repeated replication technique were utilised to correct the standard errors and significance tests for unequal probability of selection due to the complex sampling design. Within each birth cohort, only respondents who received a 12-month diagnosis of any mental disorder (affective disorders, anxiety disorders and substance use disorders) were selected for the follow-up analyses. Respondents from each birth cohort with any mental disorder were compared on a range of mental, physical and social indicators, including treatment-seeking status. The older cohort was treated as the reference group in all analyses. Frequencies and standard errors were produced for categorical variables whereas means and standard errors were produced for continuous variables. The statistical significance of birth cohort characteristics when utilising categorical variables were determined using logistic regression, significance using censored continuous variables (K10 and WHODAS were censored at the upper and lower limits of attainable scores) were determined using censored regression, and significance using count variables (days out of role) were determined using Poisson regression. Regression analyses comparing age groups in terms of distress, impairment, disability, social support and treatment seeking were adjusted by including the type of disorder present (internalising disorder only, externalising disorder only, or both). Analyses were conducted using Stata version 12 and SAS version 9.3.
Results
The presence of any mental disorder in the past 12 months was evident in 647 (23%) respondents aged 16–34 years, 691 (19%) respondents aged 35–59 years and 204 (8%) respondents aged 60–85 years. These groups formed the basis of the remaining analyses and birth cohort comparisons.
Diagnostic mental health status by birth cohort
The specific 12-month disorder diagnoses assigned to members of each birth cohort amongst those with any 12-month mental disorders are provided in Table 1. Birth cohorts significantly differed in a diagnosis of any internalising disorders and any externalising disorders. The young age cohort were significantly less likely to have an internalising disorder (OR = 0.18, 95% CI = 0.10–0.33) but significantly more likely to have an externalising disorder (OR = 7.13, 95% CI = 3.82–13.29) than the older cohort. There was no significant difference between middle age and older age cohorts in terms of internalising disorders but the middle age cohort were significantly more likely to have an externalising disorder (OR = 2.27, 95% CI = 1.24–4.15) than the older cohort. These differences were primarily driven by differential diagnoses of GAD, dysthymia and alcohol abuse and to a lesser extent major depression, PTSD, agoraphobia, panic disorder and drug abuse. A diagnosis of social phobia, in contrast, was more likely in the middle age cohort in comparison to the older age cohort (OR = 2.06, 95% CI = 1.29–3.31). Suicidal plans remained relatively stable across the age bands; however, the younger (OR = 2.17, 95% CI = 1.24–3.80) and middle age (OR = 2.08, 95% CI = 1.12–3.91) cohorts were significantly more likely to experience suicidal ideations in comparison to the older cohort. The younger cohort had a higher albeit non-significant risk of having attempted suicide (OR = 2.15, 95% CI = 0.71–6.57). Interestingly, the level of co-morbidity remained relatively stable across the three birth cohorts. However, the type of co-morbidity differed across the birth cohorts in terms of frequencies, suggesting that cross-disorder cluster co-morbidity (internalising and externalising disorders) is more common in the young cohort (32%) compared to the older cohort (6%).
Rates of specific disorders (12 months), suicidality and co-morbidity amongst those with any disorder (12 months) by birth cohort.
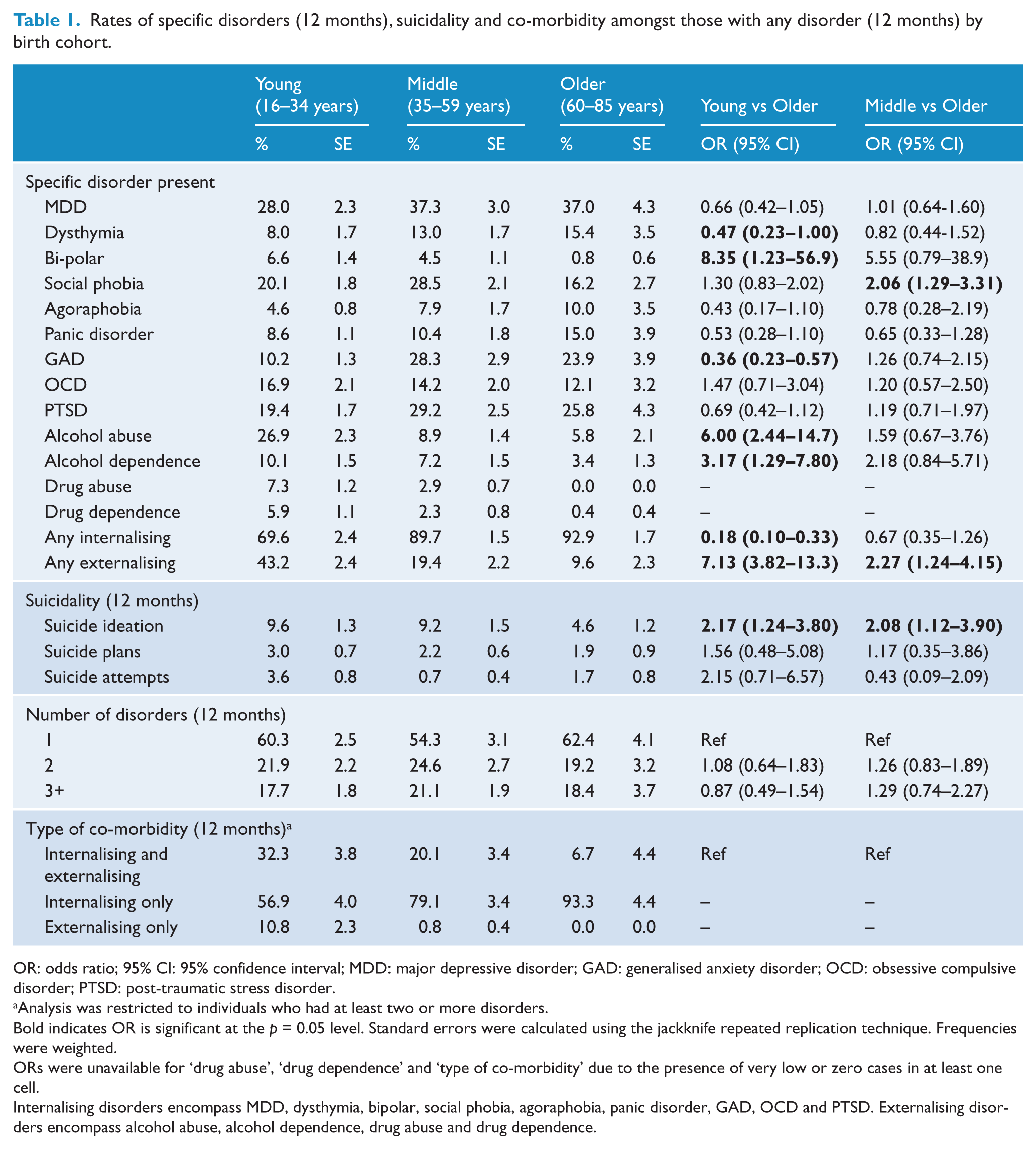
OR: odds ratio; 95% CI: 95% confidence interval; MDD: major depressive disorder; GAD: generalised anxiety disorder; OCD: obsessive compulsive disorder; PTSD: post-traumatic stress disorder.
Analysis was restricted to individuals who had at least two or more disorders.
Bold indicates OR is significant at the p = 0.05 level. Standard errors were calculated using the jackknife repeated replication technique. Frequencies were weighted.
ORs were unavailable for ‘drug abuse’, ‘drug dependence’ and ‘type of co-morbidity’ due to the presence of very low or zero cases in at least one cell.
Internalising disorders encompass MDD, dysthymia, bipolar, social phobia, agoraphobia, panic disorder, GAD, OCD and PTSD. Externalising disorders encompass alcohol abuse, alcohol dependence, drug abuse and drug dependence.
Self-assessed physical and mental health status by birth cohort
Estimates of self-assessed physical and mental health as well as the presence of diagnosed chronic physical conditions are provided in Table 2. Overall, the older cohort rated their physical health and satisfaction with life significantly lower than the young cohort. However, the difference between the older and young cohorts was less pronounced for self-assessed mental health. The presence of more physical conditions in the older age cohort confirms the results of the self-assessed measure and life satisfaction. In brief, the young cohort was significantly less likely to have cancer, stroke, cardiovascular disease, gout, rheumatism, arthritis, diabetes, sinusitis, emphysema, epilepsy, kidney problems, hernias, fluid problems/oedema, stomach ulcer, thyroid trouble, and back or neck pain in comparison to the older cohort. Similarly, the middle age cohort were significantly less likely to have cancer, stroke, cardiovascular disease, gout, rheumatism, arthritis, diabetes, emphysema, fluid problems, hernias, kidney problems, and thyroid trouble in comparison to the older cohort. Asthma was the only condition to be significantly more likely in the young age cohort in comparison to the older cohort.
Self-assessed health (physical and mental) amongst those with any disorder (12 months) by birth cohort.
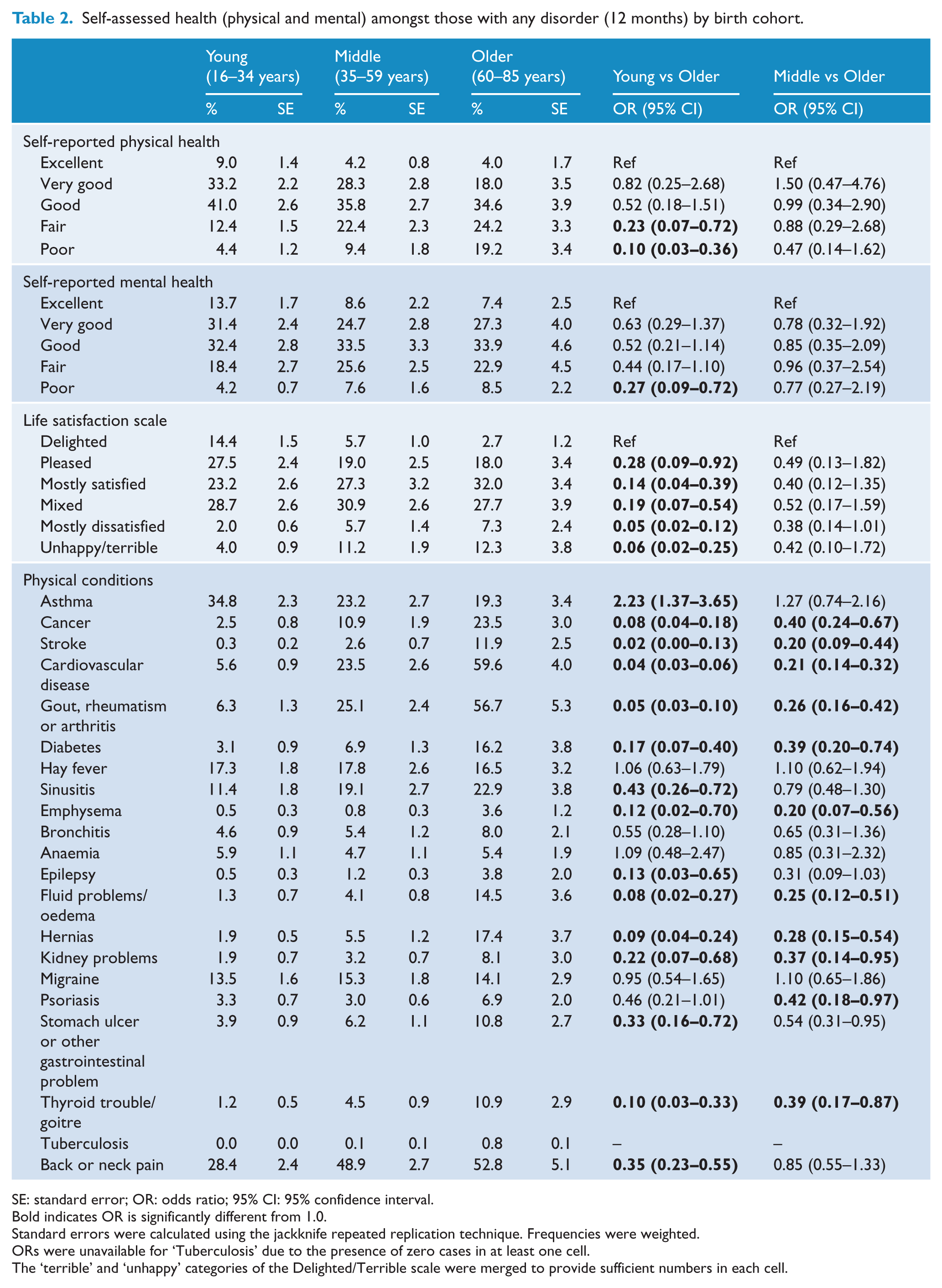
SE: standard error; OR: odds ratio; 95% CI: 95% confidence interval.
Bold indicates OR is significantly different from 1.0.
Standard errors were calculated using the jackknife repeated replication technique. Frequencies were weighted.
ORs were unavailable for ‘Tuberculosis’ due to the presence of zero cases in at least one cell.
The ‘terrible’ and ‘unhappy’ categories of the Delighted/Terrible scale were merged to provide sufficient numbers in each cell.
Distress, impairment and disability by birth cohort
Mean scores and beta coefficients for the K10, WHODAS and days out of role are provided in Table 3. Lower rates of impairment and disability according to the WHODAS and days out of role due to mental and physical health were found for the young and middle age cohorts in comparison to the older cohort, albeit the difference between the middle age and older cohorts for days out of role was not significant (β = −0.25, p = 0.07). In contrast, there were no significant differences between the three cohorts when examining mean K10 scores.
Psychological distress and impairment amongst those with any disorder (12 months) by birth cohort.
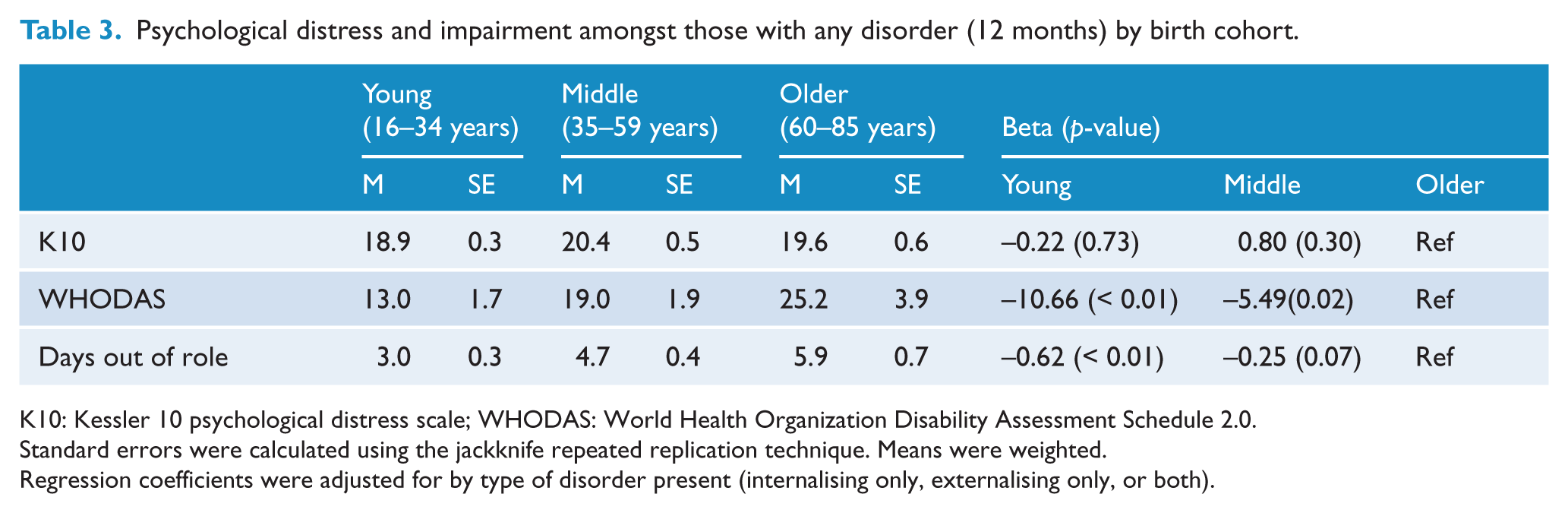
K10: Kessler 10 psychological distress scale; WHODAS: World Health Organization Disability Assessment Schedule 2.0.
Standard errors were calculated using the jackknife repeated replication technique. Means were weighted.
Regression coefficients were adjusted for by type of disorder present (internalising only, externalising only, or both).
Social networks and treatment seeking by birth cohort
Table 4 provides the frequencies, standard errors and odds ratios between birth cohorts and the number and type of social network. Examining the descriptive frequencies, the birth cohorts differed on their social networks. Across both questions, the young cohort were significantly less likely to have no contact or no friends that they could rely on and confide in about a serious problem compared to the older age cohort. However, when considering family members, there were no significant differences between the cohorts. When considering caregiver status, members from the younger cohort were significantly less likely to be a primary caregiver in comparison to the older cohort (OR = 0.57, 95% CI = 0.35–0.95).
Social networks and treatment seeking amongst those with any disorder (12 months) by birth cohort.
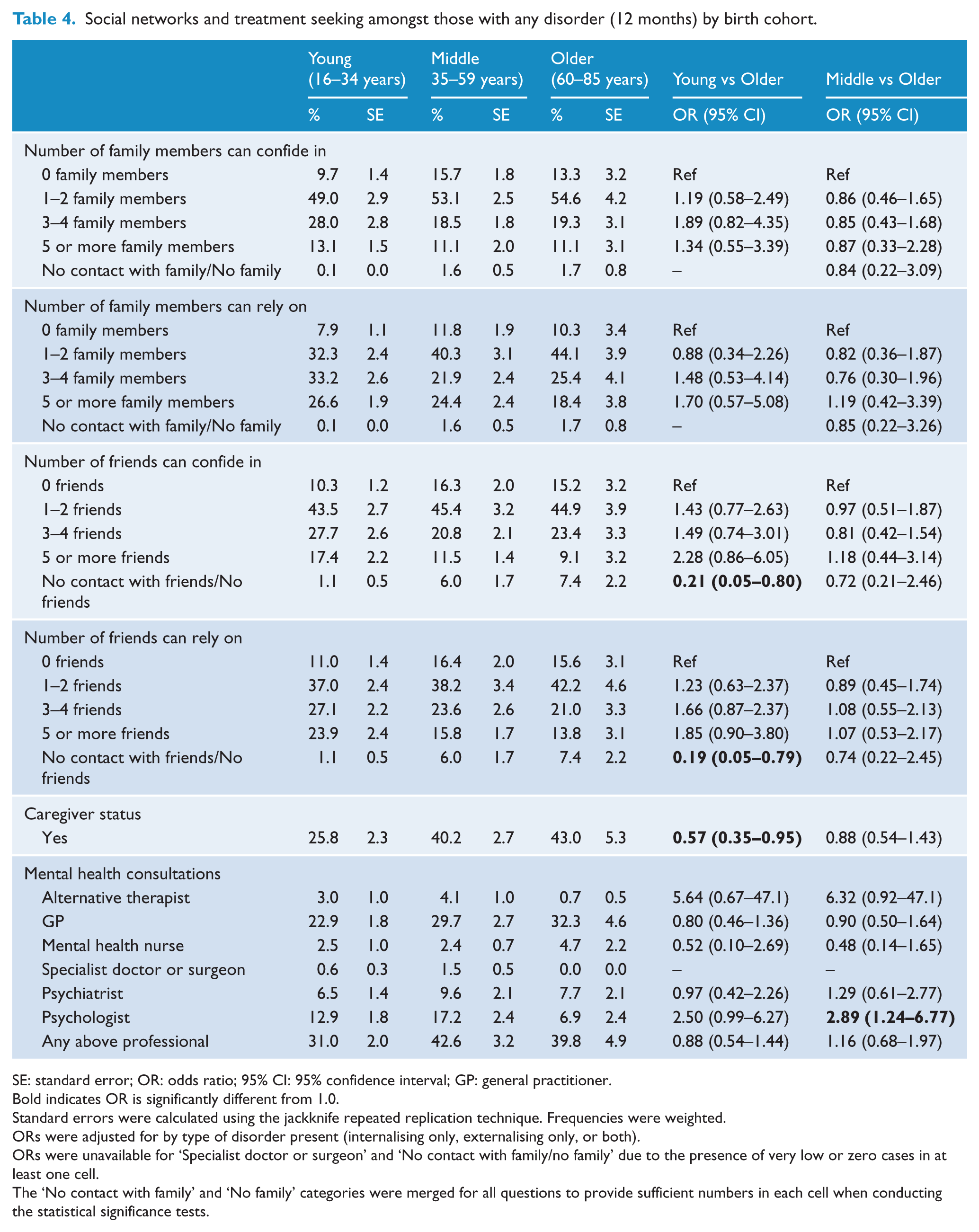
SE: standard error; OR: odds ratio; 95% CI: 95% confidence interval; GP: general practitioner.
Bold indicates OR is significantly different from 1.0.
Standard errors were calculated using the jackknife repeated replication technique. Frequencies were weighted.
ORs were adjusted for by type of disorder present (internalising only, externalising only, or both).
ORs were unavailable for ‘Specialist doctor or surgeon’ and ‘No contact with family/no family’ due to the presence of very low or zero cases in at least one cell.
The ‘No contact with family’ and ‘No family’ categories were merged for all questions to provide sufficient numbers in each cell when conducting the statistical significance tests.
The results for treatment-seeking status by birth cohort are also provided in Table 4. Overall, treatment seeking across all three birth cohorts was quite low with about 31% of the young, 43% of the middle age and 40% of the older age cohorts seeking treatment from any professional. The birth cohorts were similar with respect to seeking treatment for their mental health problem in the past 12 months across a number of different treatment professionals, including alternative therapists, mental health nurses, specialist doctors and psychiatrists. There was a significant difference between treatment-seeking rates for psychologists, with the middle age cohort and to a lesser extent the younger cohort more likely to consult a psychologist in comparison to the older age cohort (OR = 2.89, 95% CI = 1.24–6.77; OR = 2.50, 95% CI = 0.99–6.27, respectively). In contrast, approximately 32% of older respondents had reported seeing a GP for their mental health in the past 12 months compared to approximately 23% of younger respondents, although this decrease was not significant after adjusting for the type of disorder present.
Discussion
The current study demonstrated that a number of differences exist between the young, middle age and older age birth cohorts in the Australian general population on a range of clinically relevant factors. In particular, this study indicated that clinicians and researchers should be cognisant of how people from different birth cohorts in the population presenting to treatment with a mental disorder may differ in terms of their profile of specific disorders, severity and distress rates, social network, treatment-seeking behaviour and physical co-morbidities. We now focus on some of the more notable disparities observed between the three birth cohorts.
The three birth cohorts differed dramatically in terms of the profile of specific disorders experienced amongst those with any mental disorder in the past 12 months. A preponderance of internalising disorders was experienced in the middle and older age cohorts in comparison to the young cohort, particularly depression, social phobia, GAD and PTSD. In contrast, there were substantially more externalising disorders, particularly alcohol abuse, observed in the younger cohorts than the middle or older age cohort. However, this is not to say that internalising disorders are experienced only in middle to late life, as approximately 70% of the young cohort experienced any internalising disorder, a sizable proportion. Instead, it appears that there is a lack of externalising disorders diagnosed in the older cohorts. It is unclear whether this is a true finding or an artefact of assessment; for example, the older cohort may be less likely to report drug or alcohol problems or the diagnostic criteria may not accurately reflect externalising disorders in older age. That being said, previous evidence has demonstrated significant age differences in affective decision making that often precedes the engagement in risk-taking behaviour, which includes greater experimentation with alcohol and drugs by adolescents (Cauffman et al., 2010).
The rates of specific internalising and externalising disorders are relevant when considering the degree and type of co-morbidity experienced. The results suggest that the number of co-morbid disorders remains relatively stable across the age bands, with a substantial number (~40%) of individuals with any mental disorder appearing to receive two or more diagnoses. However, the type of co-morbidity appears to differ across the birth cohorts, with the young cohort experiencing a greater degree of co-morbidity across the disorder clusters of internalising and externalising in comparison to the older cohorts who experience a greater degree of co-morbidity within the internalising cluster. This has important implications for the treatment of co-morbid conditions and obtaining access to sufficient services that can treat co-occurring mental health and substance use disorders. Many existing treatment services often operate in a ‘diagnostic silo’, meaning that they specialise in the treatment of disorders within diagnostic clusters rather than between clusters, thereby creating additional burden amongst younger and middle-aged individuals who present with co-morbid disorders between clusters and who fail to receive adequate treatment (Kavanagh et al., 2003).
The results also question the notion that older age is relatively blissful with regard to mental health and especially in the context of co-morbid physical and mental disorders. The results from the K10 indicate that all three cohorts with a mental disorder experience similar rates of distress; however, older adults were more likely to rate their physical health and satisfaction with life as poor in comparison to the younger cohorts. As expected, the older age cohort experienced a preponderance of physical and mental health disorder co-morbidity with the greatest disparity occurring with cardiovascular disease and chronic pain/joint problems. The relationship between depression and vascular disease has been identified by numerous studies in the extant literature and has resulted in a vascular depression hypothesis. This states that vascular disease causes brain lesions and higher rates of white-matter hyperintensities that disrupt the capacity to regulate mood and therefore result in depressive states (McKinney and Sibille, 2013). This hypothesis would also suggest that depression may be qualitatively different in late life than early-onset, and therefore older adults will present with clinically different symptom profiles, perhaps serving as an explanation for the poor recognition of depression in older age (Mitchell et al., 2010). Other notable qualitative differences between the disorder profiles observed in the current study include the higher rate of suicidality amongst the young age cohort in comparison to the middle and older age cohorts. This finding is at odds with the finding of a higher prevalence of depression and GAD amongst the middle and older age cohorts. The finding may represent the influence of additional risk factors for suicidality among young adults, such as increased substance use (Borges et al., 2000), relationship breakdown (Beautrais et al., 1997), impulsivity and aggression (McGirr et al., 2008).
There were several significant differences between the birth cohorts and social networks, with the younger cohort less likely to have stated that they had no friends that they could confide in or rely on regarding a serious problem. Previous evidence has indicated that lower social support and a higher degree of loneliness are related to lower rates of treatment seeking (Kang et al., 2007). However, our study found the conflicting result that treatment seeking overall was highest amongst the middle age and older age cohorts. These results confirm previous studies that have questioned the link between social support and treatment seeking (Steel et al., 2006). Instead, treatment seeking might be primarily influenced by the perception and stigma of mental disorders, the quality of available services, as well as the degree of mental health literacy within the community (Cooper, et al., 2003; Jorm, 2000b). In addition, increased treatment seeking amongst the older cohorts might be due to the large lag between first onset of the disorder and time to seek treatment (Wang et al., 2005), suggesting that perhaps older individuals who have lived with a remitting and recurring disorder for most of their life may have come to the conclusion that professional help is warranted. Alternatively, poorer physical health experienced by individuals from the older cohort may result in a greater frequency of GP visits in comparison to younger cohorts and therefore additional mental health problems may be detected and treated by GPs through routine physical and mental health checks. This would also explain the finding regarding the greater role GPs have in the treatment of mental health conditions in comparison to psychologists among the older cohort. This trend may also reflect a higher rate of stigma associated with visiting a psychologist by the older age cohort. Further investigations regarding differences in treatment seeking across age cohorts and the reasons for differential treatment rates are now warranted.
There were several strengths of the current study. These include the use of a representative general population-based sample, a comprehensive assessment of mental and physical disorders that allowed for assessment of co-morbidity, and the examination of different factors of clinical interest that provide a greater perspective of mental disorders across birth cohorts. However, there were some limitations that warrant further discussion. First, the current study was based on a cross-sectional survey of the Australian population, thereby providing a snapshot of the three birth cohorts under examination. It is not known whether the clinical factors related to mental disorders in the current older age cohort will continue to emerge in the middle age cohort 20 years from now. Indeed, the differences between birth cohorts could reflect significant changes that come with age or differences between the environmental and social upbringing of the various cohorts. Further research using longitudinal designs is required to separate age from cohort effects. Second, the Australian survey was limited with respect to a maximum age range of 85 years. This restricted our ability to assess differences in mental health profiles amongst the older age cohort; for example, comparing 60–84-years-olds with those aged 85+ years. The additional burden associated with physical disorders, impairment and service use that accompany very advanced aging will most likely result in significant differences amongst the broad descriptive category of ‘older’ individuals and requires further empirical investigation. Third, the survey operationalised the standard DSM-IV diagnostic criteria across all birth cohorts using the WMH-CIDI. Whilst this instrument has desirable psychometric properties, it is not firmly established that the DSM-IV criteria accurately capture the nature of mental disorders across different age brackets, particularly qualitative differences in late-life depression. Indeed, a key area of focus for revising the DSM-IV was the ability of the criteria to adequately account for development and different symptom expression across a lifetime (Narrow et al., 2007). The extent to which the publication of the DSM-5 has addressed these notable limitations has yet to be confirmed. Therefore, further research is required that utilises various diagnostic instruments and tools that are tailored for different birth cohorts as a means of detecting any differences in how disorders present clinically across the age bands.
In conclusion, the current study indicates that birth cohorts are distinguished by a number of important clinical factors. Clinicians and researchers need to be cognisant that mental disorders manifest as highly heterogeneous constructs. The presentation of a disorder in a younger individual could be vastly different from the presentation of the same disorder in an older individual. Indeed, older individuals tend to experience a greater frequency of internalising disorders in combination with physical disability and lack of social support, yet they are more likely than their younger counterparts to seek treatment, particularly from GPs. In contrast, younger individuals demonstrate a combination of internalising and externalising disorders and co-morbidity, less physical impairment and more social support, yet suicidal ideation and attempts are experienced at a higher rate. The additional burden associated with these factors and how they apply to different birth cohorts must be taken into consideration when planning mental health services and effective treatment for the general population.
Footnotes
Funding
This research was supported by a National Health and Medical Research Council Early Career Fellowship no. 1052327 and a National Health and Medical Research Council Project grant no. 1045013.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.